
“Better If They Laugh with Me than at Me”: The Role of Humor in Coping with Obesity-Related Stigma in Women




Abstract
:1. Introduction
1.1. Obesity and Stigma
1.2. Coping with Obesity-Related Stigma
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.2.1. Humor Styles Questionnaire (HSQ)
2.2.2. Perceived Stigmatization Questionnaire (PSQ)
2.2.3. Brief COPE Scale
2.2.4. Body Composition Analyzer
2.3. Statistical Analysis
- pandas 1.1.3
- scipy 1.5.2
- numpy 1.19.2
- pingouin 0.3.9
3. Results
3.1. Anthropometric Differences
3.1.1. Perceived Stigmatization
3.1.2. Coping with Stress Situation and Sense of Humor
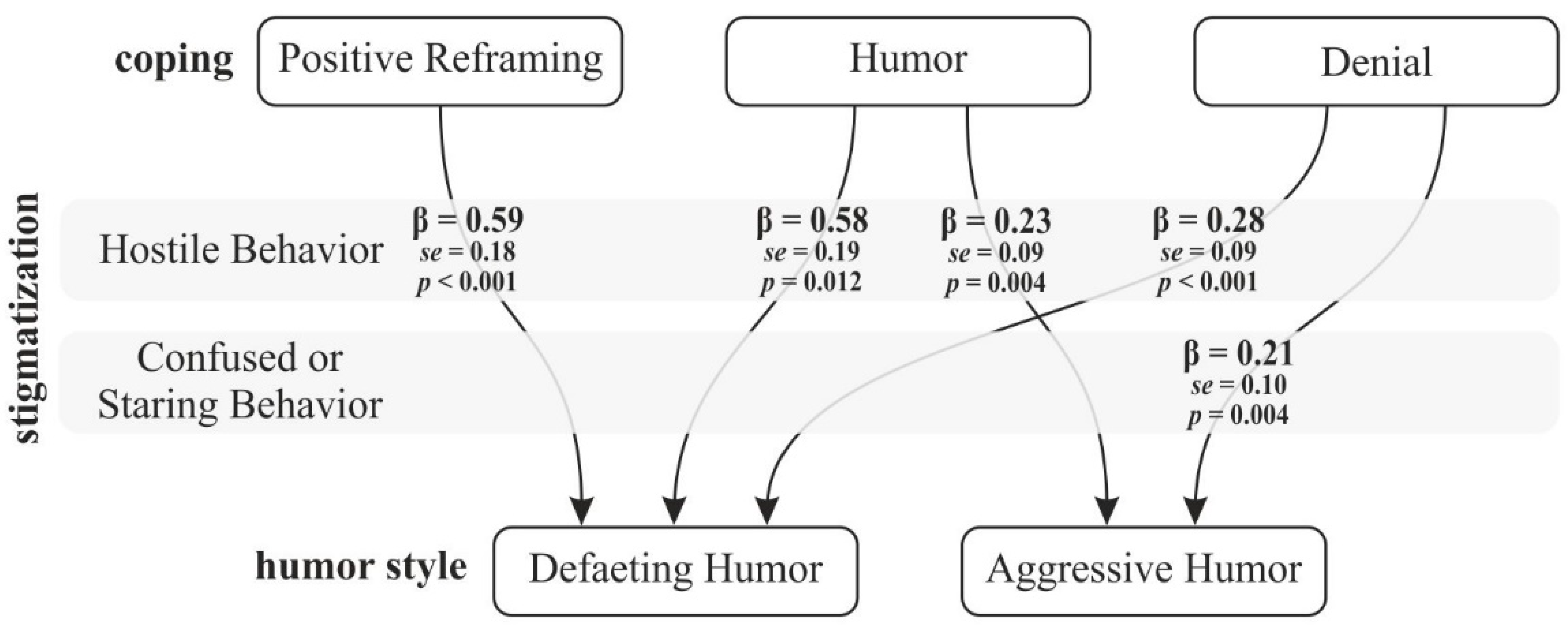
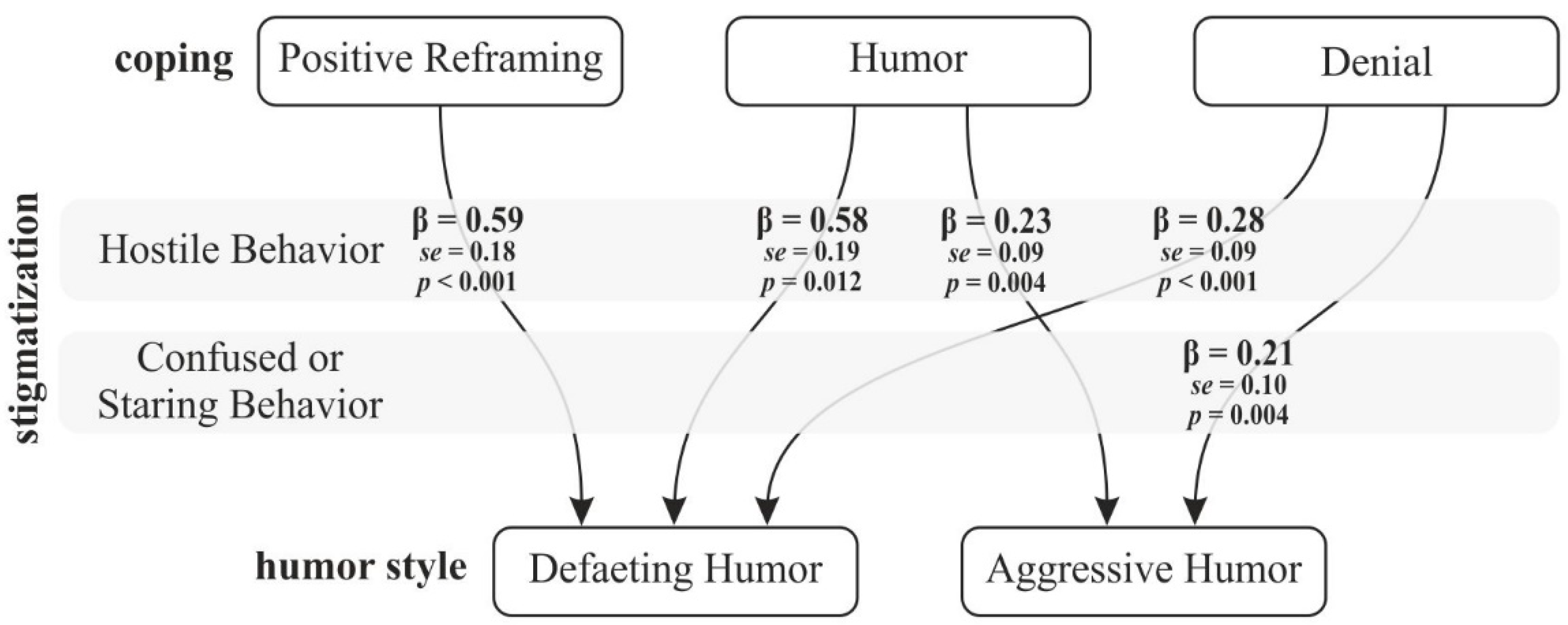
3.1.3. Perceived Stigmatization as a Mediator between Humor Styles and Coping with the Stress
4. Discussion
4.1. Anthropometric Variables
4.2. Obesity and the Subjective Perception of Stigmatization
4.3. The Role of Humor in Dealing with Obesity Stigma
4.4. Limitation and Future Perspectives
5. Conclusions
- (a)
- Prevention, starting at the earliest years, at school and at home, in terms of education about health, physical activity, and sugar and fat metabolism;
- (b)
- Providing support and comprehensive help for individuals who have excess weight, including psychological and medical help;
- (c)
- Providing support for families of obese individuals and teaching appropriate behaviors with regard to improving the health and quality of life of the affected individuals.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight; World Health Organization: Geneva, Switzerland, 2016; Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 10 May 2021).
- Central Statistical Office. Health Status of Population in Poland in 2014; Statistical Publishing Establishment: Warsaw, Poland, 2016. [Google Scholar]
- Public Opinion Research Center. Do Poles Have Problem with Overweight; CBOS: Warszawa, Poland, 2019. [Google Scholar]
- ProCon.org, B. Global Obesity Levels. Available online: https://obesity.procon.org/global-obesity-levels/?fbclid=IwAR0VXuyTgcWhWaVEc8nY3DWZiY4l6hPH72Z_tyB26pLcKLnZCf1uLHHe0ho#oecd (accessed on 20 January 2021).
