
The Effectiveness and Safety of Mind-Body Modalities for Mental Health of Nurses in Hospital Setting: A Systematic Review

 , ,
, , 
 and
and 
Abstract
:1. Introduction
2. Methods
2.1. Study Search
2.2. Study Selection and Inclusion Criteria
2.3. Risk of Bias Assessment
2.4. Data Extraction
2.5. Data Analysis
2.6. Publication Bias
3. Results
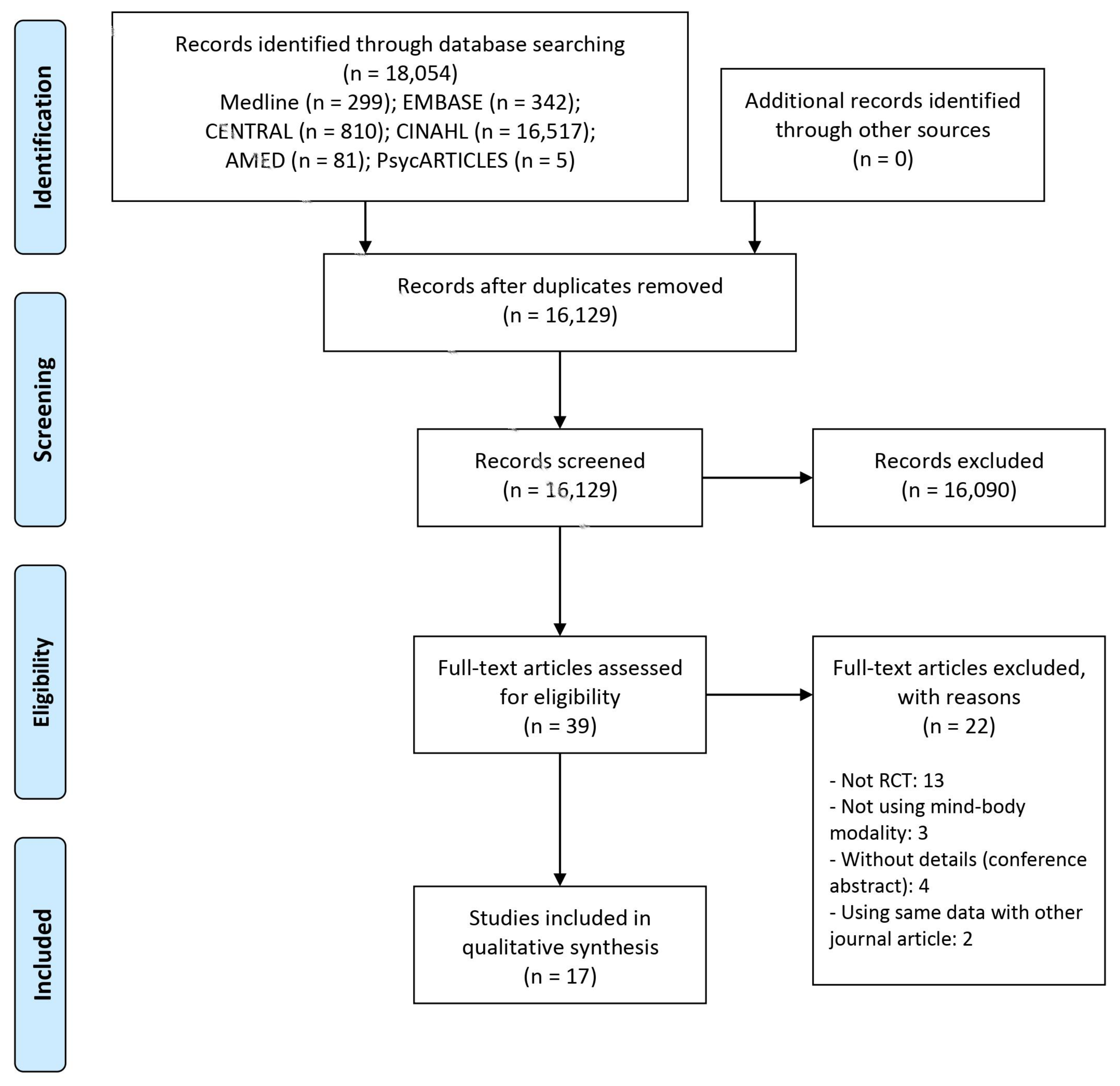
3.1. Study Search
3.2. Characteristics of Included Studies
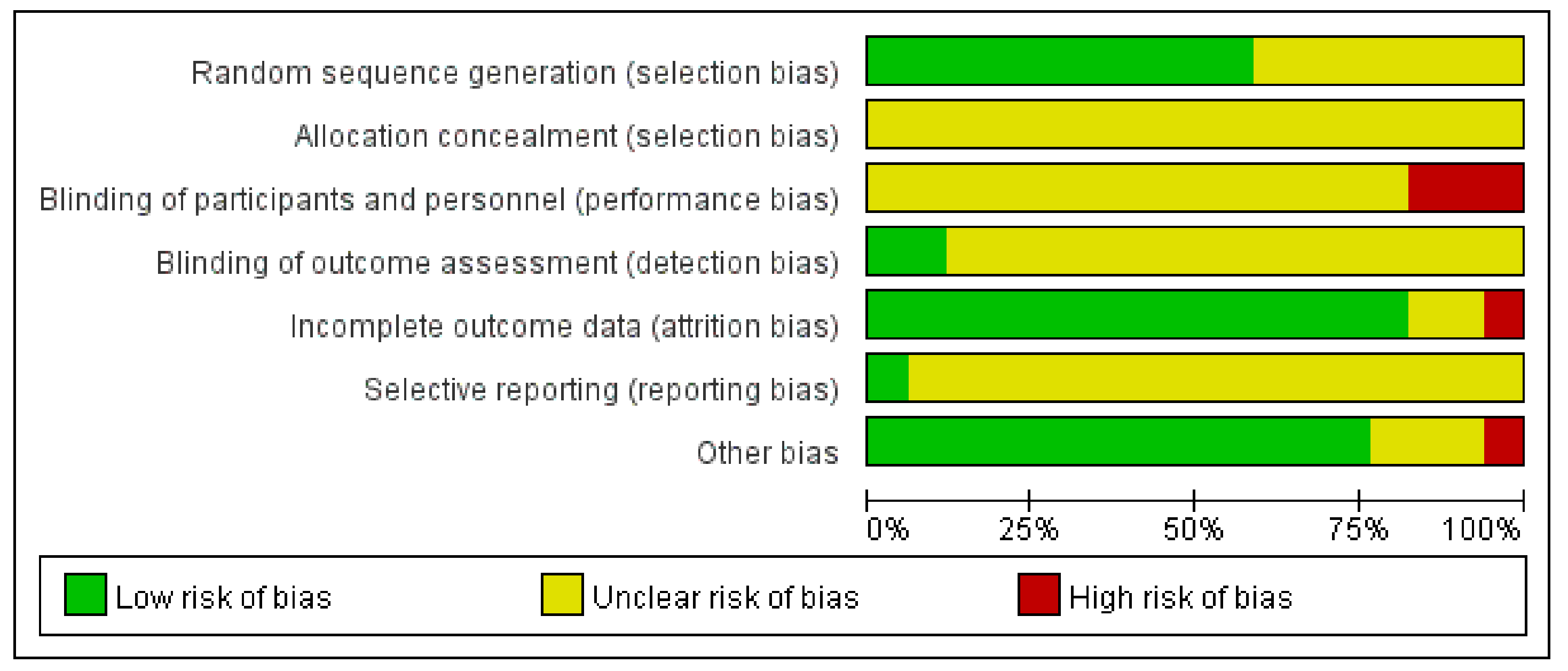
3.3. Methodological Qualities of Included Studies
3.4. Main Results
3.4.1. Primary Outcome (Burnout)
3.4.2. Secondary Outcomes
3.4.3. Safety Data
4. Discussion
4.1. Main Findings
4.2. Clinical Implications
4.3. Limitations and Suggestions for Further Studies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vasconcelos, S.C.; De Souza, S.L.; Sougey, E.B.; Ribeiro, E.C.D.O.; Nascimento, J.J.C.D.; Formiga, M.B.; Ventura, L.B.D.S.; Lima, M.D.D.C.; Silva, A.O. Nursing Staff Members Mental’s Health and Factors Associated with the Work Process: An Integrative Review. Clin. Pract. Epidemiology Ment. Health 2016, 12, 167–176. [Google Scholar] [CrossRef] [Green Version]
- Monsalve-Reyes, C.S.; Luis-Costas, C.S.; Gómez-Urquiza, J.L.; Albendín-García, L.; Aguayo, R.; La Fuente, G.A.C.-D. Burnout syndrome and its prevalence in primary care nursing: A systematic review and meta-analysis. BMC Fam. Pract. 2018, 19, 59. [Google Scholar] [CrossRef] [Green Version]
- Parker, P.A.; Kulik, J.A. Burnout, self- and supervisor-rated job performance, and absenteeism among nurses. J. Behav. Med. 1995, 18, 581–599. [Google Scholar] [CrossRef]
- Brower, V. Mind-body research moves towards the mainstream. EMBO Rep. 2006, 7, 358–361. [Google Scholar] [CrossRef]
- Younge, O.J.; Gotink, R.; Baena, C.P.; Roos-Hesselink, J.W.; Hunink, M.G.M. Mind-body practices for patients with cardiac disease: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2015, 22, 1385–1398. [Google Scholar] [CrossRef]
- Senders, A.; Wahbeh, H.; Spain, R.; Shinto, L. Mind-Body Medicine for Multiple Sclerosis: A Systematic Review. Autoimmune Dis. 2012, 2012, 567324. [Google Scholar] [CrossRef] [Green Version]
- Theadom, A.; Cropley, M.; Smith, E.H.; Feigin, V.L.; Mc Pherson, K. Mind and body therapy for fibromyalgia. Cochrane Database Syst. Rev. 2015, 4, CD001980. [Google Scholar] [CrossRef]
- Lee, M.C.; Crawford, P.; Hickey, A. Active Self-Care Therapies for Pain (PACT) Working Group Mind-body Therapies for the Self-Management of Chronic Pain Symptoms. Pain Med. 2014, 15, S21–S39. [Google Scholar] [CrossRef] [Green Version]
