
Colorectal Cancer Risk in Patients with Hemorrhoids: A 10-Year Population-Based Retrospective Cohort Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Database
2.2. Study Population and Comorbidity
2.3. Statistical Analysis
3. Results
3.1. Demography
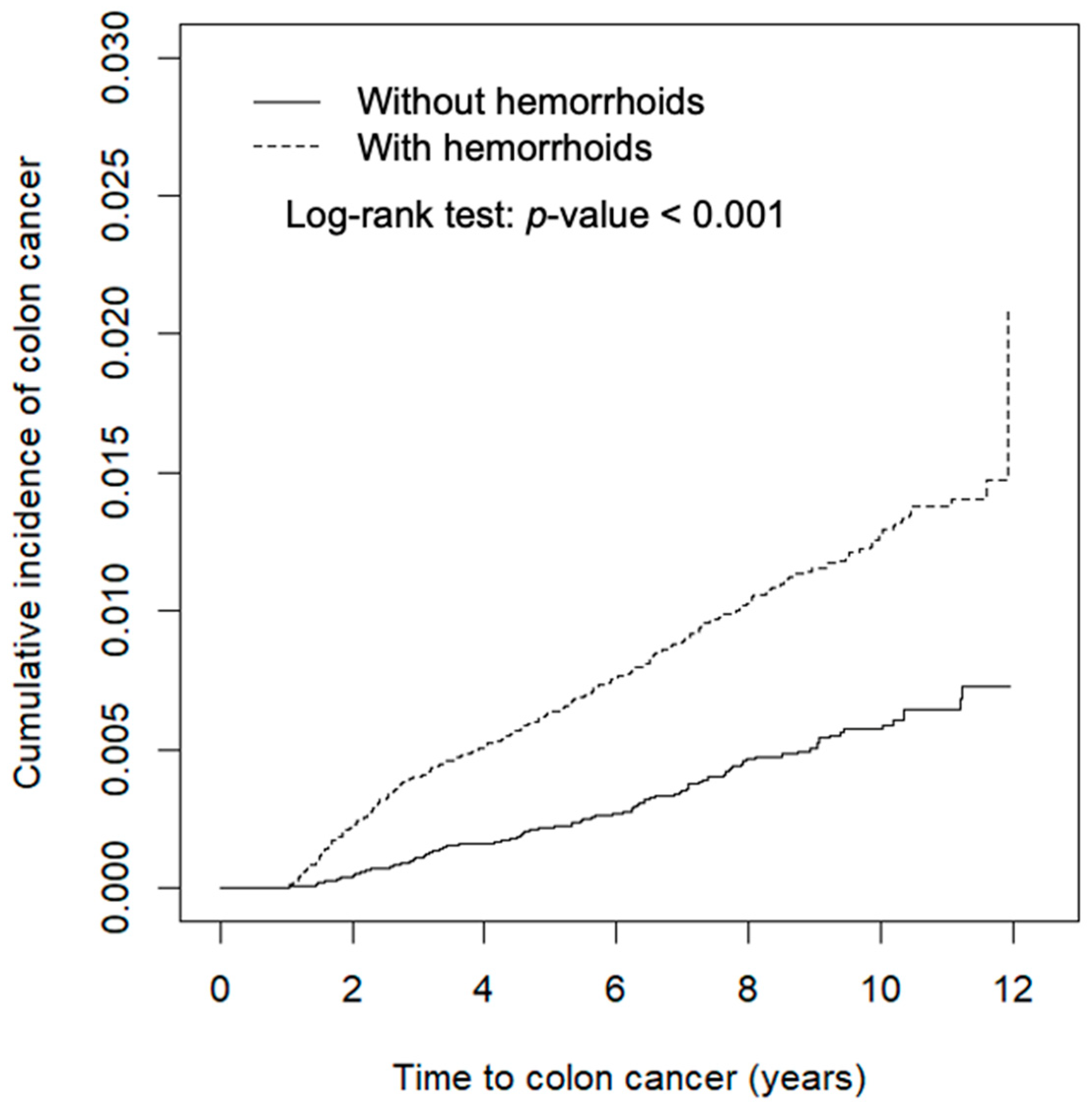
3.2. Higher Incidence Rates of CRC in Hemorrhoids Patients
3.3. Subgroup Analysis of Demographic Aspects and Comorbidities
3.4. Relevance of Tumor Site and Hemorrhoids
4. Discussion
5. Advantages and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Turner, N.D.; Lloyd, S.K. Association between red meat consumption and colon cancer: A systematic review of experimental results. Exp. Biol. Med. 2017, 242, 813–839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailie, L.; Loughrey, M.B.; Coleman, H.G. Lifestyle risk factors for serrated colorectal polyps: A systematic review and meta-analysis. Gastroenterology 2017, 152, 92–104. [Google Scholar] [CrossRef] [Green Version]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobs, D. Hemorrhoids. N. Engl. J. Med. 2014, 371, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Lohsiriwat, V. Treatment of hemorrhoids: A coloproctologist’s view. World J. Gastroenterol. 2015, 21, 9245–9252. [Google Scholar] [CrossRef]
- Sanchez, C.; Chinn, B.T. Hemorrhoids. Clin. Colon Rectal Surg. 2011, 24, 005–013. [Google Scholar] [CrossRef]
- Sandler, R.S.; Peery, A.F. Rethinking what we know about hemorrhoids. Clin. Gastroenterol. Hepatol. 2019, 17, 8–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Migaly, J.; Sun, Z. Review of hemorrhoid disease: Presentation and management. Clin. Colon Rectal Surg. 2016, 29, 022–029. [Google Scholar] [CrossRef] [Green Version]
- Boyle, T.; Keegel, T.; Bull, F.; Heyworth, J.; Fritschi, L. Physical activity and risks of proximal and distal colon cancers: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2012, 104, 1548–1561. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Administration; Ministry of Health and Welfare, Taiwan. National Health Insurance Research Database, Taiwan. Available online: https://nhird.nhri.org.tw/en/index.html (accessed on 30 May 2014).
