
Recovery of Abdominal Muscle Thickness and Contractile Function in Women after Childbirth

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
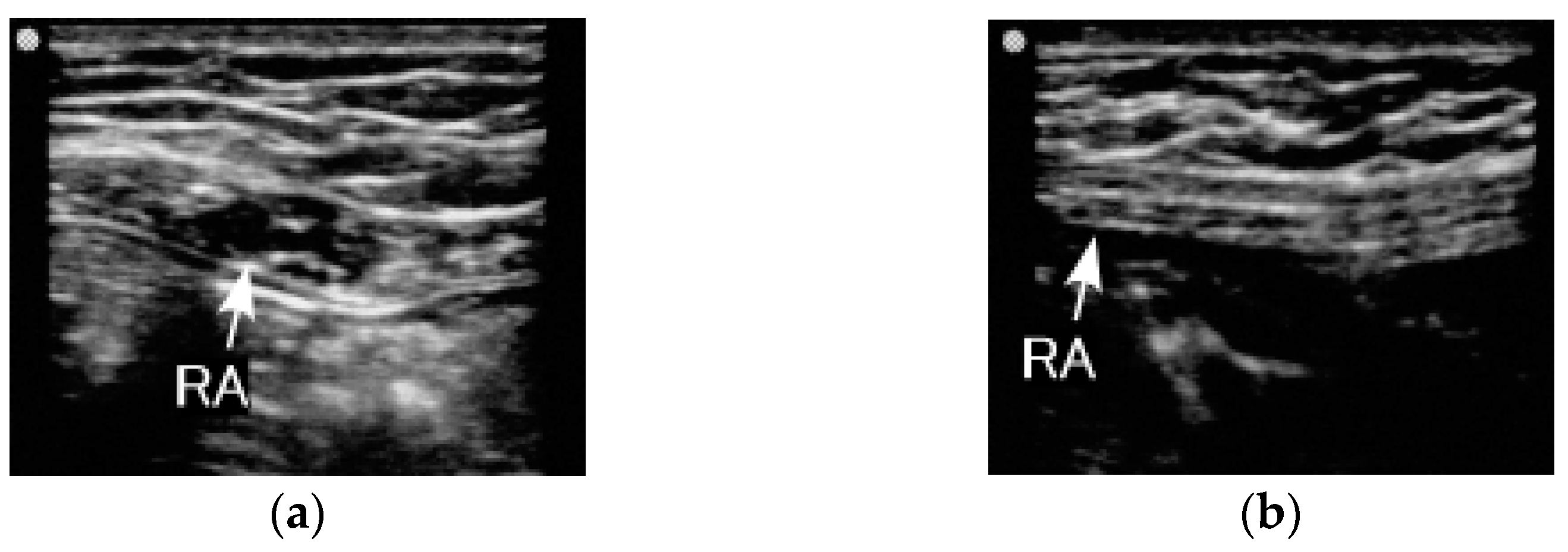
2.2. Equipment
2.3. Procedure
2.4. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, W.H.; Meijer, O.G.; Uegaki, K.; Mens, J.M.; van Dieen, J.H.; Wuisman, P.I.; Ostgaard, H.C. Pregnancy-related pelvic girdle pain (PPP), I: Terminology, clinical presentation, and prevalence. Eur. Spine J. 2004, 13, 575–589. [Google Scholar] [CrossRef]
- Hodges, P.W. Is there a role for transversus abdominis in lumbo-pelvic stability? Man Ther 1999, 4, 74–86. [Google Scholar] [CrossRef]
- Gutke, A.; Ostgaard, H.C.; Oberg, B. Association between muscle function and low back pain in relation to pregnancy. J. Rehabil. Med. 2008, 40, 304–311. [Google Scholar] [CrossRef]
- Noren, L.; Ostgaard, S.; Johansson, G.; Ostgaard, H.C. Lumbar back and posterior pelvic pain during pregnancy: A 3-year follow-up. Eur. Spine J. 2002, 11, 267–271. [Google Scholar] [CrossRef]
- Deering, R.E.; Cruz, M.; Senefeld, J.W.; Pashibin, T.; Eickmeyer, S.; Hunter, S.K. Impaired Trunk Flexor Strength, Fatigability, and Steadiness in Postpartum Women. Med. Sci. Sports Exerc. 2018, 50, 1558–1569. [Google Scholar] [CrossRef]
- Gilleard, W.L.; Brown, J.M. Structure and function of the abdominal muscles in primigravid subjects during pregnancy and the immediate postbirth period. Phys. Ther. 1996, 76, 750–762. [Google Scholar] [CrossRef] [PubMed]
- Coldron, Y.; Stokes, M.J.; Newham, D.J.; Cook, K. Postpartum characteristics of rectus abdominis on ultrasound imaging. Man Ther. 2008, 13, 112–121. [Google Scholar] [CrossRef] [PubMed]
- Weis, C.A.; Triano, J.J.; Barrett, J.; Campbell, M.D.; Croy, M.; Roeder, J. Ultrasound Assessment of Abdominal Muscle Thickness in Postpartum vs Nulliparous Women. J. Manip. Physiol. Ther. 2015, 38, 352–357. [Google Scholar] [CrossRef]
- Borders, N. After the afterbirth: A critical review of postpartum health relative to method of delivery. J. Midwifery Womens Health 2006, 51, 242–248. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists. Committee Opinion No.650 Summary: Physical Activity and Exercise During Pregnancy and the Postpartum Period. Obstet Gynecol. 2015, 126, 1326–1327. [Google Scholar]
- Henry, S.M.; Westervelt, K.C. The use of real-time ultrasound feedback in teaching abdominal hollowing exercises to healthy subjects. J. Orthop. Sports Phys. Ther 2005, 35, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Teyhen, D.S.; Miltenberger, C.E.; Deiters, H.M.; Del Toro, Y.M.; Pulliam, J.N.; Childs, J.D.; Boyles, R.E.; Flynn, T.W. The use of ultrasound imaging of the abdominal drawing-in maneuver in subjects with low back pain. J. Orthop. Sports Phys. Ther 2005, 35, 346–355. [Google Scholar] [CrossRef]