- Wells, R.E.; Phillips, R.S.; McCarthy, E.P. Patterns of Mind-Body Therapies in Adults with Common Neurological Conditions. Neuroepidemiology 2011, 36, 46–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bower, J.E.; Irwin, M.R. Mind-body therapies and control of inflammatory biology: A descriptive review. Brain Behav. Immun. 2016, 51, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanada, K.; Montero-Marin, J.; Barceló-Soler, A.; Ikuse, D.; Ota, M.; Hirata, A.; Yoshizawa, A.; Hatanaka, R.; Valero, M.S.; DeMarzo, M.; et al. Effects of Mindfulness-Based Interventions on Biomarkers and Low-Grade Inflammation in Patients with Psychiatric Disorders: A Meta-Analytic Review. Int. J. Mol. Sci. 2020, 21, 2484. [Google Scholar] [CrossRef] [Green Version]
- Cahn, B.R.; Goodman, M.S.; Peterson, C.T.; Maturi, R.; Mills, P.J. Yoga, Meditation and Mind-Body Health: Increased BDNF, Cortisol Awakening Response, and Altered Inflammatory Marker Expression after a 3-Month Yoga and Meditation Retreat. Front. Hum. Neurosci. 2017, 11, 315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacLaughlin, B.W.; Wang, D.; Noone, A.-M.; Liu, N.; Harazduk, N.; Lumpkin, M.; Haramati, A.; Saunders, P.; Dutton, M.; Amri, H. Stress Biomarkers in Medical Students Participating in a Mind Body Medicine Skills Program. Evid. Based Complement. Altern. Med. 2011, 2011, 950461. [Google Scholar] [CrossRef] [Green Version]
- Penque, S. Mindfulness to promote nurses’ well-being. Nurs. Manag. (Springhouse) 2019, 50, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Søvold, L.E.; Naslund, J.A.; Kousoulis, A.A.; Saxena, S.; Qoronfleh, M.W.; Grobler, C.; Münter, L. Prioritizing the Mental Health and Well-Being of Healthcare Workers: An Urgent Global Public Health Priority. Front. Public Health 2021, 9, 679397. [Google Scholar] [CrossRef]
- Callus, E.; Bassola, B.; Fiolo, V.; Bertoldo, E.G.; Pagliuca, S.; Lusignani, M. Stress Reduction Techniques for Health Care Providers Dealing With Severe Coronavirus Infections (SARS, MERS, and COVID-19): A Rapid Review. Front. Psychol. 2020, 11, 589698. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, A.E.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E.; Leiter, M.P.; Schaufeli, W.B.; Schwab, R.L. Maslach Burnout Inventory; Consulting psychologists press Palo Alto: Palo Alto, CA, USA, 1986; Volume 21. [Google Scholar]
- Higgins, J.; Altman, D.; Sterne, C. Chapter 8; Assessing the risk of bias in included studies. From the Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 [updated 2011]. The Cochrane Collaboration. 2011. Available online: https://handbook-5-1.cochrane.org/ (accessed on 18 March 2021).
