
Social Prestige of the Paramedic Profession

 ,
, 
Abstract
1. Introduction
2. Material and Methods
2.1. Study Participants
2.2. Data Collection
2.3. Statistical Analysis
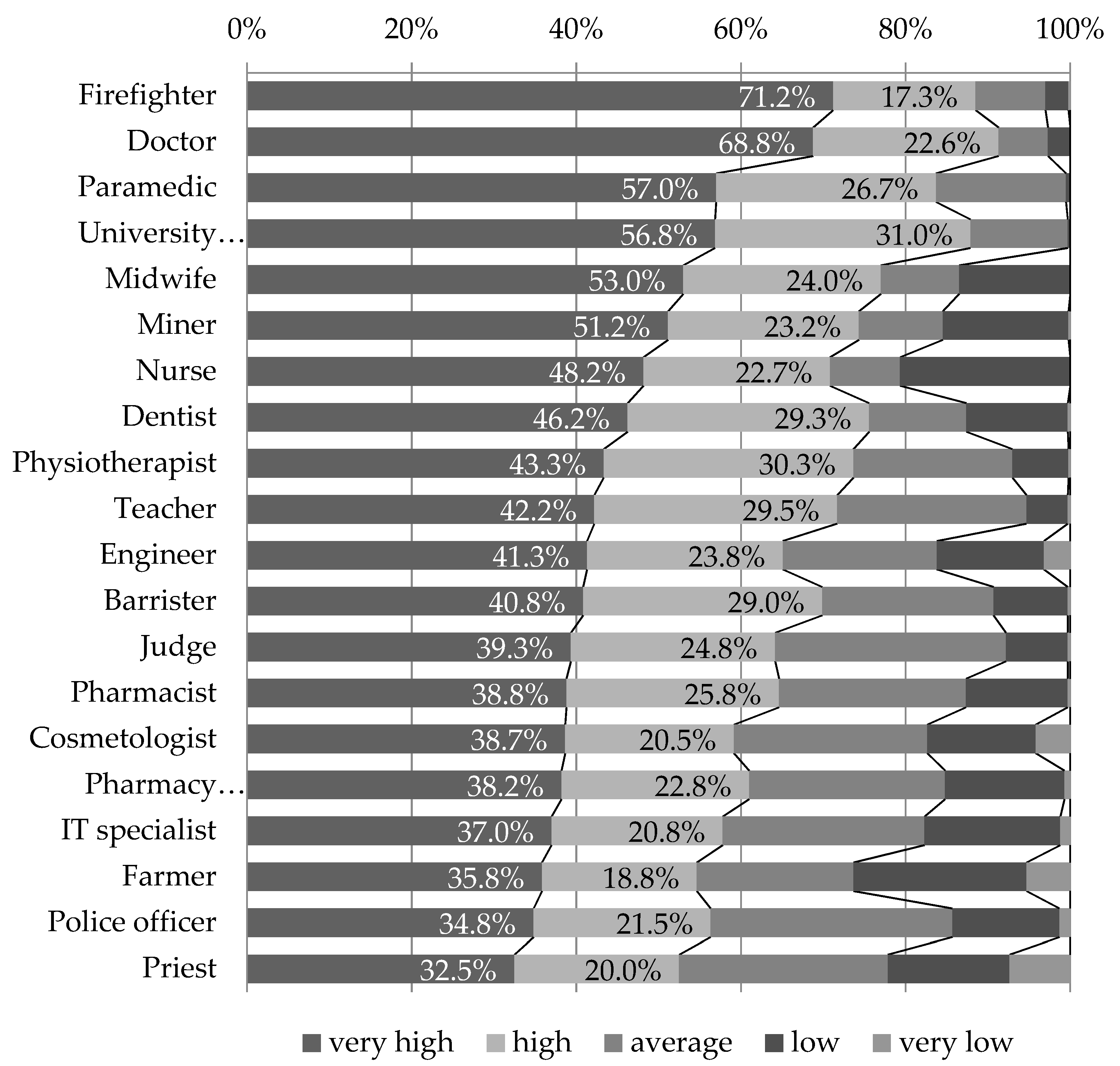
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Act of 8 September 2006 on Emergency Medical Care, Dz.U.2020.0.882. Available online: https://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU20061911410/U/D20061410Lj.pdf (accessed on 28 December 2020).
