The Night Side of Blood Pressure: Nocturnal Blood Pressure Dipping and Emotional (dys)Regulation

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Method
2.1. Participants
2.2. Assessment Tools
2.2.1. Physiological Measures
2.2.2. Ambulatory Blood Pressure Monitors (ABPM)
2.3. Socio-Demographic and Anamnestic Information
2.4. Questionnaires
20-Item Toronto Alexithymia Scale (TAS-20)
2.5. Procedure
2.6. Data Analyses
3. Results

{kind=link}
{kind=link}
{kind=link}
| Non-Dippers | Dippers | Extreme Dippers | F/χ2 | p | |
|---|---|---|---|---|---|
| n (Female/Male) | 70 (35/35) | 70 (36/34) | 70 (36/34) | ||
| Age | 59.99 (8.46) | 56.10 (10.13) | 53.69 (9.04) | 8.29 | 0.001 |
| Years of education | 11.72 (3.23) | 12.66 (3.95) | 13.56 (4.22) | 3.05 | 0.06 |
| Body mass index (BMI) | 26.64 (4.99) | 25.88 (4.28) | 26.47 (3.69) | <1 | 0.56 |
| Systolic blood pressure (SBP) | 140.61 (22.50) | 141.82 (18.68) | 141.67 (18.62) | <1 | 0.93 |
| Diastolic blood pressure (DBP) | 88.26 (12.30) | 91.57 (12.08) | 92.18 (10.50) | 2.26 | 0.11 |
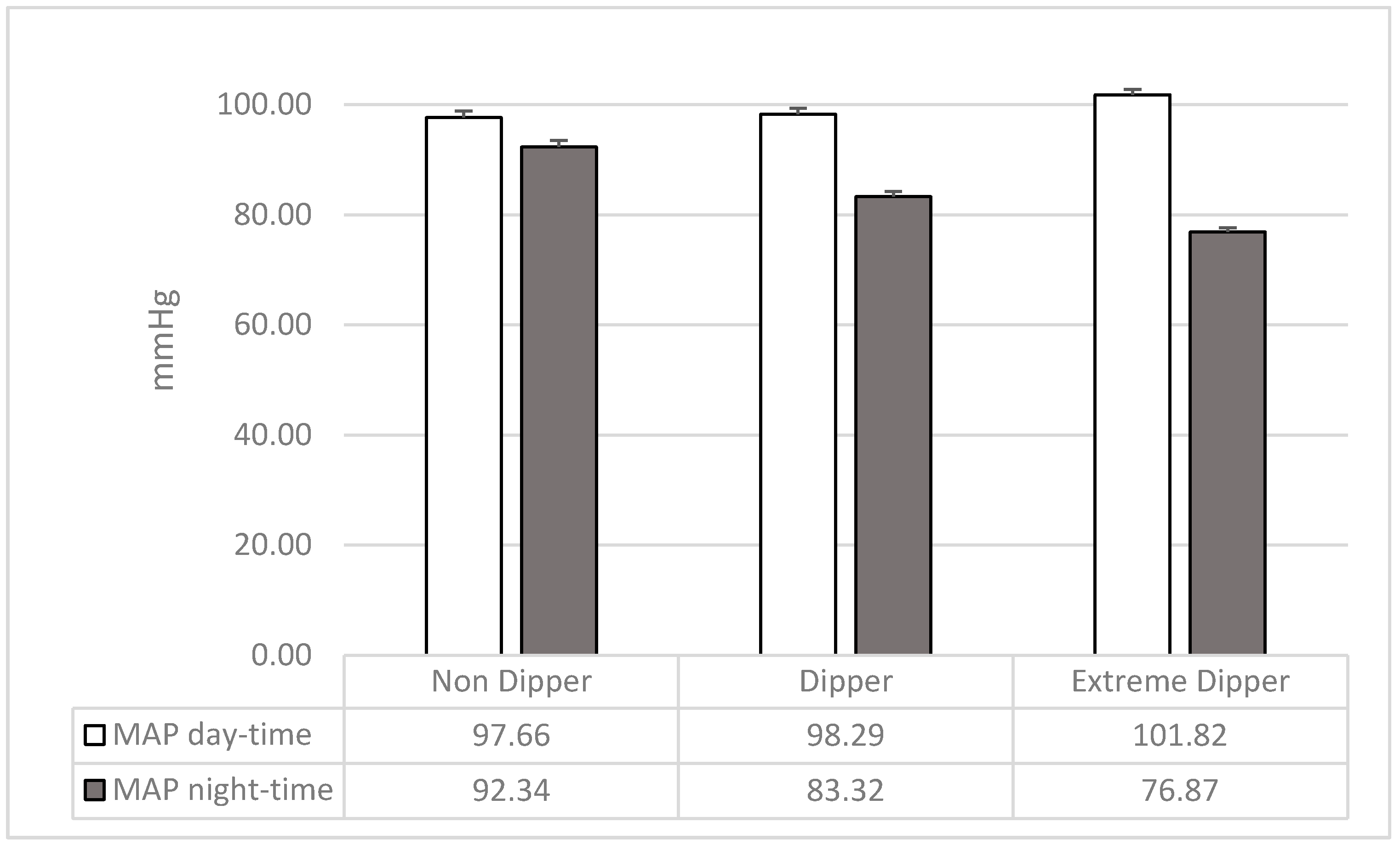
| Mean arterial pressure day (MAP) | 97.66 (10.08) | 98.30 (9.00) | 101.82 (8.16) | 4.24 | 0.02 |
| Mean arterial pressure night (MAP) | 92.15 (9.89) | 83.00 (7.40) | 76.67 (6.53) | 65.13 | 0.0001 |
| Dipping ratio MAP | 0.95 (0.03) | 0.85 (0.03) | 0.76 (0.03) | 675.4 | 0.0001 |
| Smoking cigarettes (number per day) | 0.30 (0.75) | 0.51 (0.88) | 0.32 (0.67) | 1.50 | 0.23 |
| Alcohol consumption (number of glasses per day) | 0.36 (0.48) | 0.40 (0.52) | 0.31 (0.53) | <1 | 0.60 |
| Hypertensive conditions (n (%)) | 16.98 | 0.02 | |||
| Normotensive | 14 (39) | 9 (25) | 13 (36) | ||
| Hypertensive untreated | 11 (16.7) a | 23 (34.8) | 32 (48.5) a | ||
| Hypertensive treated | 45 (41.7) b | 38 (35.2) | 25 (23.1) b | ||
| Alexithymic condition | 19.34 | 0.001 | |||
| Non-alexithymic | 46 (32.1) | 55 (38.5) | 42 (29.4) | ||
| Moderately alexithymic | 15 (32.6) | 15 (32.6) | 16 (34.8) | ||
