
Impact of Sexual Activity on the Risk of Male Genital Tumors: A Systematic Review of the Literature

 , , ,
, , ,  ,
,  ,
,  ,
, 
Abstract
1. Introduction
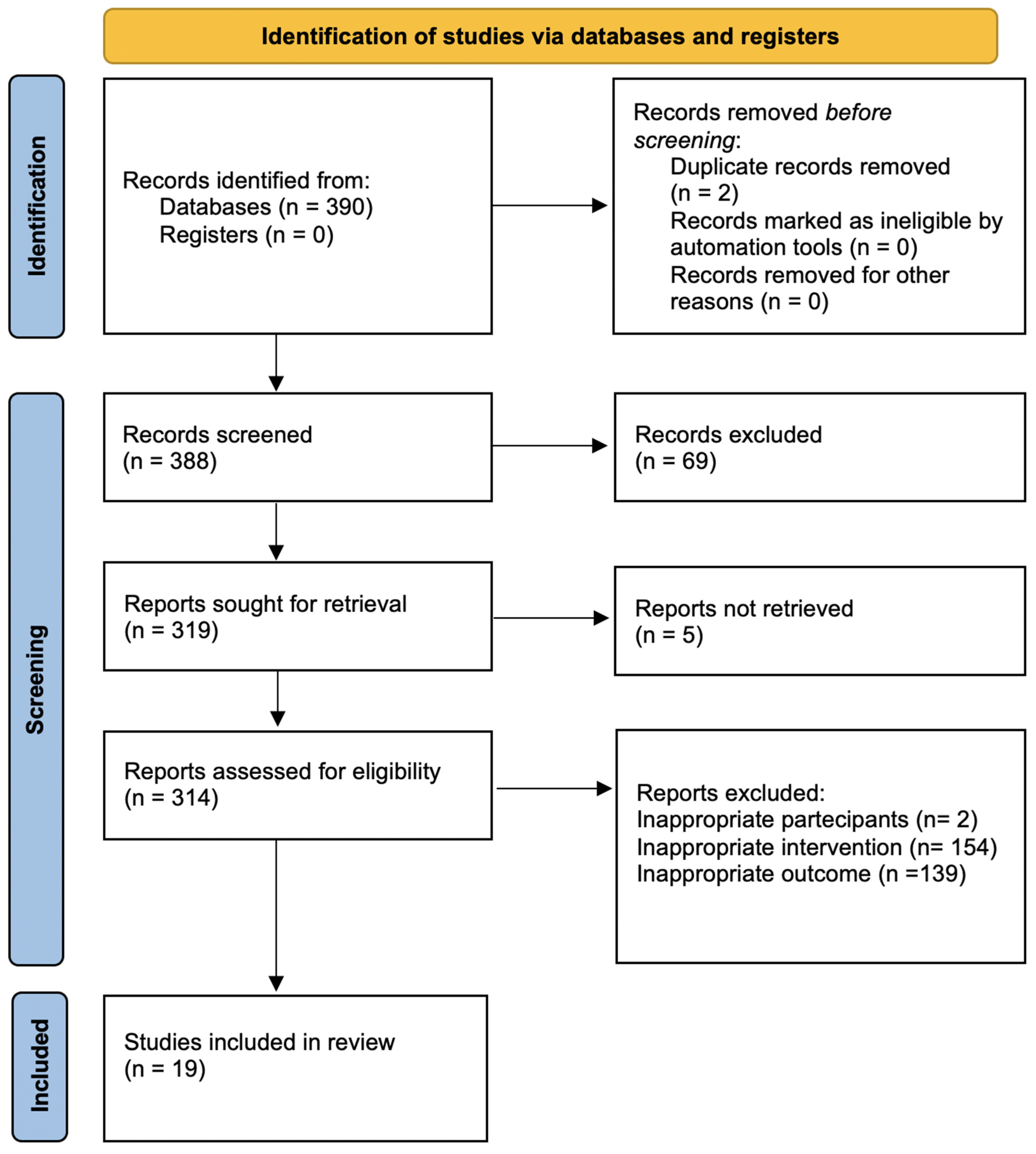
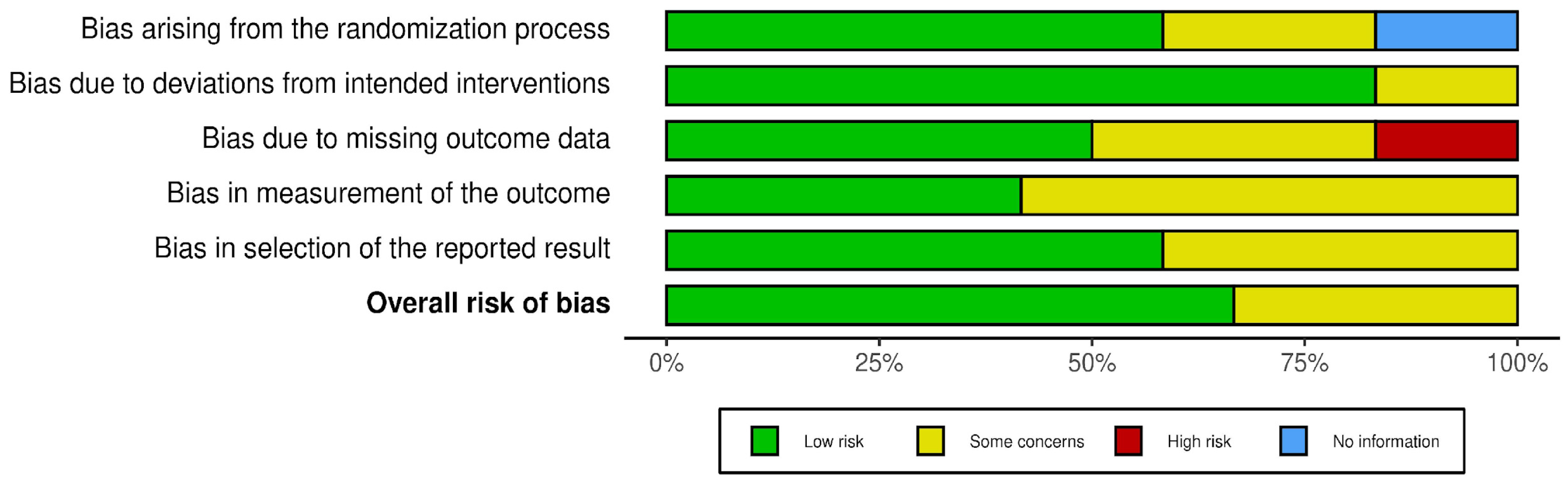
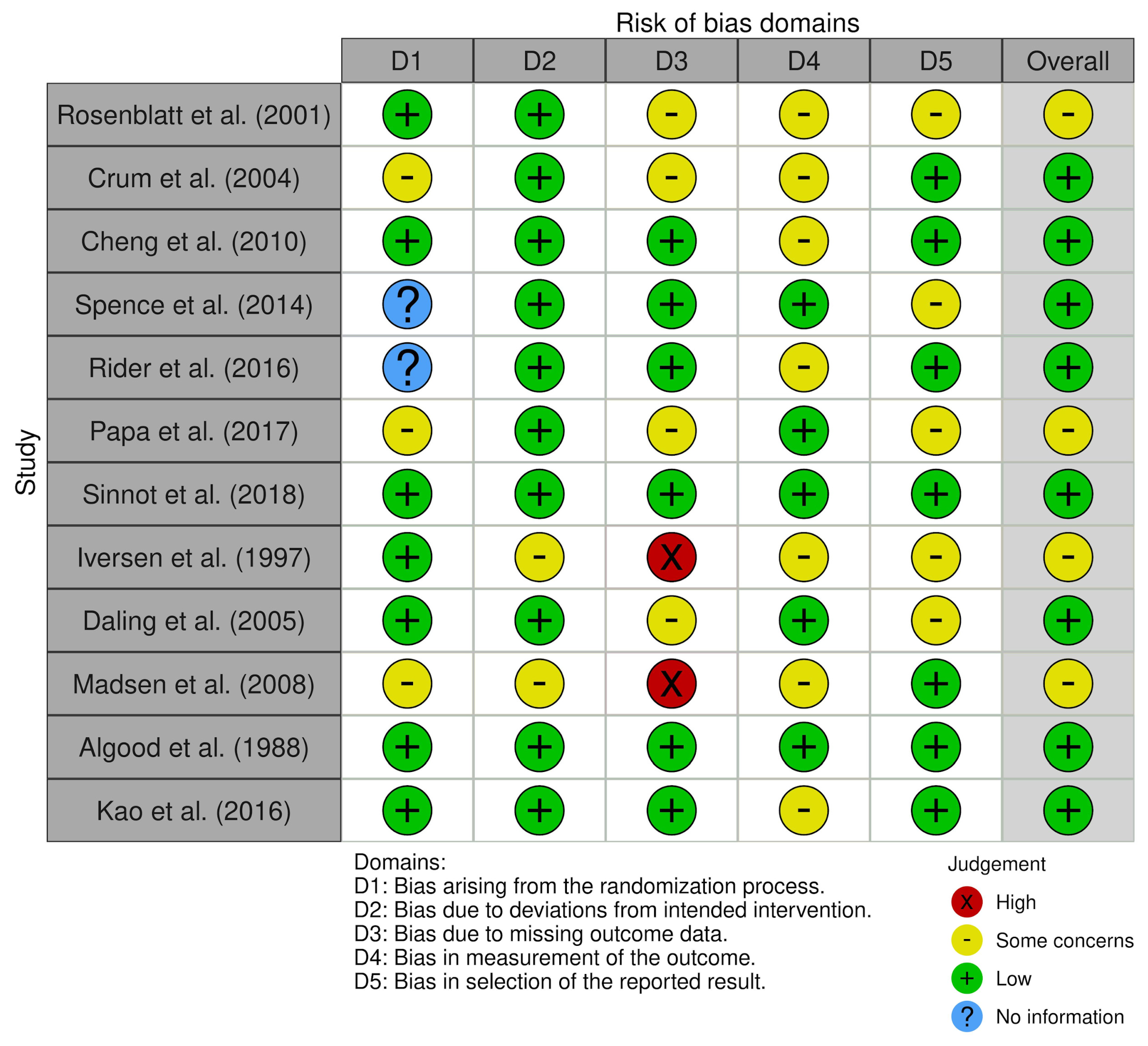
2. Materials and Methods
3. Results
3.1. Prostate Cancer (PCa)
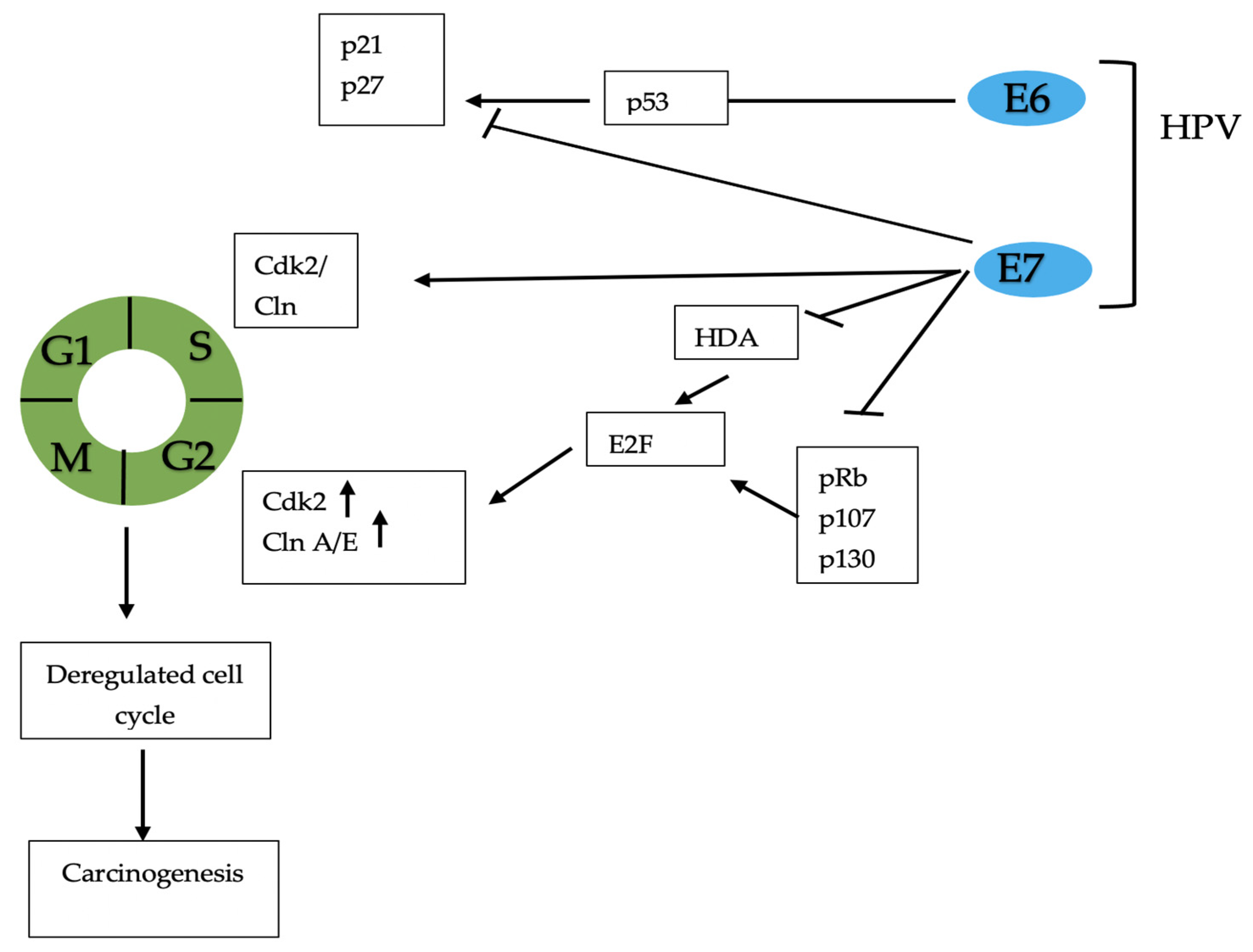
3.2. Penile Cancer (PC)
3.3. Testicular Cancer (TC)
4. Prevention
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ventriglio, A.; Bhugra, D. Sexuality in the 21st Century: Sexual Fluidity. East Asian Arch. Psychiatry 2019, 29, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; Yang, L.; Xu, T.; Cavazos-Rehg, P.A.; Liu, Q.; McDermott, D.; Veronese, N.; Waldhoer, T.; Ilie, P.C.; Shariat, S.F.; et al. Trends in Sexual Activity and Associations with All-Cause and Cause-Specific Mortality Among US Adults. J. Sex. Med. 2020, 17, 1903–1913. [Google Scholar] [CrossRef]
- De Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef]
- Grivennikov, S.I.; Greten, F.; Karin, M. Immunity, Inflammation, and Cancer. Cell 2010, 140, 883–899. [Google Scholar] [CrossRef]
- Elinav, E.; Nowarski, R.; Thaiss, C.A.; Hu, B.; Jin, C.; Flavell, R.A. Inflammation-induced cancer: Crosstalk between tumours, immune cells and microorganisms. Nat. Rev. Cancer 2013, 13, 759–771. [Google Scholar] [CrossRef] [PubMed]
- Tewari, A.K.; Stockert, J.A.; Yadav, S.S.; Yadav, K.K.; Khan, I. Inflammation and Prostate Cancer. Chem. Biol. Pteridines Folates 2018, 1095, 41–65. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.D.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inf. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.-T.; Zhang, Y.; Kwong, J.S.; Zhang, C.; Li, S.; Sun, F.; Niu, Y.; Du, L. The methodological quality assessment tools for preclinical and clinical studies, systematic review and meta-analysis, and clinical practice guideline: A systematic review. J. Evid.-Based Med. 2015, 8, 2–10. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef]
