
Obturator Prosthesis Rehabilitation after Maxillectomy: Functional and Aesthetical Analysis in 25 Patients

 ,
, 
 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
- Time 0: alginate impression to manufacture a pre-surgical obturator in thermoplastic resin;
- Time 1: surgical resection and contextual pre-surgical obturator positioning filled with periodontal dressing (Coepack); in the post-operative course, the obturator was continuously dressed to guide wound healing and exclusively removed for the removal of stiches;
- Time 2: alginate impression to fabricate a new “ad interim” obturator, with a false palate and false ridge and no retention on teeth but filling the defect;
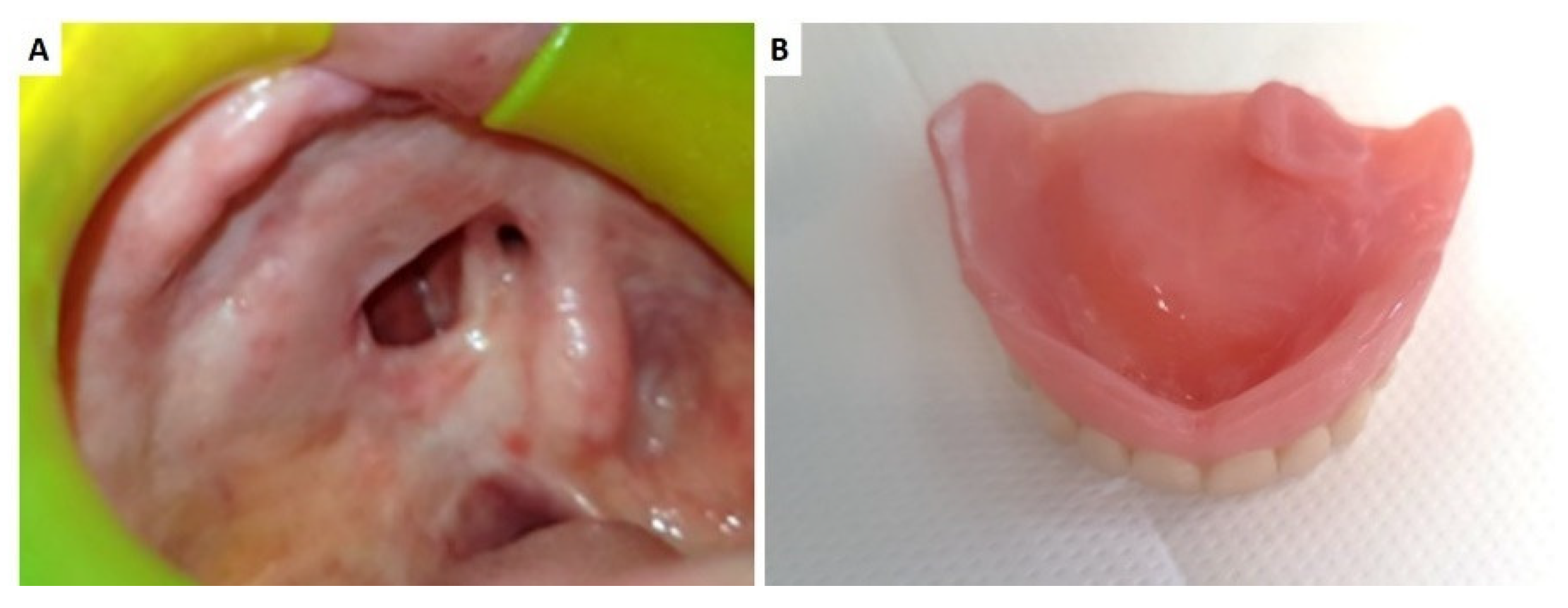
- Time 3: at the time of complete wound healing and defect dimension stability, the silicon was impressed to fabricate the definitive obturator (Figure 1).
