
Factors That Influence Use of a Patient Portal by Health Professionals

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting and the Patient Portal
2.3. Participants
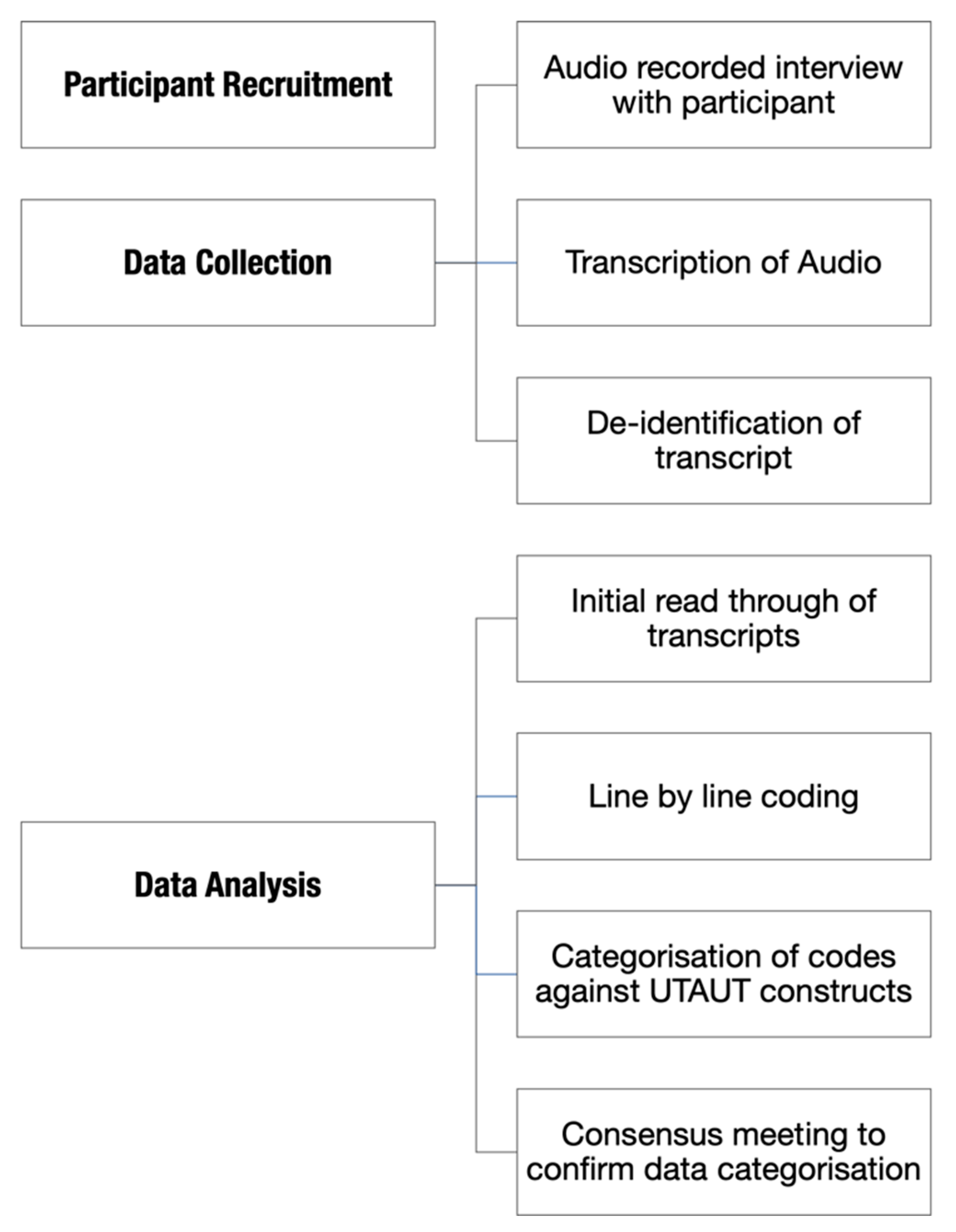
2.4. Procedures
2.5. Data Analysis
2.6. Ethics
3. Results
- Experience Design (how intended functionality influenced use of the patient portal);
- Technical Reliability (unintended functionality, e.g., technical bugs);
- Health professional workflow (how the portal integrates with health professionals’ current ways of working);
- Improved efficiency for patients/carers;
- Patient Feedback;
- Technical Support;
- Integration with systems;
- Implementation Support.