- Shea, B.J.; Reeves, B.C.; Wells, G.; Thuku, M.; Hamel, C.; Moran, J.; Moher, D.; Tugwell, P.; Welch, V.; Kristjansson, E.; et al. AMSTAR 2: A critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ 2017, 358, j4008. [Google Scholar] [CrossRef] [PubMed]
- Spence, A.R.; Rousseau, M.-C.; Parent, M.É. Sexual partners, sexually transmitted infections, and prostate cancer risk. Cancer Epidemiol. 2014, 38, 700–707. [Google Scholar] [CrossRef]
- Rider, J.R.; Wilson, K.M.; Sinnott, J.A.; Kelly, R.S.; Mucci, L.A.; Giovannucci, E.L. Ejaculation Frequency and Risk of Prostate Cancer: Updated Results with an Additional Decade of Follow-up. Eur. Urol. 2016, 70, 974–982. [Google Scholar] [CrossRef] [PubMed]
- Papa, N.P.; MacInnis, R.; English, D.R.; Bolton, D.; Davis, I.D.; Lawrentschuk, N.; Millar, J.; Pedersen, J.; Severi, G.; Southey, M.C.; et al. Ejaculatory frequency and the risk of aggressive prostate cancer: Findings from a case-control study. Urol. Oncol. Semin. Orig. Investig. 2017, 35, 530.e7–530.e13. [Google Scholar] [CrossRef]
- Sinnott, J.A.; Brumberg, K.; Wilson, K.M.; Ebot, E.M.; Giovannucci, E.L.; Mucci, L.A.; Rider, J.R. Differential Gene Expression in Prostate Tissue According to Ejaculation Frequency. Eur. Urol. 2018, 74, 545–548. [Google Scholar] [CrossRef] [PubMed]
- Rosenblatt, K.A.; Wicklund, K.G.; Stanford, J.L. Sexual factors and the risk of prostate cancer. Am. J. Epidemiol. 2001, 153, 1152–1158. [Google Scholar] [CrossRef][Green Version]
- Jian, Z.; Ye, D.; Chen, Y.; Li, H.; Wang, K. Sexual Activity and Risk of Prostate Cancer: A Dose–Response Meta-Analysis. J. Sex. Med. 2018, 15, 1300–1309. [Google Scholar] [CrossRef]
- Cheng, I.; Witte, J.S.; Jacobsen, S.; Haque, R.; Quinn, V.P.; Quesenberry, C.P.; Caan, B.; Eeden, S.K.V.D. Prostatitis, Sexually Transmitted Diseases, and Prostate Cancer: The California Men’s Health Study. PLoS ONE 2010, 5, e8736. [Google Scholar] [CrossRef]