- The Regulation of the Polish Minister of Health of 16 December 2019 on Medical Rescue Activities and Medical Services Different Than Rescue Activities That Can Be Provided by Paramedics. Dz.U2019.2478. Available online: http://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU20190002478/O/D20192478.pdf (accessed on 28 December 2020).
- Givati, A.; Markham, C.; Street, K. The bargaining of professionalism in emergency care practice: NHS paramedics and higher education. Adv. Health Sci. Educ. 2018, 23, 353–369. [Google Scholar] [CrossRef] [PubMed]
- NHS England. Summary of the Responses to the Public Consultation on Proposals to Introduce Independent Prescribing by Paramedics Across the United Kingdom. 2016. Available online: https://www.england.nhs.uk/wp-content/uploads/2016/02/Paramedics-summary-consult-responses.pdf (accessed on 15 May 2020).
- Evans, R.; McGovern, R.; Birch, J.; Newbury-Birch, D. Which extended paramedic skills are making an impact in emergency care and can be related to the UK paramedic system? A systematic review of the literature. Emerg. Med. J. 2014, 31, 594–603. [Google Scholar] [CrossRef] [PubMed]
- Eaton, G.; Mahtani, K.; Catterall, M. The evolving role of paramedics—A NICE problem to have? J. Health Serv. Res. Policy 2018, 23, 193–195. [Google Scholar] [CrossRef]
- Bigham, B.L.; Kennedy, S.M.; Drennan, I.; Morrison, L.J. Expanding Paramedic Scope of Practice in the Community: A Systematic Review of the Literature. Prehosp. Emerg. Care 2013, 17, 361–372. [Google Scholar] [CrossRef]
- FitzGerald, G.J. Paramedics and scope of practice. Med. J. Aust 2015, 203, 240–241. [Google Scholar] [CrossRef][Green Version]
- Freidson, E. Introduction. In Profession of Medicine: A Study of the Sociology of Applied Knowledge; The University of Chicago Press: Chicago, IL, USA, 1988; pp. XV–XIX. [Google Scholar]
- Williams, B.; Edlington, T. Attitudes towards continuing professional development: A qualitative study of Australian paramedics. Australas. J. Paramed. 2019, 16. [Google Scholar] [CrossRef]
- Williams, B.; Onsman, A.; Brown, T. Is the Australian Paramedic Discipline a Full Profession? Australas. J. Paramed. 2010, 8. [Google Scholar] [CrossRef]
- McClelland, G. The research paramedic: A new role. J. Paramed. Pr. 2013, 5, 582–586. [Google Scholar] [CrossRef]
- First, S.; Tomlins, L.; Swinburn, A. From trade to profession-the professionalisation of the paramedic workforce. J. Paramedic Pr. 2012, 4, 378–381. [Google Scholar] [CrossRef]
- Williams, B.; Onsman, A.; Brown, T. From stretcher-bearer to paramedic: The Australian paramedics’ move towards professionalization. J. Emerg. Prim. Health Care 2009, 7, 990346. [Google Scholar] [CrossRef]
- Brown, P. A day in the life of a paramedic advanced clinical practitioner in primary care. J. Paramed. Pr. 2017, 9, 378–386. [Google Scholar] [CrossRef]
- Seim, J. The Ambulance: Toward a Labor Theory of Poverty Governance. Am. Sociol. Rev. 2017, 82, 451–475. [Google Scholar] [CrossRef]
- Seim, J. Bandage, Sort, and Hustle: Ambulance Crews on the Front Lines of Urban Suffering, 1st ed.; University of California Press: Berkeley, CA, USA, 2020. [Google Scholar]
- Wankhade, P. Different cultures of management and their relationships with organizational performance: Evidence from the UK ambulance service. Public Money Manag. 2012, 32, 381–388. [Google Scholar] [CrossRef]
- Charman, S. Sharing a laugh: The role of humour in relationships between police officers and ambulance staff. Int. J. Sociol. Soc. Policy 2013, 33, 152–166. [Google Scholar] [CrossRef]
- McCann, L.; Granter, E.; Hyde, P.; Hassard, J. Still Blue-Collar after all these Years? An Ethnography of the Professionalization of Emergency Ambulance Work. J. Manag. Stud. 2013, 50, 5. [Google Scholar] [CrossRef]
- McCann, L.; Granter, E.; Hassard, J.; Hyde, P. Where next for the paramedic profession? An ethnography of work culture and occupational identity. Emerg. Med. J. 2015, 32, e6–e7. [Google Scholar] [CrossRef]