| Alexithymic | 9 (42.9) c | 0 (0.0) cd | 12 (57.1) d |
3.1. Demographical, Physiological, and Lifestyle Variables
3.2. Alexithymia
3.3. Alexithymia in Normotensive and Hypertensive Subgroups
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kario, K.; Schwartz, J.E.; Pickering, T.G. Changes of nocturnal blood pressure dipping status in hypertensives by nighttime dosing of α-adrenergic blocker, doxazosin: Results from the HALT Study. Hypertension 2000, 35, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Bishop, G.D.; Pek, J.; Ngau, F. Blunted cardiovascular responses to daytime activities as related to reduced nocturnal blood pressure decline. Ann. Behav. Med. 2006, 31, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Fagard, R.H.; Celis, H.; Thijs, L.; Staessen, J.A.; Clement, D.L.; De Buyzere, M.L.; De Bacquer, D.A. Daytime and nighttime blood pressure as predictors of death and cause-specific cardiovascular events in hypertension. Hypertension 2008, 51, 55–61. [Google Scholar] [CrossRef] [PubMed]
- De La Sierra, A.; Redon, J.; Banegas, J.R.; Segura, J.; Parati, G.; Gorostidi, M.; Vinyoles, E. Prevalence and factors associated with circadian blood pressure patterns in hypertensive patients. Hypertension 2009, 53, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Smolensky, M.H.; Haus, E. Circadian rhythms and clinical medicine with applications to hypertension. Am. J. Hypert. 2001, 14, 280S–290S. [Google Scholar] [CrossRef]
- Tadic, M.; Cuspidi, C.; Grassi, G. Heart rate as a predictor of cardiovascular risk. Eur. J. Clin. Investig. 2018, 48, e12892. [Google Scholar] [CrossRef]
- Ohkubo, T.; Hozawa, A.; Yamaguchi, J.; Kikuya, M.; Ohmori, K.; Michimata, M.; Tsuji, I. Prognostic significance of the nocturnal decline in blood pressure in individuals with and without high 24-h blood pressure: The Ohasama study. J. Hypertens. 2002, 20, 2183–2189. [Google Scholar] [CrossRef]
