Sex- and Gender-Based Analysis in Cannabis Treatment Outcomes: A Systematic Review



Abstract
1. Introduction
2. Sex- and Gender-Based Analysis in Cannabis Research
3. Objective of the Present Study
4. Methods
4.1. Search Strategy
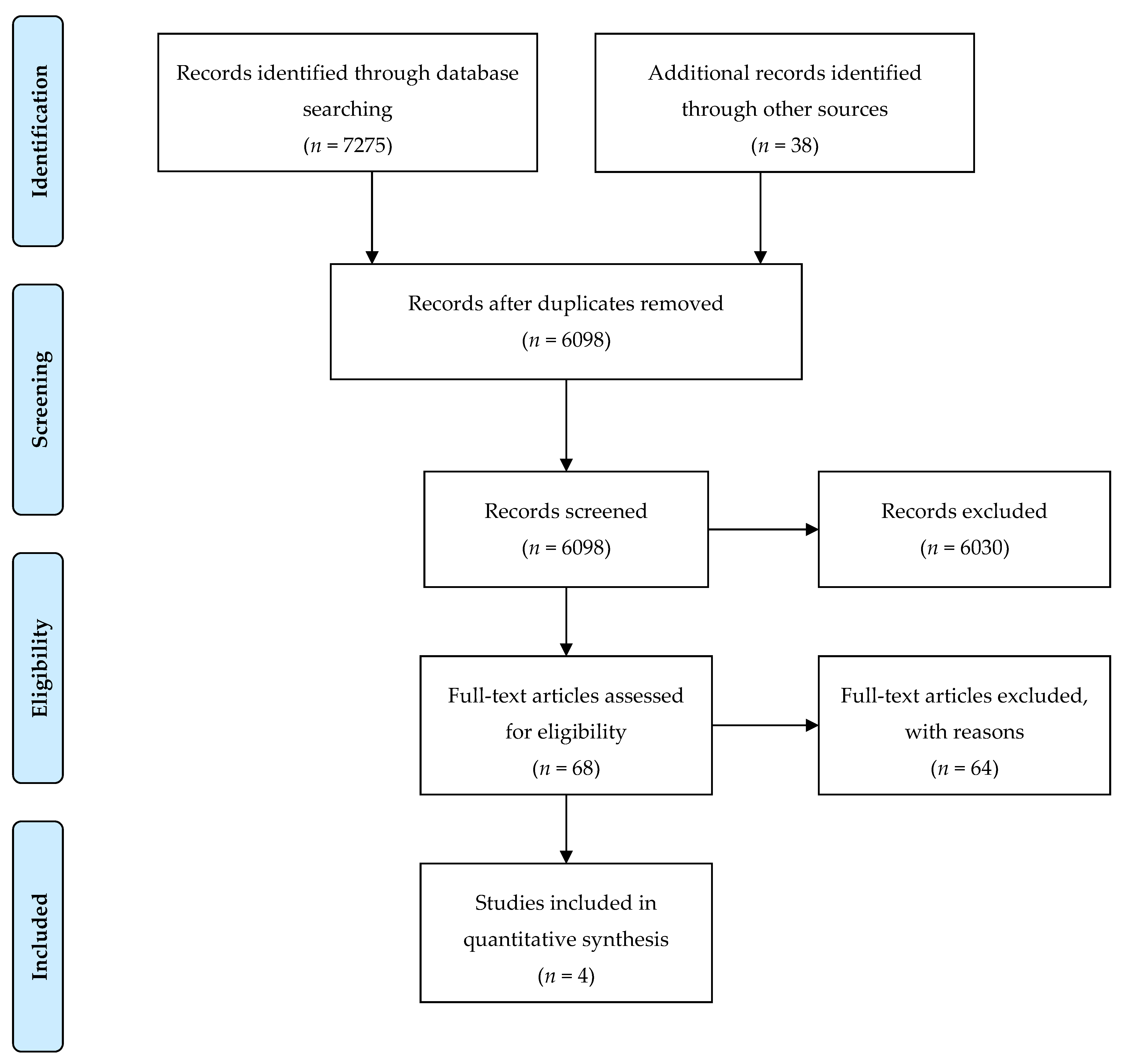
4.2. Literature Screening
4.3. Study Selection
4.4. Data Extraction
4.5. Sex- and Gender-Based Analysis in the Included Studies
- Use of sex and gender in the aim and research questions: were sex and gender included in the aim of the study or explicitly mentioned in the research question and the study design?
- Study design and reporting results: how were the outcomes analyzed and reported in relation to sex and gender?
- Interpretation of sex/gender findings: how were findings related to sex and gender included in the interpretation of the data?
