
Cerebrospinal Fluid Protein Concentration in Healthy Older Japanese Volunteers

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Research Subjects and CSF Sampling
2.3. Statistical Analysis
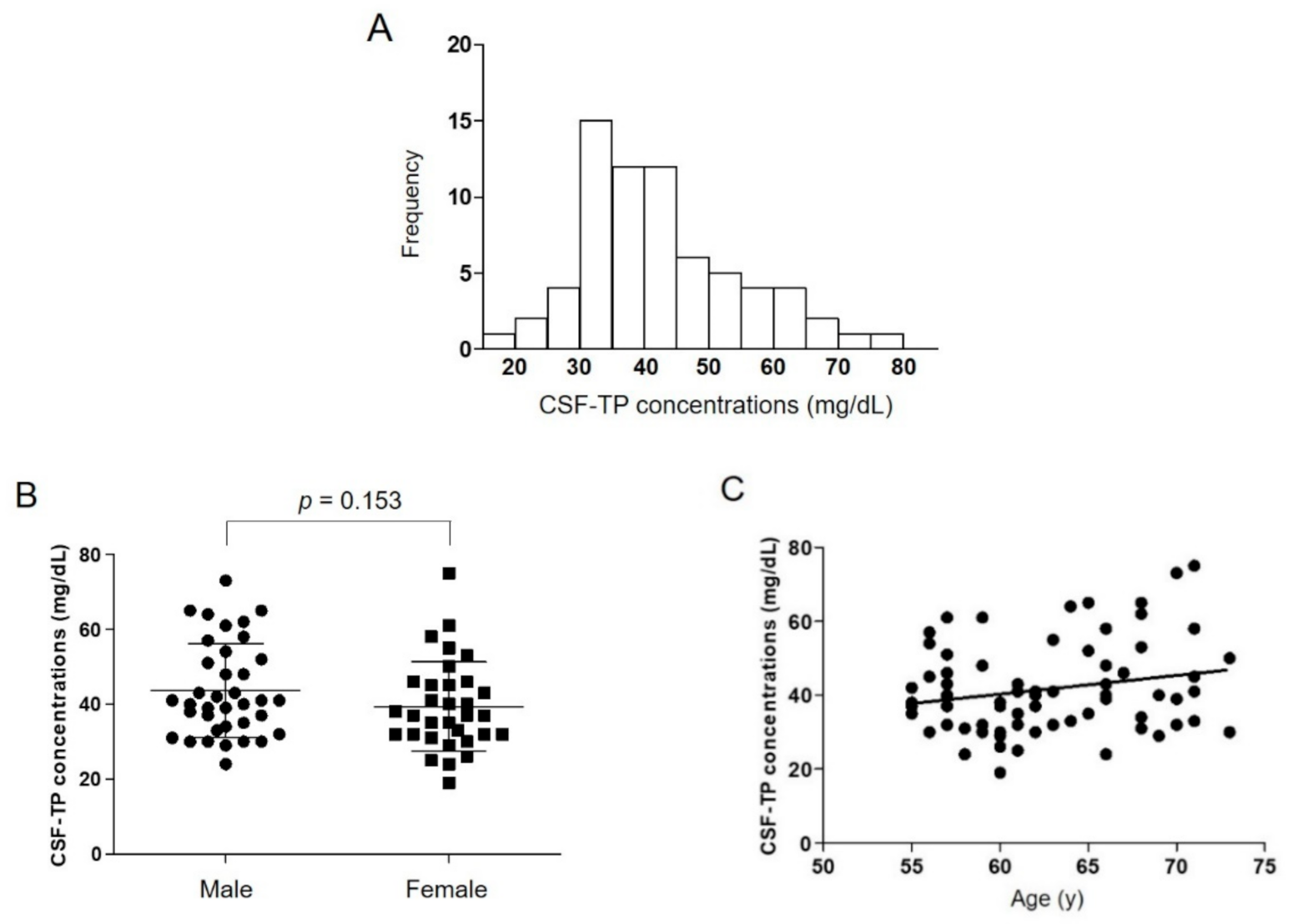
3. Results
4. Discussion
Limitations and Strengths of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Breiner, A.; Moher, D.; Brooks, J.; Cheng, W.; Hegen, H.; Deisenhammer, F.; McCudden, C.R.; Bourque, P.R. Adult CSF total protein upper reference limits should be age-partitioned and significantly higher than 0.45 g/L: A systematic review. J. Neurol. 2019, 266, 616–624. [Google Scholar] [CrossRef]
- Bourque, P.R.; McCudden, C.R.; Warman-Chardon, J.; Brooks, J.; Hegen, H.; Deisenhammer, F.; Breiner, A. A Survey of Cerebrospinal Fluid Total Protein Upper Limits in Canada: Time for an Update? Can. J. Neurol. Sci. 2019, 46, 283–286. [Google Scholar] [CrossRef]
- Hegen, H.; Auer, M.; Zeileis, A.; Deisenhammer, F. Upper reference limits for cerebrospinal fluid total protein and albumin quotient based on a large cohort of control patients: Implications for increased clinical specificity. Clin. Chem. Lab. Med. 2016, 54, 285–292. [Google Scholar] [CrossRef]
- McCudden, C.R.; Brooks, J.; Figurado, P.; Bourque, P.R. Cerebrospinal fluid total protein reference intervals derived from 20 years of patient data. Clin. Chem. 2017, 63, 1856–1865. [Google Scholar] [CrossRef]
- Bourque, P.R.; Breiner, A.; Moher, D.; Brooks, J.; Hegen, H.; Deisenhammer, F.; McCudden, C.R. Adult CSF total protein: Higher upper reference limits should be considered worldwide. A web-based survey. J. Neurol. Sci. 2019, 396, 48–51. [Google Scholar] [CrossRef]
- Dufour-Rainfray, D.; Beaufils, E.; Vourc’h, P.; Vierron, E.; Mereghetti, L.; Gendrot, C.; Hommet, C.; Andres, C.R.; Guilloteau, D.; Mondon, K. Total protein level in cerebrospinal fluid is stable in elderly adults. J. Am. Geriatr. Soc. 2013, 61, 1819–1821. [Google Scholar] [CrossRef]
- Breiner, A.; Bourque, P.R.; Allen, J.A. Updated cerebrospinal fluid total protein reference values improve chronic inflammatory demyelinating polyneuropathy diagnosis. Muscle Nerve 2019, 60, 180–183. [Google Scholar] [CrossRef]
- Brooks, J.A.; McCudden, C.; Breiner, A.; Bourque, P.R. Causes of albuminocytological dissociation and the impact of age-adjusted cerebrospinal fluid protein reference intervals: A retrospective chart review of 2627 samples collected at tertiary care centre. BMJ Open 2019, 9. [Google Scholar] [CrossRef] [Green Version]