- Foureur, M.; Besley, K.; Burton, G.; Yu, N.; Crisp, J. Enhancing the resilience of nurses and midwives: Pilot of a mindfulnessbased program for increased health, sense of coherence and decreased depression, anxiety and stress. Contemp. Nurse 2013, 45, 114–125. [Google Scholar] [CrossRef]
- Gauthier, T.; Meyer, R.; Grefe, D.; Gold, J. An On-the-Job Mindfulness-Based Intervention for Pediatric ICU Nurses: A Pilot Study. J. Altern. Complement. Med. 2014, 20, A87. [Google Scholar] [CrossRef]
- Watanabe, N.; Furukawa, A.T.; Horikoshi, M.; Katsuki, F.; Narisawa, T.; Kumachi, M.; Oe, Y.; Shinmei, I.; Noguchi, H.; Hamazaki, K.; et al. A mindfulness-based stress management program and treatment with omega-3 fatty acids to maintain a healthy mental state in hospital nurses (Happy Nurse Project): Study protocol for a randomized controlled trial. Trials 2015, 16, 36. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.A.; Park, J.S. Development and Application of an Overcoming Compassion Fatigue Program for Emergency Nurses. J. Korean Acad. Nurs. 2016, 46, 260–270. [Google Scholar] [CrossRef] [Green Version]
- Calisi, C.C. The Effects of the Relaxation Response on Nurses’ Level of Anxiety, Depression, Well-Being, Work-Related Stress, and Confidence to Teach Patients. J. Holist. Nurs. 2017, 35, 318–327. [Google Scholar] [CrossRef]
- Halm, M. The Role of Mindfulness in Enhancing Self-Care for Nurses. Am. J. Crit. Care 2017, 26, 344–348. [Google Scholar] [CrossRef]
- Daigle, S.; Talbot, F.; French, D.J. Mindfulness-based stress reduction training yields improvements in well-being and rates of perceived nursing errors among hospital nurses. J. Adv. Nurs. 2018, 74, 2427–2430. [Google Scholar] [CrossRef]
- Pan, C.; Wang, H.; Chen, M.; Cai, Y.; Xiao, C.; Tang, Q.; Koniak-Griffin, D. Mindfulness-Based Intervention For Nurses In AIDS Care In China: A Pilot Study. Neuropsychiatr. Dis. Treat. 2019, 15, 3131–3141. [Google Scholar] [CrossRef] [Green Version]
- Torres, L.-A.P.-D.; Atalaya, J.C.V.-M.; García-Campayo, J.; Roldán-Villalobos, A.; Magallón-Botaya, R.; Bartolomé-Moreno, C.; Moreno-Martos, H.; Melús-Palazón, E.; Liétor-Villajos, N.; Valverde-Bolívar, F.J.; et al. Controlled clinical trial comparing the effectiveness of a mindfulness and self-compassion 4-session programme versus an 8-session programme to reduce work stress and burnout in family and community medicine physicians and nurses: MINDUUDD study protocol. BMC Fam. Pract. 2019, 20, 24. [Google Scholar] [CrossRef]
- Yong, J.; Park, J.; Park, Y.; Lee, H.; Lee, G.; Rim, S. Effects of Holy Name Meditation on the Quality of Life of Hospital Middle Manager Nurses in Korea: A 6-Month Follow-Up. J. Contin. Educ. Nurs. 2020, 51, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Maguire, P. The Effect of Coloring Mandalas on the Anxiety of Medical-Surgical Nurses and Nursing Support Staff. MEDSURG Nurs. 2020, 29, 192–199. [Google Scholar]
- Owens, R.A.; Alfes, C.; Evans, S.; Wyka, K.; Fitzpatrick, J.J. An Exploratory Study of a 3-Minute Mindfulness Intervention on Compassion Fatigue in Nurses. Holist. Nurs. Pract. 2020, 34, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Xie, C.; Zeng, Y.; Lv, Y.; Li, X.; Xiao, J.; Hu, X. Educational intervention versus mindfulness-based intervention for ICU nurses with occupational burnout: A parallel, controlled trial. Complement. Ther. Med. 2020, 52, 102485. [Google Scholar] [CrossRef] [PubMed]
- McElligott, D.; Holz, M.B.; Carollo, L.; Somerville, S.; Baggett, M.; Kuzniewski, S.; Shi, Q. A pilot feasibility study of the effects of touch therapy on nurses. J. N. Y. State Nurses’ Assoc. 2003, 34, 16–24. [Google Scholar]
- Bost, N.; Wallis, M. The effectiveness of a 15 minute weekly massage in reducing physical and psychological stress in nurses. Aust. J. Adv. Nurs. Q. Publ. R. Aust. Nurs. Fed. 2006, 23, 28–33. [Google Scholar]
- El Khamali, R.; Mouaci, A.; Valera, S.; Cano-Chervel, M.; Pinglis, C.; Sanz, C.; Allal, A.; Attard, V.; Malardier, J.; Delfino, M.; et al. Effects of a Multimodal Program Including Simulation on Job Strain Among Nurses Working in Intensive Care Units. JAMA 2018, 320, 1988–1997. [Google Scholar] [CrossRef]
- Wlazelek, B.G. The Effects of Stress Inoculation for Anger Control and Relaxation Training on Anger and Related Measures with Nurses. Ph.D. Thesis, Lehigh University, Bethlehem, PA, USA, 1990. [Google Scholar]
- Rad, Z.Z.; Shafiabadi, A.; ZareBahramAbadi, M.; Moghaddam, L.F. The Use of Mindfulness-based Cognitive Therapy for Improving Flow Experience of Nurses in the Psychiatric Hospitals. Eur. Psychiatry 2015, 30, 1037. [Google Scholar] [CrossRef]
- Smith, O.; Faulkner, K.; Skiffington, A.; McShane, J.; Wan, C.; Krock, M. A randomized controlled trial of an intervention to enhance resilience in acute care nurses (ARISE). Crit. Care Med. 2019, 47, 35. [Google Scholar] [CrossRef]