- Intentional and accurate use of language: were the terms sex and gender used intentionally and appropriately by the authors of the study?
5. Results
5.1. Included Studies
5.2. Sex-Disaggregated Outcomes
5.3. Sex- and Gender-Based Analysis of the Included Studies
6. Discussion
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tannenbaum, C.; Greaves, L.; Graham, I.D. Why sex and gender matter in implementation research. Med. Res. Methodol. 2016, 16, 145. [Google Scholar] [CrossRef]
- Johnson, J.; Sharman, Z.; Vissandjée, B.; Stewart, E.D. Does a Change in Health Research Funding Policy Related to the Integration of Sex and Gender Have an Impact? PloS ONE 2014, 9, e99900. [Google Scholar] [CrossRef] [PubMed]
- Institute of Gender and Health. Science is Better with Sex and Gender, Strategic Plan; Canadian Institutes of Health Research: Ottawa, ON, Canada, 2019.
- Johnson, J.L.; Greaves, L.; Repta, R. Better Science with Sex and Gender: A Primer for Health Research; Women’s Health Research Network: Vancouver, BC, Canada, 2007. [Google Scholar]
- Krieger, N. Genders, sexes, and health: What are the connections—And why does it matter? Int. J. Epidemiol. 2003, 32, 652–657. [Google Scholar] [CrossRef] [PubMed]
- Welch, V.; Doull, M.; Yoganathan, M.; Jull, J.; Boscoe, M.; Coen, S.E.; Marshall, Z.; Pardo Pardo, J.; Pederson, A.; Petkovic, J.; et al. Reporting of sex and gender in randomized controlled trials in Canada: A cross-sectional methods study. Res. Integr. Peer Rev. 2017, 2, 15. [Google Scholar] [CrossRef] [PubMed]
- Bazargan-Hejazi, S.; Doull, M.; Yoganathan, M.; Jull, J.; Boscoe, M.; Coen, S.E.; Marshall, Z.; Pardo, P.J.; Pederson, A.; Petkovic, J.; et al. Gender comparison in referrals and treatment completion to residential and outpatient alcohol treatment. Subst. Abuse 2016, 10, S39943. [Google Scholar] [CrossRef] [PubMed]
- Greenfield, S.F. Substance abuse treatment entry, retention, and outcome in women: A review of the literature. Drug Alcohol Depend. 2007, 86, 1–21. [Google Scholar] [CrossRef]
- Grella, C.E.; Mitchell, P.K.; Alison, A.M. Gender and comorbidity among individuals with opioid use disorders in the NESARC study. Addict. Behav. 2009, 34, 498–504. [Google Scholar] [CrossRef]
- Greenfield, S.F.; Rosa, C.; Putnins, S.I.; Green, C.A.; Brooks, A.J.; Calsyn, D.A.; Cohen, L.R.; Erickson, S.; Gordon, S.M. Gender research in the National Institute on Drug Abuse National Treatment Clinical Trials Network: A summary of findings. Am. J. Drug Alcohol Abuse 2011, 37, 301–312. [Google Scholar] [CrossRef]
- Small, J.; Curran, G.M.; Booth, B. Barriers and facilitators for alcohol treatment for women: Are there more or less for rural women? J. Subst. Abuse 2010, 39, 1–13. [Google Scholar] [CrossRef]
- Bold, K.W.; Epstein, E.E.; McCrady, B.S. Baseline health status and quality of life after alcohol treatment for women with alcohol dependence. Addict. Behav. 2017, 64, 35–41. [Google Scholar] [CrossRef]
- Storbjörk, J. Gender differences in substance use, problems, social situation and treatment experiences among clients entering addiction treatment in Stockholm. Nordisk. Alkohol. Nark. 2011, 28, 185–209. [Google Scholar] [CrossRef]
- Perkins, K.A.; Scott, J. Sex differences in long-term smoking cessation rates due to nicotine patch. Nicotine Tob. Res. 2008, 10, 1245–1250. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.H.; Andrea, H.W.; Zhang, J.; Erin, E. Sex Differences in Smoking Cessation Pharmacotherapy Comparative Efficacy: A Network Meta-analysis. Nicotine Tob. Res. 2017, 19, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.H.; Zhang, J.; Weinberger, A.H.; Mazure, C.M.; McKee, S.A. Gender differences in the real-world effectiveness of smoking cessation medications: Findings from the 2010–2011 Tobacco Use Supplement to the Current Population Survey. Drug Alcohol Depend. 2017, 178, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Glatard, A.; Dobrinas, M.; Gholamrezaee, M.; Lubomirov, R.; Cornuz, J.; Csajka, C.; Eap, C.B. Association of nicotine metabolism and sex with relapse following varenicline and nicotine replacement therapy. Exp. Clin. Psychopharmacol. 2017, 25, 353–362. [Google Scholar] [CrossRef] [PubMed]
- McKee, S.A.; Smith, P.H.; Kaufman, M.; Mazure, C.M.; Weinberger, A.H. Sex Differences in Varenicline Efficacy for Smoking Cessation: A Meta-Analysis. Nicotine Tob. Res. 2016, 18, 1002–1011. [Google Scholar] [CrossRef]