3.1. Performance Expectancy
3.1.1. Experience Design
3.1.2. Technical Reliability
3.2. Effort Expectancy
3.2.1. Health Professional Workflow
3.2.2. Improved Efficiency for Patients/Carers
3.3. Social Influence
Patient Feedback
3.4. Facilitating Conditions
3.4.1. Technical Support
3.4.2. Integration with Systems
3.4.3. Implementation Support
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hennemann, S.; Beutel, M.E.; Zwerenz, R. Ready for eHealth? Health professionals’ acceptance and adoption of eHealth interventions in inpatient routine care. J. Health Commun. 2017, 22, 274–284. [Google Scholar] [CrossRef]
- Kruse, C.S.; Ozoa, N.M.; Smith, J.G. Patient portals and the management of pediatric chronic diseases–a systematic literature review. Med. Res. Arch. 2015, 2, 1. [Google Scholar] [CrossRef][Green Version]
- Bush, R.A.; Connelly, C.D.; Fuller, M.; Pérez, A. Implementation of the integrated electronic patient portal in the pediatric population: A systematic review. Telemed. E-Health 2016, 22, 144–152. [Google Scholar] [CrossRef]
- Britto, M.T.; Hesse, E.A.; Kamdar, O.J.; Munafo, J.K. Parents’ perceptions of a patient portal for managing their child’s chronic illness. J. Pediatr. 2013, 163, 280–281.e282. [Google Scholar] [CrossRef]
- Byczkowski, T.L.; Munafo, J.K.; Britto, M.T. Family perceptions of the usability and value of chronic disease web-based patient portals. Health Inform. J. 2014, 20, 151–162. [Google Scholar] [CrossRef]
- Otte-Trojel, T.; de Bont, A.; Rundall, T.G.; van de Klundert, J. How outcomes are achieved through patient portals: A realist review. J. Am. Med. Inf. Assoc. 2014, 21, 751–757. [Google Scholar] [CrossRef]
- Kruse, C.S.; Argueta, D.A.; Lopez, L.; Nair, A. Patient and provider attitudes toward the use of patient portals for the management of chronic disease: A systematic review. J. Med. Internet Res. 2015, 17, e40. [Google Scholar] [CrossRef] [PubMed]
- Golden, S.L.; Nageswaran, S. Caregiver voices: Coordinating care for children with complex chronic conditions. Clin. Pediatr. 2012, 51, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Eichenberg, C.; Wolters, C.; Brähler, E. The internet as a mental health advisor in Germany—results of a national survey. PLoS ONE 2013, 8, e79206. [Google Scholar] [CrossRef] [PubMed]
- Hannan, A. Providing patients online access to their primary care computerised medical records: A case study of sharing and caring. J. Innov. Health Inf. 2010, 18, 41–49. [Google Scholar] [CrossRef] [PubMed]
- De Waal, B.M.; Batenburg, R.; Fruytier, B. Metastructuration actions of management: Critical for stakeholder intervention in IS/IT implementations. Int. J. Healthc. Technol. Manag. 2012, 13, 242–261. [Google Scholar] [CrossRef]
- Abdrbo, A.A.; Hudak, C.A.; Anthony, M.K.; Douglas, S.L. Information systems use, benefits, and satisfaction among Ohio RNs. CIN Comput. Inf. Nurs. 2011, 29, 59–65. [Google Scholar] [CrossRef]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User acceptance of information technology: Toward a unified view. MIS Q. 2003, 425–478. [Google Scholar] [CrossRef]
- Cimperman, M.; Brenčič, M.M.; Trkman, P. Analyzing older users’ home telehealth services acceptance behavior—applying an Extended UTAUT model. Int. J. Med. Inf. 2016, 90, 22–31. [Google Scholar] [CrossRef] [PubMed]
- Hoque, R.; Sorwar, G. Understanding factors influencing the adoption of mHealth by the elderly: An extension of the UTAUT model. Int. J. Med. Inf. 2017, 101, 75–84. [Google Scholar] [CrossRef]
- Shiferaw, K.B.; Mehari, E.A. Modeling predictors of acceptance and use of electronic medical record system in a resource limited setting: Using modified UTAUT model. Inform. Med. Unlocked 2019, 100182. [Google Scholar] [CrossRef]
- Venkatesh, V.; Sykes, T.A.; Zhang, X. ‘Just what the doctor ordered’: A revised UTAUT for EMR system adoption and use by doctors. In Proceedings of the 2011 44th Hawaii International Conference on System Sciences, Kauai, HI, USA, 4–7 January 2011; pp. 1–10. [Google Scholar] [CrossRef]
- Cohen, J.F.; Bancilhon, J.-M.; Jones, M. South African physicians’ acceptance of e-prescribing technology: An empirical test of a modified UTAUT model. S. Afr. Comput. J. 2013, 50, 43–54. [Google Scholar] [CrossRef]
- Krueger, N.F. Entrepreneurial Resilience: Real & Perceived Barriers to Implementing Entrepreneurial Intentions. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=1155269 (accessed on 15 February 2021).
