
A Qualitative Study Exploring the Management of Medicine Shortages in the Community Pharmacy of Pakistan

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
2.3. Interview Guide Development
2.4. Participant Enrollment
2.5. Qualitative Analysis
2.6. Reporting
2.7. Ethical Permission
3. Results
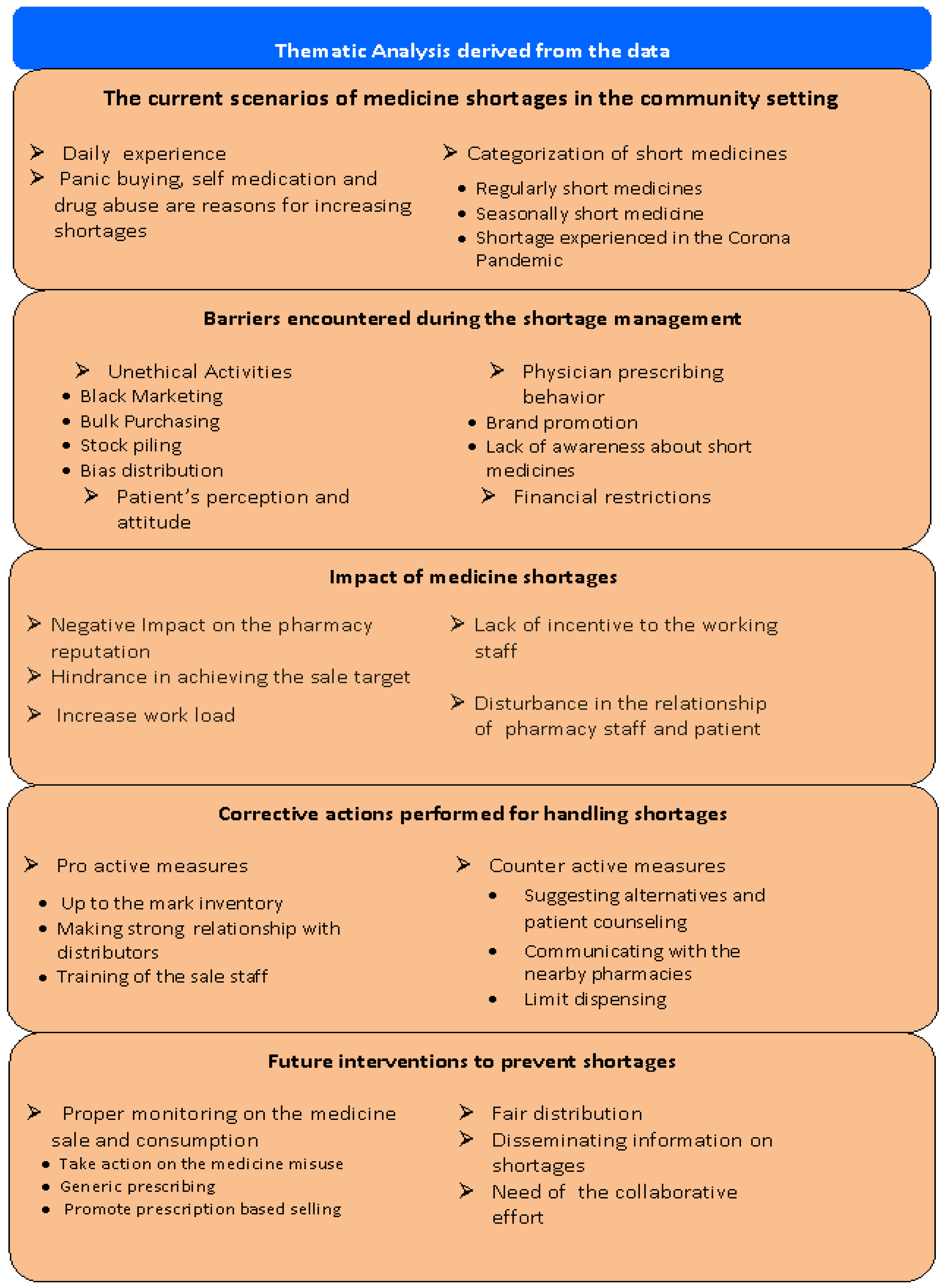
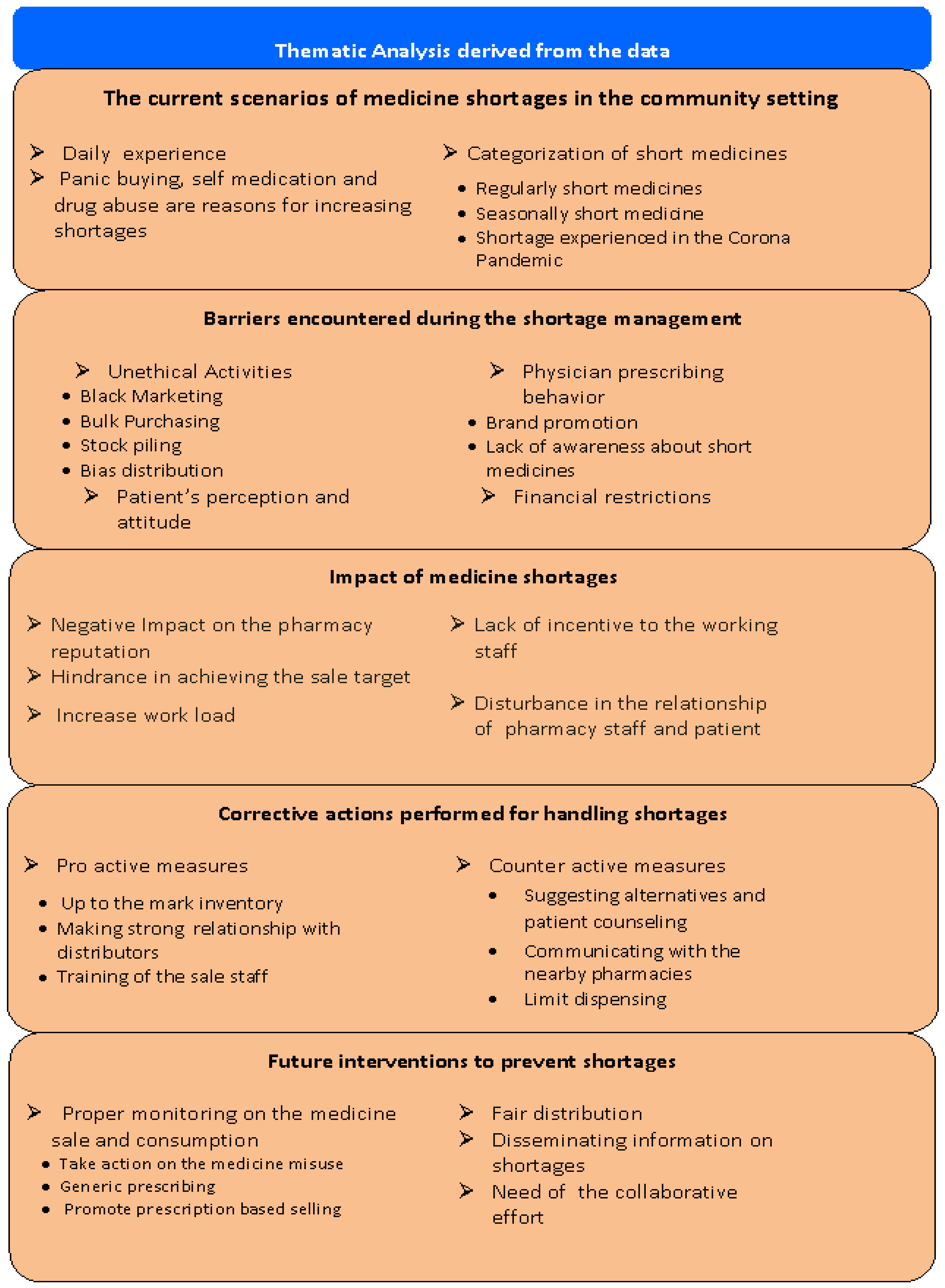
3.1. Theme 1: The Current Scenarios of Medicine Shortages in the Community Setting
3.2. Theme 2: Barriers Encountered during the Shortage Management
3.3. Theme 3: Impact of Medicine Shortages
3.4. Theme 4: Corrective Actions Performed for Handling Shortages
3.5. Theme 5: Future Interventions to Prevent Shortages
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- De Oliveira, G.S., Jr.; Theilken, L.S.; McCarthy, R.J. Shortage of perioperative drugs: Implications for anesthesia practice and patient safety. Anesth. Analg. 2011, 113, 1429–1435. [Google Scholar] [CrossRef]
- World Health Organization. Access to Medicines: Making Market Forces Serve the Poor. 2017. Available online: https://www.who.int/publications/10-year-review/chapter-medicines.pdf (accessed on 19 June 2021).