- Hodges, P.W.; Pengel, L.H.; Herbert, R.D.; Gandevia, S.C. Measurement of muscle contraction with ultrasound imaging. Muscle Nerve 2003, 27, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Hides, J.; Wilson, S.; Stanton, W.; McMahon, S.; Keto, H.; McMahon, K.; Bryant, M.; Richardson, C. An MRI investigation into the function of the transversus abdominis muscle during "drawing-in" of the abdominal wall. Spine (Phila Pa 1976) 2006, 31, E175–E178. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.E.; Goldspink, G. Changes in sarcomere length and physiological properties in immobilized muscle. J. Anat. 1978, 127 Pt 3, 459–468. [Google Scholar]
- Friden, J.; Ponten, E.; Lieber, R.L. Effect of muscle tension during tendon transfer on sarcomerogenesis in a rabbit model. J. Hand Surg. Am. 2000, 25, 138–143. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Makarov, M.; Birch, J.; Samchukov, M. The role of variable muscle adaptation to limb lengthening in the development of joint contractures: An experimental study in the goat. J. Pediatr. Orthop. 2009, 29, 175–181. [Google Scholar] [CrossRef]
- Elsalanty, M.; Makarov, M.; Cherkashin, A.; Birch, J.; Samchukov, M. Changes in pennate muscle architecture after gradual tibial lengthening in goats. Anat. Rec. (Hoboken) 2007, 290, 461–467. [Google Scholar] [CrossRef]
- Takahashi, M.; Ward, S.R.; Friden, J.; Lieber, R.L. Muscle excursion does not correlate with increased serial sarcomere number after muscle adaptation to stretched tendon transfer. J. Orthop. Res. 2012, 30, 1774–1780. [Google Scholar] [CrossRef]
- Winters, T.M.; Takahashi, M.; Lieber, R.L.; Ward, S.R. Whole muscle length-tension relationships are accurately modeled as scaled sarcomeres in rabbit hindlimb muscles. J. Biomech. 2011, 44, 109–115. [Google Scholar] [CrossRef]
- Heslinga, J.W.; te Kronnie, G.; Huijing, P.A. Growth and immobilization effects on sarcomeres: A comparison between gastrocnemius and soleus muscles of the adult rat. Eur. J. Appl. Physiol. Occup. Physiol. 1995, 70, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.H.; Matsumoto, D.E. Adaptation of skeletal muscle to immobilization in a shortened position. Muscle Nerve 1988, 11, 231–244. [Google Scholar] [CrossRef]
- Fink, B.; Neuen-Jacob, E.; Lienert, A.; Francke, A.; Niggemeyer, O.; Ruther, W. Changes in canine skeletal muscles during experimental tibial lengthening. Clin. Orthop. Relat. Res. 2001, 385, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Kaljumae, U.; Martson, A.; Haviko, T.; Hanninen, O. The effect of lengthening of the femur on the extensors of the knee. An electromyographic study. J. Bone Jt. Surg. Am. 1995, 77, 247–250. [Google Scholar] [CrossRef] [PubMed]
- Fujita, N.; Fujimoto, T.; Tasaki, H.; Arakawa, T.; Matsubara, T.; Miki, A. Influence of muscle length on muscle atrophy in the mouse tibialis anterior and soleus muscles. Biomed. Res. 2009, 30, 39–45. [Google Scholar] [CrossRef]
- Ohira, Y.; Yasui, W.; Roy, R.R.; Edgerton, V.R. Effects of muscle length on the response to unloading. Acta Anat. (Basel) 1997, 159, 90–98. [Google Scholar] [CrossRef] [PubMed]