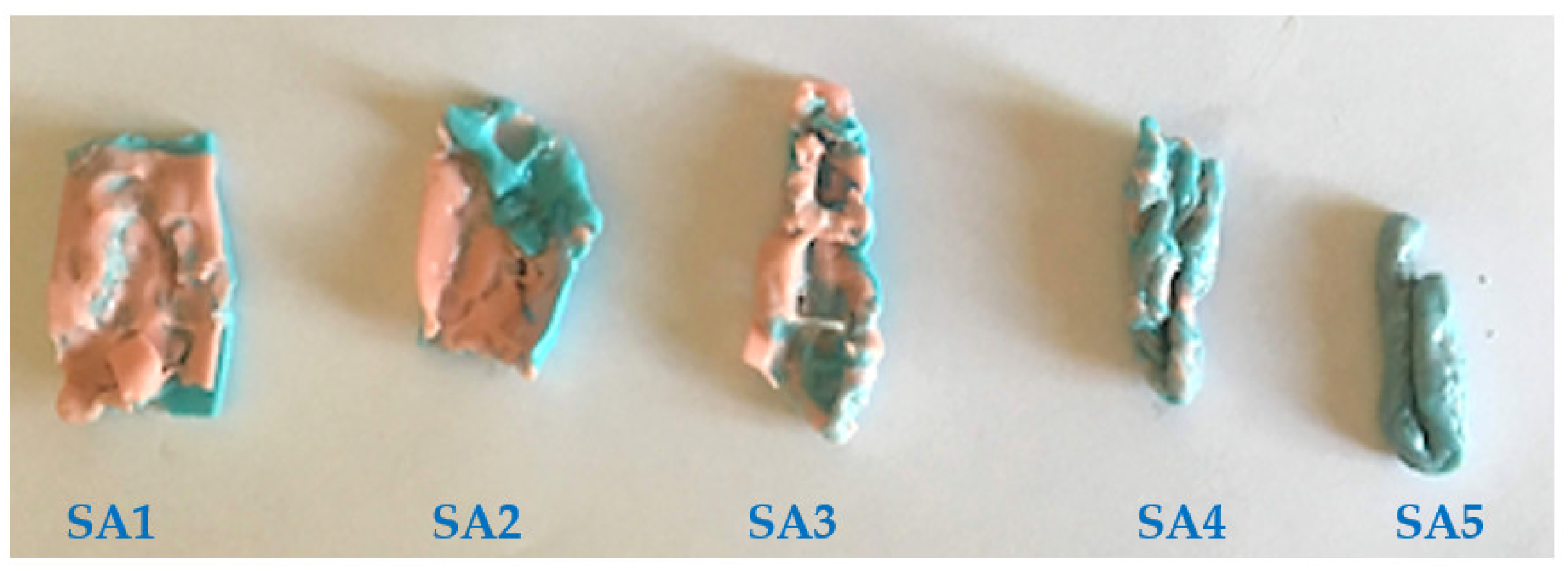
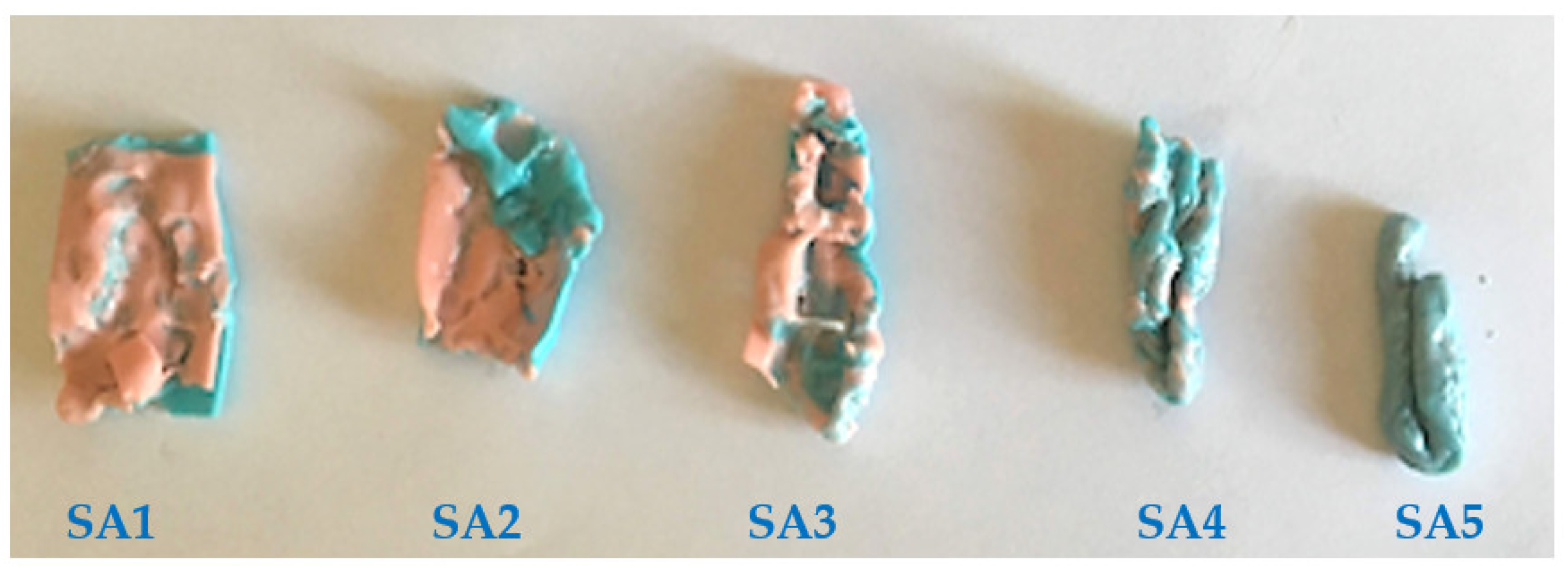
- SA1: double-layer colors were not mixed; only teeth cusps’ impressions were observable;
- SA2: Most of the double-layer colors was not mixed;
- SA3: A large part of the double-layer colors was mixed;
- SA4: The mixing of colors was observable in the whole sample but not uniform;
- SA5: The color distribution was perfectly uniform.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mirna, G.; Lokanath, G.; Aswini, K.K.; Chittaranjan, B. Prosthetic rehabilitation of a unilateral maxillary defect with an intermediate obturator. Indian J. Dent. Adv. 2010, 2, 378–383. [Google Scholar]
- Capodiferro, S.; Favia, G.; Lacaita, M.; Muzio, L.L.; Favia, G. Juvenile angiofibroma: Report of a case with primary intra-oral presentation. Oral Oncol. Extra 2005, 41, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Limongelli, L.; Cascardi, E.; Capodiferro, S.; Favia, G.; Corsalini, M.; Tempesta, A.; Maiorano, E. Multifocal amelanotic melanoma of the hard palate: A challenging case. Diagnostics 2020, 10, 424. [Google Scholar] [CrossRef]
- Capodiferro, S.; Calabrese, L.; Maffini, F.; Cascardi, E.; Favia, G.; Maiorano, E. Dentinogenic ghost cell tumour in a 20-year-old male with previous squamous cell carcinoma of the tongue. J. Biol. Regul. Homeost. Agents 2019, 33, 269–273. [Google Scholar]
- Limongelli, L.; Capodiferro, S.; Tempesta, A.; Sportelli, P.; Dell’Olio, F.; Angelelli, G.; Maiorano, E.; Favia, G. Early tongue carcinomas (clinical stage I and II): Echo-guided three-dimensional diode laser mini-invasive surgery with evaluation of histological prognostic parameters. A study of 85 cases with prolonged follow-up. Lasers Med. Sci. 2020, 35, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Maiorano, E.; Favia, G.; Capodiferro, S.; Montagna, M.T.; Lo Muzio, L. Combined mucormycosis and aspergillosis of the oro-sinonasal region in a patient affected by Castleman disease. Virchows Arch. 2005, 446, 28–33. [Google Scholar] [CrossRef] [PubMed]
- Tempesta, A.; Capodiferro, S.; Mauceri, R.; Lauritano, D.; Maiorano, E.; Favia, G.; Limongelli, L. Peri-implantitis-like medication-related osteonecrosis of the jaw: Clinical considerations and histological evaluation with confocal laser scanning microscope. Oral Dis. 2021. [Google Scholar] [CrossRef]
- Di Cosola, M.; Turco, M.; Bizzoca, G.; Tavoulari, K.; Capodiferro, S.; Escudero-Castaño, N.; Muzio, L. Ameloblastoma of the maxillar and mandibular bones: An evidence-based clinical study. Av. Odontoestomatol. 2007, 23, 359–365. [Google Scholar]