- Hegen, H.; Ladstätter, F.; Bsteh, G.; Auer, M.; Berek, K.; Di Pauli, F.; Walde, J.; Wanschitz, J.; Zinganell, A.; Deisenhammer, F. Cerebrospinal fluid protein in Guillain–Barré syndrome: Need for age-dependent interpretation. Eur. J. Neurol. 2021, 28, 965–973. [Google Scholar] [CrossRef]
- Kanai, M. Kanai’s Manual of Clinical Laboratory Medicine, 34th ed.; KANEHARA & Co., Ltd.: Tokyo, Japan, 2015. (In Japanese) [Google Scholar]
- Takeoka, T.; Gotoh, F.; Furumi, K.; Mori, K. Polyacrylamide-gel disc electrophoresis of native cerebrospinal fluid proteins with special reference to immunoglobulins and some clinical applications. J. Neurol. Sci. 1976, 29, 213–239. [Google Scholar] [CrossRef]
- Hirohata, S.; Inoue, T.; Yamada, A.; Hirose, S.; Miyamoto, T. Quantitation of IgG, IgA and IgM in the cerebrospinal fluid by a solid-phase enzyme-immunoassay. Establishment of normal control values. J. Neurol. Sci. 1984, 63, 101–110. [Google Scholar] [CrossRef]
- Weisner, B.; Bernhardt, W. Protein fractions of lumbar, cisternal, and ventricular cerebrospinal fluid. Separate areas of reference. J. Neurol. Sci. 1978, 37, 205–214. [Google Scholar] [CrossRef]
- Ozarda, Y. Reference intervals: Current status, recent developments and future considerations. Biochem. Med. 2016, 26, 5–16. [Google Scholar] [CrossRef] [Green Version]
- Horn, P.S.; Feng, L.; Li, Y.; Pesce, A.J. Effect of outliers and nonhealthy individuals on reference interval estimation. Clin. Chem. 2001, 47, 2137–2145. [Google Scholar] [CrossRef] [Green Version]
- Breebaart, K.; Becker, H.; Jongebloed, F.A. Investigation of reference values of components of cerebrospinal fluid. J. Clin. Chem. Clin. Biochem. 1978, 16, 561–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atack, J.R.; May, C.; Kaye, J.A.; Kay, A.D.; Rapoport, S.I. Cerebrospinal fluid cholinesterases in aging and in dementia of the alzheimer type. Ann. Neurol. 1988, 23, 161–167. [Google Scholar] [CrossRef]
- May, C.; Kaye, J.A.; Atack, J.R.; Schapiro, M.B.; Friedland, R.P.; Rapoport, S.I. Cerebrospinal fluid production is reduced in healthy aging. Neurology 1990, 40, 500–503. [Google Scholar] [CrossRef]
- Garton, M.J.; Keir, G.; Lakshmi, M.V.; Thompson, E.J. Age-related changes in cerebrospinal fluid protein concentrations. J. Neurol. Sci. 1991, 104, 74–80. [Google Scholar] [CrossRef]