- McMeeken, J.M.; Beith, I.D.; Newham, D.J.; Milligan, P.; Critchley, D.J. The relationship between EMG and change in thickness of transversus abdominis. Clin. Biomech. (Bristol, Avon) 2004, 19, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Pulkovski, N.; Mannion, A.F.; Caporaso, F.; Toma, V.; Gubler, D.; Helbling, D.; Sprott, H. Ultrasound assessment of transversus abdominis muscle contraction ratio during abdominal hollowing: A useful tool to distinguish between patients with chronic low back pain and healthy controls? Eur. Spine J. 2012, 21 (Suppl. 6), S750–S759. [Google Scholar] [CrossRef]
- Mannion, A.F.; Pulkovski, N.; Gubler, D.; Gorelick, M.; O’Riordan, D.; Loupas, T.; Schenk, P.; Gerber, H.; Sprott, H. Muscle thickness changes during abdominal hollowing: An assessment of between-day measurement error in controls and patients with chronic low back pain. Eur. Spine J. 2008, 17, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.G.; Lee, L.J.; McLaughlin, L. Stability, continence and breathing: The role of fascia following pregnancy and delivery. J. Bodyw. Mov. Ther. 2008, 12, 333–348. [Google Scholar] [CrossRef]
- Madokoro, S.; Miaki, H. Relationship between transversus abdominis muscle thickness and urinary incontinence in females at 2 months postpartum. J. Phys. Ther. Sci. 2019, 31, 108–111. [Google Scholar] [CrossRef] [PubMed]
- Betran, A.P.; Ye, J.; Moller, A.B.; Zhang, J.; Gulmezoglu, A.M.; Torloni, M.R. The Increasing Trend in Caesarean Section Rates: Global, Regional and National Estimates: 1990–2014. PLoS ONE 2016, 11, e0148343. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Group | PN | CTL | |||
|---|---|---|---|---|---|
| (n = 9) | (n = 15) | ||||
| Parameter | Mean | SD | Mean | SD | p-Value |
| Height (cm) | 162.4 | 2.8 | 161.3 | 6.1 | 0.86 |
| Weight (kg) 1 | 53.5 | 5.2 | 53.8 | 5.2 | 0.97 |
| Age (years) | 33.2 | 5.2 | 29.4 | 4.1 | 0.12 |
| Group | CTL | PN | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 36–39 weeks | 1 month | 2 months | 3 months | 4 months | 5 months | 6 months | ||||||||||
| Muscle | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| Muscle thicknesses (mm) | ||||||||||||||||
| RA | 9.47 | 1.44 | 4.80 | 0.84 * | 8.49 | 2.10 | 8.20 | 1.84 | 7.87 | 1.35 | 7.41 | 1.14 | 7.20 | 1.06 | 8.00 | 1.32 |
| EO | 4.87 | 1.44 | 3.70 | 1.17 | 4.70 | 1.28 | 5.33 | 1.45 | 4.98 | 1.68 | 4.90 | 1.59 | 5.06 | 1.67 | 5.16 | 1.45 |
| IO | 7.73 | 1.71 | 5.45 | 1.58 * | 5.58 | 0.94 * | 6.06 | 1.03 * | 6.56 | 1.88 * | 6.20 | 1.35 * | 7.13 | 2.35 | 6.36 | 1.60 * |
| TrA | 3.38 | 1.10 | 2.56 | 0.54 * | 4.32 | 2.94 | 3.14 | 0.69 | 4.18 | 2.64 | 3.40 | 0.59 | 3.27 | 0.53 | 2.99 | 0.39 * |
| Muscle length (mm) | ||||||||||||||||
| RA (L1) | 57.7 | 22.7 | 94.5 | 20.6 * | 63.3 | 11.7 | 59.7 | 12.5 | 53.4 | 11.3 | 56.9 | 12.0 | 54.7 | 51.4 | 10.7 | 10.7 |
| RA (L2) | 66.1 | 8.3 | 80.8 | 26.9 | 60.8 | 8.6 | 60.0 | 15.2 | 58.9 | 9.5 | 59.3 | 14.3 | 58.8 | 13.5 | 60.2 | 12.1 |