- Smith, P.H.; Karin, A.K.; Sherry, A.M. Gender differences in medication use and cigarette smoking cessation: Results from the International Tobacco Control Four Country Survey. Nicotine Tob. Res. 2015, 17, 463–472. [Google Scholar] [CrossRef]
- Greenfield, S.F.; Pettinati, H.M.; O’Malley, S.; Randall, P.K.; Randall, C.L. Gender differences in alcohol treatment: An analysis of outcome from the COMBINE study. Alcohol Clin. Exp. Res. 2010, 34, 1803–1812. [Google Scholar] [CrossRef]
- Mason, B.J.; Lehert, P. Acamprosate for alcohol dependence: A sex-specific meta-analysis based on individual patient data. Alcohol Clin. Exp. Res. 2012, 36, 497–508. [Google Scholar] [CrossRef]
- Hitschfeld, M.J.; Schneekloth, T.D.; Ebbert, J.O.; Hall-Flavin, D.K.; Karpyak, V.M.; Abulseoud, O.A.; Patten, C.A.; Geske, J.R.; Frye, M.A. Female smokers have the highest alcohol craving in a residential alcoholism treatment cohort. Drug Alcohol Depend. 2015, 150, 179–182. [Google Scholar] [CrossRef]
- Baros, A.M.; Latham, P.K.; Anton, R.F. Naltrexone and cognitive behavioral therapy for the treatment of alcohol dependence: Do sex differences exist? Alcohol Clin. Exp. Res. 2008, 32, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Herbeck, D.M.; Schneekloth, T.D.; Ebbert, J.O.; Hall-Flavin, D.K.; Karpyak, V.M.; Abulseoud, O.A.; Patten, C.A.; Geske, J.R.; Frye, M.A. Gender differences in treatment and clinical characteristics among patients receiving extended release naltrexone. J. Addict. Dis. 2016, 35, 305–314. [Google Scholar] [CrossRef] [PubMed]
- Pettinati, H.M.; Kampman, K.M.; Lynch, K.G.; Suh, J.J.; Dackis, C.A.; Oslin, D.W.; O’Brien, C.P. Gender differences with high-dose naltrexone in patients with co-occurring cocaine and alcohol dependence. J. Subst. Abuse Treat. 2008, 34, 378–390. [Google Scholar] [CrossRef] [PubMed]
- McHugh, R.K.; Devito, E.E.; Dodd, D.; Carroll, K.M.; Potter, J.S.; Greenfield, S.F.; Connery, H.S.; Weiss, R.D. Gender differences in a clinical trial for prescription opioid dependence. J. Subst. Abuse Treat. 2013, 45, 38–43. [Google Scholar] [CrossRef]
- Johnson, R.M.; Fairman, B.; Gilreath, T.; Xuan, Z.; Rothman, E.F.; Parnham, T.; Furr-Holden, C.D. Past 15-year trends in adolescent marijuana use: Differences by race/ethnicity and sex. Drug Alcohol Depend. 2015, 155, 8–15. [Google Scholar] [CrossRef]
- Legleye, S.; Daniela, P.; Fred, P.; Céline, G.; Myriam, K.; Ludwig, K. Is there a cannabis epidemic model? Evidence from France, Germany and USA. Int. J. Drug Policy 2014, 25, 1103–1112. [Google Scholar] [CrossRef]
- Hall, W.; Louisa, D. Adverse health effects of non-medical cannabis use. Lancet 2009, 374, 1383–1391. [Google Scholar] [CrossRef]
- Lopez-Quintero, C.; Pérez, C.J.; Hasin, D.S.; Okuda, M.; Wang, S.; Grant, B.F.; Blanco, C. Probability and predictors of transition from first use to dependence on nicotine, alcohol, cannabis, and cocaine: Results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Drug Alcohol Depend. 2011, 115, 120–130. [Google Scholar] [CrossRef]
- Noack, R.; Hofler, M.; Lueken, U. Cannabis use patterns and their association with DSM-IV cannabis dependence and gender. Eur. Addict. Res. 2011, 17, 321–328. [Google Scholar] [CrossRef]
- Foster, K.T.; Li, N.; McClure, E.A.; Sonne, S.C.; Gray, K.M. Gender Differences in Internalizing Symptoms and Suicide Risk Among Men and Women Seeking Treatment for Cannabis Use Disorder from Late Adolescence to Middle Adulthood. J. Subst. Abuse Treat. 2016, 66, 16–22. [Google Scholar] [CrossRef]
- Blanco, C.; Rafful, C.; Wall, M.M.; Ridenour, T.A.; Wang, S.; Kendler, K.S. Towards a comprehensive developmental model of cannabis use disorders. Addiction 2014, 109, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.S.; Secades-Villa, R.; Okuda, M.; Wang, S.; Pérez-Fuentes, G.; Kerridge, B.T.; Blanco, C. Gender differences in cannabis use disorders: Results from the National Epidemiologic Survey of Alcohol and Related Conditions. Drug Alcohol Depend. 2013, 130, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Schepis, T.S.; Desai, R.A.; Cavallo, D.A.; Smith, A.E.; McFetridge, A.; Liss, T.B.; Potenza, M.N.; Krishnan-Sarin, S. Gender differences in adolescent marijuana use and associated psychosocial characteristics. J. Addict. Med. 2011, 5, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Kerridge, B.T.; Desai, R.A.; Cavallo, D.A.; Smith, A.E.; McFetridge, A.; Liss, T.B.; Potenza, M.N.; Krishnan-Sarin, S. DSM-5 cannabis use disorder in the National Epidemiologic Survey on Alcohol and Related Conditions-III: Gender-specific profiles. Addict. Behav. 2018, 76, 52–60. [Google Scholar] [CrossRef]