- Favia, G.; Maiorano, E.; Capodiferro, S.; Pilolli, G.P.; Lacaita, M.G.; Lajolo, C.; Giuliani, M.; Martinelli, D.; Germinario, C. Oral squamous cell carcinoma: A mono-institutional epidemiological study on 462 cases highlighting differences among young and adult patients. Minerva Stomatol. 2008, 57, 413–421. [Google Scholar] [PubMed]
- Van Dijk, B.A.C.; Gatta, G.; Capocaccia, R.; Pierannunzio, D.; Strojan, P.; Licitra, L. Rare cancers of the head and neck area in Europe. Eur. J. Cancer 2012, 48, 783–796. [Google Scholar] [CrossRef]
- Ellis, G.L.; Auclair, P.L. Tumors of the Salivary Glands, Atlas of Tumor Pathology: Third Series, Fascicle 17; American Registry of Pathology Press: Arlington, VA, USA, 1996. [Google Scholar]
- Eneroth, C.M. Incidence and prognosis of salivary-gland tumours at different sites. A study of parotid, submandibular and palatal tumours in 2632 patients. Acta Otolaryngol. Suppl. 1969, 263, 174–178. [Google Scholar]
- de Carvalho-Teles, V.; Pegoraro-Krook, M.I.; Lauris, J.R.P. Speech evaluation with and without palatal obturator in patients submitted to maxillectomy. J. Appl. Oral Sci. 2006, 14, 421–426. [Google Scholar] [CrossRef] [Green Version]
- Aramany, M.A. Basic principles of obturator design for partially edentulous patients. Part I: Classification. J. Prosthet. Dent. 1978, 40, 554–557. [Google Scholar] [CrossRef]
- Aramany, M.A. Basic principles of obturator design for partially edentulous patients. Part II: Design principles. J. Prosthet. Dent. 1978, 40, 656–662. [Google Scholar] [CrossRef]
- Ali, M.M.; Khalifa, N.; Alhajj, M.N. Quality of life and problems associated with obturators of patients with maxillectomies. Head Face Med. 2018, 14, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Artopoulou, I.; Karademas, E.C.; Papadogeorgakis, N.; Papathanasiou, I.; Polyzois, G. Effects of sociodemographic, treatment variables, and medical characteristics on quality of life of patients with maxillectomy restored with obturator prostheses. J. Prosthet. Dent. 2017, 118, 783–789. [Google Scholar] [CrossRef]
- Ferro, K.J.; Morgano, S.M.; Driscoll, C.F.; Freilich, M.A.; Guckes, A.D.; Knoernschild, K.L.; McGarry, T.J.; Twain, M. The Glossary of Prosthodontic Terms: Ninth Edition. J. Prosthet. Dent. 2017, 117, e1–e105. [Google Scholar] [CrossRef] [Green Version]
- Depprich, R.; Naujoks, C.; Lind, D.; Ommerborn, M.; Meyer, U.; Kübler, N.R.; Handschel, J. Evaluation of the quality of life of patients with maxillofacial defects after prosthodontic therapy with obturator prostheses. Int. J. Oral Maxillofac. Surg. 2011, 40, 71–79. [Google Scholar] [CrossRef]