- Sun, D.; Cao, M.; Li, H.; Ren, J.; Shi, J.; Li, N.; Chen, W. Risk of prostate cancer in men with HIV/AIDS: A systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2021, 24, 24–34. [Google Scholar] [CrossRef]
- Crum, N.F.; Spencer, C.R.; Amling, C.L. Prostate carcinoma among men with human immunodeficiency virus infection. Cancer 2004, 101, 294–299. [Google Scholar] [CrossRef]
- Daling, J.R.; Madeleine, M.M.; Johnson, L.G.; Schwartz, S.; Shera, K.A.; Wurscher, M.A.; Carter, J.J.; Porter, P.L.; Galloway, D.A.; McDougall, J.K.; et al. Penile cancer: Importance of circumcision, human papillomavirus and smoking inin situ and invasive disease. Int. J. Cancer 2005, 116, 606–616. [Google Scholar] [CrossRef] [PubMed]
- Mirghani, H.; Sturgis, E.M.; Aupérin, A.; Monsonego, J.; Blanchard, P. Is there an increased risk of cancer among spouses of patients with an HPV-related cancer: A systematic review. Oral Oncol. 2017, 67, 138–145. [Google Scholar] [CrossRef]
- Iversen, T.H.; Tretli, S.; Johansen, A.; Holte, T. Squamous cell carcinoma of the penis and of the cervix, vulva and vagina in spouses: Is there any relationship? An epidemiological study from Norway, 1960–1992. Br. J. Cancer 1997, 76, 658–660. [Google Scholar] [CrossRef][Green Version]
- Madsen, B.S.; Brule, A.J.V.D.; Jensen, H.L.; Wohlfahrt, J.; Frisch, M. Risk Factors for Squamous Cell Carcinoma of the Penis--Population-Based Case-Control Study in Denmark. Cancer Epidemiol. Biomark. Prev. 2008, 17, 2683–2691. [Google Scholar] [CrossRef] [PubMed]
- Lekoane, K.M.B.; Kuupiel, D.; Mashamba-Thompson, T.P.; Ginindza, T.G. The interplay of HIV and human papillomavirus-related cancers in sub-Saharan Africa: Scoping review. Syst. Rev. 2020, 9, 1–13. [Google Scholar] [CrossRef]
- Algood, C.B.; Newell, G.R.; Johnson, D.E. Viral Etiology of Testicular Tumors. J. Urol. 1988, 139, 308–310. [Google Scholar] [CrossRef]