- Hermida, R.C.; Ayala, D.E.; Mojón, A.; Fernández, J.R. Influence of circadian time of hypertension treatment on cardiovascular risk: Results of the MAPEC study. Chronobiol. Int. 2010, 27, 1629–1651. [Google Scholar] [CrossRef]
- Surtees, P.G.; Wainwright, N.W.; Khaw, K.T.; Day, N.E. Functional health status, chronic medical conditions and disorders of mood. Br. J. Psychiatry 2003, 183, 299–303. [Google Scholar] [CrossRef]
- Shen, B.J.; Countryman, A.J.; Spiro, A.; Niaura, R. The prospective contribution of hostility characteristics to high fasting glucose levels: The moderating role of marital status. Diabetes Care 2008, 31, 1293–1298. [Google Scholar] [CrossRef][Green Version]
- Casagrande, M.; Boncompagni, I.; Mingarelli, A.; Favieri, F.; Forte, G.; Germanò, R.; Guarino, A. Coping styles in individuals with hypertension of varying severity. Stress Health 2019, 35, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Casagrande, M.; Mingarelli, A.; Guarino, A.; Favieri, F.; Boncompagni, I.; Germanò, R.; Forte, G. Alexithymia: A facet of uncontrolled hypertension. Int. J. Psychophysiol. 2019, 146, 180–189. [Google Scholar] [CrossRef] [PubMed]
- Todarello, O.; Taylor, G.J.; Parker, J.D.; Fanelli, M. Alexithymia in essential hypertensive and psychiatric outpatients: A comparative study. J. Psychosom. Res. 1995, 39, 987–994. [Google Scholar] [CrossRef]
- Jula, A.; Salminen, J.K.; Saarijärvi, S. Alexithymia: A facet of essential hypertension. Hypertension 1999, 33, 1057–1061. [Google Scholar] [CrossRef] [PubMed]
- Mezick, E.J.; Matthews, K.A.; Hall, M.; Kamarck, T.W.; Strollo, P.J.; Buysse, D.J.; Reis, S.E. Low life purpose and high hostility are related to an attenuated decline in nocturnal blood pressure. Health Psychol. 2010, 29, 196. [Google Scholar] [CrossRef] [PubMed]
- Linden, W.; Klassen, K.; Phillips, M. Can psychological factors account for a lack of nocturnal blood pressure dipping? Ann. Behav. Med. 2008, 36, 253–258. [Google Scholar] [CrossRef]