- Zgliczyński, W.S. Overweight and obesity in Poland. INFOS Socio Econ. Issues 2017, 227, 1–4. [Google Scholar]
- Riffer, F.; Sprung, M.; Münch, H.; Kaiser, E.; Streibl, L.; Heneis, K.; Kautzky-Willer, A. Relationship between psychological stress and metabolism in morbidly obese individuals. Wien. Klin. Wochenschr. 2019, 132, 139–149. [Google Scholar] [CrossRef] [PubMed]
- Finer, N. Medical consequences of obesity. Medicine 2015, 43, 88–93. [Google Scholar] [CrossRef]
- Park, A. Pathophysiology and aetiology and medical consequences of obesity. Medicine 2019, 47, 169–174. [Google Scholar] [CrossRef]
- Gerlach, G.; Loeber, S.; Herpertz, S. Personality disorders and obesity: A systematic review. Obes. Rev. 2016, 17, 691–723. [Google Scholar] [CrossRef]
- Darimont, T.; Karavasiloglou, N.; Hysaj, O.; Richard, A.; Rohrmann, S. Body weight and self-perception are associated with depression: Results from the National Health and Nutrition Examination Survey (NHANES) 2005–2016. J. Affect. Disord. 2020, 274, 929–934. [Google Scholar] [CrossRef]
- Sarwer, D.B.; Hanson, A.J.; Voeller, J.; Steffen, K. Obesity and Sexual Functioning. Curr. Obes. Rep. 2018, 7, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Lipowska, M.; Bidzan, M.; Mazurkiewicz, N.; Lipowski, M. Jakość życia w przewlekłej widocznej chorobie a poczucie stygmatyzacji u młodych kobiet [Quality of life chronic visible illness and the sense of stigmatization in young women]. Prz. Psychol. 2015, 58, 303–323. [Google Scholar]
- Patist, C.M.; Stapelberg, N.J.C.; Du Toit, E.F.; Headrick, J.P. The brain-adipocyte-gut network: Linking obesity and depression subtypes. Cogn. Affect. Behav. Neurosci. 2018, 18, 1121–1144. [Google Scholar] [CrossRef]
- Luppino, F.S.; de Wit, L.; Bouvy, P.F.; Stijnen, T.; Cuijpers, P.; Penninx, B.W.J.H.; Zitman, F.G. Overweight, Obesity, and Depression. Arch. Gen. Psychiatry 2010, 67, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Franzoi, S.L.; Vasquez, K.; Sparapani, E.; Frost, K.; Martin, J.; Aebly, M. Exploring Body Comparison Tendencies. Psychol. Women Q. 2011, 36, 99–109. [Google Scholar] [CrossRef] [Green Version]
- Lipowska, M.; Lipowski, M. Narcissism as a Moderator of Satisfaction with Body Image in Young Women with Extreme Underweight and Obesity. PLoS ONE 2015, 10, e0126724. [Google Scholar] [CrossRef]
- Garawi, F.; Devries, K.; Thorogood, N.; Uauy, R. Global differences between women and men in the prevalence of obesity: Is there an association with gender inequality? Eur. J. Clin. Nutr. 2014, 68, 1101–1106. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.; Shaw, D. The worldwide epidemic of female obesity. Best Pr. Res. Clin. Obstet. Gynaecol. 2015, 29, 289–299. [Google Scholar] [CrossRef]
- Goffman, E. Stigma; Notes on the Management of Spoiled Identity; Prentice-Hall: Englewood Cliffs, NJ, USA, 1963. [Google Scholar]
- Czykwin, E. Stygmat Społeczny [Social Stigma]; Wydawnictwo Naukowe PWN: Warszawa, Poland, 2007. [Google Scholar]
- Dovidio, J.F.; Major, B.; Crocker, J. Stigma: Introduction and overview. In The Social Psychology of Stigma; Heatherton, T.F., Kleck, R.E., Hebl, M.R., Hull, J.G., Eds.; The Guilford Press: New York, NY, USA, 2003; pp. 1–28. [Google Scholar]