- Association, C.P. Canadian Drug Shortages Survey: Final Report. 2010. Available online: http://www.pharmacists.ca/cpha-ca/assets/File/cpha-on-the-issues/DrugShortagesReport.pdf (accessed on 19 June 2021).
- Heiskanen, K.; Ahonen, R.; Karttunen, P.; Kanerva, R.; Timonen, J. Medicine shortages–a study of community pharmacies in Finland. Health Policy 2015, 119, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Costelloe, E.; Guinane, M.; Nugent, F.; Halley, O.; Parsons, C. An audit of drug shortages in a community pharmacy practice. Irish J. Med. Sci. 2015, 184, 435–440. [Google Scholar] [CrossRef]
- AESGP; EAHP; EAEPC; EFPIA; EIPG; GIRP; Medicines for Europe; PGEU. Joint Supply Chain Actors Statement on Information and Medicinal Products Shortages. 2 February 2017. Available online: https://www.efpia.eu/media/25913/joint_supply_chain_actors_statement_on_information_and_medicinal_products_shortages.pdf (accessed on 23 September 2021).
- Zaidi, S.; Nishtar, N. Access to Essential Medicines: In Pakistan Identifying Policy Research and Concerns. 2011. Available online: https://ecommons.aku.edu/cgi/viewcontent.cgi?referer=https://scholar.google.co.uk/&httpsredir=1&article=1189&context=pakistan_fhs_mc_chs_chs (accessed on 27 September 2021).
- Kiani, A.; Qadeer, A.; Mirza, Z.; Khanum, A.; Tisocki, K.; Mustafa, T. Prices, Availability and Affordability of Medicines in Pakistan. Geneva: Health Action International. 2006. Available online: http://www.haiweb.org/medicineprices/surveys/200407PK/survey_report.pdf (accessed on 19 June 2021).
- Qidwai, W.; Krishanani, M.K.; Hashmi, S.; Abu Ali, R. Private drug sellers education in improving prescribing practices. J. Coll. Physicians Surg. Pak. 2006, 16, 743. [Google Scholar] [PubMed]
- Hussain, A.; Malik, M.; Toklu, H.Z. A literature review: Pharmaceutical care an evolving role at community pharmacies in Pakistan. Pharmacol. Pharm. 2013, 2013. [Google Scholar] [CrossRef] [Green Version]
- Atif, M.; Malik, I.; Mushtaq, I.; Asghar, S. Medicines shortages in Pakistan: A qualitative study to explore current situation, reasons and possible solutions to overcome the barriers. BMJ Open 2019, 9, e027028. [Google Scholar] [CrossRef] [PubMed]
- Dawani, K.; Sayeed, A. Pakistan’s Pharmaceutical Sector: Issues of Pricing, Procurement and the Quality of Medicines; SOAS ACE Working Papers: London, UK, 2019. [Google Scholar]
- DAWN. Medcines Being Sold in Black Market. Available online: https://www.dawn.com/news/1057502 (accessed on 23 September 2021).