- Garolla, A.; Vitagliano, A.; Muscianisi, F.; Valente, U.; Ghezzi, M.; Andrisani, A.; Ambrosini, G.; Foresta, C. Role of Viral Infections in Testicular Cancer Etiology: Evidence from a Systematic Review and Meta-Analysis. Front. Endocrinol. 2019, 10, 1–12. [Google Scholar] [CrossRef]
- Grulich, A.E.; van Leeuwen, M.; Falster, M.; Vajdic, C. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: A meta-analysis. Lancet 2007, 370, 59–67. [Google Scholar] [CrossRef]
- Kao, L.-T.; Lin, H.-C.; Chung, S.-D.; Huang, C.-Y. Association between Testicular Cancer and Epididymoorchitis: A Population-Based Case-Control Study. Sci. Rep. 2016, 6, 23079. [Google Scholar] [CrossRef] [PubMed]
- Trabert, B.; Graubard, B.I.; Erickson, R.L.; McGlynn, K.A. Childhood infections, orchitis and testicular germ cell tumours: A report from the STEED study and a meta-analysis of existing data. Br. J. Cancer 2012, 106, 1331–1334. [Google Scholar] [CrossRef] [PubMed]
- Capece, M.; Creta, M.; Calogero, A.; La Rocca, R.; Napolitano, L.; Barone, B.; Sica, A.; Fusco, F.; Santangelo, M.; Dodaro, C.; et al. Does Physical Activity Regulate Prostate Carcinogenesis and Prostate Cancer Outcomes? A Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 1441. [Google Scholar] [CrossRef] [PubMed]
- Maggi, M.; Gentilucci, A.; Salciccia, S.; Gatto, A.; Gentile, V.; Colarieti, A.; Von Heland, M.; Busetto, G.M.; Del Giudice, F.; Sciarra, A. Psychological impact of different primary treatments for prostate cancer: A critical analysis. Andrology 2019, 51, e13157. [Google Scholar] [CrossRef]
- Tarantino, G.; Crocetto, F.; Di Vito, C.; Martino, R.; Pandolfo, S.D.; Creta, M.; Aveta, A.; Buonerba, C.; Imbimbo, C. Clinical factors affecting prostate-specific antigen levels in prostate cancer patients undergoing radical prostatectomy: A retrospective study. Futur. Sci. OA 2021, 7, FSO643. [Google Scholar] [CrossRef] [PubMed]
- Jsselmuiden, C.B.I.; Faden, R.R. The New England Journal of Medicine. 1956. Available online: https://www.massmed.org/About/MMS-Leadership/History/Docendo-Discimus-(PDF)/ (accessed on 12 March 2021).