- Wadden, T.A.; Stunkard, A.J. Social and Psychological Consequences of Obesity. Ann. Intern. Med. 1985, 103, 1062–1067. [Google Scholar] [CrossRef]
- Brytek-Matera, A. Body image among obese women: Consequences and degree of body dissatisfaction, relationship with low self-esteem and coping strategies. Psychiatr. Polska 2010, 44, 267–275. [Google Scholar]
- Izydorczyk, B.; Sitnik-Warchulska, K.; Lizińczyk, S.; Lipowska, M. Socio-Cultural Standards Promoted by the Mass Media as Predictors of Restrictive and Bulimic Behavior. Front. Psychiatry 2020, 11. [Google Scholar] [CrossRef]
- Harrison, K. The Body Electric: Thin-Ideal Media and Eating Disorders in Adolescents. J. Commun. 2000, 50, 119–143. [Google Scholar] [CrossRef]
- Makara-Studzińska, M.; Buczyjan, A.; Morylowska, J. Jedzenie—przyjaciel i wróg. Korelaty psychologiczne otyłości. [Eating—a friend and an enemy. Psychological correlates of obesity]. Zdr. Publ. 2007, 117, 392–396. [Google Scholar]
- Puhl, R.M.; Heuer, C.A. Obesity Stigma: Important Considerations for Public Health. Am. J. Public Health 2010, 100, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; King, K.M. Weight discrimination and bullying. Best Pr. Res. Clin. Endocrinol. Metab. 2013, 27, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Annis, N.M.; Cash, T.F.; I Hrabosky, J. Body image and psychosocial differences among stable average weight, currently overweight, and formerly overweight women: The role of stigmatizing experiences. Body Image 2004, 1, 155–167. [Google Scholar] [CrossRef]
- Vartanian, L.; Pinkus, R.T.; Smyth, J. The phenomenology of weight stigma in everyday life. J. Context. Behav. Sci. 2014, 3, 196–202. [Google Scholar] [CrossRef]
- Tomiyama, A.J.; Carr, D.; Granberg, E.M.; Major, B.; Robinson, E.; Sutin, A.R.; Brewis, A. How and why weight stigma drives the obesity ‘epidemic’ and harms health. BMC Med. 2018, 16, 1–6. [Google Scholar] [CrossRef]
- Lipowska, M.; Khanh, H.T.T.; Lipowski, M.; Różycka-Tran, J.; Bidzan, M.; Ha, T.T. The Body as an Object of Stigmatization in Cultures of Guilt and Shame: A Polish–Vietnamese Comparison. Int. J. Environ. Res. Public Health 2019, 16, 2814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izydorczyk, B.; Truong Thi Khanh, H.; Lizińczyk, S.; Sitnik-Warchulska, K.; Lipowska, M.; Gulbicka, A. Body Dissatisfaction, Restrictive, and Bulimic Behaviours among Young Women: A Polish–Japanese Comparison. Nutrients 2020, 12, 666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedman, K.E.; Reichmann, S.K.; Costanzo, P.R.; Musante, G.J. Body Image Partially Mediates the Relationship between Obesity and Psychological Distress. Obes. Res. 2002, 10, 33–41. [Google Scholar] [CrossRef]
- Marcysiak, I.M. Otyłość jako źródło lęku i stresu u kobiet [Obesity as a source of stress in women]. Studia Psychol. 2001, 2, 129–136. [Google Scholar]
- Yau, Y.H.C.; Potenza, M.N. Stress and eating behaviors. Minerva Endocrinol. 2013, 38, 255–267. [Google Scholar]
- Robbins, T.; Fray, P. Stress-induced eating: Fact, fiction or misunderstanding? Appetite 1980, 1, 103–133. [Google Scholar] [CrossRef]
- Puhl, R.; Brownell, K.D. Ways of coping with obesity stigma: Review and conceptual analysis. Eat. Behav. 2003, 4, 53–78. [Google Scholar] [CrossRef]