- Watanabe, N. Brief mindfulness-based stress management program for a better mental state in working populations-happy nurse project: A randomized controlled trials. Psychosomat. Med. 2019, 81, A136. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S. The Effects of Relaxation Training, Combining Meditation and Guided Imagery, on Self-Perceived Stress among Chinese Nurses in Large Teaching Hospitals in Taiwan, China. Ph.D. Thesis, University of Texas at Austin, Austin, TX, USA, 1992. [Google Scholar]
- Mealer, M.; Conrad, D.; Evans, J.; Jooste, K.; Rothbaum, B.; Moss, M. A 12-week multimodal resilience training program for intensive care unit nurses: Results of a pilot study. Am. J. Respir. Crit. Care Med. 2014, 189, A5217–A5247. [Google Scholar]
- Tsai, S.-L.; Crockett, M.S. Effects of Relaxation Training, Combining Imagery, and Meditation the Stress Level of Chinese Nurses Working in Modern Hospitals in Taiwan. Issues Ment. Health Nurs. 1993, 14, 51–66. [Google Scholar] [CrossRef]
- Yung, P.M.B.; Fung, M.Y.; Chan, T.M.F.; Lau, B.W.K. Relaxation training methods for nurse managers in Hong Kong: A controlled study. Int. J. Ment. Health Nurs. 2004, 13, 255–261. [Google Scholar] [CrossRef]
- Lai, H.-L.; Li, Y.-M. The effect of music on biochemical markers and self-perceived stress among first-line nurses: A randomized controlled crossover trial. J. Adv. Nurs. 2011, 67, 2414–2424. [Google Scholar] [CrossRef]
- Mealer, M.; Conrad, D.; Evans, J.; Jooste, K.; Solyntjes, J.; Rothbaum, B.; Moss, M. Feasibility and Acceptability of a Resilience Training Program for Intensive Care Unit Nurses. Am. J. Crit. Care 2014, 23, e97–e105. [Google Scholar] [CrossRef]
- Alexander, G.K.; Rollins, K.; Walker, D.; Wong, L.; Pennings, J. Yoga for Self-Care and Burnout Prevention Among Nurses. Work. Health Saf. 2015, 63, 462–470. [Google Scholar] [CrossRef]
- Fang, R.; Li, X. A regular yoga intervention for staff nurse sleep quality and work stress: A randomised controlled trial. J. Clin. Nurs. 2015, 24, 3374–3379. [Google Scholar] [CrossRef]
- Chang, S.J.; Kwak, E.Y.; Hahm, B.-J.; Seo, S.H.; Lee, D.W.; Jang, S.J. Effects of a Meditation Program on Nurses’ Power and Quality of Life. Nurs. Sci. Q. 2016, 29, 227–234. [Google Scholar] [CrossRef]
- Ploukou, S.; Panagopoulou, E. Playing music improves well-being of oncology nurses. Appl. Nurs. Res. 2018, 39, 77–80. [Google Scholar] [CrossRef]
- Yang, J.; Tang, S.; Zhou, W. Effect of mindfulness-based stress reduction therapy on work stress and mental health of psychiatric nurses. Psychiatr. Danub. 2018, 30, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; He, G.; Yan, J.; Gu, C.; Xie, J. The Effects of a Modified Mindfulness-Based Stress Reduction Program for Nurses: A Randomized Controlled Trial. Work. Health Saf. 2018, 67, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Miyoshi, Y. Restorative yoga for occupational stress among Japanese female nurses working night shift: Randomized crossover trial. J. Occup. Health 2019, 61, 508–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozgundondu, B.; Metin, Z.G. Effects of progressive muscle relaxation combined with music on stress, fatigue, and coping styles among intensive care nurses. Intensiv. Crit. Care Nurs. 2019, 54, 54–63. [Google Scholar] [CrossRef]
- Rostami, K.; Ghodsbin, F. Effect of Yoga on the Quality of Life of Nurses Working in Intensive Care Units. Randomized Controlled Clinical Trial. Investig. Educ. Enferm. 2019, 37. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, N.; Horikoshi, M.; Shinmei, I.; Oe, Y.; Narisawa, T.; Kumachi, M.; Matsuoka, Y.; Hamazaki, K.; Furukawa, T.A. Brief mindfulness-based stress management program for a better mental state in working populations—Happy Nurse Project: A randomized controlled trial✰✰. J. Affect. Disord. 2019, 251, 186–194. [Google Scholar] [CrossRef]
- Ghawadra, S.F.; Abdullah, K.L.; Choo, W.Y.; Danaee, M.; Phang, C.K. The effect of mindfulness-based training on stress, anxiety, depression and job satisfaction among ward nurses: A randomized control trial. J. Nurs. Manag. 2020, 28, 1088–1097. [Google Scholar] [CrossRef]
- Grabbe, L.; Higgins, M.K.; Baird, M.; Craven, P.A.; Fratello, S.S. The Community Resiliency Model® to promote nurse well-being. Nurs. Outlook 2020, 68, 324–336. [Google Scholar] [CrossRef] [PubMed]
- Zamanifar, S.; Bagheri-Saveh, M.I.; Nezakati, A.; Mohammadi, R.; Seidi, J. The Effect of Music Therapy and Aromatherapy with Chamomile-Lavender Essential Oil on the Anxiety of Clinical Nurses: A Randomized and Double-Blind Clinical Trial. J. Med. Life 2020, 13, 87–93. [Google Scholar] [PubMed]