- Rosser, B.S.; Hunt, S.; Capistrant, B.; Kohli, N.; Konety, B.; Mitteldorf, D.; Ross, M.; Talley, K.; West, W. Understanding Prostate Cancer in Gay, Bisexual, and Other Men Who Have Sex with Men and Transgender Women: A Review of the Literature. In Gay & Bisexual Men Living with Prostate Cancer; Harrington New York: New York, NY, USA, 2018; pp. 12–37. [Google Scholar]
- Isaacs, J.T. Prostatic structure and function in relation to the etiology of prostatic cancer. Prostate 1983, 4, 351–366. [Google Scholar] [CrossRef]
- Crocetto, F.; Boccellino, M.; Barone, B.; Di Zazzo, E.; Sciarra, A.; Galasso, G.; Settembre, G.; Quagliuolo, L.; Imbimbo, C.; Boffo, S.; et al. The Crosstalk between Prostate Cancer and Microbiota Inflammation: Nutraceutical Products Are Useful to Balance This Interplay? Nutrition 2020, 12, 2648. [Google Scholar] [CrossRef]
- Costello, L.; Franklin, R. The Intermediary Metabolism of the Prostate: A Key to Understanding the Pathogenesis and Progression of Prostate Malignancy. Oncology 2000, 59, 269–282. [Google Scholar] [CrossRef]
- Lian, W.-Q.; Luo, F.; Song, X.-L.; Lu, Y.-J.; Zhao, S.-C. Gonorrhea and Prostate Cancer Incidence: An Updated Meta-Analysis of 21 Epidemiologic Studies. Med. Sci. Monit. 2015, 21, 1895–1903. [Google Scholar] [CrossRef]
- Goedert, J.J.; Purdue, M.; McNeel, T.S.; McGlynn, K.A.; Engels, E.A. Risk of Germ Cell Tumors among Men with HIV/Acquired Immunodeficiency Syndrome. Cancer Epidemiol. Biomark. Prev. 2007, 16, 1266–1269. [Google Scholar] [CrossRef]
- Hessol, N.A.; Pipkin, S.; Schwarcz, S.; Cress, R.D.; Bacchetti, P.; Scheer, S. The Impact of Highly Active Antiretroviral Therapy on Non-AIDS-Defining Cancers among Adults with AIDS. Am. J. Epidemiol. 2007, 165, 1143–1153. [Google Scholar] [CrossRef] [PubMed]
- Arbyn, M.; De Sanjosé, S.; Saraiya, M.; Sideri, M.; Palefsky, J.; Lacey, C.; Gillison, M.; Bruni, L.; Ronco, G.; Wentzensen, N.; et al. EUROGIN 2011 roadmap on prevention and treatment of HPV-related disease. Int. J. Cancer 2012, 131, 1969–1982. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, M.; Castle, P.E.; Jeronimo, J.; Rodriguez, A.C.; Wacholder, S. Human papillomavirus and cervical cancer. Lancet 2007, 370, 890–907. [Google Scholar] [CrossRef]
- Scully, C. Oral squamous cell carcinoma; from an hypothesis about a virus, to concern about possible sexual transmission. Oral Oncol. 2002, 38, 227–234. [Google Scholar] [CrossRef]
- Bleeker, M.; Heideman, D.A.M.; Snijders, P.J.F.; Horenblas, S.; Dillner, J.; Meijer, C.J.L.M. Penile cancer: Epidemiology, pathogenesis and prevention. World J. Urol. 2009, 27, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Buitrago-Pérez, A.; Garaulet, G.; Vázquez-Carballo, A.; Paramio, J.M.; García-Escudero, R. Molecular Signature of HPV-Induced Carcinogenesis: pRb, p53 and Gene Expression Profiling. Curr. Genom. 2009, 10, 26–34. [Google Scholar] [CrossRef]
- Glenn, W.K.; Ngan, C.C.; Amos, T.G.; Edwards, R.J.; Swift, J.; Lutze-Mann, L.; Shang, F.; Whitaker, N.J.; Lawson, J.S. High risk human papilloma viruses (HPVs) are present in benign prostate tissues before development of HPV associated prostate cancer. Infect. Agents Cancer 2017, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Yin, B.; Liu, W.; Yue, C.; Liu, C.; Chen, Y.; Duan, X.; Liao, Z.; Chen, Y.; Wang, X.; Pan, X.; et al. Association between human papillomavirus and prostate cancer: A meta-analysis. Oncol. Lett. 2017, 14, 1855–1865. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, G.C.; Rocha, R.M.; Zequi, S.C.; Cunha, I.W.; Soares, F.A. Penile Cancer: Epidemiology and Treatment. Curr. Oncol. Rep. 2011, 13, 231–239. [Google Scholar] [CrossRef]
- Parkin, D.M.; Bray, F. Chapter 2: The burden of HPV-related cancers. Vaccine 2006, 24, S11–S25. [Google Scholar] [CrossRef] [PubMed]
- Calmon, M.F.; Mota, M.T.; Vassallo, J.; Rahal, P. Penile Carcinoma: Risk Factors and Molecular Alterations. Sci. World J. 2011, 11, 269–282. [Google Scholar] [CrossRef]
- Chipollini, J.; Tang, D.H.; Sharma, P.; Spiess, P.E. National Trends and Predictors of Organ-sparing for Invasive Penile Tumors: Expanding the Therapeutic Window. Clin. Genitourin. Cancer 2018, 16, e383–e389. [Google Scholar] [CrossRef]
- Kieffer, J.; Djajadiningrat, R.S.; Van Muilekom, E.A.; Graafland, N.M.; Horenblas, S.; Aaronson, N.K. Quality of Life for Patients Treated for Penile Cancer. J. Urol. 2014, 192, 1105–1110. [Google Scholar] [CrossRef] [PubMed]
- Barocas, D.A.; Chang, S.S. Penile Cancer: Clinical Presentation, Diagnosis, and Staging. Urol. Clin. N. Am. 2010, 37, 343–352. [Google Scholar] [CrossRef]