- Cooper, Z.D.; Craft, R.M. Sex-Dependent Effects of Cannabis and Cannabinoids: A Translational Perspective. Neuropsychopharmacology 2017, 43, 34–35. [Google Scholar] [CrossRef]
- Anderson, B.M.; Matthew, R.; Robert, I.B.; Godfrey, P. Sex, drugs, and cognition: Effects of marijuana. J. Psychoact. Drugs 2010, 42, 413–424. [Google Scholar] [CrossRef]
- Cooper, Z.D.; Haney, M. Investigation of sex-dependent effects of cannabis in daily cannabis smokers. Drug Alcohol Depend. 2014, 136, 85–91. [Google Scholar] [CrossRef]
- Fogel, J.S.; Kelly, T.H.; Westgate, P.M.; Lile, J.A. Sex differences in the subjective effects of oral DELTA9-THC in cannabis users. Pharmacol. Biochem. Behav. 2017, 152, 44–51. [Google Scholar] [CrossRef]
- Fattore, L.; Fratta, W. How important are sex differences in cannabinoid action? Br. J. Pharmacol. 2010, 160, 544–548. [Google Scholar] [CrossRef]
- Copersino, M.L.; Boyd, S.J.; Tashkin, D.P.; Huestis, M.A.; Heishman, S.J.; Dermand, J.C.; Simmons, M.S.; Gorelick, D.A. Sociodemographic characteristics of cannabis smokers and the experience of cannabis withdrawal. Am. J. Drug Alcohol Abuse 2010, 36, 311–319. [Google Scholar] [CrossRef]
- Herrmann, E.; Weerts, E.; Vandrey, R. Sex Differences in Cannabis Withdrawal Symptoms Among Treatment-Seeking Cannabis Users. Exp. Clin. Psychopharmacol. 2015, 156, 415–421. [Google Scholar] [CrossRef]
- Sherman, B.J.; McRae-Clark, A.L.; Baker, N.L.; Sonne, S.C.; Killeen, T.K.; Cloud, K.; Gray, K.M. Gender differences among treatment-seeking adults with cannabis use disorder: Clinical profiles of women and men enrolled in the achieving cannabis cessation-evaluating N-acetylcysteine treatment (ACCENT) study. Am. J. Addict. 2017, 26, 136–144. [Google Scholar] [CrossRef]
- Cuttler, C.; Mischley, L.K.; Sexton, M. Sex Differences in Cannabis Use and Effects: A Cross-Sectional Survey of Cannabis Users. Cannabis Cannabinoid Res. 2016, 1, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.P.; Smith, D.C.; Morphew, J.W.; Lei, X.; Zhang, S. Cannabis Withdrawal, Posttreatment Abstinence, and Days to First Cannabis Use Among Emerging Adults in Substance Use Treatment: A Prospective Study. J. Drug Issues 2016, 46, 64–83. [Google Scholar] [CrossRef] [PubMed]
- Lev-Ran, S.; Imtiaz, S.; Taylor, B.J.; Shield, K.D.; Rehm, J.; Foll, B. Gender differences in health-related quality of life among cannabis users: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. Drug Alcohol Depend. 2012, 123, 190–200. [Google Scholar] [CrossRef]
- Marusich, J.A.; Lefever, T.W.; Antonazzo, K.R.; Craft, R.M.; Wiley, J.L. Evaluation of sex differences in cannabinoid dependence. Drug Alcohol Depend. 2014, 137, 20–28. [Google Scholar] [CrossRef]
- Harte-Hargrove, L.C.; Dow-Edwards, D.L. Withdrawal from THC during adolescence: Sex differences in locomotor activity and anxiety. Behav. Brain Res. 2012, 231, 48–59. [Google Scholar] [CrossRef]
- Hemsing, N.; Greaves, L. Gender norms, roles and relations and cannabis use patterns: A scoping review. Int. J. Environ. Res. Public Health. Forthcoming. [CrossRef]
- Marshall, K.; Gowing, L.; Ali, R.; Le Foll, B. Pharmacotherapies for cannabis dependence. Cochrane Database Syst. Rev. 2014, 12. [Google Scholar] [CrossRef]
- Nielsen, S.; Gowing, L.; Sabioni, P.; Le Foll, B. Pharmacotherapies for cannabis dependence. Cochrane Database Syst. Rev. 2019, 1. [Google Scholar] [CrossRef]
- Moher, D.; Iberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Hammarström, A. A tool for developing gender research in medicine: Examples from the medical literature on work life. Gender Med. 2007, 4, S123–S132. [Google Scholar] [CrossRef]
- McCarthy, L.; Milne, E.; Waite, N.; Cooke, M.; Cook, K.; Chang, F.; Sproule, B.A. Sex and gender-based analysis in pharmacy practice research: A scoping review. Res. Soc. Adm. Pharm. 2017, 13, 1045–1054. [Google Scholar] [CrossRef] [PubMed]