- Granter, E.; Wankhade, P.; McCann, L.; Hassard, J.; Hyde, P. Multiple Dimensions of Work Intensity: Ambulance Work as Edgework. Work. Employ. Soc. 2018, 33, 280–297. [Google Scholar] [CrossRef]
- Hansen, C.D.; Rasmussen, K.; Kyed, M. Physical and psychosocial work environment factors and their association with health outcomes in Danish ambulance personnel—A cross-sectional study. BMC Public Health 2012, 12, 534. [Google Scholar] [CrossRef]
- Corman, M.K. Paramedics On and Off the Streets: Emergency Medical Services in the Age of Technological Governance; University of Toronto Press: Toronto, ON, Canada, 2017. [Google Scholar]
- Nurok, M.; Henckes, N. Between professional values and the social valuation of patients: The fluctuating economy of pre-hospital emergency work. Soc. Sci. Med. 2009, 68, 504–510. [Google Scholar] [CrossRef]
- Palmer, C.E. “Trauma Junkies” and Street Work: Occupational Behavior of Paramedics and Emergency Medical Technicians. J. Contemp. Ethnogr. 1983, 12, 162–183. [Google Scholar] [CrossRef]
- Greatbatch, D.; Hanlon, G.; Goode, J.; O’Cathain, A.; Strangleman, T.; Luff, D. Telephone triage, expert systems and clinical expertise. Sociol. Health Illn. 2005, 27, 802–830. [Google Scholar] [CrossRef]
- Hughes, D. The Ambulance Journey as an Information Generating Process. Sociol. Health Illn. 1980, 2, 115–132. [Google Scholar] [CrossRef]
- Tangherlini, T.L. Heroes and Lies: Storytelling Tactics among Paramedics. Folklore 2000, 111, 43–66. [Google Scholar] [CrossRef]
- Corman, M.K.; Melon, K. What Counts? Managing Professionals on the Front Line of Emergency Services. In Under New Public Management: Institutional Ethnographies of Changing Front-Line Work; Griffith, A.I., Smith, D.E., Eds.; University of Toronto Press: Toronto, ON, Canada, 2014; pp. 148–176. [Google Scholar]
- Metz, D.L. Running Hot: Structure and Stress in Ambulance Work; ABT Books: Cambridge, UK, 1981. [Google Scholar]
- James, A. Perceptions of stress in British ambulance personnel. Work. Stress 1988, 2, 319–326. [Google Scholar] [CrossRef]
- Young, K.M.; Cooper, C.L. Occupational stress in the ambulance service: A diagnostic study. Health Manpow. Manag. 1997, 23, 140–147. [Google Scholar] [CrossRef]
- Cydulka, R.K.; Lyons, J.; Moy, A.; Shay, K.; Hammer, J.; Mathews, J. A follow-up report of occupational stress in urban EMT-paramedics. Ann. Emerg. Med. 1989, 18, 1151–1156. [Google Scholar] [CrossRef]
- Clohessy, S.; Ehlers, A. PTSD symptoms, response to intrusive memories and coping in ambulance service workers. Br. J. Clin. Psychol. 1999, 38, 251–265. [Google Scholar] [CrossRef]
- Bennett, P.; Williams, Y.; Page, N.; Hood, K.; Woollard, M. Levels of mental health problems among UK emergency ambulance workers. Emerg. Med. J. 2004, 21, 235–236. [Google Scholar] [CrossRef]
- Kyed, M. Masculinity, Emotions and ‘Communities of Relief’ among Male Emergency Medical Technicians. In Masculinities, Gender Equality and Crisis Management; Ericson, M., Mellstrom, U., Eds.; Routledge: Abingdon, UK, 2016; pp. 34–46. [Google Scholar]
- Ganzeboom, H.B.; De Graaf, P.M.; Treiman, D.J. A standard international socio-economic index of occupational status. Soc. Sci. Res. 1992, 21, 1–56. [Google Scholar] [CrossRef]
- Domański, H. Prestige; Peter Lang: Frankfurt am Main, Germany, 2015. [Google Scholar]
- Bogusz, R.; Nowakowska, L.; Majchrowska, A.; Wiechetek, M.; Piątkowski, W.; Pawlikowski, J. Social prestige of internal medicine. Pol. Arch. Intern. Med. 2020, 130, 155–157. [Google Scholar] [CrossRef]
- Meyer, J.W.; Hammond, P.E. Forms of Status Inconsistency. Soc. Forces 1971, 50, 91–101. [Google Scholar] [CrossRef]
- Domański, H.; Sawiński, Z.; Słomczyński, K.M. Sociological Tools Measuring Occupations. New Classification and Scales; IFIS Publishers: Warsaw, Poland, 2009; pp. 168–179. [Google Scholar]
- Nakao, K.; Treas, J. Computing 1989 Occupational Prestige. Available online: http://www.gss.norc.org/Documents/reports/methodological-reports/MR070.pdf#search=prestige (accessed on 29 June 2020).