- García-Gutiérrez, M.S.; Navarrete, F.; Sala, F.; Gasparyan, A.; Austrich-Olivares, A.; Manzanares, J. Biomarkers in Psychiatry: Concept, Definition, Types and Relevance to the Clinical Reality. Front. Psychiatry 2020, 11, 432. [Google Scholar] [CrossRef]
- Parekh-Bhurke, S.; Kwok, C.S.; Pang, C.L.; Hooper, L.; Loke, Y.K.; Ryder, J.J.; Sutton, A.J.; Hing, C.; Harvey, I.; Song, F. Uptake of methods to deal with publication bias in systematic reviews has increased over time, but there is still much scope for improvement. J. Clin. Epidemiol. 2011, 64, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Murad, M.H.; Chu, H.; Lin, L.; Wang, Z. The effect of publication bias magnitude and direction on the certainty in evidence. BMJ Evid. Based Med. 2018, 23, 84–86. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Study ID (Study Design/Country) | Sample Size (Included→Analyzed) | Mean Age (Range) (Years) | Ward In Which Nurses Work | Pathological Condition | Treatment Intervention | Control Intervention | Intervention Period (Assessment) | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Tsai 1993 (Parallel RCT/Taiwan) | 137→134 TG: unclear CG: unclear | 25.2 (21–41) | MU, SU, ICU, PED, OB, OR, OPD, GYN, etc. | NA | Relaxation training (90 min/session, 1 session/week) | Traditional in-service education through lectures on theory analysis (90 min/session, 1 session/week) | 2 weeks (Week 0, 2, 5) | 1. NSC; 2. GHQ |
| Yung 2004 (Parallel RCT/Hong Kong) | 65→65 TG1: 17→17 TG2: 18→18 CG: 30→30 | NR | NR | NA | TG1: Stretch-release relaxation TG2: Cognitive relaxation (20 min/session, 1 session/week) | No intervention | 4 weeks (Week 0, 4) | 1. State-STAI; 2. Trait-STAI; 3. GHQ |
| Lai 2011 (Cross-over RCT/Taiwan) | 54→54 TG: 27 (music→chair rest) CG: 54 (chair rest→music) | 23.4 ± 2.46 | MU, SU, maternal & PED, ICU | VAS stress ≥ 6 | Music (30 min/session) | Chair rest (30 min/session) | 1 x 1 session, wash-out 20 min (Min 0, 15, 30) | 1. Self-perceived stress (0–10 cm VAS); 2. HR; 3. Mean arterial BP (mmHg); 4. Finger temperature; 5. Serum cortisol (ug/dL) |
| Mealer 2014 (Parallel RCT/America) | 27→27 TG: 13 CG: 14 | NR | ICU | 82 ≥ CDRS | Multimodal resilience training program (2-day educational workshop; written exposure therapy (twelve 30 min sessions via email); MBSR (self-practice, 15 min at least 3 times per week); aerobic exercise (30–45 min at least 3 times per week); event-triggered counseling (30–60 min per session if needed)) | No intervention | 1. HADS; 2. MBI; 3. PDS; 4. CDRS | |
| Alexander 2015 (Parallel RCT/America) | 40→40 TG: 20 CG: 20 | NR | NR | NA | Yoga (1 session/week) | Usual care | 8 weeks (Week 0, 8) | 1. HPLP-II; 2. FMI; 3. MBI |
| Fang 2015 (Parallel RCT/China) | 120→105 TG: 61→54 CG: 59→51 | TG: 35.13 ± 10.98 CG: 36.05 ± 9.91 (25–51) | NR | NA | Yoga (50–60 min/session, more than 2 sessions/week) | No intervention | 6 months (Month 0, 6) | 1. PSQI; 2. QMWS |
| Chang 2016 (Parallel RCT/Korea) | 50→40 TG: 25→21 CG: 25→19 | 31.5 ± 5.45 TG: 30.9 ± 5.59 CG: 32.1 ± 5.38 | nurses of special nursing department | NA | Meditation (1–1.5 hours/session, 1 session/week) | No intervention | 8 weeks (Week 0, 8) | 1. PKPCT v II; 2. WHOQOL-BREF |
| Ploukou 2018 (Parallel RCT/Greece) | 48→48 TG: 22 CG: 26 | NR | ONC | NA | Percussion music (1 h/session, 1 session/week) | No intervention | 4 weeks (Week 0, 4) | 1. HADS; 2. PILL |
| Yang 2018 (Parallel RCT/China) | 100→95 TG: 50→48 CG: 50→47 | 29.5 ± 7.1 | PSY | positive in more than 30 items of SCL-90-R | MBSR (1 session/week) | Routine psychological support and activities. | 8 weeks (Week 0, 8) | 1. SCL-90-R; 2. SDS; 3. SAS; 4. NSS |
| Lin 2019 (Parallel RCT/China) | 110→90 TG: 55→44 CG: 55→46 | TG: 32.86 ± 7.49 CG: 30.20 ± 6.09 | NR | NA | MBSR (2.5 h/session, 1 session/week) | No intervention | 8 weeks (Week 0, 8, 12) | 1. PSS; 2. PANAS; 3. CDRS; 4. MMSS |
| Miyoshi 2019 (Cross-over RCT/Japan) | 20→20 TG: 10 (yoga→normal stress relief) CG: 10 (normal stress relief →yoga) | 28.7 ± 4.9 (24–39) | NR | NA | Yoga (initial 1 h group session, and then self-practice, more than 5–15 min/session, more than 3 times/week) | Stress relief (including sleeping, shopping, and chatting with friends) | 4 weeks × 4 weeks, wash-out 1 week (Week 0, 5, 10) | 1. BJSQ |
| Ozgundondu 2019 (Parallel RCT/Turkey) | 63→56 TG: 31→28 CG: 21→28 | TG: 24.61 ± 2.61 CG: 27.75 ± 4.75 | IM, ANE, CICU | NA | PMR (20 min/session, 1 session/week) | Face-to-face attention-matched education (a 20 min session) | 8 weeks (Week 0, 4, 8, 12) | 1. PSS; 2. FSS; 3. Brief COPE |
| Rostami 2019 (Parallel RCT/France) | 70→70 TG: 35 CG: 35 | TG: 30.5 ± 5.14 CG: 29.3 ± 5.1 | ICU | NA | Yoga (2 session/week) | No intervention | 8 weeks (Week 0, 4, 8, 24) | WHOQOL–BREF |