| RA (L3) | 64.5 | 8.3 | 73.5 | 12.0 | 58.3 | 10.4 | 53.8 | 4.8 | 57.7 | 13.1 | 47.7 | 4.6 | 52.5 | 9.6 | 59.2 | 12.6 |
| Tendinous intersection length | ||||||||||||||||
| L1-L2 | 12.1 | 4.4 | 19.8 | 6.6 | 14.3 | 3.1 | 14.0 | 4.0 | 12.4 | 5.9 | 10.7 | 4.1 | 11.1 | 3.2 | 12.6 | 4.7 |
| L2-L3 | 10.6 | 3.0 | 20.0 | 7.1 * | 12.8 | 2.0 | 13.7 | 4.3 | 11.0 | 2.5 | 11.1 | 4.7 | 14.3 | 5.1 | 13.7 | 4.5 |
| Group | CTL | PN | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Month | 2 Months | 3 Months | 4 Months | 5 Months | 6 Months | |||||||||
| Muscle | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| RA | 1.12 | 0.15 | 1.09 | 0.04 | 1.18 | 0.16 | 1.17 | 0.23 | 1.21 | 0.18 | 1.14 | 0.20 | 0.26 | 0.21 |
| EO | 1.11 | 0.28 | 1.18 | 0.76 | 0.96 | 0.37 | 1.02 | 0.39 | 1.12 | 0.35 | 1.03 | 0.38 | 1.12 | 0.39 |
| IO | 1.21 | 0.23 | 1.13 | 0.13 | 1.29 | 0.34 | 1.11 | 0.31 | 1.28 | 0.39 | 1.26 | 0.31 | 1.22 | 0.32 |
| TrA | 1.68 | 0.56 | 1.07 | 0.20 * | 1.13 | 0.20 * | 1.18 | 0.19 * | 1.02 | 0.26 * | 1.26 | 0.36 | 1.40 | 0.59 |
| Muscle Thickness | Muscle Thickness Ratio | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RA | EO | IO | TrA | RA | EO | IO | TrA | |||||||||
| r | p | r | p | r | p | r | p | r | p | r | p | r | p | r | p | |
| Age | 0.36 | 0.38 | 0.37 | 0.37 | 0.30 | 0.46 | 0.24 | 0.55 | 0.32 | 0.43 | 0.59 | 0.12 | 0.41 | 0.31 | 0.27 | 0.56 |
| Body mass index | 0.48 | 0.23 | 0.35 | 0.40 | 0.28 | 0.51 | 0.44 | 0.27 | −0.12 | 0.78 | 0.21 | 0.61 | 0.50 | 0.21 | 0.04 | 0.94 |
| Number of births | 0.33 | 0.43 | 0.54 | 0.16 | 0.06 | 0.90 | 0.22 | 0.60 | 0.00 | 1.00 | 0.22 | 0.60 | 0.00 | 1.00 | 0.29 | 0.53 |
| Foetal weight | −0.24 | 0.57 | −0.32 | 0.43 | 0.16 | 0.71 | 0.14 | 0.73 | 0.42 | 0.29 | 0.71 | 0.07 | 0.50 | 0.21 | 0.57 | 0.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fukano, M.; Tsukahara, Y.; Takei, S.; Nose-Ogura, S.; Fujii, T.; Torii, S. Recovery of Abdominal Muscle Thickness and Contractile Function in Women after Childbirth. Int. J. Environ. Res. Public Health 2021, 18, 2130. https://doi.org/10.3390/ijerph18042130
Fukano M, Tsukahara Y, Takei S, Nose-Ogura S, Fujii T, Torii S. Recovery of Abdominal Muscle Thickness and Contractile Function in Women after Childbirth. International Journal of Environmental Research and Public Health. 2021; 18(4):2130. https://doi.org/10.3390/ijerph18042130
Chicago/Turabian StyleFukano, Mako, Yuka Tsukahara, Seira Takei, Sayaka Nose-Ogura, Tomoyuki Fujii, and Suguru Torii. 2021. "Recovery of Abdominal Muscle Thickness and Contractile Function in Women after Childbirth" International Journal of Environmental Research and Public Health 18, no. 4: 2130. https://doi.org/10.3390/ijerph18042130
APA StyleFukano, M., Tsukahara, Y., Takei, S., Nose-Ogura, S., Fujii, T., & Torii, S. (2021). Recovery of Abdominal Muscle Thickness and Contractile Function in Women after Childbirth. International Journal of Environmental Research and Public Health, 18(4), 2130. https://doi.org/10.3390/ijerph18042130