- Cornelius, J.R.; Bukstein, O.G.; Douaihy, A.B.; Clark, D.B.; Chung, T.A.; Daley, D.C.; Wood, D.S.; Brown, S.J. Double-blind fluoxetine trial in comorbid MDD-CUD youth and young adults. Drug Alcohol Depend. 2010, 112, 39–45. [Google Scholar] [CrossRef]
- Gray, K.M.; Sonne, S.C.; McClure, E.A.; Ghitza, U.E.; Matthews, A.G.; McRae-Clark, A.L.; Carroll, K.M.; Potter, J.S.; Wiest, K.; Mooney, L.J.; et al. A randomized placebo-controlled trial of N-acetylcysteine for cannabis use disorder in adults. Drug Alcohol Depend. 2017, 177, 249–257. [Google Scholar] [CrossRef]
- McRae-Clark, A.L.; Sonne, S.C.; McClure, E.A.; Ghitza, U.E.; Matthews, A.G.; McRae-Clark, A.L.; Carroll, K.M.; Potter, J.S.; Wiest, K.; Mooney, L.J.; et al. Vilazodone for cannabis dependence: A randomized, controlled pilot trial. Am. J. Addict. 2016, 25, 69–75. [Google Scholar] [CrossRef]
- McRae-Clark, A.L.; Baker, N.L.; Gray, K.M.; Killeen, T.K.; Wagner, A.M.; Brady, K.T.; DeVane, C.L.; Norton, J. Buspirone treatment of cannabis dependence: A randomized, placebo-controlled trial. Drug Alcohol Depend. 2015, 156, 29–37. [Google Scholar] [CrossRef]
- Smith, P.H.; Bessette, A.J.; Weinberger, A.H.; Sheffer, C.E.; McKee, S.A. Sex/gender differences in smoking cessation: A review. Prev. Med. 2016, 92, 135–140. [Google Scholar] [CrossRef]
- Franconi, F.; Campesi, I.; Occhioni, S.; Antonini, P.; Murphy, M.F. Sex and gender in adverse drug events, addiction, and placebo. Handb. Exp. Pharmacol. 2012, 214, 107–126. [Google Scholar]
- Petkovic, J.; Trawin, J.; Dewidar, O.; Yoganathan, M.; Tugwell, P.; Welch, V. Sex/gender reporting and analysis in Campbell and Cochrane systematic reviews: A cross-sectional methods study. Syst. Rev. 2018, 7, 113. [Google Scholar] [CrossRef]
- Song, M.M.; Imonsen, C.K.; Wilson, J.D.; Jenkins, M.R. Development of a PubMed Based Search Tool for Identifying Sex and Gender Specific Health Literature. J. Womens Health 2016, 25, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Morgan, T.; Williams, L.A.; Gott, M. A Feminist Quality Appraisal Tool: Exposing gender bias and gender inequities in health research. Crit. Public Health 2017, 27, 263–274. [Google Scholar] [CrossRef]


{kind=link}
| Research Phase | Model 1: Sex/Gender Differences | Model 2: Sex and Gender-Based Analysis (SGBA) | Model 2(a): SGBA+ | Model 3: Intersectional Approach |
|---|---|---|---|---|
| Research question | Sex/gender included, but not primary focus of study. Sex/gender included in the study design or the reporting but are not specifically stated in the research question or aim of the study. | Specific questions related to sex/gender. Looking for sex/gender differences, or the impact of sex/gender an explicit aim of the study or stated research question. | Specific questions related to sex/gender, and additional subgroups/identities included. Research question includes sex/gender and other factors such as race, age, sexual orientation, etc. | Specific questions related to sex/gender, and additional subgroups/identities included. Research question includes sex/gender and other factors such as race, age, sexual orientation, etc. |
| Data analysis and reporting of findings | Disaggregation by sex/gender; sex as confounder/controlled for (e.g., included in a model). Data related to the outcomes is reported for different sex/gender groups or sex/gender is controlled for in the analysis. | Sex/gender as analysis category Beyond reporting results by different sex/gender group, there is testing of significance between gender groups in relation to the outcomes of the study. | Sex/gender as analysis category; other factors included (e.g., race, SES). There is testing of significance between sex/gender groups in relation to the outcomes of the study and related to other factors such as race, ethnicity, age, etc. But as sperate analysis, not combined into one analysis. Must be beyond reporting demographic characteristics of a sample. | Multi-faceted analysis of multiple factors. More than one factor is included in the same analysis (e.g., comparing young and old white and Hispanic men, to the same 4 groups of women). |