- Rahnavard, F.; Sadati, A.K.; Amini, M. How do Obese Women Cope with Social Stigma? A Phenomenological Study. J. Health Sci. Surveill. Syst. 2014, 2, 151–157. [Google Scholar]
- Myers, A.; Rosen, J. Obesity stigmatization and coping: Relation to mental health symptoms, body image, and self-esteem. Int. J. Obes. 1999, 23, 221–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puhl, R.M.; Brownell, K.D. Confronting and Coping with Weight Stigma: An Investigation of Overweight and Obese Adults. Obesity 2006, 14, 1802–1815. [Google Scholar] [CrossRef] [PubMed]
- Himes, S.M.; Thompson, J.K. Fat Stigmatization in Television Shows and Movies: A Content Analysis. Obesity 2007, 15, 712–718. [Google Scholar] [CrossRef] [Green Version]
- Freud, S. Humour. Int. J. Psychoanal. 1928, 9, 1–6. [Google Scholar]
- Suls, J. Cognitive Processes in Humor Appreciation. In Handbook of Humor Research; McGhee, P.E., Goldstein, J.H., Eds.; Springer: New York, NY, USA, 1983. [Google Scholar] [CrossRef]
- Rynkiewicz, J. Kognitywne spojrzenie na poczucie humoru [The Cognitive Views on a Sense of Humour]. Via Mentis 2012, 1, 86–98. [Google Scholar]
- Abel, M.H. Humor, stress, and coping strategies. Humor Int. J. Humor Res. 2002, 15. [Google Scholar] [CrossRef]
- Pérez-Aranda, A.; Hofmann, J.; Feliu-Soler, A.; Ramírez-Maestre, C.; Andrés-Rodríguez, L.; Ruch, W.; Luciano, J.V. Laughing away the pain: A narrative review of humour, sense of humour and pain. Eur. J. Pain 2018, 23, 220–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cann, A.; Collette, C. Sense of Humor, Stable Affect, and Psychological Well-Being. Eur. J. Psychol. 2014, 10, 464–479. [Google Scholar] [CrossRef] [Green Version]
- Satici, B. Exploring the relationship between coping humor and subjective happiness: Belongingness and forgiveness as serial mediators. Health Psychol. Rep. 2020, 8, 228–237. [Google Scholar] [CrossRef]
- Winiarska, J. Jokes in contrast to stereotypes. Ethnolinguistics Probl. Lang. Cult. 2019, 31, 211. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Powell, K.J.; Fokuo, J.K.; Kosyluk, K.A. Does Humor Influence the Stigma of Mental Illnesses? J. Nerv. Ment. Dis. 2014, 202, 397–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schermer, J.A.; Martin, R.A.; Vernon, P.A.; Martin, N.G.; Conde, L.C.; Statham, D.; Lynskey, M.T. Lonely people tend to make fun of themselves: A behavior genetic analysis of humor styles and loneliness. Pers. Individ. Differ. 2017, 117, 71–73. [Google Scholar] [CrossRef]
- De Clercq, D.; Belausteguigoitia, I. Coping and laughing in the face of broken promises: Implications for creative behavior. Pers. Rev. 2019, 49, 993–1014. [Google Scholar] [CrossRef]
- Kruczek, A.; Basińska, M.A. Coping humor for the relationship between a sense of stress at work and job satisfaction. Med. Pr. 2018. [Google Scholar] [CrossRef]
- Martin, R.A. Approaches to the sense of humor: A historical review. In The Sense of Humor; Ruch, W., Ed.; De Gruyter Mouton: Berlin, Germany, 2015; pp. 15–60. [Google Scholar] [CrossRef]
- Martin, R.A.; Puhlik-Doris, P.; Larsen, G.; Gray, J.; Weir, K. Individual differences in uses of humor and their relation to psychological well-being: Development of the Humor Styles Questionnaire. J. Res. Pers. 2003, 37, 48–75. [Google Scholar] [CrossRef]