- Hanawa, S.; Kitaoka, A.; Koyama, S.; Sasaki, K. Influence of maxillary obturator prostheses on facial morphology in patients with unilateral maxillary defects. J. Prosthet. Dent. 2015, 113, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Rieger, J.M.; Tang, J.A.L.; Wolfaardt, J.; Harris, J.; Seikaly, H. Comparison of speech and aesthetic outcomes in patients with maxillary reconstruction versus maxillary obturators after maxillectomy. J. Otolaryngol. Head Neck Surg. 2011, 40, 40–47. [Google Scholar]
- Irish, J.; Sandhu, N.; Simpson, C.; Wood, R.; Gilbert, R.; Gullane, P.; Brown, D.; Goldstein, D.; Devins, G.; Barker, E. Quality of life in patients with maxillectomy prostheses. Head Neck 2009, 31, 813–821. [Google Scholar] [CrossRef]
- Ortholan, C.; Benezery, K.; Dassonville, O.; Poissonnet, G.; Bozec, A.; Guiochet, N.; Belkacemi, Y. A specific approach for elderly patients with head and neck cancer. Anticancer Drugs 2011, 22, 647–655. [Google Scholar] [CrossRef]
- Moreno, M.A.; Skoracki, R.J.; Hanna, E.Y.; Hanasono, M.M. Microvascular free flap reconstruction versus palatal obturation for maxillectomy defects. Head Neck 2010, 32, 860–868. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Luthra, R.; Gupta, S. Evaluation of quality of life of maxillectomy patients after prosthetic obturator rehabilitation. Int. Dent. Med. J. Adv. Res. 2016, 2, 1–4. [Google Scholar] [CrossRef]
- Desjardins, R.P. Obturator prosthesis design for acquired maxillary defects. J. Prosthet. Dent. 1978, 39, 424–435. [Google Scholar] [CrossRef]
- Keyf, F. Obturator prostheses for hemimaxillectomy patients. J. Oral Rehabil. 2001, 28, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Huryn, J.M.; Piro, J.D. The maxillary immediate surgical obturator prosthesis. J. Prosthet. Dent. 1989, 61, 343–347. [Google Scholar] [CrossRef]
- Kar, S.; Tripathi, A. Treatment outcome with delayed maxillary obturator prosthesis: Case series of four patients. J. Prosthodont. 2016, 25, 174–177. [Google Scholar] [CrossRef]
- Tripathi, A.; Gupta, A.; Arora, V. Effect of prosthodontic rehabilitation of maxillary defects on hypernasality of speech. J. Prosthodont. 2016, 25, 202–206. [Google Scholar] [CrossRef]
- Brandão, T.B.; Vechiato Filho, A.J.; de Batista, S.; de Oliveira, M.C.Q.; Santos-Silva, A.R. Obturator prostheses versus free tissue transfers: A systematic review of the optimal approach to improving the quality of life for patients with maxillary defects. J. Prosthet. Dent. 2016, 115, 247–253. [Google Scholar] [CrossRef]