- Sherman, R.E.; Anderson, S.A.; Dal Pan, G.J.; Gray, G.W.; Gross, T.; Hunter, N.L.; LaVange, L.; Marinac-Dabic, D.; Marks, P.W.; Robb, M.A.; et al. Real-world evidence—What is it and what can it tell us? N. Engl. J. Med. 2016, 375, 2293–2297. [Google Scholar] [CrossRef] [Green Version]
- Gallimore, A.M.; Godkin, A. Epithelial barriers, microbiota, and colorectal cancer. N. Engl. J. Med. 2013, 368, 282–284. [Google Scholar] [CrossRef] [PubMed]
- Rustgi, A.K. The genetics of hereditary colon cancer. Genes Dev. 2007, 21, 2525–2538. [Google Scholar] [CrossRef] [Green Version]
- Tenesa, A.; Dunlop, M. New insights into the aetiology of colorectal cancer from genome-wide association studies. Nat. Rev. Genet. 2009, 10, 353–358. [Google Scholar] [CrossRef]
- Brenner, H.; Kloor, M.; Pox, C.P. Colorectal cancer. Lancet 2014, 383, 1490–1502. [Google Scholar] [CrossRef]
- Nakao, S.K.; Fassler, S.; Sucandy, I.; Kim, S.; Zebley, D.M. Colorectal cancer following negative colonoscopy: Is 5-year screening the correct interval to recommend? Surg. Endosc. 2012, 27, 768–773. [Google Scholar] [CrossRef] [PubMed]
- Pai, R.K.; Bettington, M.; Srivastava, A.; Rosty, C. An update on the morphology and molecular pathology of serrated colorectal polyps and associated carcinomas. Mod. Pathol. 2019, 32, 1390–1415. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Network. Comprehensive molecular characterization of human colon and rectal cancer. Nature 2012, 487, 330–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giannakis, M.; Mu, X.J.; Shukla, S.A.; Qian, Z.R.; Cohen, O.; Nishihara, R.; Bahl, S.; Cao, Y.; Amin-Mansour, A.; Yamauchi, M.; et al. Genomic correlates of immune-cell infiltrates in colorectal carcinoma. Cell Rep. 2016, 15, 857–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balkwill, F.; Mantovani, A. Inflammation and cancer: Back to virchow? Lancet 2001, 357, 539–545. [Google Scholar] [CrossRef]
- Lai, H.-W.; Loong, C.-C.; Tai, L.-C.; Wu, C.-W.; Lui, W.-Y. Incidence and odds ratio of appendicitis as first manifestation of colon cancer: A retrospective analysis of 1873 patients. J. Gastroenterol. Hepatol. 2006, 21, 1693–1696. [Google Scholar] [CrossRef]
- Yuan-Kun, C.; Tao, Y. Does a decrease of NK cells in the appendix increase the risk of developing colon cancer? Hepato-Gastroenterology 2012, 59, 1819–1821. [Google Scholar] [PubMed]
- Feagins, L.A.; Souza, R.F.; Spechler, S.J. Carcinogenesis in IBD: Potential targets for the prevention of colorectal cancer. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.C.; Shaker, A.; Levin, M.S. Chronic intestinal inflammation: Inflammatory bowel disease and colitis-associated colon cancer. Front. Immunol. 2012, 3, 107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ullman, T.A.; Itzkowitz, S.H. Intestinal inflammation and cancer. Gastroenterology 2011, 140, 1807–1816.e1. [Google Scholar] [CrossRef]
- Grivennikov, S.I. Inflammation and colorectal cancer: Colitis-associated neoplasia. Semin. Immunopathol. 2013, 35, 229–244. [Google Scholar] [CrossRef] [PubMed]