| Watanabe 2019 (Parallel RCT/Japan) | 80→76,75 TG: 40→37 (assessed via phone), 36 (via internet) CG: 40→39 (via both phone and internet) | TG: 30.2 ± 9.0 (21–53) CG: 30.0 ± 7.9 (22–55) | IPD | NA | Brief mindfulness-based stress management program (30 min/session, 4 session/week) | Psychoeducation using a leaflet | 26 weeks (Week 0, 13, 26, 52) | 1. HADS; 2. PHQ-9; 3. GAD-7; 4. ISI; 5. MBI; 6. WHO-WPQ; 7. EQ-5D utility score |
| Ghawadra 2020 (Parallel RCT/Malaysia) | 249→224 TG: 123→118 CG: 126→106 | unclear | ICU, MU, SU, PED, OB & GYN | DASS-21 (stress (15–25), anxiety (8–14), depression (10–20)) | Mindfulness-based training (initial 2 h workshop, and then self-practice via website) | No intervention | 5 weeks (Week 0, 5, 8) | 1. DASS-21; 2. JSS; 3. MAAS |
| Grabbe 2020 (Parallel RCT/America) | 77→69 TG: 40→33 CG: 37→36 | TG: 44.6 ± 13.4 (23–70) CG: 45.9 ± 13.0 (23–73) | ED, OR, ICU, specialty units, OPD, SU | NA | Community resiliency model (psychoeducation/sensory awareness skills training class, including mindful eating) (initial 3 h class, and then self-practice via application) | Nutrition/healthy eating (initial 3 h class, and then self-practice via application) | 1 year (Week 0, 1, 12, 52) | 1. WHO-5; 2. CDRS; 3. STSS; 4. CBI; 5. SSS-8 |
| Zamanifar 2020 (Parallel RCT/Iran) | 120→120 TG1: 30 TG2: 30 TG3: 30 CG: 30 | TG1: 32.33 ± 4.59 TG2: 32.27 ± 4.66 TG3: 32 ± 5.53 CG: 32.60 ± 5.83 | ED & PED-ED, ICU & PED-ICU, IM & PED-IM, PED-IU, NU, ONC, IM, NB | BAI ≥ 8 | TG1: music therapy TG2: aromatherapy (with chamomile–lavender essential oil) TG3: aromatherapy & music therapy (20 min/session, 1 session/week) | No intervention | 12 weeks (Week 0, 12) | BAI |
| Outcomes | Comparison (TG vs. CG) | Results | Reference |
|---|---|---|---|
| Outcomes on occupation and environment | |||
| (1) JSS (job satisfaction) | MBIs vs. No intervention | By generalized estimating equations, Wald Chi–Square and df value (time x group interaction) was presented. Wald Chi-Square = 7.594 (2), df = 2 (p = 0.040) | Ghawadra 2020 |
| (2) MMSS (job satisfaction) | MBSR vs. No intervention | TG: 102.27 ± 14.44, CG: 96.17 ± 18.05 (p > 0.05) | Lin 2019 |
| (3) WHO-WPQ (presenteeism) | MBIs vs. Psychoeducation | (1) Absolute presenteeism -TG: 59.0 ± 14.19798, CG: 55.4 ± 13.55262 (p = 0.258) (2) Relative presenteeism -TG: 0.93 ± 0.322681, CG:0.88 ± 0.322681 (p = 0.065) | Watanabe 2019 |
| Outcomes on the individual’s resistance to stress | |||
| (1) Brief-COPE (coping style) | PMR vs. Education | Median value (25th–75th quartiles) (1) Use of instrumental support –TG: 5.5 (4.0–7.0), CG: 6.0 (5.0–6.0) (p = 0.980) (2) Humor -TG: 4.0 (3.0–4.7), CG: 4.0 (3.0–5.0) (p = 0.425) (3) Active coping -TG: 6.0 (6.0–7.0), CG: 6.0 (5.2–6.7) (p = 0.237) (4) Substance use -TG: 2.0 (2.0–2.0), CG: 2.0 (2.0–2.7) (p = 0.631) (5) Acceptance -TG: 6.0 (5.0–7.0), CG: 5.0 (4.0–6.0) (p = 0.038) (6) Venting -TG: 6.0 (5.0–6.0), CG: 5.0 (5.0–6.0) (p = 0.235) (7) Religion -TG: 6.0 (6.0–6.7), CG: 6.0 (4.2–6.0) (p = 0.108) (8) Denial: TG-3.5 (3.0–5.0), CG: 3.5 (2.2–4.0) (p = 0.302) (9) Behavioral disengagement –TG: 2.0 (2.0–3.0), CG: 3.0 (2.0–3.0) (p = 0.413) (10) Self-distraction -TG: 6.0 (6.0–7.0), CG: 6.0 (5.2–7.0) (p = 0.224) (11) Self-blame -TG: 4.0 (4.0–6.0), CG: 4.5 (4.0–5.0) (p = 0.758) (12) Positive reframing -TG: 6.0 (6.0–7.0), CG: 6.0 (6.0–7.0) (p = 0.295) (13) Use of emotional support -TG: 6.0 (5.0–7.0), CG: 5.0 (4.0–6.0) (p = 0.101) (14) Planning -TG: 6.0 (6.0–7.0), CG: 6.0 (5.0–7.0) (p = 0.160) | Ozgundondu 2019 |
| (2) HPLP–II (healthy lifestyle) | Yoga vs. Usual care | TG: 3.08 ± 0.40, CG: 2.69 ± 0.38 (p = 0.006) | Alexander 2015 |
| (3) CDRS (resilience) | Multimodal resilience training program vs. No intervention | Median value TG: 78, CG: 79 (The two groups were not statistically compared.) | Mealer 2014 |
| MBSR vs. No intervention | TG: 57.98 ± 11.58, CG: 55.11 ± 12.80 (p > 0.05) | Lin 2019 | |
| Community resiliency model (including mindful eating) vs. Nutrition/healthy eating | TG: 31.72 ± 4.02, CG: 30.54 ± 4.99 (p = 0.910) | Grabbe 2020 | |
| (4) PKPCT v II (power) | Meditation vs. No intervention | (1) Global score –TG: 228.20 ± 36.97, CG:214.10 ± 33.82 (p = 0.001) (2) Awareness –TG:55.20 ± 9.60, CG:51.50 ± 8.44 (p = 0.049) (3) Choices –TG:56.80 ± 10.64, CG:52.90 ± 11.13 (p = 0.017) (4) Freedom –TG:59.70 ± 9.75, CG: 54.10 ± 10.67 (p = 0.005) (5) Involvement –TG: 56.60 ± 9.01, CG:54.60 ± 7.32 (p = 0.001) | Chang 2016 |
| (5) FMI (mindfulness) | Yoga vs. Usual care | TG: 43.60 ± 7.32, CG: 39.65 ± 7.07 (p = 0.067) | Alexander 2015 |
| (6) MAAS (mindfulness) | MBIs vs. No intervention | By generalized estimating equations, Wald Chi–Square and df value (time x group interaction) was presented. Wald Chi–Square = 0.066 (2), df = 2 (p = 0.967) | Ghawadra 2020 |
| Outcomes on the Individual’s Global Health and Wellness | |||