- Wildenbos, G.A.; Peute, L.; Jaspers, M. Facilitators and barriers of electronic health record patient portal adoption by older adults: A literature study. Stud. Health Technol. Inform. 2017, 235, 308–312. [Google Scholar] [CrossRef]
- Hennington, A.; Janz, B.D. Information systems and healthcare XVI: Physician adoption of electronic medical records: Applying the UTAUT model in a healthcare context. Commun. Assoc. Inf. Syst. 2007, 19, 5. [Google Scholar] [CrossRef][Green Version]
- Petersen, F.; Jacobs, M.; Pather, S. Barriers for User Acceptance of Mobile Health Applications for Diabetic Patients: Applying the UTAUT Model. In Conference on e-Business, e-Services and e-Society; Springer: Cham, Switzerland, 2020; pp. 61–72. [Google Scholar]
- Brinkel, J.; Dako-Gyeke, P.; Krämer, A.; May, J.; Fobil, J.N. An investigation of users’ attitudes, requirements and willingness to use mobile phone-based interactive voice response systems for seeking healthcare in Ghana: A qualitative study. Public Health 2017, 144, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Murray, E.; Burns, J.; May, C.; Finch, T.; O’Donnell, C.; Wallace, P.; Mair, F. Why is it difficult to implement e-health initiatives? A qualitative study. Implement. Sci. 2011, 6, 6. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| UTAUT Construct | Data Categories | Exemplar Quotes |
|---|---|---|
| Performance Expectancy | Experience Design (how intended functionality influenced use of the patient portal) | “I think it looks good on the phone. I think you can see how many messages you’ve got, just like you can if you’ve got emails or something.” |
| “I like the way that you can skip group conversations, so I can read in context… I can read the nursing part, the physio component, and then I can read where my part fits in. I think the families also seem to really like it…” | ||
| Technical Reliability (unintended functionality, e.g., technical bugs) | “I believe that if it’s working the way it’s meant to be working, they can reschedule appointments, or they can request to reschedule appointments, it pops up into their calendars, it’s meant to allow them to have longer or maybe better communication with us.” “We’ll send that initial message out to them, and then we don’t get confirmation there that they’ve received it. So, initially we weren’t sure whether that was because there was a glitch happening at the time, or whether they just hadn’t got it.” “It’s difficult if it’s a one-on-one communication that only comes back to that person, but it needs to be addressed or someone else needs to know about it, needs to be actioned, so that was one of the limitations.” “I think the frustration at this point is that the communication’s getting there and I can see it’s got potential, but there’s so much more that the app can do. And to keep people engaged, I think we need to start rolling out some of those other features. We can’t roll those features out until we fix the glitches, so I feel like it’s slightly losing momentum a little bit.” “So, the challenges would be, what we’ve all had, is with the app crashing. So, we got a lot of people signed up, and then we had quite few consecutive glitches, and we really lost quite a bit of their confidence in using the app.” “There’s been issues where the actual app has crashed…until all of this is running smoothly, I don’t think we will completely get people on board.” | |
| Effort Expectancy | Health professional workflow (how the portal integrates with health professionals’ current ways of working) | “I really like the fact that it’s built into [EMR] and that whatever is typed automatically goes into the notes, so there’s no copying and pasting you need to do from emails or from text messages; that becomes an instant part of the clinical progress notes. That’s really important for workflow and for absolute transparency to when things are happening in a live situation.” “I’ve had less pages for sure. I’m sure I’ve had less pages about little things, like can I have a script? What was my result? … They know if they message me in the app and it’s, “My child is sick”, that I will probably ring them as opposed to reply in the app because I will want more information about that. It’s worked really well for me like that.” “…to come back to our office and sit down, and then look at that [the patient portal]. You know, often we have lots of interruptions, so to spend the time, and just make the part of you do it, I think that’s