- Umino, S.; Masuda, G.; Ono, S.; Fujita, K. Speech intelligibility following maxillectomy with and without a prosthesis: An analysis of 54 cases. J. Oral Rehabil. 1998, 25, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Parr, G.R.; Tharp, G.E.; Rahn, A.O. Prosthodontic principles in the framework design of maxillary obturator prostheses. J. Prosthet. Dent. 1989, 62, 205–212. [Google Scholar] [CrossRef]
- Kumar, P.; Alvi, H.A.; Rao, J.; Singh, B.P.; Jurel, S.K.; Kumar, L.; Aggarwal, H. Assessment of the quality of life in maxillectomy patients: A longitudinal study. J. Adv. Prosthodont. 2013, 5, 29–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arigbede, A.O.; Dosumu, O.O.; Shaba, O.P.; Esan, T.A. Evaluation of speech in patients with partial surgically acquired defects: Pre and post prosthetic obturation. J. Contemp. Dent. Pract. 2006, 7, 89–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kornblith, A.B.; Zlotolow, I.M.; Gooen, J.; Huryn, J.M.; Lerner, T.; Strong, E.W.; Shah, J.P.; Spiro, R.H.; Holland, J.C. Quality of life of maxillectomy patients using an obturator prosthesis. Head Neck 1996, 18, 323–334. [Google Scholar] [CrossRef]
- Rogers, S.N.; Lowe, D.; McNally, D.; Brown, J.S.; Vaughan, E.D. Health-related quality of life after maxillectomy: A comparison between prosthetic obturation and free flap. J. Oral Maxillofac. Surg. 2003, 61, 174–181. [Google Scholar] [CrossRef]
- Seignemartin, C.P.; Miranda, M.E.; Luz, J.G.C.; Teixeira, R.G. Understandability of speech predicts quality of life among maxillectomy patients restored with obturator prosthesis. J. Oral Maxillofac. Surg. 2015, 73, 2040–2048. [Google Scholar] [CrossRef] [Green Version]
- Hertrampf, K.; Wenz, H.J.; Lehmann, K.M.; Lorenz, W.; Koller, M. Quality of life of patients with maxillofacial defects after treatment for malignancy. Int. J. Prosthodont. 2004, 17, 657–665. [Google Scholar]
- Kaya, M.S.; Güçlü, B.; Schimmel, M.; Akyüz, S. Two-colour chewing gum mixing ability test for evaluating masticatory performance in children with mixed dentition: Validity and reliability study. J. Oral Rehabil. 2017, 44, 827–834. [Google Scholar] [CrossRef] [PubMed]
- Schimmel, M.; Christou, P.; Miyazaki, H.; Halazonetis, D.; Herrmann, F.R.; Müller, F. A novel colourimetric technique to assess chewing function using two-coloured specimens: Validation and application. J. Dent. 2015, 43, 955–964. [Google Scholar] [CrossRef]
- van der Bilt, A.; Mojet, J.; Tekamp, F.A.; Abbink, J.H. Comparing masticatory performance and mixing ability. J. Oral. Rehabil. 2010, 37, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, D.V.; Toljanic, J.A.; Graham, L. Obturator prosthesis retention for edentulous patients with large palatal defects: A clinical report. J. Prosthet. Dent. 1996, 76, 227–229. [Google Scholar] [CrossRef]