- Pauwels, K.; Huys, I.; Casteels, M.; Simoens, S. Drug shortages in European countries: A trade-off between market attractiveness and cost containment? BMC Health Serv. Res. 2014, 14, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Said, A.; Goebel, R.; Ganso, M.; Zagermann-Muncke, P.; Schulz, M. Drug shortages may compromise patient safety: Results of a survey of the reference pharmacies of the Drug Commission of German Pharmacists. Health Policy 2018, 122, 1302–1309. [Google Scholar] [CrossRef]
- Kitzinger, J. Qualitative research: Introducing focus groups. BMJ 1995, 311, 299–302. [Google Scholar] [CrossRef] [Green Version]
- Berg, B.L.; Lune, H. Qualitative Research Methods for the Social Sciences; Pearson Education, Inc.: Boston, MA, USA, 2009. [Google Scholar]
- PAKISTAN: Provinces and Major Cities. Available online: https://www.citypopulation.de/en/pakistan/cities/ (accessed on 6 June 2021).
- Panic, G.; Yao, X.; Gregory, P.; Austin, Z. How do community pharmacies in Ontario manage drug shortage problems? Results of an exploratory qualitative study. Can. Pharm. J./Rev. Pharm. Can. 2020, 153, 371–377. [Google Scholar] [CrossRef]
- Hashmi, F.K.; Hassali, M.A.; Khalid, A.; Saleem, F.; Aljadhey, H.; Bashaar, M. A qualitative study exploring perceptions and attitudes of community pharmacists about extended pharmacy services in Lahore, Pakistan. BMC Health Serv. Res. 2017, 17, 1–9. [Google Scholar] [CrossRef]
- Pandey, M.; Pandey, P. Better English for better employment opportunities. Int. J. Multidiscip. Approach Stud. 2014, 1, 93–100. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Walker, J.; Chaar, B.B.; Vera, N.; Pillai, A.S.; Lim, J.S.; Bero, L.; Moles, R.J. Medicine shortages in Fiji: A qualitative exploration of stakeholders’ views. PLoS ONE 2017, 12, e0178429. [Google Scholar] [CrossRef] [Green Version]
- Chen, E.; Goold, S.; Harrison, S.; Ali, I.; Makki, I.; Kent, S.S.; Shuman, A.G. Drug shortage management: A qualitative assessment of a collaborative approach. PLoS ONE 2021, 16, e0243870. [Google Scholar]
- Al-Ruthia, Y.S.; Mansy, W.; Barasin, M.; Ghawaa, Y.M.; AlSultan, M.; Alsenaidy, M.A.; Alhawas, S.; AlGhadeer, S. Shortage of psychotropic medications in community pharmacies in Saudi Arabia: Causes and solutions. Saudi Pharm. J. 2017, 25, 744–749. [Google Scholar] [CrossRef] [Green Version]
- Makowska, M. Polish physicians’ cooperation with the pharmaceutical industry and its potential impact on public health. PLoS ONE 2017, 12, e0184862. [Google Scholar] [CrossRef] [Green Version]
- Mansoor, H. The Politics of Medicine Pricing. Available online: https://www.dawn.com/news/1289752 (accessed on 19 July 2021).
- Cherici, C.; McGinnis, P.; Russell, W. Buyer Beware: Drug Shortages and the Gray Market. Charlotte (NC) Premier Healthcare Alliance. 2011. Available online: https://nebula.wsimg.com/d3a344fdd23eb3bb66bb8aa740c5e417?AccessKeyId=62BC662C928C06F7384C&disposition=0&alloworigin=1 (accessed on 19 June 2021).
- Tan, Y.X.; Moles, R.J.; Chaar, B.B. Medicine shortages in Australia: Causes, impact and management strategies in the community setting. Int. J. Clin. Pharm. 2016, 38, 1133–1141. [Google Scholar] [CrossRef]
- De Weerdt, E.; Simoens, S.; Casteels, M.; Huys, I. Time investment in drug supply problems by flemish community pharmacies. Front. Pharmacol. 2017, 8, 568. [Google Scholar] [CrossRef] [Green Version]
- Fox, E.R.; Birt, A.; James, K.B.; Kokko, H.; Salverson, S.; Soflin, D.L. ASHP guidelines on managing drug product shortages in hospitals and health systems. Am. J. Health-Syst. Pharm. 2009, 66, 1399–1406. [Google Scholar] [CrossRef] [PubMed]
- Johnson, L. Associated Press. Drug Shortage Stirs Fear. Available online: https://www.inquirer.com/philly/business/20110924_Drug_shortage_stirs_fears.html (accessed on 27 September 2021).