the challenge, I think that’s what we have to do.” “That’s not something that’s currently built into my day at all [checking messages], and I would have to say that, really, I’ve been very reliant on somebody else flagging that there’s a message for me … And mainly because our days can look very different; that’s a big concern, because there might be days where I won’t actually sit in front of a computer until midday. And yes, I do have a little concern with that.” “We kind of look after half the patients each. So we’re able to manage the communication by just us using it. The dietician and physio have used it very occasionally, but they tend to not use it too much, because they’re not in <the EMR> as often as us. So if they send a message, and a message gets sent back, and it’s for us, it’s going to sit in their inbox until they notice it.” “part of the issue around this is that we are all doubling up on … I don’t know, I’m assuming it’s one of the issues that they’re concerned that clinicians are doubling up on communication and I believe the app is meant to be how we communicate. That’s what the hospital wants, I think.” “The families need to remember that what they’re saying can be read by everyone. So, I think one family made a comment to one of the nurses the other day along the lines of, “This is great, you’re the best team.” We’ve had type of thing. But then people are sending kids, eventually we’ll be able to … It’s just they’ve got to be careful that you don’t offend other health professionals. And it will go both ways.” |
| Improved efficiency for patients/carers | “I think because it’s easy for them to send me a quick message they might be messaging more readily when they might have gone, “Oh, it’s too hard to try and page her and wait for her to ring back” and all of those sorts of things.” “I like that it has made it easier for me to communicate simple things to families rather than have to get into phone calls. It’s easier for families to communicate simple things to me. Definitely more families are using the app than used to email me.” “They can understand and appreciate how it goes into their child’s medical record and they also like that they can go back and read what they’ve sent me, and what my response has been, and that stays on their app, and they know that stays there for me as well. That’s been really good.” | |
| Social Influence | Patient Feedback | “I think that the patient group in general are really impressed with it, and like it as an option, and understand that it’s in its basic phases, and are really quite happy with it.” “I think one of the families was concerned about with information that’s going back and forward, and the security around that information, and obviously, it’s very secure, but they just had an issue with that. That’s the only reason behind not accepting, that I know of.” “Definitely families need to see more benefit from it. There needs to be more for them, I think for the complex kids. I think you’ll find … when this goes live throughout the hospital, the majority of families that will be utilising this will be the frequent fliers, and it’s the frequent attenders that need to see a benefit. So, it probably needs to be solved to them. That probably needs a lot more support to sell it to them, support them, continue to get them to see the benefit of it, and also the support for us as well.” |
| Facilitating Conditions | Technical Support | “They’ve been good. We’ve used [the vendor] as our first port of call and [the vendor] would tell us how to action it.” “[The Vendor] does feed back to us, they were sending through graphs and lists after clinic with who was on it, and then he was following up with who had actually activated it properly… Haven’t had that for a few weeks, but in the initial phase, he was giving stats of what percentage we had taken, things like that.” “I think that they’ve been quite supportive. [The vendor] is the main person who we deal with, and they’ve has been really supportive.” “[The Vendor’s] been very helpful, but our IT department, there seems to be a bit of a gap between [their] knowledge and understanding, and what they would know to do, and what they actually did know to do, because a few times they were just like, no, we don’t know.” “Sometimes or when we would ring a patient, or they would ring us, they would say, ‘We sent you a message earlier today about dah-dah-dah-dah-dah-dah.’ Then they’d keep talking about and we’d go, ‘Oh, we didn’t get a message earlier today from you.’ That kind of thing.” “If I am not sure that something is working, I’m not going to use something. Especially if I have to send information about an appointment or about a change in medication or something.” “I guess, as would be expected, when you’re trialling something, there have certainly been some teething issues…There’s also been a fair bit of time where it’s gone down. The concern for me around that is that families at the other end trying to use it, and it’s not working properly. So they get frustrated and revert back to the old means of communicating with us.” |