- Muñoz, N.; Bosch, F.X.; De Sanjosé, S.; Herrero, R.; Castellsagué, X.; Shah, K.V.; Snijders, P.J.; Meijer, C.J. Epidemiologic Classification of Human Papillomavirus Types Associated with Cervical Cancer. N. Engl. J. Med. 2003, 348, 518–527. [Google Scholar] [CrossRef] [PubMed]
- Diorio, G.J.; Giuliano, A.R. The Role of Human Papilloma Virus in Penile Carcinogenesis and Preneoplastic Lesions. Urol. Clin. N. Am. 2016, 43, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Flaherty, A.; Kim, T.; Giuliano, A.; Magliocco, A.; Hakky, T.S.; Pagliaro, L.C.; Spiess, P.E. Implications for human papillomavirus in penile cancer. Urol. Oncol. Semin. Orig. Investig. 2014, 32, 53.e1–53.e8. [Google Scholar] [CrossRef]
- De Bruijn, R.E.; Heideman, D.A.; Kenter, G.G.; Van Beurden, M.; Van Tinteren, H.; Horenblas, S. Patients with penile cancer and the risk of (pre)malignant cervical lesions in female partners: A retrospective cohort analysis. BJU Int. 2013, 112, 905–908. [Google Scholar] [CrossRef]
- Ghosn, J.; Taiwo, B.; Seedat, S.; Autran, B.; Katlama, C. HIV. Lancet 2018, 392, 685–697. [Google Scholar] [CrossRef]
- Onywera, H.; Williamson, A.-L.; Ponomarenko, J.; Meiring, T.L. The Penile Microbiota in Uncircumcised and Circumcised Men: Relationships With HIV and Human Papillomavirus Infections and Cervicovaginal Microbiota. Front. Med. 2020, 7, 383. [Google Scholar] [CrossRef] [PubMed]
- Morris, B.J. Why circumcision is a biomedical imperative for the 21st century. BioEssays 2007, 29, 1147–1158. [Google Scholar] [CrossRef] [PubMed]
- Morris, B.J.; Krieger, J.N. Penile inflammatory skin disorders and the preventive role of circumcision. Int. J. Prev. Med. 2017, 8, 32. [Google Scholar] [CrossRef]
- Han, J.J.; Beltran, T.H.; Song, J.W.; Klaric, J.; Choi, Y.S. Prevalence of Genital Human Papillomavirus Infection and Human Papillomavirus Vaccination Rates among US Adult Men. JAMA Oncol. 2017, 3, 810–816. [Google Scholar] [CrossRef] [PubMed]
- Dunne, E.F.; Nielson, C.M.; Stone, K.M.; Markowitz, L.E.; Giuliano, A.R. Prevalence of HPV Infection among Men: A Systematic Review of the Literature. J. Infect. Dis. 2006, 194, 1044–1057. [Google Scholar] [CrossRef]
- Barnholtz-Sloan, J.; Maldonado, J.L.; Pow-Sang, J.; Guiliano, A.R. Incidence trends in primary malignant penile cancer. Urol. Oncol. Semin. Orig. Investig. 2007, 25, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Larke, N.L.; Thomas, S.L.; Silva, I.D.S.; Weiss, H.A. Male circumcision and penile cancer: A systematic review and meta-analysis. Cancer Causes Control 2011, 22, 1097–1110. [Google Scholar] [CrossRef]
- Horwich, A.; Shipley, J.; Huddart, R. Testicular germ-cell cancer. Lancet 2006, 367, 754–765. [Google Scholar] [CrossRef]
- Gilligan, T.; Lin, D.W.; Aggarwal, R.; Chism, D.; Cost, N.; Derweesh, I.H.; Emamekhoo, H.; Feldman, D.R.; Geynisman, D.M.; Hancock, S.L.; et al. Testicular Cancer, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 1529–1554. [Google Scholar] [CrossRef] [PubMed]
- Ghazarian, A.A.; Rusner, C.; Trabert, B.; Braunlin, M.; McGlynn, K.A.; Stang, A. Testicular cancer among US men aged 50 years and older. Cancer Epidemiol. 2018, 55, 68–72. [Google Scholar] [CrossRef]
- Dieckmann, K.-P.; Pichlmeier, U. Clinical epidemiology of testicular germ cell tumors. World J. Urol. 2004, 22, 2–14. [Google Scholar] [CrossRef]
- Aggarwal, B.B. Nuclear factor-κB: The enemy within. Cancer Cell 2004, 6, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Baby, D.; Rajguru, J.P.; Patil, P.B.; Thakkannavar, S.S.; Pujari, V.B. Inflammation and cancer. Ann. Afr. Med. 2019, 18, 121–126. [Google Scholar] [CrossRef]
- Pollard, J.W. Tumour-educated macrophages promote tumour progression and metastasis. Nat. Rev. Cancer 2004, 4, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Newell, G.R.; Mills, P.K.; Johnson, D.E. Epidemiologic comparison of cancer of the testis and Hodgkin’s dis-ease among young males. Cancer 1984, 54, 1117–1123. [Google Scholar] [CrossRef]
- Fenton, K.A. Changing Epidemiology of HIV/AIDS in the United States: Implications for Enhancing and Promoting HIV Testing Strategies. Clin. Infect. Dis. 2007, 45, S213–S220. [Google Scholar] [CrossRef] [PubMed]
- Hentrich, M.; Pfister, D. HIV-Associated Urogenital Malignancies. Oncol. Res. Treat. 2017, 40, 106–112. [Google Scholar] [CrossRef]
- Fenton, L.Z.; Karakas, S.P.; Baskin, L.; Campbell, J.B. Sonography of pediatric blunt scrotal trauma: What the pediatric urologist wants to know. Pediatr. Radiol. 2016, 46, 1049–1058. [Google Scholar] [CrossRef]
- Bieniek, J.M.; Juvet, T.; Margolis, M.; Grober, E.D.; Lo, K.C.; Jarvi, K.A. Prevalence and Management of Incidental Small Testicular Masses Discovered on Ultrasonographic Evaluation of Male Infertility. J. Urol. 2018, 199, 481–486. [Google Scholar] [CrossRef]