- Casagrande, M.; Favieri, F.; Guarino, A.; Di Pace, E.; Langher, V.; Germanò, G.; Forte, G. The Night Effect of Anger: Relationship with Nocturnal Blood Pressure Dipping. Int. J. Environ. Res. Public Health 2020, 17, 2705. [Google Scholar] [CrossRef]
- Kario, K.; Pickering, T.G.; Matsuo, T.; Hoshide, S.; Schwartz, J.E.; Shimada, K. Stroke prognosis and abnormal nocturnal blood pressure falls in older hypertensives. Hypertension 2001, 38, 852–857. [Google Scholar] [CrossRef]
- Troxel, W.M.; Buysse, D.J.; Monk, T.H.; Begley, A.; Hall, M. Does social support differentially affect sleep in older adults with versus without insomnia? J. Psychosom. Res. 2010, 69, 459–466. [Google Scholar] [CrossRef]
- Tomfohr, L.; Pung, M.A.; Edwards, K.M.; Dimsdale, J.E. Racial differences in sleep architecture: The role of ethnic discrimination. Biol. Psychol. 2012, 89, 34–38. [Google Scholar] [CrossRef]
- Fan, L.B.; Blumenthal, J.A.; Hinderliter, A.L.; Sher wood, A. The effect of job strain on nighttime blood pressure dipping among men and women with high blood pressure. Scand. J. Work Environ. Health 2013, 39, 112. [Google Scholar] [CrossRef] [PubMed]
- Pierdomenico, S.D.; Pierdomenico, A.M.; Coccina, F.; Lapenna, D.; Porreca, E. Circadian blood pressure changes and cardiovascular risk in elderly-treated hypertensive patients. Hypertens. Res. 2016, 39, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, T.; Yano, Y.; Hoshide, S.; Kanegae, H.; Kario, K. Association of cardiovascular outcomes with masked hypertension defined by home blood pressure monitoring in a Japanese general practice population. JAMA Cardiol. 2018, 3, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Mancia, G.; Fagard, R.; Narkiewicz, K.; Redán, J.; Zanchetti, A.; Böhm, M.; Galderisi, M. 2013 Practice guidelines for the management of arterial hypertension of the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC): ESH/ESC Task Force for the Management of Arterial Hypertension. J. Hypertens. 2013, 31, 1925–1938. [Google Scholar] [CrossRef]