- Favia, G.; Corsalini, M.; Di Venere, D.; Pettini, F.; Favia, G.; Capodiferro, S.; Maiorano, E. Immunohistochemical evaluation of neuroreceptors in healthy and pathological temporo-mandibular joint. Int. J. Med. Sci. 2013, 10, 1698–1701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koyama, S.; Sasaki, K.; Inai, T.; Watanabe, M. Effects of defect configuration, size, and remaining teeth on masticatory function in post-maxillectomy patients. J. Oral Rehabil. 2005, 32, 635–641. [Google Scholar] [CrossRef]
- Kapur, K.K. A clinical evaluation of denture adhesives. J. Prosthet. Dent. 1967, 18, 550–558. [Google Scholar] [CrossRef]
- Corsalini, M.; Di Venere, D.; Sportelli, P.; Magazzino, D.; Ripa, C.; Cantatore, F.; Cagnetta, G.; de Rinaldis, C.; Montemurro, N.; de Giacomo, A.; et al. Evaluation of prosthetic quality and masticatory efficiency in patients with total removable prosthesis study of 12 cases. Oral Implantol. 2018, 11, 230–240. [Google Scholar]
- Corsalini, M.; Di Venere, D.; Stefanachi, G.; Muci, G.; Palminteri, A.; Laforgia, A.; Pettini, F. Maxillary overdenture retained with an implant support CAD-CAM bar: A 4 years follow up case. Open Dent. J. 2017, 11, 247–256. [Google Scholar] [CrossRef] [Green Version]
- Kreeft, A.M.; Krap, M.; Wismeijer, D.; Speksnijder, C.M.; Smeele, L.E.; Bosch, S.D.; Muijen, M.S.; Balm, A.J. Oral function after maxillectomy and reconstruction with an obturator. Int. J. Oral Maxillofac. Surg. 2012, 41, 1387–1392. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Patient | Sex | Age | Aramany | Dentition | Oral Hygiene | Smoking Habits | Alcohol Habits | Subjective Evaluation | Subjective Function Evaluation | SA Score | Quality of Life |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 67 | I | D | G | Until Cancer | Never | High | 3 | 3 | Satisfactory |
| 2 | M | 54 | I | E | G | Yes | Significant | Low | 0 | 2 | Good |
| 3 | M | 62 | III | D | B | Until Cancer | Never | High | 1 | 4 | Good |
| 4 | F | 73 | I | D | B | Until Cancer | Never | High | 2 | 4 | Satisfactory |
| 5 | F | 48 | VI | E | G | Until Cancer | Never | Low | 0 | 2 | Good |
| 6 | M | 65 | I | D | B | Yes | Occasionally | High | 2 | 3 | Good |
| 7 | F | 59 | IV | E | G | Until Cancer | Occasionally | Low | 0 | 2 | Good |
| 8 | M | 68 | I | E | G | Until Cancer | Never | Low | 0 | 1 | Very Low |
| 9 | F | 63 | III | D | B | Never | Never | High | 3 | 3 | Satisfactory |
| 10 | M | 73 | III | D | B | Until Cancer | Never | High | 1 | 4 | Good |