- Grivennikov, S.I.; Wang, K.; Mucida, D.; Stewart, C.A.; Schnabl, B.; Jauch, D.; Taniguchi, K.; Yu, G.Y.; Osterreicher, C.H.; Hung, K.E.; et al. Adenoma-linked barrier defects and microbial products drive IL-23/IL-17-mediated tumour growth. Nature 2012, 491, 254–258. [Google Scholar] [CrossRef] [Green Version]
- Chapelle, N.; Martel, M.; Toes-Zoutendijk, E.; Barkun, A.N.; Bardou, M. Recent advances in clinical practice: Colorectal cancer chemoprevention in the average-risk population. Gut 2020, 69, 2244–2255. [Google Scholar] [CrossRef]
- Drew, D.A.; Chin, S.; Gilpin, K.K.; Parziale, M.; Pond, E.; Schuck, M.M.; Stewart, K.; Flagg, M.; Rawlings, C.A.; Backman, V.; et al. ASPirin intervention for the REDuction of colorectal cancer risk (ASPIRED): A study protocol for a randomized controlled trial. Trials 2017, 18, 50. [Google Scholar] [CrossRef] [Green Version]
- Tseng, H.-F.; Morgenstern, H.; Mack, T.M.; Peters, R.K. Risk factors for anal cancer: Results of a population-based case—Control study. Cancer Causes Control. 2003, 14, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Holly, E.A.; Whittemore, A.S.; Aston, D.A.; Ahn, D.K.; Nickoloff, B.J.; Kristiansen, J.J. Anal cancer incidence: Genital warts, anal fissure or fistula, hemorrhoids, and smoking. J. Natl. Cancer Inst. 1989, 81, 1726–1731. [Google Scholar] [CrossRef]
- Ungerbäck, J.; Belenki, D.; Ul-Hassan, A.J.; Fredrikson, M.; Fransén, K.; Elander, N.; Verma, D.; Söderkvist, P. Genetic variation and alterations of genes involved in NFκB/TNFAIP3- and NLRP3-inflammasome signaling affect susceptibility and outcome of colorectal cancer. Carcinogenesis 2012, 33, 2126–2134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuhara, H.; Steinmaus, C.; Cohen, S.E.; Corley, D.A.; Tei, Y.; Buffler, P.A. Is diabetes mellitus an independent risk factor for colon cancer and rectal cancer? Am. J. Gastroenterol. 2011, 106, 1911–1921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, P.-C.; Hu, Y.-W.; Hung, M.-H.; Chen, C.-C.; Lin, H.-C.; Lee, F.-Y.; Hung, Y.-P.; Su, V.Y.-F.; Yen, S.-H.; Tzeng, C.-H.; et al. The risk of cancer in patients with benign anal lesions: A nationwide population-based study. Am. J. Med. 2013, 126, 1143.e9–1143.e18. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | Hemorrhoids | Standardized Difference § | |
|---|---|---|---|
| No | Yes | ||
| n = 36,864 | n = 36,864 | ||
| Sex | n (%) | n (%) | |
| Female | 17,582 (47.7) | 16,809 (45.6) | 0.04 |
| Male | 19,282 (52.3) | 20,055 (54.4) | 0.04 |
| Age, mean (SD) | 45.8 (15.9) | 46.9 (15.8) | 0.07 |
| Stratified | |||
| ≤49 years | 23,569 (63.9) | 22,622 (61.4) | 0.05 |
| 50–64 | 7836 (21.3) | 8443 (22.9) | 0.04 |
| 65+ | 5459 (14.8) | 5799 (15.7) | 0.03 |
| Comorbidity | |||
| IBD | 566 (1.54) | 585 (1.59) | 0.004 |
| Hypertension | 8580 (23.3) | 9694 (26.3) | 0.07 |
| Diabetes | 2120 (5.75) | 2252 (6.11) | 0.02 |
| Hyperlipidemia | 7206 (19.6) | 7263 (19.7) | 0.004 |
| Stroke | 830 (2.25) | 894 (2.43) | 0.01 |
| Congestive heart failure | 984 (2.67) | 1116 (3.03) | 0.02 |
| Obesity | 173 (0.47) | 193 (0.52) | 0.008 |
| PLA | 22 (0.06) | 23 (0.06) | 0.001 |
| HBV | 1512 (4.10) | 1512 (4.10) | 0.000 |
| HCV | 452 (1.23) | 505 (1.37) | 0.01 |
| COPD | 3879 (10.5) | 3860 (10.5) | 0.002 |