| (1) WHOQOL-BREF (quality of life) | Meditation vs. No intervention | (1) Global score -TG: 54.00 ± 9.20, CG: 52.50 ± 6.77 (p = 0.006) (2) Physical -TG: 13.90 ± 2.90, CG:13.40 ± 1.90 (p = 0.018) (3) Psychological -TG: 13.00 ± 2.96, CG: 13.30 ± 1.80 (p = 0.039) (4) Social -TG: 13.70 ± 2.63, CG: 12.60 ± 2.15 (p = 0.034) (5) Environmental -TG: 13.60 ± 2.05, CG: 13.20 ± 2.26 (p = 0.057) | Chang 2016 |
| Yoga vs. No intervention | (1) Global score -TG: 72.8 ± 2.8, CG: 62.4 ± 2.2 (p < 0.001) (2) Physical -TG: 70.14 ± 3.1, CG: 62.1 ± 2.3 (p < 0.001) (3) Psychological -TG: 73.3 ± 3.0, CG: 62.2 ± 1.8 (p < 0.001) (4) Social -TG: 72.6 ± 2.8, CG: 64.2 ± 2.4 (p < 0.001) (5) Environment -TG: 75.5 ± 2.4, CG: 61.3 ± 2.5 (p < 0.001) | Rostami 2019 | |
| (2) EQ-5D (quality of life) | MBIs vs. Psychoeducation | (1) Utility -TG: 0.85 ± 0.129073, CG: 0.88 ± 0.129073 (p = 0.131) | Watanabe 2019 |
| (3) WHO-5 (well–being) | Community resiliency model (including mindful eating) vs. Nutrition/healthy eating | TG: 70.24 ± 16.74, CG: 62.46 ± 18.93 (p = 0.168) | Grabbe 2020 |
| (4) GHQ (general health) | Relaxation vs. Traditional in-service education | Repeated measures ANOVA, interaction effect of treatment and time F [1, 132] = 1.86, p < 0.05 | Tsai 1993 |
| Stretch-release relaxation vs. Cognitive relaxation vs. No intervention | TG1: 26.24 ± 9.23, TG2: 24.78 ± 7.03, CG: 28.83 ± 10.35 (p = 0.320) | Yung 2004 | |
| Outcomes on Psychological Symptoms | |||
| (1) SCL-90-R (psychological pathology) | MBSR vs. Routine psychological support and activities | TG:119.6 ± 21.6, CG:132.6 ± 24.9 (p < 0.001) | Yang 2018 |
| (2) MBI (burnout) - The primary outcome | Multimodal resilience training program vs. No intervention | Median value (25th-75th quartiles) (1) Emotional exhaustion -TG: 13.0 (8–28), CG: 25.0 (13–28) (2) Depersonalization - TG: 9 (5–16), CG: 10 (7–15) (3) Lack of personal accomplishment -TG: 37 (30–42), CG: 32 (28–40) (The two groups were not statistically compared.) | Mealer 2014 |
| Yoga vs. Usual care | (1) Emotional exhaustion -TG: 12.95 ± 8.76, CG: 20.60 ± 12.09 (p = 0.041) (2) Depersonalization -TG: 2.50 ± 3.65, CG: 5.15 ± 4.51 (p = 0.035) (3) Lack of personal accomplishment -TG: 39.60 ± 8.90, CG: 37.05 ± 9.98 (p = 0.554) | Alexander 2015 | |
| MBI vs. Psychoeducation | (1) Emotional exhaustion -TG: 24.3 ± 9.35776, CG: 21.7 ± 8.712398 (p = 0.341) (2) Depersonalization -TG: 7.3 ± 4.840221, CG: 8.4 ± 4.840221 (p = 0.266) (3) Lack of personal accomplishment -TG: 22.2 ± 6.776309, CG: 22.2 ± 6.776309 (p = 0.664) | Watanabe 2019 | |
| (3) CBI (burnout) - The primary outcome | Community resiliency model (including mindful eating) vs. Nutrition/healthy eating | TG: 43.90 ± 18.32, CG: 38.22 ± 20.26 (p = 0.777) | Grabbe 2020 |
| (4) NSC (stress) | Relaxation vs. Traditional in–service education | Repeated measures ANOVA, interaction effect of treatment and time F [1, 132] = 12.5, p < 0.05 | Tsai 1993 |
| (5) NSS (stress) | MBSR vs. Routine psychological support and activities | TG: 68.2 ± 9.1, CG: 83.1 ± 8.4 (p < 0.001) | Yang 2018 |
| (6) Self-perceived stress (stress) | Music vs. Chair rest | TP: 2.98 ± 1.51, CP: 4.78 ± 1.62 (p < 0.001) | Lai 2011 |
| (7) PSS (stress) | MBSR vs. No intervention | TG: 37.39 ± 5.97, CG: 40.76 ± 5.01 (p < 0.01) | Lin 2019 |
| PMR vs. Education | Median value (25th–75th quartiles) TG: 27.00 (25.00–29.75), CG: 29.00 (27.00–31.75) (p = 0.030) | Ozgundondu 2019 | |
| (8) BJSQ (stress) | Yoga vs. Stress relief method | TP: 56.1 ± 8.5, CP: 64.1 ± 12.7 (p = 0.01) | Miyoshi 2019 |
| (9) QMWS (stress) | Yoga vs. No intervention | Number of QMWS score > 32 (high stress) TG: 19/54, CG: 39/51 (p = 0.001) | Fang 2015 |
| (10) STSS (posttraumatic stress) | Community resiliency model (including mindful eating) vs. Nutrition/healthy eating | TG: 32.31 ± 9.53, CG: 30.30 ± 9.56 (p = 0.846) | Grabbe 2020 |
| (11) PDS (posttraumatic stress) | Multimodal resilience training program vs. No intervention | Median value (25th–75th quartiles) TG: 37 (30–42), CG: 32 (28–40) (The two groups were not statistically compared.) | Mealer 2014 |
| (12) STAI-state (anxiety state) | Stretch-release relaxation vs. Cognitive relaxation vs. No intervention | TG1: 38.35 ± 7.36, TG2: 36.89 ± 5.75, CG: 41.48 ± 8.16 (p = 0.097) | Yung 2004 |
| (13) STAI-trait (anxiety trait) | Stretch-release relaxation vs. Cognitive relaxation vs. No intervention | TG1: 43.59 ± 6.58, TG2: 42.06 ± 6.26, CG: 40.48 ± 6.33 (p = 0.679) | Yung 2004 |
| (14) DASS-21 (depression, anxiety, stress) | MBIs vs. No intervention | By generalized estimating equations, Wald Chi–Square and df value (time × group interaction) was presented. (1) Stress -Wald Chi–Square = 3.673 (2), df = 2 (p = 0.159) (2) Anxiety -Wald Chi–Square = 9.694 (2), df = 2 (p = 0.008) (3) Depression -Wald Chi–Square = 0.686 (2), df = 2 (p = 0.709) | Ghawadra 2020 |