- O’Brien, E.; Asmar, R.; Beilin, L.; Imai, Y.; Mancia, G.; Mengden, T.; Pickering, T. Practice guidelines of the European Society of Hypertension for clinic, ambulatory and self blood pressure measurement. J. Hypertens. 2005, 23, 697–701. [Google Scholar] [CrossRef]
- Loredo, J.S.; Nelesen, R.; Ancoli-Israel, S.; Dimsdale, J.E. Sleep quality and blood pressure dipping in normal adults. Sleep 2004, 27, 1097–1103. [Google Scholar] [CrossRef]
- Bagby, R.M.; Parker, J.D.; Taylor, G.J. The twenty-item Toronto Alexithymia Scale—I. Item selection and cross-validation of the factor structure. J. Psychosom. Res. 1994, 38, 23–32. [Google Scholar] [CrossRef]
- Bressi, C.; Taylor, G.; Parker, J.; Bressi, S.; Brambilla, V.; Aguglia, E.; Todarello, O. Cross validation of the factor structure of the 20-item Toronto Alexithymia Scale: An Italian multicenter study. J. Psychosom. Res. 1996, 41, 551–559. [Google Scholar] [CrossRef]
- Friedman, O.; Logan, A.G. Can nocturnal hypertension predict cardiovascular risk? Integr. Blood Press. Control 2009, 2, 25. [Google Scholar]
- Thomas, K.S.; Nelesen, R.A.; Dimsdale, J.E. Relationships between hostility, anger expression, and blood pressure dipping in an ethnically diverse sample. Psychosom. Med. 2004, 66, 298–304. [Google Scholar]
- Thayer, J.F.; Hansen, A.L.; Saus-Rose, E.; Johnsen, B.H. Heart rate variability, prefrontal neural function, and cognitive performance: The neurovisceral integration perspective on self-regulation, adaptation, and health. Ann. Behav. Med. 2009, 37, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Biaggioni, I. Circadian clocks, autonomic rhythms, and blood pressure dipping. Hypertension 2008, 52, 797–798. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, E.; Coats, A.; Owens, P.; Petrie, J.; Padfield, P.L.; Littler, W.A.; Mee, F. Use and interpretation of ambulatory blood pressure monitoring: Recommendations of the British Hypertension Society. BMJ 2000, 320, 1128–1134. [Google Scholar] [CrossRef] [PubMed]