| Interpretation of sex/gender findings | Findings related to sex and gender are not necessarily included in the interpretation of the data. Differences reported are not necessarily explained. | Findings related to sex and/or gender are reported in the discussion/conclusion. The differences reported in the results section are interpreted and explained. | Findings related to sex and/or gender are reported in the discussion/conclusion in relationship to at least another factor. | Findings related to sex and/or gender are reported in the discussion/conclusion in relationship to other factors such as race, age, etc. The differences reported in the results section are interpreted and explained. |
| Use of language | Not dependent on specific aim, design/results and interpretation. | Not dependent on specific interpretation and use of language. | Not dependent on specific interpretation and use of language. | Not dependent on specific interpretation and use of language. |
| Cornelius et al. (2010) [56] | Characteristics and Findings of Included Studies |
|---|---|
| Study design | Randomized controlled trial |
| Participants | Recruitment: Through referrals from the Western Psychiatric Institute and Clinic (WPIC) treatment programs and by responding to newspaper, radio, and bus advertisements. Setting: Outpatient clinic, Pittsburgh, USA. Scheduled for 12 weeks. Participants: In total, 70 participants between 14 and 25 years of age at baseline and comorbid presence of both a current CUD (using DSM-IV) and a current major depressive disorder (MDD). Exclusion criteria: Diagnosis of bipolar disorder, schizoaffective disorder, or schizophrenia; subjects with hyper- or hypothyroidism, significant cardiac, neurological, or renal impairment, and significant liver disease; substance abuse or dependence other than alcohol abuse or dependence, nicotine dependence, or cannabis abuse; any history of intravenous drug use; pregnancy, inability or unwillingness to use contraceptive methods, and an inability to read or understand study forms. Sample size: Intervention, 34; placebo: 36. Demographics: Mean age 21.1 years ±2.4 years; 61% male; 56% Caucasian, 37% African-American. In total, 94% cannabis dependent, using on average of 76% of days in prior month; 20 participants met diagnostic criteria for alcohol dependence; seven for alcohol abuse and 16 reported a history of an antidepressant medication in the moth prior to recruitment. |
| Interventions | Intervention: In total, one capsule of 10 mg of fluoxetine for 2 weeks and increased to two capsules of 10 mg of fluoxetine. Placebo: In total, one capsule of 10 mg of placebo and after 2 weeks, two capsules of 10 mg of placebo. The low dose was used to maximize the safety and minimize the risk of medication side effects. In total, nine sessions of cognitive behavior therapy (CBT) for depression and CUD, and motivation enhancement therapy (MET) for CUD. |
| Outcomes | Severity of abuse or dependence (cannabis and alcohol), number of days of cannabis use, quantity and frequency, number completing the treatment Timeline follow-back method (TLFB) for the cannabis use behaviors and other substance use behaviors; Hamilton Rating Scale for Depression (HAM-D-27) for observer-rated depressive symptoms; Beck Depression Inventory (BDI) for participant-rated depressive symptoms; Number of drinks per drinking day, the number of drinking days, number of heavy drinking days (defined as greater than or equal to four drinks per day for women and five for men); Side Effects Questionnaire for Children and Adolescent for the side effects during each assessment throughout the course of the clinical trial. |
| Findings | The group that received fluoxetine did not have better cannabis or depressive than the group that received placebo. The improvement of the depressive symptoms and decrease of number of days of cannabis use may have resulted either from the psychosocial therapy or the natural course of the disorders. |
| Gray et al. (2017) [57] | |
| Study design | Randomized controlled trial |
| Participants | Recruitment: Community media advertisements. Setting: Outpatient, six sites within the National Drug Abuse Treatment Clinical Trials Network, USA. Scheduled duration 12 weeks. Participants: In total, 302 treatment-seeking adults ages 18–50 with CUD and submitting a positive Urine cannabinoid testing UCT during the initial screening visit. Exclusion criteria: Individuals with acutely unstable medical or psychiatric disorders, DSM-IV-TR substance dependence aside from cannabis or tobacco, contraindications for N-acetylcysteine (NAC) treatment, or recent synthetic cannabinoid use. Sample size: Intervention, 153; placebo, 149. Demographics: Mean age 29.8 years ±8.74 years; 71.5% male; 58.3% White; 27.8% Black or African-American. Mean cannabis use 26.0/30 days at baseline. |