| Alcohol-related illness | 1395 (3.78) | 1397 (3.79) | 0.000 |
| Chronic pancreatitis | 46 (0.12) | 62 (0.17) | 0.01 |
| Variable | Hemorrhoids | Crude HR (95% CI) | Adjusted HR (95% CI) | |||||
|---|---|---|---|---|---|---|---|---|
| No | Yes | |||||||
| Event | PY | Rate # | Event | PY | Rate # | |||
| All | 138 | 255,722 | 0.54 | 337 | 261,466 | 1.29 | 2.39 (1.96, 2.93) * | 2.18 (1.78, 2.67) * |
| Gender | ||||||||
| Female | 52 | 113,232 | 0.46 | 128 | 121,173 | 1.06 | 2.35 (1.71, 3.25) * | 2.19 (1.59, 3.03) * |
| Male | 86 | 142,490 | 0.60 | 209 | 140,293 | 1.49 | 2.38 (1.84, 3.09) * | 2.16 (1.66, 2.80) * |
| Age-stratified | ||||||||
| ≤49 | 23 | 162,628 | 0.14 | 71 | 165,694 | 0.43 | 3.53 (2.15, 5.79) * | 3.53 (2.15, 5.79) * |
| 50–64 | 45 | 55,159 | 0.82 | 113 | 57,499 | 1.97 | 1.95 (1.39, 2.73) * | 1.91 (1.36, 2.68) * |
| 65+ | 70 | 37,935 | 1.85 | 153 | 38,272 | 4.00 | 2.12 (1.58, 2.85) * | 2.06 (1.53, 2.77) * |
| Comorbidity | ||||||||
| No | 54 | 161,577 | 0.33 | 98 | 149,717 | 0.65 | 2.58 (1.79, 3.72) * | 2.53 (1.76, 3.66) * |
| Yes | 84 | 94,145 | 0.89 | 239 | 111,749 | 2.14 | 2.13 (1.67, 2.72) * | 2.09 (1.64, 2.67) * |
| Site of CRC | Hemorrhoids | Crude HR (95% CI) | Adjusted HR (95% CI) | |||
|---|---|---|---|---|---|---|
| No | Yes | |||||
| Event | Rate # | Event | Rate # | |||
| Ascending colon (ICD-9-CM 153.0, 153.4-6) | 13 | 0.05 | 21 | 0.08 | 1.49 (0.75, 2.97) | 1.34 (0.67, 2.69) |
| Transverse colon (ICD-9-CM 153.1) | 4 | 0.02 | 5 | 0.02 | 1.18 (0.32, 4.41) | 1.08 (0.29, 4.07) |
| Descending colon (ICD-9-CM 153.2, 153.7) | 3 | 0.01 | 10 | 0.04 | 3.13 (0.86, 11.4) | 2.83 (0.78, 10.3) |
| Sigmoid colon (ICD-9-CM 153.3) | 21 | 0.08 | 43 | 0.17 | 1.92 (1.14, 3.24) * | 1.79 (1.06, 3.02) * |
| Rectum (ICD-9-CM 154.0-1) | 34 | 0.14 | 86 | 0.33 | 2.40 (1.61, 3.57) ** | 2.20 (1.48, 3.28) ** |
| Other (ICD-9-CM 153.8-9, 154.2-3, 154.8) | 18 | 0.07 | 39 | 0.15 | 2.08 (1.19, 3.64) | 1.86 (1.06, 3.26) |
| Unknown | 45 | 0.17 | 133 | 0.51 | 2.99 (1.97, 3.66) ** | 2.76 (1.85, 3.67) ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, E.-B.; Sung, F.-C.; Lin, C.-L.; Wu, K.-L.; Chen, K.-B. Colorectal Cancer Risk in Patients with Hemorrhoids: A 10-Year Population-Based Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 8655. https://doi.org/10.3390/ijerph18168655
Wu E-B, Sung F-C, Lin C-L, Wu K-L, Chen K-B. Colorectal Cancer Risk in Patients with Hemorrhoids: A 10-Year Population-Based Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(16):8655. https://doi.org/10.3390/ijerph18168655
Chicago/Turabian StyleWu, En-Bo, Fung-Chang Sung, Cheng-Li Lin, Kuen-Lin Wu, and Kuen-Bao Chen. 2021. "Colorectal Cancer Risk in Patients with Hemorrhoids: A 10-Year Population-Based Retrospective Cohort Study" International Journal of Environmental Research and Public Health 18, no. 16: 8655. https://doi.org/10.3390/ijerph18168655
APA StyleWu, E.-B., Sung, F.-C., Lin, C.-L., Wu, K.-L., & Chen, K.-B. (2021). Colorectal Cancer Risk in Patients with Hemorrhoids: A 10-Year Population-Based Retrospective Cohort Study. International Journal of Environmental Research and Public Health, 18(16), 8655. https://doi.org/10.3390/ijerph18168655