- Azhar, S.; Hassali, M.; Ibrahim, M. Doctors’ perception and expectations of the role of the pharmacist in Punjab, Pakistan. Trop. J. Pharm. Res. 2010, 9, 3. [Google Scholar] [CrossRef] [Green Version]
- Steeb, D.R.; Ramaswamy, R. Recognizing and engaging pharmacists in global public health in limited resource settings. J. Glob. Health 2019, 9, 010318. [Google Scholar] [CrossRef] [PubMed]
- Ammar, M.A.; Tran, L.J.; McGill, B.; Ammar, A.A.; Huynh, P.; Amin, N.; Guerra, M.; Rouse, G.E.; Lemieux, D.; McManus, D. Pharmacists leadership in a medication shortage response: Illustrative examples from a health system response to the COVID-19 crisis. J. Am. Coll. Clin. Pharm. 2021, 4, 1134–1143. [Google Scholar] [CrossRef] [PubMed]
- Shuman, A.G.; Fox, E.R.; Unguru, Y. COVID-19 and drug shortages: A call to action. J. Manag. Care Spec. Pharm. 2020, 26, 945–947. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Participants’ Recruitment | Number = (n) |
|---|---|
| Participants approached | 90 |
| Participants selected based on the inclusion criteria | 51 |
| Refused due to specific reason | 18 |
| Agreed for participation | 33 |
| Final participants at saturation | 31 |
| Demographic | Interviewees |
|---|---|
| Sex (n, %) | |
| Male | 25 (80.6) |
| Female | 6 (19.3) |
| Age (n, %) | |
| 20–30 | 11 (35.5) |
| 31–40 | 18 (58.1) |
| >40 | 2 (6.4) |
| Experience | 7.3 ± (3.8) |
| Representative of community pharmacy type | |
| Chain | 14 (45.2) |
| Independent | 17 (54.8) |
| Theme 1: The Current Scenarios of Medicine Shortages in the Community Setting | |
|---|---|
| Subtheme 1: Daily experience Subtheme 2: Panic buying, self medication and drug abuse are reasons for increasing shortages. Subtheme 3: Categorization of the short medicine Regularly short medicines Seasonally short medicines Shortages experienced in the COVID-19 pandemic | “I think the drug shortage is the situation in which our total supply of medicines is insufficient to meet the current or projected demand. I believe that shortage occurs every day in community setup of Pakistan” (CP11) “In my experience, the last year was much more difficult than the previous one, because we have the corona virus in the world beside this if we compare the last five years with the last year, so, we have multiple short medicines in only last year” (CP8) “The main drug which gets short is the Clonazepam comes under the brand name of Rivotril and Magura. All these brands are short from a couple of months and get short every year” (CP3) “We have shortage of antibiotics that is related to the upper respiratory tract infection specifically talking about in the winter season, as you know, the infection prevails in the winter season due to high smog and high fog level so, that medicine in the winter season is always got short from a distributor end” (CP1) “Last year there was a pandemic situation if we take an example; Azithromycin alternates were short and the Hydroxycloroquine tablet was too short, even the patients having arthritis couldn’t get it, just because of the pandemic situation” (CP6) |
| Theme 2: Barriers Encountered during the Shortage Management | |
|---|---|
Sub theme 1: Unethical activities
Subtheme 3:Physician prescribing behavior
| “Black marketing is the major offense which we see in a shortage situation. It should not be done”. (CP31) “In the shortage situation, some pharmacies do stockpiling when they get to know that some brands are becoming short in the market, they take bulk quantities. They hoard extra, not affective for the patient and not according to the demand of the patient”. (CP27) “Some distributors are biased for some re known chain pharmacies when they get stock of short medicine they don’t equally distribute their stock to the market”(CP3) “In Pakistan it is a common trend that the physician writes the brands not generics, so they have an edge to promote some brands and when we contact these physicians to write some other brands. They simply stick and refuse” (CP7). “The other barrier which we faced is the financial barrier, because we have to purchase other than our routine and we feel extra overload on ourselves” (CP29) |
| Theme 3: Impact of Medicine Shortages | |
|---|---|