| Interventions | Intervention: In total, two capsules of 600 mg of United States Pharmacopeia grade NAC powder (twice-daily dose). Placebo: In total, two capsules of 600 mg of placebo (twice per day). Riboflavin 25 mg was added to all capsules (100 mg/day total) as a biomarker for medication adherence. All participants received contingence management twice weekly during treatment. Medical management. |
| Outcomes | Urine specimens were collected at baseline, twice weekly throughout treatment, at end-of-treatment. UCT at post-treatment follow-up. Medication adherence included taking ≥80% of prescribed study medication per study week, confirmed by urine riboflavin level >1500 ng/mL. Adverse effects at each study visit. |
| Findings | No statistically significant differences between the NAC and placebo groups in cannabis abstinence. In the NAC group, 22.3% of urine cannabinoid tests were negative compared to 22.4% in the placebo group. Exploratory analysis within medication-adherent subgroups revealed no significant differential abstinence outcomes by treatment group. |
| McRae-Clark et al. (2015) [59] | |
| Study design | Randomized controlled trial. |
| Participants | Recruitment: Media and internet advertisements. Setting: Outpatient. Scheduled duration 12 weeks. Participants: In total, 175 participants between 18 and 65 years of age and met DSM-IV criteria for current cannabis dependence. Exclusion criteria: current dependence on any other substance (with the exception of caffeine and nicotine), history of psychotic, bipolar or eating disorder, current suicidal or homicidal risk, current major depression, current treatment with psychoactive medication (with the exception of stimulants and non-benzodiazepine sedative/hypnotics), major medical illness or disease, significant cognitive impairment, hypersensitivity to buspirone or other product component, current consumption of substances that inhibit or induce CYP3A4, and pregnancy, lactation or inadequate birth control. Sample size: intervention, 88; placebo, 87. Demographics: Mean age 24.00 years (23.1-25 years); 76.6% male; 64% Caucasian. |
| Interventions | Intervention: Dosage initiated at 5 mg buspirone or placebo twice daily and increased by 5–10 mg every three to four days as tolerated, to a maximum dose of 60 mg daily for 12 weeks. Placebo: Up to 60 mg of placebo. Adjunctive motivational enhancement therapy sessions (MET) during the first four weeks of the treatment period. |
| Outcomes | Semi-quantitative urine cannabinoid tests (UCTs) for cannabinoids administered at screening and weekly throughout the study. Proportion of negative urine test during treatment. Point prevalence of abstinence by urine test at the end of the treatment Number of reporting adverse events. |
| Findings | No differences of UCTs and the weekly creatinine adjusted cannabinoid levels between the two groups. Although participants in both groups reduced their cannabis craving over the course of the study, there were no differences between the buspirone and placebo groups. However, participants who attained abstinence from cannabis reported less cannabis craving. |
| McRae-Clark et al. (2016) [58] | |
| Study design | Randomized controlled trial |
| Participants | Recruitment: Media and internet advertisements. Setting: Outpatient, 8 weeks. Participants: In total, 76 participants between 18 and 65 years of age and CUD. Exclusion criteria: current dependence on any other substance (exception caffeine and nicotine), history of psychotic, bipolar, or eating disorder, current suicidal or homicidal risk, current treatment with psychoactive medication (exception stimulants and non-benzodiazepine sedative/hypnotics) or CYP3A4 inhibitors, major medical illness or disease, pregnancy, lactation, or inadequate birth control, patients that would be unable to comply with study procedures or assessments. Sample size: Intervention, 41; placebo, 35. Demographics: Mean age 22.2 (21.3–23.1) years; 79% male; 54.8% Caucasian. |