- Smith, T.W.; Son, J. Measuring Occupational Prestige on the 2012 General Social Survey; University of Chicago GSS Methodological Report No. 122; University of Chicago: Chicago, IL, USA, 2014. [Google Scholar]
- McCarthy, N. America’s most Prestigious Professions in 2016. Available online: https://www.forbes.com/sites/niallmccarthy/2016/03/31/americas-most-prestigious-professions-in-2016-infographic/#5b5d55b91926 (accessed on 25 June 2020).
- Kuisma, M.; Maatta, T.; Hakala, T.; Sivula, T.; Nousila-Wiik, M. Customer Satisfaction Measurement in Emergency Medical Services. Acad. Emerg. Med. 2003, 10, 812–815. [Google Scholar] [CrossRef] [PubMed]
- Crowe, R.P.; Levine, R.; Rodriguez, S.; Larrimore, A.D.; Pirrallo, R.G. Public Perception of Emergency Medical Services in the United States. Prehosp. Disaster Med. 2016, 31, 112–117. [Google Scholar] [CrossRef]
- Bernard, A.W.; Lindsell, C.J.; Handel, D.A.; Collett, L.; Gallo, P.; Kaiser, K.D.; Locasto, D. Postal survey methodology to assess patient satisfaction in a suburban emergency medical services system: An observational study. BMC Emerg. Med. 2007, 7, 5. [Google Scholar] [CrossRef] [PubMed]
- Halter, M.; Marlow, T.; Tye, C.; Ellison, G.T.H. Patients’ experiences of care provided by emergency care practitioners and traditional ambulance practitioners: A survey from the London Ambulance Service. Emerg. Med. J. 2006, 23, 865–866. [Google Scholar] [CrossRef]
- Murcot, P.; Williams, B.; Morgans, A.; Boyle, M. Community perceptions of the professional status of the paramedic discipline. Int. Paramed. Pr. 2014, 4, 13–18. [Google Scholar] [CrossRef]
- Perry, M.; Usher, K.; Jackson, D. Global patient experience of paramedic practice. Int. Paramed. Pract. 2019, 9, 3–12. [Google Scholar] [CrossRef]
- Statistics Poland. First aid and Emergency Medical Services in 2019. 26.05.2020 r. Available online: https://stat.gov.pl/en/topics/health/health/first-aid-and-emergency-medical-services-in-2019,7,4.html (accessed on 29 December 2020).
- Dopelt, K.; Wacht, O.; Strugo, R.; Miller, R.; Kushnir, T. Factors that affect Israeli paramedics’ decision to quit the profession: A mixed methods study. Isr. J. Health Policy Res. 2019, 8, 78. [Google Scholar] [CrossRef]
- Regehr, C.; Millar, D. Situation Critical: High Demand, Low Control, and Low Support in Paramedic Organizations. Traumatology 2007, 13, 49–58. [Google Scholar] [CrossRef]
- Grisby, D.W.; McKnew, M.A. Work-stress burnout among paramedics. Psychol. Rep. 1988, 63, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Omyła-Rudzka, M. What Professions Do We Respect? Public Opinion Research Centre: Warsaw, Poland, 2019; Available online: https://www.cbos.pl/SPISKOM.POL/2019/K_157_19.PDF (accessed on 10 September 2020).