| 11 | M | 79 | IV | E | G | Never | Never | High | 3 | 4 | Satisfactory |
| 12 | F | 60 | I | E | G | Until Cancer | Occasionally | High | 1 | 3 | Good |
| 13 | F | 55 | IV | E | G | Yes | Significant | Low | 1 | 2 | Bad |
| 14 | M | 64 | I | E | G | Until Cancer | Never | High | 3 | 4 | Excellent |
| 15 | F | 72 | I | D | B | Never | Never | High | 1 | 3 | Good |
| 16 | M | 57 | IV | E | G | Until Cancer | Occasionally | High | 2 | 4 | Satisfactory |
| 17 | F | 66 | VI | E | G | Never | Never | Low | 1 | 2 | Bad |
| 18 | F | 61 | I | D | B | Never | Occasionally | High | 2 | 3 | Satisfactory |
| 19 | M | 60 | VI | E | G | Yes | Never | High | 1 | 4 | Satisfactory |
| 20 | M | 71 | III | D | B | Until Cancer | Never | High | 1 | 4 | Satisfactory |
| 21 | F | 68 | I | D | B | Until Cancer | Significant | High | 4 | 4 | Excellent |
| 22 | M | 56 | IV | E | G | Never | Never | Low | 0 | 2 | Bad |
| 23 | F | 59 | IV | E | G | Until Cancer | Occasionally | High | 4 | 4 | Excellent |
| 24 | M | 66 | VI | E | G | Until Cancer | Occasionally | High | 4 | 3 | Excellent |
| 25 | M | 62 | I | E | G | Never | Never | High | 1 | 3 | Good |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Corsalini, M.; Barile, G.; Catapano, S.; Ciocia, A.; Casorelli, A.; Siciliani, R.; Di Venere, D.; Capodiferro, S. Obturator Prosthesis Rehabilitation after Maxillectomy: Functional and Aesthetical Analysis in 25 Patients. Int. J. Environ. Res. Public Health 2021, 18, 12524. https://doi.org/10.3390/ijerph182312524
Corsalini M, Barile G, Catapano S, Ciocia A, Casorelli A, Siciliani R, Di Venere D, Capodiferro S. Obturator Prosthesis Rehabilitation after Maxillectomy: Functional and Aesthetical Analysis in 25 Patients. International Journal of Environmental Research and Public Health. 2021; 18(23):12524. https://doi.org/10.3390/ijerph182312524
Chicago/Turabian StyleCorsalini, Massimo, Giuseppe Barile, Santo Catapano, Annamaria Ciocia, Assunta Casorelli, Rosaria Siciliani, Daniela Di Venere, and Saverio Capodiferro. 2021. "Obturator Prosthesis Rehabilitation after Maxillectomy: Functional and Aesthetical Analysis in 25 Patients" International Journal of Environmental Research and Public Health 18, no. 23: 12524. https://doi.org/10.3390/ijerph182312524
APA StyleCorsalini, M., Barile, G., Catapano, S., Ciocia, A., Casorelli, A., Siciliani, R., Di Venere, D., & Capodiferro, S. (2021). Obturator Prosthesis Rehabilitation after Maxillectomy: Functional and Aesthetical Analysis in 25 Patients. International Journal of Environmental Research and Public Health, 18(23), 12524. https://doi.org/10.3390/ijerph182312524