- Brettschneider, J.; Claus, A.; Kassubek, J.; Tumani, H. Isolated blood-cerebrospinal fluid barrier dysfunction: Prevalence and associated diseases. J. Neurol. 2005, 252, 1067–1073. [Google Scholar] [CrossRef]
- Ebert, S.; Phillips, D.J.; Jenzewski, P.; Nau, R.; O’Connor, A.E.; Michel, U. Activin A concentrations in human cerebrospinal fluid are age-dependent and elevated in meningitis. J. Neurol. Sci. 2006, 250, 50–57. [Google Scholar] [CrossRef]
- Johansson, P.A.; Dziegielewska, K.M.; Liddelow, S.A.; Saunders, N.R. The blood-CSF barrier explained: When development is not immaturity. BioEssays 2008, 30, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.S.; Ebberson, J.; Kestenbaum, L.A.; Hodinka, R.L.; Zorc, J.J. Age-specific reference values for cerebrospinal fluid protein concentration in neonates and young infants. J. Hosp. Med. 2011, 6, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Kahlmann, V.; Roodbol, J.; van Leeuwen, N.; Ramakers, C.R.B.; van Pelt, D.; Neuteboom, R.F.; Catsman-Berrevoets, C.E.; de Wit, M.C.Y.; Jacobs, B.C. Validated age-specific reference values for CSF total protein levels in children. Eur. J. Paediatr. Neurol. 2017, 21, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Saunders, N.R.; Liddelow, S.A.; Dziegielewska, K.M. Barrier mechanisms in the developing brain. Front. Pharmacol. 2012, 3, 46. [Google Scholar] [CrossRef] [Green Version]
- Blennow, K.; Fredman, P.; Wallin, A.; Gottfries, C.G.; Långström, G.; Svennerholm, L. Protein analyses in cerebrospinal fluid. I. Influence of concentration gradients for proteins on cerebrospinal fluid/serum albumin ratio. Eur. Neurol. 1993, 33, 126–128. [Google Scholar] [CrossRef]

{kind=link}
| Mean (SD) | 2.5th Percentile | 97.5th Percentile | |
|---|---|---|---|
| CSF-TP (mg/dL) | |||
| All participants (n = 69) | 41.7 (12.3) | 22.5 | 73.2 |
| Male (n = 37) | 43.7 (12.5) | 24.4 | 72.5 |
| Female (n = 32) | 39.4 (11.9) | 19.0 | 75.0 |
| CSF-glucose (mg/dL) | |||
| All participants (n = 69) | 59.9 (5.5) | 49.8 | 72.0 |
| Male (n = 37) | 61.1 (5.1) | 49.2 | 72.8 |
| Female (n = 32) | 58.6 (5.7) | 50.0 | 72.0 |
| Age Group | 55–64, Year (n = 42) Mean (SD) | ≥65, Year (n = 27) Mean (SD) | p-Value a |
|---|---|---|---|
| CSF-TP (mg/dL) | 39.0 (10.5) | 45.9 (13.9) | 0.044 |
| CSF-glucose (mg/dL) | 60.3 (6.1) | 59.4 (4.5) | 0.658 |
| Historical Controls | Setting | Subject | Mean Age (Range), year | Number | Mean CSF-TP (SD), mg/dL | p-Value a |