- Pickering, T.G.; Kario, K. Nocturnal non-dipping: What does it augur? Curr. Opin. Nephrol. Hypertens. 2001, 10, 611–616. [Google Scholar] [CrossRef]
- Forte, G.; Casagrande, M. Heart rate variability and cognitive function: A systematic review. Front. Neurosci. 2019, 13, 710. [Google Scholar] [CrossRef] [PubMed]
- Forte, G.; De Pascalis, V.; Favieri, F.; Casagrande, M. Effects of Blood Pressure on Cognitive Performance: A Systematic Review. J. Clin. Med. 2020, 9, 34. [Google Scholar] [CrossRef]
- Hypertension, D.A.; Dawood, T.; Lambert, E.A.; Esler, M.D.; Haikerwal, D.; Brenchley, C.; Lambert, G.W. Sympathetic activity in major depressive disorder: Identifying those at increased cardiac risk? J. Hypertens. 2007, 25, 2117–2124. [Google Scholar]
- Roth, W.T.; Doberenz, S.; Dietel, A.; Conrad, A.; Mueller, A.; Wollburg, E.; Kim, S. Sympathetic activation in broadly defined generalized anxiety disorder. J. Psychiatr. Res. 2008, 42, 205–212. [Google Scholar] [CrossRef]
- Moriguchi, Y.; Komaki, G. Neuroimaging studies of alexithymia: Physical, affective, and social perspectives. BioPsychoSocial Med. 2013, 7, 8. [Google Scholar] [CrossRef]
- Kuwaki, T.; Zhang, W. Orexin neurons as arousal-associated modulators of central cardiorespiratory regulation. Respir. Physiol. Neurobiol. 2010, 174, 43–54. [Google Scholar] [CrossRef]
- Neumann, S.A.; Sollers, J.J., III; Thayer, J.F.; Waldstein, S.R. Alexithymia predicts attenuated autonomic reactivity, but prolonged recovery to anger recall in young women. Int. J. Psychophysiol. 2004, 53, 183–195. [Google Scholar] [CrossRef] [PubMed]
- Goerlich, K.S. Electrophysiology of Alexithymia. In Alexithymia: Advances in Research, Theory, and Clinical Practice; Cambridge University Press: Cambridge, UK, 2018; p. 250. [Google Scholar]