- Lawson, R.M. Sexually Transmitted Infections and Human Immunodeficiency Virus. Nurs. Clin. N. Am. 2020, 55, 445–456. [Google Scholar] [CrossRef]
- Li, Z.; Purcell, D.W.; Sansom, S.L.; Hayes, D.; Hall, H.I. Vital Signs:HIV Transmission Along the Continuum of Care—United States, 2016. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 267–272. [Google Scholar] [CrossRef]
- Hirth, J. Disparities in HPV vaccination rates and HPV prevalence in the United States: A review of the literature. Hum. Vaccines Immunother. 2018, 15, 146–155. [Google Scholar] [CrossRef]
- World Health Organization; Electronic address: sageexecsec@who.int. Human papillomavirus vaccines: WHO position paper, May 2017-Recommendations. Vaccine 2017, 35, 5753–5755. [Google Scholar] [CrossRef]
- José, F.X.B.; Quint, W.G.; Alemany, L.; Geraets, D.T.; Klaustermeier, J.E.; Lloveras, B.; Tous, S.; Felix, A.; Bravo, L.E.; Shin, H.-R.; et al. Human papillomavirus genotype attribution in invasive cervical cancer: A retrospective cross-sectional worldwide study. Lancet Oncol. 2010, 11, 1048–1056. [Google Scholar] [CrossRef]
- Cheng, L.; Wang, Y.; Du, J. Human Papillomavirus Vaccines: An Updated Review. Vaccines 2020, 8, 391. [Google Scholar] [CrossRef] [PubMed]
- Dobson, S.R.M.; McNeil, S.; Dionne, M.; Dawar, M.; Ogilvie, G.S.; Krajden, M.; Sauvageau, C.; Scheifele, D.W.; Kollmann, T.R.; Halperin, S.A.; et al. Immunogenicity of 2 Doses of HPV Vaccine in Younger Adolescents vs. 3 Doses in Young Women: A randomized clinical trial. JAMA 2013, 309, 1793–1802. [Google Scholar] [CrossRef] [PubMed]
- Romanowski, B.; Schwarz, T.F.; Ferguson, L.M.; Peters, K.; Dionne, M.; Schulze, K.; Ramjattan, B.; Hillemanns, P.; Catteau, G.; Dobbelaere, K.; et al. Immunogenicity and safety of the HPV-16/18 AS04-adjuvanted vaccine administered as a 2-dose schedule compared to the licensed 3-dose schedule. Hum. Vaccines 2011, 7, 1374–1386. [Google Scholar] [CrossRef]
- Athanasiou, A.; Bowden, S.; Paraskevaidi, M.; Fotopoulou, C.; Martin-Hirsch, P.; Paraskevaidis, E.; Kyrgiou, M. HPV vaccination and cancer prevention. Best Pract. Res. Clin. Obstet. Gynaecol. 2020, 65, 109–124. [Google Scholar] [CrossRef]
- Herrero, R.; Quint, W.; Hildesheim, A.; Gonzalez, P.; Struijk, L.; Katki, H.A.; Porras, C.; Schiffman, M.; Rodriguez, A.C.; Solomon, D.; et al. Reduced Prevalence of Oral Human Papillomavirus (HPV) 4 Years after Bivalent HPV Vaccination in a Randomized Clinical Trial in Costa Rica. PLoS ONE 2013, 8, e68329. [Google Scholar] [CrossRef]
- Hillman, R.J.; Giuliano, A.R.; Palefsky, J.M.; Goldstone, S.; Moreira, E.D.; Vardas, E.; Aranda, C.; Jessen, H.; Ferris, D.G.; Coutlee, F.; et al. Immunogenicity of the Quadrivalent Human Papillomavirus (Type 6/11/16/18) Vaccine in Males 16 to 26 Years Old. Clin. Vaccine Immunol. 2012, 19, 261–267. [Google Scholar] [CrossRef]
- Giuliano, A.R.; Palefsky, J.M.; Goldstone, S.; Moreira, E.; Penny, M.; Aranda, C.; Vardas, E.; Moi, H.; Jessen, H.; Hillman, R.; et al. Efficacy of Quadrivalent HPV Vaccine against HPV Infection and Disease in Males. N. Engl. J. Med. 2011, 364, 401–411. [Google Scholar] [CrossRef]
- Harder, T.; Wichmann, O.; Klug, S.J.; AB van der Sande, M.; Wiese-Posselt, M. Efficacy, effectiveness and safety of vaccination against human papillomavirus in males: A systematic review. BMC Med. 2018, 16, 110. [Google Scholar] [CrossRef]
- Albero, G.; Castellsagué, X.; Lin, H.-Y.; Fulp, W.; Villa, L.L.; Lazcano-Ponce, E.; Papenfuss, M.; Abrahamsen, M.; Salmerón, J.; Quiterio, M.; et al. Male circumcision and the incidence and clearance of genital human papillomavirus (HPV) infection in men: The HPV Infection in men (HIM) cohort study. BMC Infect. Dis. 2014, 14, 75. [Google Scholar] [CrossRef]
- Tobian, A.A.R.; Serwadda, D.; Quinn, T.C.; Kigozi, G.; Gravitt, P.E.; Laeyendecker, O.; Charvat, B.; Ssempijja, V.; Riedesel, M.; Oliver, A.E.; et al. Male Circumcision for the Prevention of HSV-2 and HPV Infections and Syphilis. N. Engl. J. Med. 2009, 360, 1298–1309. [Google Scholar] [CrossRef] [PubMed]
- Auvert, B.; Sobngwi-Tambekou, J.; Cutler, E.; Nieuwoudt, M.; Lissouba, P.; Puren, A.; Taljaard, D. Effect of Male Circumcision on the Prevalence of High-Risk Human Papillomavirus in Young Men: Results of a Randomized Controlled Trial Conducted in Orange Farm, South Africa. J. Infect. Dis. 2009, 199, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Friedman, B.; Khoury, J.; Petersiel, N.; Yahalomi, T.; Paul, M.; Neuberger, A. Pros and cons of circumcision: An evidence-based overview. Clin. Microbiol. Infect. 2016, 22, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Hakenberg, O.W.; Dräger, D.L.; Erbersdobler, A.; Naumann, C.M.; Jünemann, K.-P.; Protzel, C. The Diagnosis and Treatment of Penile Cancer. Dtsch. Aerzteblatt Online 2018, 115, 646–652. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author and Publication Year | Study Design | Sample Size | Main Findings | Study Quality |