| Integration with systems | “On the ward they’ve got the computer’s on wheels, and in a lot of the rooms there’s the fixed computers in the patient care areas, so it’s pretty easy to access anywhere within the hospital.” “I can jump onto [EMR] at any time, so if I’m on night duty in another job, I can log into power chart and find out what the follow up was from that outcome that I knew was being looked into on the Tuesday, or whatever, so it does keep me in the loop, and it’s an easy way to just be able to jump onto power chart any time. You know, midnight, three in the morning, it’s not restrictive like it would be with a telephone. So, it’s good for that way of sharing information around and having it accessible and visible there to easily go through and track the conversation.” “I think the thing for us is that… we have email on our phones, so we’re out and about, we’re not always at our desk and you have to log on. So I think that the beauty for us is that when we have patients emailing us, we have the opportunity on our phone to actually look at it, and respond almost immediately. Whereas we don’t have the opportunity to log on to Powerchart on our phones.” | |
| Implementation Support | “There’s been a lot of good ideas, and plans, and projects in this hospital, but I think there was the appreciation and the realisation that staff just can’t keep taking on extra thing and getting them up and going for people. If you want to get something up and going properly, you need to put in the resources to do it and they did do that, which was excellent. I’m glad they had the foresight to do that, because it’s really good and it would’ve been another thing that fell down if it was allowed to happen naturally, it wouldn’t have…” “Initially it was all very positive. We got lots of information. There was [vendor] staff that were there at the clinic to help with the initial trial in chest and asthma clinic.” “In order to get more uptake for more patients, you actually need more people on the ground who are just doing that… to expect clinicians to do that as well as their clinical work is unrealistic, especially if you really want to roll something out. We’re very happy to mention it, here’s the information on it, but we can’t spend 10 min explaining it, helping them putting it on their phone. We’re in the middle of a clinic. We might be trying to see 10, 12 patients in a half hour, in a two-hour clinic, so we can’t do that.” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janssen, A.; Keep, M.; Selvadurai, H.; Kench, A.; Hunt, S.; Simonds, S.; Marshall, T.; Hatton, L.; Dalla-Pozza, L.; McCullagh, C.; et al. Factors That Influence Use of a Patient Portal by Health Professionals. Int. J. Environ. Res. Public Health 2021, 18, 1877. https://doi.org/10.3390/ijerph18041877
Janssen A, Keep M, Selvadurai H, Kench A, Hunt S, Simonds S, Marshall T, Hatton L, Dalla-Pozza L, McCullagh C, et al. Factors That Influence Use of a Patient Portal by Health Professionals. International Journal of Environmental Research and Public Health. 2021; 18(4):1877. https://doi.org/10.3390/ijerph18041877
Chicago/Turabian StyleJanssen, Anna, Melanie Keep, Hiran Selvadurai, Andrea Kench, Sharon Hunt, Sharon Simonds, Tracey Marshall, Lucy Hatton, Luciano Dalla-Pozza, Cheryl McCullagh, and et al. 2021. "Factors That Influence Use of a Patient Portal by Health Professionals" International Journal of Environmental Research and Public Health 18, no. 4: 1877. https://doi.org/10.3390/ijerph18041877
APA StyleJanssen, A., Keep, M., Selvadurai, H., Kench, A., Hunt, S., Simonds, S., Marshall, T., Hatton, L., Dalla-Pozza, L., McCullagh, C., & Shaw, T. (2021). Factors That Influence Use of a Patient Portal by Health Professionals. International Journal of Environmental Research and Public Health, 18(4), 1877. https://doi.org/10.3390/ijerph18041877