|---|---|---|---|---|---|---|
| Hirohata et al. 1984 [12] | Japan | Patients with no neurological disease | 34.2 (13–57) | 30 | 29.9 (9.0) | <0.001 |
| Breebaart et al. 1978 [16] | Netherlands | Patients with no neurological disease | 38 | 139 | 31 (18) | <0.001 |
| Takeoka et al. 1976 [11] | Japan | Patients with no neurological disease | 41.0 (18–77) | 27 | 30.0 (6.9) | <0.001 |
| Hegen et al. 2016 [3] | Austria | Patients with no neurological disease | 42.1 (18–80) | 332 | 40.2 (12.6) | 0.367 |
| McCudden et al. 2017 [4] | Canada | Female patients with no neurological disease | 43 (18–97) | 3804 | 32 (10) | <0.001 |
| Male patients with no neurological disease | 44 (18–94) | 2264 | 38 (11) | 0.006 | ||
| Atack et al. 1988 [17] | USA | Healthy normal subjects | 48.1 (20–86) | 26 | 49 (10) | 0.069 |
| Dufour-Rainfray et al. 2013 [6] | France | CSF samples with cellularity and high glucose levels were excluded | (50–100) | 1192 | 48 (24) | 0.031 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshihara, T.; Zaitsu, M.; Ito, K.; Hanada, R.; Chung, E.; Yazawa, R.; Sakata, Y.; Furusho, K.; Tsukikawa, H.; Chiyoda, T.; et al. Cerebrospinal Fluid Protein Concentration in Healthy Older Japanese Volunteers. Int. J. Environ. Res. Public Health 2021, 18, 8683. https://doi.org/10.3390/ijerph18168683
Yoshihara T, Zaitsu M, Ito K, Hanada R, Chung E, Yazawa R, Sakata Y, Furusho K, Tsukikawa H, Chiyoda T, et al. Cerebrospinal Fluid Protein Concentration in Healthy Older Japanese Volunteers. International Journal of Environmental Research and Public Health. 2021; 18(16):8683. https://doi.org/10.3390/ijerph18168683
Chicago/Turabian StyleYoshihara, Tatsuya, Masayoshi Zaitsu, Kazuya Ito, Ryuzo Hanada, Eunhee Chung, Rie Yazawa, Yukikuni Sakata, Koki Furusho, Hiroshi Tsukikawa, Takeshi Chiyoda, and et al. 2021. "Cerebrospinal Fluid Protein Concentration in Healthy Older Japanese Volunteers" International Journal of Environmental Research and Public Health 18, no. 16: 8683. https://doi.org/10.3390/ijerph18168683
APA StyleYoshihara, T., Zaitsu, M., Ito, K., Hanada, R., Chung, E., Yazawa, R., Sakata, Y., Furusho, K., Tsukikawa, H., Chiyoda, T., Matsuki, S., & Irie, S. (2021). Cerebrospinal Fluid Protein Concentration in Healthy Older Japanese Volunteers. International Journal of Environmental Research and Public Health, 18(16), 8683. https://doi.org/10.3390/ijerph18168683