|---|---|---|---|---|
| Prostate Cancer | ||||
| Rosenblatt 2001 [16] | Case-control | 1456 | Association between sexual factor and PCa | 5 # |
| Spence 2014 [12] | Case-control | 3208 | Reduction of risk of PCa in men with >20 sexual partners No correlation between Risk of PCa and age at first sexual intercourse No association between STDs and PCa | 8 # |
| Papa 2017 [14] | Case-control | 2141 | Inverse associations with EF and PCa | 6 # |
| Crum 2004 [20] | Prospective cohort study | 269 | Positive correlation between incidence of PCa and duration of HIV infection | 6 # |
| Cheng 2010 [18] | Prospective cohort study | 68,675 | Positive correlation between prostatitis, STDs and Pca | 8 # |
| Rider 2016 [13] | Prospective cohort study | 31,925 | Inverse association between EF and PCa | 7 # |
| Sinnott 2018 [15] | Prospective cohort study | 157 | Inverse association between EF and PCa | 6 # |
| Jian 2018 [17] | Systematic Review | 55,490 | Positive association between number of female sexual partners, age at first intercourse, EF, and the risk of PCa | Intermediate * |
| Sun 2021 [19] | Systematic Review | 2780 | Reduced risk of PCa among people with HIV/AIDS | High * |
| Penile Cancer | ||||
| Iversen 1997 [23] | Case-control | 867 | Not significant increased of incidence of HPV related cancers in partner of patients with HPV related cancer | 5 # |
| Daling 2005 [21] | Case-control | 808 | Positive association between HPV and penile cancer | 7 # |
| Madsen 2008 [24] | Case-control | 293 | Positive correlation between oral sex as a risk factor in PC | 5 # |
| Mirghani 2017 [22] | Systematic Review | 1356 | Higher incidence of HPV related cancers in partner of patients with HPV related cancer | Low * |
| Lekoane 2020 [25] | Systematic Review | 16,351 | Positive correlation between HIV andHPV-related cancers | Intermediate * |
| Testicular Cancer | ||||
| Algood 1988 [26] | Prospective Cohort study | 86 | Positive correlation between Viral infections (Epstein-Barr virus, cytomegalovirus, and hepatitis A and B viruses) and TGCTs | 6 # |
| Kao 2016 [29] | Case-control | 4092 | Positive association between TGCTs and Epididymoorchitis | 8 # |
| Garolla 2019 [27] | Meta-analysis | 285,878 | Positive correlation between viral infections and risk of developing TGCTs | High * |
| Trabert 1969 [30] | Meta-analysis | 1696 | No association between common infections and TGCTs | Intermediate * |
| Grulich 2017 [28] | Meta-analysis | 476,149 | Higher incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients | High * |
| Protective Factors | Risk Factors | |
|---|---|---|
| Penile cancer | Circumcision * | Transmission of HPV 16 and HPV 18; transmission of HIV; phimosis |
| Prostate cancer | High ejaculatory frequency | High number of sexual partners; homosexuality; STDs (e.g., gonorrhea) |
| Testicular cancer | Trauma ** | Viral infection and epididymoorchitis *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crocetto, F.; Arcaniolo, D.; Napolitano, L.; Barone, B.; La Rocca, R.; Capece, M.; Caputo, V.F.; Imbimbo, C.; De Sio, M.; Calace, F.P.; et al. Impact of Sexual Activity on the Risk of Male Genital Tumors: A Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2021, 18, 8500. https://doi.org/10.3390/ijerph18168500
Crocetto F, Arcaniolo D, Napolitano L, Barone B, La Rocca R, Capece M, Caputo VF, Imbimbo C, De Sio M, Calace FP, et al. Impact of Sexual Activity on the Risk of Male Genital Tumors: A Systematic Review of the Literature. International Journal of Environmental Research and Public Health. 2021; 18(16):8500. https://doi.org/10.3390/ijerph18168500
Chicago/Turabian StyleCrocetto, Felice, Davide Arcaniolo, Luigi Napolitano, Biagio Barone, Roberto La Rocca, Marco Capece, Vincenzo Francesco Caputo, Ciro Imbimbo, Marco De Sio, Francesco Paolo Calace, and et al. 2021. "Impact of Sexual Activity on the Risk of Male Genital Tumors: A Systematic Review of the Literature" International Journal of Environmental Research and Public Health 18, no. 16: 8500. https://doi.org/10.3390/ijerph18168500
APA StyleCrocetto, F., Arcaniolo, D., Napolitano, L., Barone, B., La Rocca, R., Capece, M., Caputo, V. F., Imbimbo, C., De Sio, M., Calace, F. P., & Manfredi, C. (2021). Impact of Sexual Activity on the Risk of Male Genital Tumors: A Systematic Review of the Literature. International Journal of Environmental Research and Public Health, 18(16), 8500. https://doi.org/10.3390/ijerph18168500