| (15) PANAS (positive and negative emotion) | MBSR vs. No intervention | (1) Positive emotion/affect –TG: 32.02 ± 6.45, CG: 29.00 ± 5.51 (p < 0.05) (2) Negative emotion/affect –TG: 20.80 ± 4.72, CG: 23.61 ± 5.17 (p < 0.01) | Lin 2019 |
| (16) HADS (depression, anxiety) | Multimodal resilience training program vs. No intervention | Median value (25th–75th quartiles) (1) Anxiety -TG: 12.0 (10–13), CG: 11 (10–12) (2) Depression - TG: 9.0 (7–10), CG: 9.0 (8–11) (The two groups were not statistically compared.) | Mealer 2014 |
| Percussion music vs. No intervention | (1) Depression -TG: 13.23 ± 2.83, CG: 13.04 ± 2.72 (p > 0.05) | Ploukou 2018 | |
| MBIs vs. Psychoeducation | (1) Depression -TG: 3.21 ± 2.25877, CG: 2.54 ± 2.226502 (p = 0.192) (2) Anxiety -TG: 3.98 ± 2.226502, CG: 3.43 ± 2.161965 (p = 0.190) | Watanabe 2019 | |
| (17) SAS (anxiety) | MBSR vs. Routine psychological support and activities | TG:36.4 ± 7.1, CG: 45.1 ± 6.7 (p < 0.001) | Yang 2018 |
| (18) BAI (anxiety) | Music therapy vs. Aromatherapy vs. Music & Aromatherapy vs. No intervention | TG1: 39.74 ± 8.45, TG2: 37.83 ± 8.79, TG3: 39.97 ± 9.38, CG: 51.37 ± 9.58 (p = 0.999 for TG1 vs. TG2; p = 0.999 for TG2 vs. TG3; p = 0.0001 for TG2 vs. CG; p = 0.999 for TG1 vs. TG3; p = 0.0001 for TG1 vs. CG; p = 0.0001 for TG3 vs. CG) | Zamanifar 2020 |
| (19) GAD-7 (anxiety) | MBIs vs. Psychoeducation | TG: 4.13 ± 2.484647, CG: 3.11 ± 2.387842 (p = 0.057) | Watanabe 2019 |
| (20) SDS (depression) | MBSR vs. Routine psychological support and activities | TG: 35.4 ± 8.3, CG: 41.2 ± 8.7 (p < 0.001) | Yang 2018 |
| (21) PHQ-9 (depression) | MBIs vs. Psychoeducation | TG: 5.78 ± 3.065473, CG: 4.97 ± 2.936401 (p = 0.315) | Watanabe 2019 |
| (22) PSQI (insomnia) | Yoga vs. No intervention | (1) Global score –TG: 7.61 ± 1.25, CG: 10.31 ± 2.42 (2) Sleep quality –TG: 1.34 ± 0.35, CG: 1.68 ± 0.31 (3) Sleep duration –TG: 1.34 ± 0.09, CG: 1.68 ± 0.45 (4) Sleep efficiency –TG: 1.42 ± 0.11, CG: 1.79 ± 0.38 (5) Sleep disturbance –TG: 1.51 ± 0.17, CG: 1.93 ± 0.45 (6) Use of sleep medication –TG: 1.41 ± 0.23, CG: 1.79 ± 0.34 (7) Daytime dysfunction –TG: 1.24 ± 0.11, CG: 1.83 ± 0.41 (The two groups were not statistically compared.) | Fang 2015 |
| (23) ISI (insomnia) | MBIs vs. Psychoeducation | TG: 6.18 ± 3.743104, CG: 5.35 ± 3.549495 (p = 0.435) | Watanabe 2019 |
| Outcomes on Somatic Symptoms | |||
| (1) SSS-8 (somatic symptom) | Community resiliency model (including mindful eating) vs. Nutrition/healthy eating | TG: 5.81 ± 4.55, CG: 5.27 ± 4.26 (p = 0.563) | Grabbe 2020 |
| (2) PILL (psychosomatic symptom) | Percussion music vs. No intervention | Median value (25th–75th quartiles) TG: 99.5 (77.75–128.25), CG: 114.5 (86.75–144.75) (p > 0.05) | Ploukou 2018 |
| (3) FSS (fatigue) | PMR vs. Education | TG: 30.86 ± 10.41, CG: 42.82 ± 9.66 (p < 0.001) | Ozgundondu 2019 |
| Outcomes on Biological Data | |||
| (1) mean arterial BP (mmHg) | Music vs. Chair rest | TP: 84.80 ± 7.54, CP: 90.52 ± 7.75 (p < 0.001) | Lai 2011 |
| (2) serum cortisol (nmol/mmol) | Music vs. Chair rest | TP: 4.97 ± 3.42, CP: 6.42 ± 3.46 (p < 0.025) | Lai 2011 |
| (3) HR (per minute) | Music vs. Chair rest | TP: 65.44 ± 8.82, CP: 69.06 ± 9.55 (p < 0.001) | Lai 2011 |
| (4) finger temperature (℃) | Music vs. Chair rest | TP: 26.92 ± 4.70, CP: 24.11 ± 4.53 (p < 0.001) | Lai 2011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, S.-E.; Ha, D.-J.; Park, J.-H.; Lee, B.; Kim, M.-S.; Sim, K.-L.; Choi, Y.-H.; Kwon, C.-Y. The Effectiveness and Safety of Mind-Body Modalities for Mental Health of Nurses in Hospital Setting: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8855. https://doi.org/10.3390/ijerph18168855
Jung S-E, Ha D-J, Park J-H, Lee B, Kim M-S, Sim K-L, Choi Y-H, Kwon C-Y. The Effectiveness and Safety of Mind-Body Modalities for Mental Health of Nurses in Hospital Setting: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(16):8855. https://doi.org/10.3390/ijerph18168855
Chicago/Turabian StyleJung, Su-Eun, Da-Jung Ha, Jung-Hyun Park, Boram Lee, Myo-Sung Kim, Kyo-Lin Sim, Yung-Hyun Choi, and Chan-Young Kwon. 2021. "The Effectiveness and Safety of Mind-Body Modalities for Mental Health of Nurses in Hospital Setting: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 16: 8855. https://doi.org/10.3390/ijerph18168855
APA StyleJung, S.-E., Ha, D.-J., Park, J.-H., Lee, B., Kim, M.-S., Sim, K.-L., Choi, Y.-H., & Kwon, C.-Y. (2021). The Effectiveness and Safety of Mind-Body Modalities for Mental Health of Nurses in Hospital Setting: A Systematic Review. International Journal of Environmental Research and Public Health, 18(16), 8855. https://doi.org/10.3390/ijerph18168855