- Cybulska, A. Occupational Prestige; Public Opinion Research Centre: Warsaw, Poland, 2013; Available online: https://www.cbos.pl/SPISKOM.POL/2013/K_164_13.PDF (accessed on 10 September 2020).
- Communication of the Head of Statistics Poland for Q2 2019. Available online: http://isap.sejm.gov.pl/isap.nsf/download.xsp/WMP20200000711/O/M20200711.pdf (accessed on 10 September 2020).



{kind=link}
{kind=link}
| Feature | Demographic Variables | N | % |
|---|---|---|---|
| Gender | Women | 306 | 51.0% |
| Men | 294 | 49.0% | |
| Age | ≤29 | 106 | 17.7% |
| 30–39 | 126 | 21.0% | |
| 40–49 | 102 | 17.0% | |
| 50–59 | 98 | 16.3% | |
| 60+ | 168 | 28.0% | |
| Education | Primary | 13 | 2.2% |
| Basic vocational | 116 | 19.3% | |
| Secondary | 212 | 35.3% | |
| Bachelor’s degree | 131 | 21.8% | |
| Master’s degree | 128 | 21.3% | |
| Place of residence | Village | 33 | 5.5% |
| Town with a population of up to 20,000 | 60 | 10.0% | |
| City with a population of between 20,000 and 100,000 | 228 | 38.0% | |
| City with a population of between 100,000 and 500,000 | 225 | 37.5% | |
| City with a population of 500,000 or more | 54 | 9.0% | |
| Self-assessment of health | Very good | 144 | 24.0% |
| Good | 372 | 62.0% | |
| Average | 76 | 12.7% | |
| Poor | 8 | 1.3% | |
| Assessment of material circumstances | Very good | 68 | 11.3% |
| Good | 359 | 59.8% | |
| Average | 166 | 27.7% | |
| Poor | 7 | 1.2% |
| Median | Respect for the Paramedic | Respect for the Paramedic among Medical Profession | |
|---|---|---|---|
| Respect for paramedics | 4.49 | ||
| Respect for paramedics among the medical profession | 4.60 | 0.596 ** | |
| Age | 44.58 | 0.028 | 0.012 |
| Education | 3.38 | 0.051 | −0.035 |
| Place of residence | 3.41 | 0.095 * | 0.070 |
| Self-assessment of health | 4.12 | −0.003 | 0.030 |
| Assessment of material conditions | 3.80 | 0.223 ** | 0.232 ** |
| Assessment of paramedics’ income | 3.47 | 0.248 ** | 0.217 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Majchrowska, A.; Pawlikowski, J.; Jojczuk, M.; Nogalski, A.; Bogusz, R.; Nowakowska, L.; Wiechetek, M. Social Prestige of the Paramedic Profession. Int. J. Environ. Res. Public Health 2021, 18, 1506. https://doi.org/10.3390/ijerph18041506
Majchrowska A, Pawlikowski J, Jojczuk M, Nogalski A, Bogusz R, Nowakowska L, Wiechetek M. Social Prestige of the Paramedic Profession. International Journal of Environmental Research and Public Health. 2021; 18(4):1506. https://doi.org/10.3390/ijerph18041506
Chicago/Turabian StyleMajchrowska, Anita, Jakub Pawlikowski, Mariusz Jojczuk, Adam Nogalski, Renata Bogusz, Luiza Nowakowska, and Michał Wiechetek. 2021. "Social Prestige of the Paramedic Profession" International Journal of Environmental Research and Public Health 18, no. 4: 1506. https://doi.org/10.3390/ijerph18041506
APA StyleMajchrowska, A., Pawlikowski, J., Jojczuk, M., Nogalski, A., Bogusz, R., Nowakowska, L., & Wiechetek, M. (2021). Social Prestige of the Paramedic Profession. International Journal of Environmental Research and Public Health, 18(4), 1506. https://doi.org/10.3390/ijerph18041506