| Subtheme 1: Negative impact on the pharmacy reputation Subtheme 2: Hinderance in achieving the sale target Subtheme 3:Increase work load Subtheme 4:Lack of incentive to the working staff Subtheme 5:Distrubance in the relationship of pharmacy staff and patients | “Reputation hits so badly as customers perceived that we don’t have these medicines. So patients would not visit next time to purchase any type of medicine either it is present or not” (CP7) “Drug shortages definitely affected badly our routine operations, it increases workload and it takes a lot of energy in order to overcome such issues.” (CP28) “When customers get bounce due to the shortage of medicines so, we are unable to give incentives and any bonus to the working pharmacy staff”(CP8) “Patients don’t understand any logics and reasons, because they are totally in need of the drug that physicians have prescribed to them” (CP15) |
| Theme 4: Corrective Actions Performed for Handling Shortages | |
|---|---|
Subtheme 1: Proactive measures
| “Firstly we keep a sufficient stock of running items. The second practice we have is that we also keep a stock of these products which are not frequently in demand, but we keep it to avoid any rebound of customers”. (CP12) “We have to make relations with the distributions so that they can intimate us properly before any shortages of medicines we can purchase it prior to its shortage” (CP3) “When the medicine is short from the supplier end so either we have to suggest the alternate, or we can ask the patients to contact their doctors to change the medicine” (CP6) “If the patient doesn’t agree to take the alternative so, we then go towards the local purchase. Initially, we try to look for the surrounding pharmacies if they can avail the medicine for us” (CP4) “If we talk about the selling of short medicines, we try to sell it in a limited quantity to maximum customers. For example, if we sell one pack to one customer, in a shortage situation it’s better to sell three blisters to three customers so all people get benefit” (CP13) |
| Theme 5: Future Interventions to Prevent the Shortages | |
|---|---|
Subtheme 1: Proper monitoring on the medicine sale and consumption
Subtheme 3:Disseminating the information on shortages Subtheme 4:Need of the collaborative effort | “There should be strict actions taken by the regulatory authorities. And not without the recommendation of a doctor, if it’s written on the prescription the right patient will get the medicine” (CP6) “The distributor should distribute medicines first to the retailers and then when they have excess stock then they should deliver to the local market, but the priority should be the retailers”(CP3) “There must be a proper intimation from the supplier end before the medicine shortage. This reporting will be helpful as the medicine suddenly gets short and due to this shortage, we suffer a huge pressure from the consumers’ end because we don’t know the medicine re-availability” (CP7) “Everyone must fulfil their duties to overcome the medicine shortages, because it is not only pharmacist’s task. Purchasers to planners and suppliers to pharmacy managers, everyone is included in it” (CP21) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Omer, S.; Ali, S.; Shukar, S.; Gillani, A.H.; Fang, Y.; Yang, C. A Qualitative Study Exploring the Management of Medicine Shortages in the Community Pharmacy of Pakistan. Int. J. Environ. Res. Public Health 2021, 18, 10665. https://doi.org/10.3390/ijerph182010665
Omer S, Ali S, Shukar S, Gillani AH, Fang Y, Yang C. A Qualitative Study Exploring the Management of Medicine Shortages in the Community Pharmacy of Pakistan. International Journal of Environmental Research and Public Health. 2021; 18(20):10665. https://doi.org/10.3390/ijerph182010665
Chicago/Turabian StyleOmer, Sumaira, Salamat Ali, Sundus Shukar, Ali Hassan Gillani, Yu Fang, and Caijun Yang. 2021. "A Qualitative Study Exploring the Management of Medicine Shortages in the Community Pharmacy of Pakistan" International Journal of Environmental Research and Public Health 18, no. 20: 10665. https://doi.org/10.3390/ijerph182010665
APA StyleOmer, S., Ali, S., Shukar, S., Gillani, A. H., Fang, Y., & Yang, C. (2021). A Qualitative Study Exploring the Management of Medicine Shortages in the Community Pharmacy of Pakistan. International Journal of Environmental Research and Public Health, 18(20), 10665. https://doi.org/10.3390/ijerph182010665