| Interventions | Intervention: In total, 10 mg daily dose of Vilazodone tablets provided by Forest Pharmaceuticals for 7 days, increased to 20 mg daily for 7 days, followed by 40 mg daily as tolerated. Placebo: In total, 10 mg daily dose of placebo tablets for 7 days, increased to 20 mg daily for 7 days, followed by 40 mg daily. Both groups received three adjunctive motivational enhancement therapy sessions (MET). First session, prior to medication initiation. Second session, approximately 1 week later. Third session, week 4. |
| Outcomes | Quantitative urine cannabinoid tests (UCTs) for cannabinoids administered at screening and weekly throughout the study. Self-report cannabis use measured by TLFB (Time-Line Follow-Back). Marijuana Craving Questionnaire (MCQ) for levels of cannabis craving. Adverse effects assessed weekly. Medication compliance by weekly patient report. Proportion of scheduled visits attended. |
| Findings | The vilazodone group did not show greater efficacy when compared to the placebo group on cannabis use outcomes. Participants in both groups reported lower cannabis use with no differences between the two groups. |
| Authors | Publication Date | SGBA Categorization | Sex/Gender in the Research Question | Results | Interpretation of Sex/Gender Findings | Use of Terminology | Findings Related to Sex and Gender |
|---|---|---|---|---|---|---|---|
| [56] | 2010 | Sex/Gender Differences | No | Sex by time was analyzed in relation to the outcomes. | No | Use only sex | Females showed a greater improvement with time on the depressive symptoms and DSM cannabis abuse criteria count than males. |
| [57] | 2017 | Sex/Gender Differences | No | Examined whether sex was a predictor of cannabis abstinence, and whether there was a sex-by-treatment interaction. | No | Sex and gender used interchangeably | Sex was not a significant predictor of cannabis abstinence, and there was no sex-by-treatment interaction. |
| [59] | 2015 | SGBA | No | Sex was used as a randomized stratification variable. Sex was analyzed in relationship to the negative UCTs and cannabinoid levels. | Yes | Sex and gender used interchangeably | In males, 8.7% of buspirone participant UCTs were negative and 4.5% of placebo UCTs were negative. In females, 2.4% of buspirone participant UCTs were negative and 12.9% of placebo; although the difference was not statistically significant (p = 0.007). There was a sex by treatment interaction for the creatinine adjusted cannabinoid levels: for males, those randomized to buspirone treatment had significantly lower creatinine adjusted cannabinoid levels as compared to those randomized to placebo; for females, those randomized to placebo had lower creatinine adjusted cannabinoid levels compared to those randomized to buspirone. |
| [58] | 2016 | SGBA | No | Sex was used as a variable for randomization. Sex and sex by treatment group interactions were analyzed. | Yes | Sex and gender used interchangeably | Men had significantly lower creatinine-adjusted cannabinoid levels and a trend for increased negative urine cannabinoid tests than women. There were no sex differences regarding the self-reported frequency and amount of cannabis use; nor significant interactions between sex and treatment. Male participants randomized to vilazodone showed a reduction in the Purposefulness subscale of the MCQ; it did not happen for females. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brabete, A.C.; Greaves, L.; Hemsing, N.; Stinson, J. Sex- and Gender-Based Analysis in Cannabis Treatment Outcomes: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 872. https://doi.org/10.3390/ijerph17030872
Brabete AC, Greaves L, Hemsing N, Stinson J. Sex- and Gender-Based Analysis in Cannabis Treatment Outcomes: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(3):872. https://doi.org/10.3390/ijerph17030872
Chicago/Turabian StyleBrabete, Andreea C., Lorraine Greaves, Natalie Hemsing, and Julie Stinson. 2020. "Sex- and Gender-Based Analysis in Cannabis Treatment Outcomes: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 3: 872. https://doi.org/10.3390/ijerph17030872
APA StyleBrabete, A. C., Greaves, L., Hemsing, N., & Stinson, J. (2020). Sex- and Gender-Based Analysis in Cannabis Treatment Outcomes: A Systematic Review. International Journal of Environmental Research and Public Health, 17(3), 872. https://doi.org/10.3390/ijerph17030872