- Kruczek, A.; Basińska, M.A. Humour, stress and coping in adults. Adv. Psychiatry Neurol. 2018, 27, 181–195. [Google Scholar] [CrossRef]
- Voges, M.M.; Giabbiconi, C.-M.; Schöne, B.; Waldorf, M.; Hartmann, A.S.; Vocks, S. Gender Differences in Body Evaluation: Do Men Show More Self-Serving Double Standards Than Women? Front. Psychol. 2019, 10. [Google Scholar] [CrossRef]
- Tovee, M.; Maisey, D.; Vale, E.; Cornelissen, P. Characteristics of male attractiveness for women. Lancet 1999, 353, 1500. [Google Scholar] [CrossRef]
- Lipowska, M.; Lipowski, M.; Jurek, P.; Jankowska, A.M.; Pawlicka, P. Gender and Body-Fat Status as Predictors of Parental Feeding Styles and Children’s Nutritional Knowledge, Eating Habits and Behaviours. Int. J. Environ. Res. Public Health 2018, 15, 852. [Google Scholar] [CrossRef] [Green Version]
- Leighton, K.; Kardong-Edgren, S.; Schneidereith, T.; Foisy-Doll, C. Using Social Media and Snowball Sampling as an Alternative Recruitment Strategy for Research. Clin. Simul. Nurs. 2021, 55, 37–42. [Google Scholar] [CrossRef]
- Hornowska, E.; Charytonik, J. Polska adaptacja kwestionariusza stylów humoru (HSQ) r.; Martina, p.; Puhlik-Doris, g.; Larsena, j.; Gray, i.k. Weir [Polish Adaptation of the Humor Styles Questionnaire by R. Martin, P. Puhlik-Doris, G. Larsen, J. Gray And K. Weir]. Psychol. Stud. 2011, 49, 5–22. [Google Scholar] [CrossRef]
- Lawrence, J.W.; Fauerbach, J.A.; Heinberg, L.J.; Doctor, M.; Thombs, B.D. The reliability and validity of the Perceived Stig-matization Questionnaire (PSQ) and the Social Comfort Questionnaire (SCQ) among an adult burn survivor sample. Psycho-Log. Assess. 2006, 18, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S. You want to measure coping but your protocol’ too long: Consider the brief cope. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef]
- Juczyński, Z. Narzędzia Pomiaru w Promocji i Psychologii Zdrowia [Instruments for Measurements in Health Promotion and Psychology]; Pracownia Testów PTP: Warsaw, Poland, 2001. [Google Scholar]
- Sweeting, H.N. Measurement and Definitions of Obesity in Childhood and Adolescence: A field guide for the uninitiated. Nutr. J. 2007, 6, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elffers, T.W.; De Mutsert, R.; Lamb, H.J.; De Roos, A.; Van Dijk, K.W.; Rosendaal, F.R.; Jukema, J.W.; Trompet, S. Body fat distribution, in particular visceral fat, is associated with cardiometabolic risk factors in obese women. PLoS ONE 2017, 12, e0185403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maffetone, P.B.; Rivera-Dominguez, I.; Laursen, P.B. Overfat and Underfat: New Terms and Definitions Long Overdue. Front. Public Health 2017, 4, 279. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, D.; Heymsfield, S.B.; Heo, M.; Jebb, S.A.; Murgatroyd, P.R.; Sakamoto, Y. Healthy percentage body fat ranges: An approach for developing guidelines based on body mass index. Am. J. Clin. Nutr. 2000, 72, 694–701. [Google Scholar] [CrossRef]
- Source, O. Pandas. Available online: https://pandas.pydata.org/docs/reference/api/pandas.DataFrame.html?fbclid=IwAR1AmU3AEnjcmaWbhLWXQO8tdSueCGoeUhNsoa07dtg0Nj_93YVOACs47Ig (accessed on 4 February 2021).