- Stergiou, G.S.; Bliziotis, I.A. Home blood pressure monitoring in the diagnosis and treatment of hypertension: A systematic review. Am. J. Hypertens. 2011, 24, 123–134. [Google Scholar] [CrossRef] [PubMed]



| Non Dippers | Dippers | Extreme Dippers | F | p | |
|---|---|---|---|---|---|
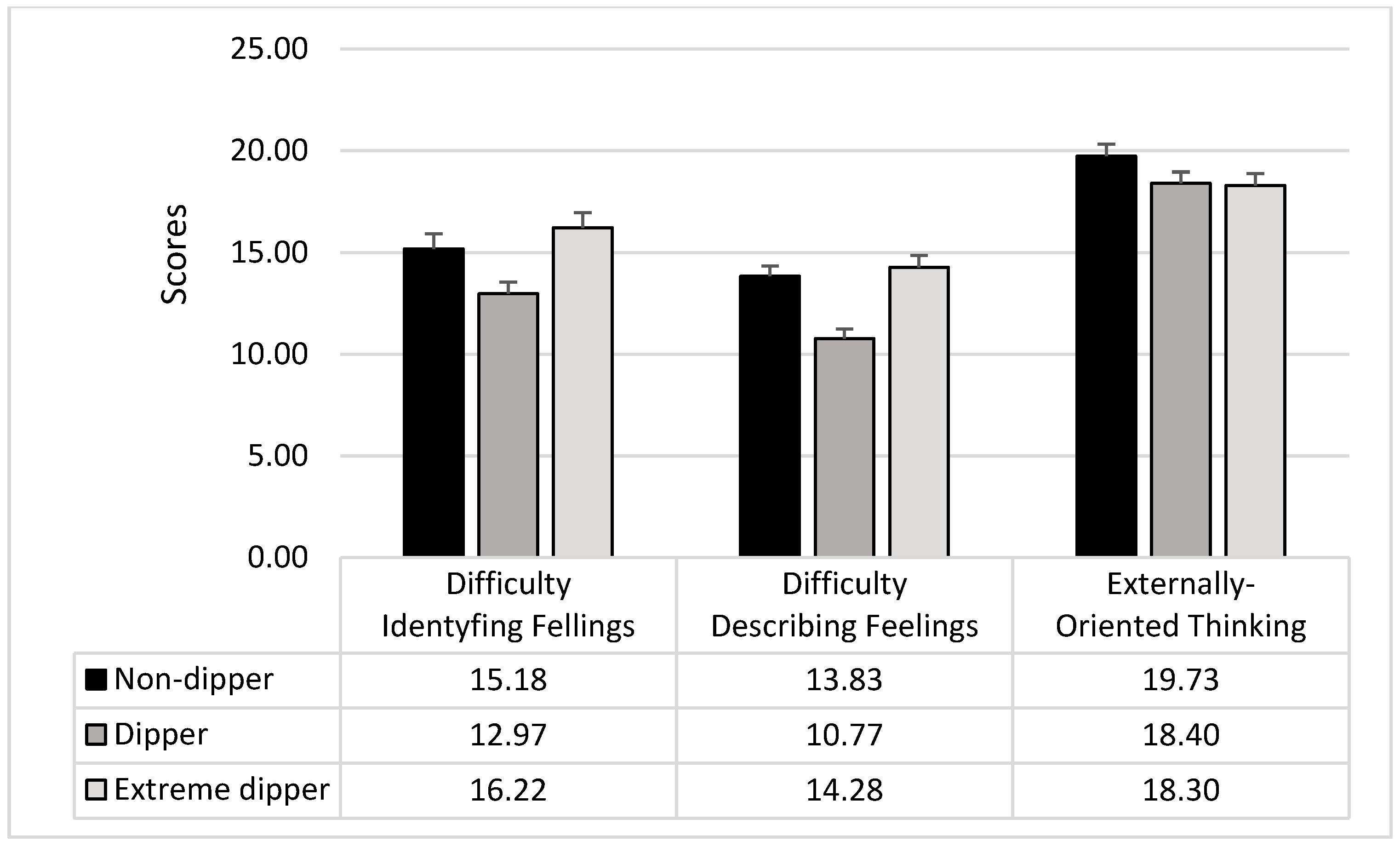
| DIF | 15.18 (6.28) | 12.97 (4.89) | 16.22 (6.27) | 5.63 | 0.005 |
| DDF | 13.83 (4.20) | 10.77 (3.93) | 14.28 (4.84) | 13.56 | 0.0001 |
| EOT | 19.73 (4.95) | 18.40 (4.71) | 18.30 (4.87) | 1.91 | 0.15 |
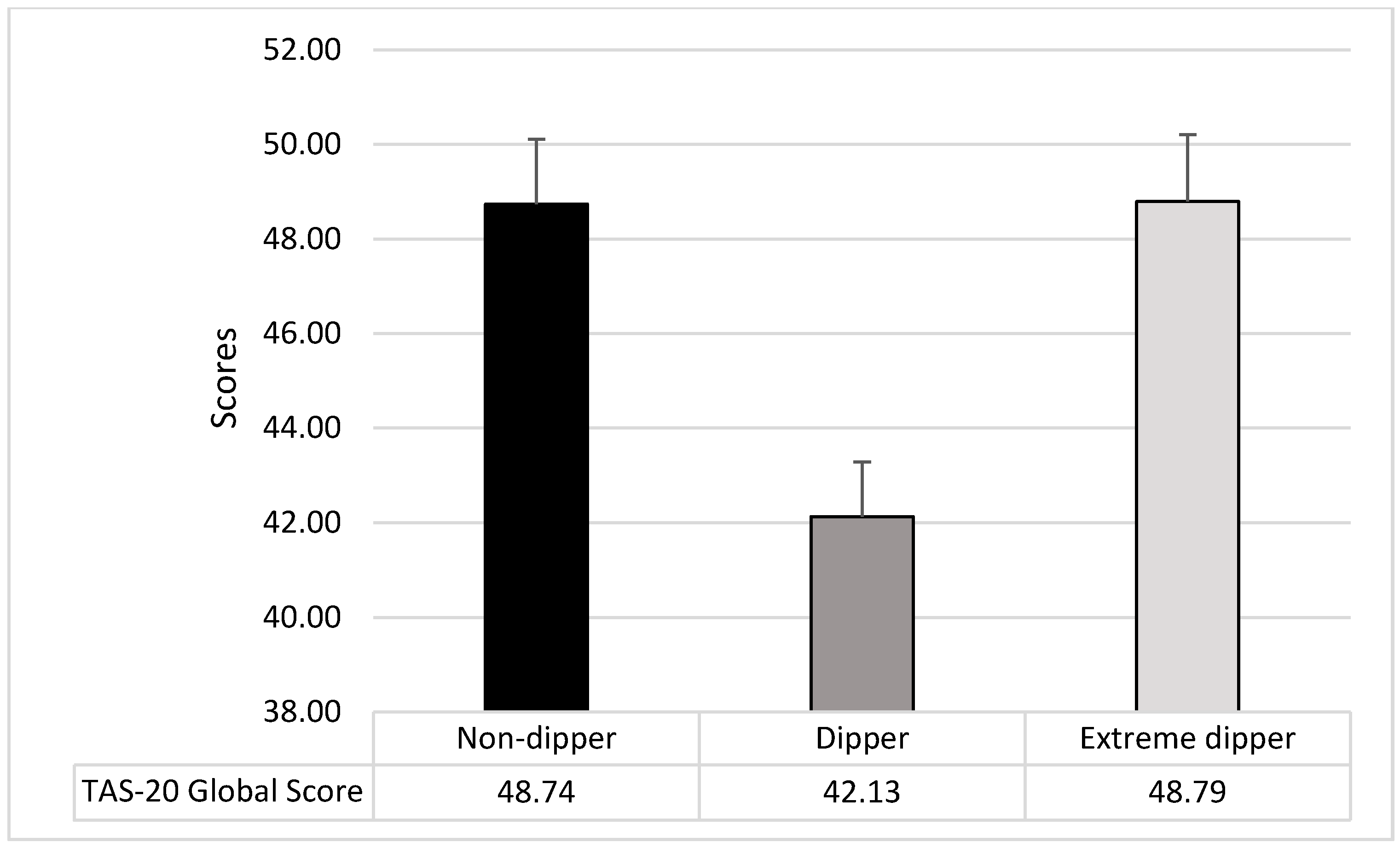
| Total score | 48.74 (11.43) | 42.13 (9.67) | 48.79 (11.86) | 8.45 | 0.0003 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casagrande, M.; Favieri, F.; Langher, V.; Guarino, A.; Di Pace, E.; Germanò, G.; Forte, G. The Night Side of Blood Pressure: Nocturnal Blood Pressure Dipping and Emotional (dys)Regulation. Int. J. Environ. Res. Public Health 2020, 17, 8892. https://doi.org/10.3390/ijerph17238892
Casagrande M, Favieri F, Langher V, Guarino A, Di Pace E, Germanò G, Forte G. The Night Side of Blood Pressure: Nocturnal Blood Pressure Dipping and Emotional (dys)Regulation. International Journal of Environmental Research and Public Health. 2020; 17(23):8892. https://doi.org/10.3390/ijerph17238892
Chicago/Turabian StyleCasagrande, Maria, Francesca Favieri, Viviana Langher, Angela Guarino, Enrico Di Pace, Giuseppe Germanò, and Giuseppe Forte. 2020. "The Night Side of Blood Pressure: Nocturnal Blood Pressure Dipping and Emotional (dys)Regulation" International Journal of Environmental Research and Public Health 17, no. 23: 8892. https://doi.org/10.3390/ijerph17238892
APA StyleCasagrande, M., Favieri, F., Langher, V., Guarino, A., Di Pace, E., Germanò, G., & Forte, G. (2020). The Night Side of Blood Pressure: Nocturnal Blood Pressure Dipping and Emotional (dys)Regulation. International Journal of Environmental Research and Public Health, 17(23), 8892. https://doi.org/10.3390/ijerph17238892