- Siervo, M.; Montagnese, C.; Muscariello, E.; Evans, E.; Stephan, B.; Nasti, G.; Papa, A.; Iannetti, E.; Colantuoni, A. Weight loss expectations and body dissatisfaction in young women attempting to lose weight. J. Hum. Nutr. Diet. 2013, 27, 84–89. [Google Scholar] [CrossRef] [Green Version]
- Smart, R.; Tsong, Y. Weight, body dissatisfaction, and disordered eating: Asian American women’s perspectives. Asian Am. J. Psychol. 2014, 5, 344–352. [Google Scholar] [CrossRef] [Green Version]
- Lipowski, M.; Lipowska, M. Poziom narcyzmu jako moderator relacji pomiędzy obiektywnymi wymiarami ciała a stosunk-iem do własnej cielesności młodych mężczyzn [The role of narcissism in the relationship between objective body measure-ments and body self-esteem of young men]. Polskie Forum Psychol. 2015, 20, 31–46. [Google Scholar] [CrossRef]
- Franzoi, S.L. The body-as-object versus the body-as-process: Gender differences and gender considerations. Sex Roles 1995, 33, 417–437. [Google Scholar] [CrossRef]
- Blodorn, A.; Major, B.; Hunger, J.; Miller, C. Unpacking the psychological weight of weight stigma: A rejection-expectation pathway. J. Exp. Soc. Psychol. 2016, 63, 69–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asbury, M.B.; Woszidlo, A. Understanding the relationship between family communication and the development of weight stigma. Health Psychol. Rep. 2016, 3, 213–223. [Google Scholar] [CrossRef] [Green Version]
- Anesbury, T.; Tiggemann, M. An attempt to reduce negative stereotyping of obesity in children by changing controllability beliefs. Health Educ. Res. 2000, 15, 145–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burmeister, J.M.; Carels, R.A. Weight-related humor in the media: Appreciation, distaste, and anti-fat attitudes. Psychol. Popul. Media Cult. 2014, 3, 223–238. [Google Scholar] [CrossRef]
- Himmelstein, M.S.; Puhl, R.M.; Quinn, D.M. Weight stigma and health: The mediating role of coping responses. Health Psychol. 2018, 37, 139–147. [Google Scholar] [CrossRef]
- Varela, C.; Andrés, A.; Saldaña, C. The behavioral pathway model to overweight and obesity: Coping strategies, eating behaviors and body mass index. Eat. Weight. Disord. Stud. Anorex. Bulim. Obes. 2019, 25, 1277–1283. [Google Scholar] [CrossRef] [PubMed]
- Kubie, L.S. The Destructive Potential of Humor in Psychotherapy. Am. J. Psychiatry 1971, 127, 861–866. [Google Scholar] [CrossRef]
- Fabrizi, M.S.; Pollio, H.R. A naturalistic study of humorous activity in a third, seventh, and eleventh grade classroom. Merrill-Palmer Q. 1987, 33, 107–128. [Google Scholar]
- Schermer, J.A.; Rogoza, R.; Kwiatkowska, M.M.; Kowalski, C.M.; Aquino, S.; Ardi, R.; Bolló, H.; Branković, M.; Chegeni, R.; Crusius, J.; et al. Humor styles across 28 countries. Curr. Psychol. 2019, 1–16. [Google Scholar] [CrossRef]
- Kushner, R.F.; Zeiss, D.M.; Feinglass, J.M.; Yelen, M. An obesity educational intervention for medical students addressing weight bias and communication skills using standardized patients. BMC Med. Educ. 2014, 14, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phelan, S.M.; Burgess, D.J.; Yeazel, M.W.; Hellerstedt, W.L.; Griffin, J.M.; Van Ryn, M. Impact of weight bias and stigma on quality of care and outcomes for patients with obesity. Obes. Rev. 2015, 16, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Powers, T.A.; Koestner, R.; Gorin, A.A. Autonomy support from family and friends and weight loss in college women. Fam. Syst. Health 2008, 26, 404–416. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Feature/Index | Healthy Fat (n = 73) | Overfat (n = 54) | Differences (df = 125) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | min | max | SD | M | min | max | SD | t | p | |
| %BF | 28.82 | 19.60 | 37.40 | 3.60 | 43.44 | 29.80 | 52.80 | 4.91 | 18.52 | <0.001 |
| Visceral Fat | 1.89 | 1.00 | 4.00 | 0.79 | 8.63 | 5.00 | 15.00 | 2.47 | 19.29 | <0.001 |
| Weight | 61.36 | 52.20 | 71.00 | 5.93 | 98.17 | 64.50 | 143.00 | 15.14 | 16.93 | <0.001 |
| Heigh | 167.55 | 148.00 | 182.00 | 6.14 | 167.37 | 153.00 | 180.00 | 5.36 | 0.17 | 0.863 |
| Age | 25.41 | 19.00 | 30.00 | 2.79 | 26.19 | 21.00 | 30.00 | 2.62 | 1.60 | 0.110 |
| BMI | 21.84 | 18.70 | 24.50 | 1.63 | 35.01 | 30.10 | 45.70 | 4.15 | 22.11 | <0.001 |
| Desired weight reduction in % | 8.82 | 0.55 | 17.46 | 4.37 | 27.41 | 10.21 | 43.96 | 8.97 | 14.04 | <0.001 |
| PSQ Scales | %BF | Visceral Fat | Desired Weight Reduction in % | |||
|---|---|---|---|---|---|---|
| Overfat | Healthy Fat | Overfat | Healthy Fat | Overfat | Healthy Fat | |
| Absence of Friendly Behavior | 0.05 | −0.34 ** | −0.01 | −0.18 | 0.04 | −0.17 |
| Confused/Staring Behavior | 0.38 ** | −0.14 | 0.34 * | −0.20 | 0.42 ** | 0.08 |
| Hostile Behavior | 0.32 * | −0.11 | 0.25 | −0.06 | 0.17 | 0.00 |
| Total | 0.38 ** | −0.28 * | 0.31 * | −0.21 | 0.31 * | −0.06 |
| Brief Cope Scales | %BF | Visceral Fat | Desired Weight Reduction in% | |||
|---|---|---|---|---|---|---|
| Overfat | Healthy Fat | Overfat | Healthy Fat | Overfat | Healthy Fat | |
| Active Coping | 0.22 | −0.04 | 0.23 | −0.02 | 0.12 | −0.21 |
| Planning | 0.30 * | −0.06 | 0.32 * | 0.03 | 0.20 | −0.01 |
| Positive reframing | 0.18 | −0.02 | 0.20 | −0.04 | 0.24 | −0.25 * |
| Acceptance | −0.03 | −0.16 | −0.01 | −0.15 | −0.01 | −0.05 |
| Humor | 0.02 | −0.04 | 0.07 | −0.20 | 0.06 | −0.25 * |
| Religion | 0.07 | −0.01 | −0.07 | −0.06 | 0.00 | −0.28 * |
| Use of emotional support | 0.22 | −0.05 | 0.14 | −0.01 | 0.04 | 0.03 |
| Use of informational support | 0.29 * | −0.15 | 0.29 * | −0.15 | 0.13 | 0.04 |
| Self-distraction | −0.03 | 0.21 | −0.06 | 0.09 | 0.27 * | 0.11 |
| Denial | 0.32 * | 0.06 | 0.37 ** | 0.07 | 0.26 | 0.28 * |
| Venting | −0.04 | 0.02 | 0.05 | 0.02 | 0.17 | 0.13 |
| Substance Use | −0.06 | 0.05 | −0.18 | −0.03 | 0.00 | 0.10 |
| Behavioral disengagement | 0.00 | −0.23 * | 0.06 | −0.23 | 0.35 ** | 0.19 |
| Self-blame | 0.16 | 0.02 | 0.15 | 0.09 | 0.40 ** | 0.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazurkiewicz, N.; Lipowski, M.; Krefta, J.; Lipowska, M. “Better If They Laugh with Me than at Me”: The Role of Humor in Coping with Obesity-Related Stigma in Women. Int. J. Environ. Res. Public Health 2021, 18, 7974. https://doi.org/10.3390/ijerph18157974
Mazurkiewicz N, Lipowski M, Krefta J, Lipowska M. “Better If They Laugh with Me than at Me”: The Role of Humor in Coping with Obesity-Related Stigma in Women. International Journal of Environmental Research and Public Health. 2021; 18(15):7974. https://doi.org/10.3390/ijerph18157974
Chicago/Turabian StyleMazurkiewicz, Natalia, Mariusz Lipowski, Jarosław Krefta, and Małgorzata Lipowska. 2021. "“Better If They Laugh with Me than at Me”: The Role of Humor in Coping with Obesity-Related Stigma in Women" International Journal of Environmental Research and Public Health 18, no. 15: 7974. https://doi.org/10.3390/ijerph18157974
APA StyleMazurkiewicz, N., Lipowski, M., Krefta, J., & Lipowska, M. (2021). “Better If They Laugh with Me than at Me”: The Role of Humor in Coping with Obesity-Related Stigma in Women. International Journal of Environmental Research and Public Health, 18(15), 7974. https://doi.org/10.3390/ijerph18157974