Acute Effects of ACL Injury-Prevention Warm-Up and Soccer-Specific Fatigue Protocol on Dynamic Knee Valgus in Youth Male Soccer Players

 ,
,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.2.1. Single-Leg Squat (SLS) Test
2.2.2. ACL Injury Prevention Protocol (ACL-IPP)
Knee-Band Squat Exercise
Side-Steps Exercise
Bulgarian Split-Squat Exercise
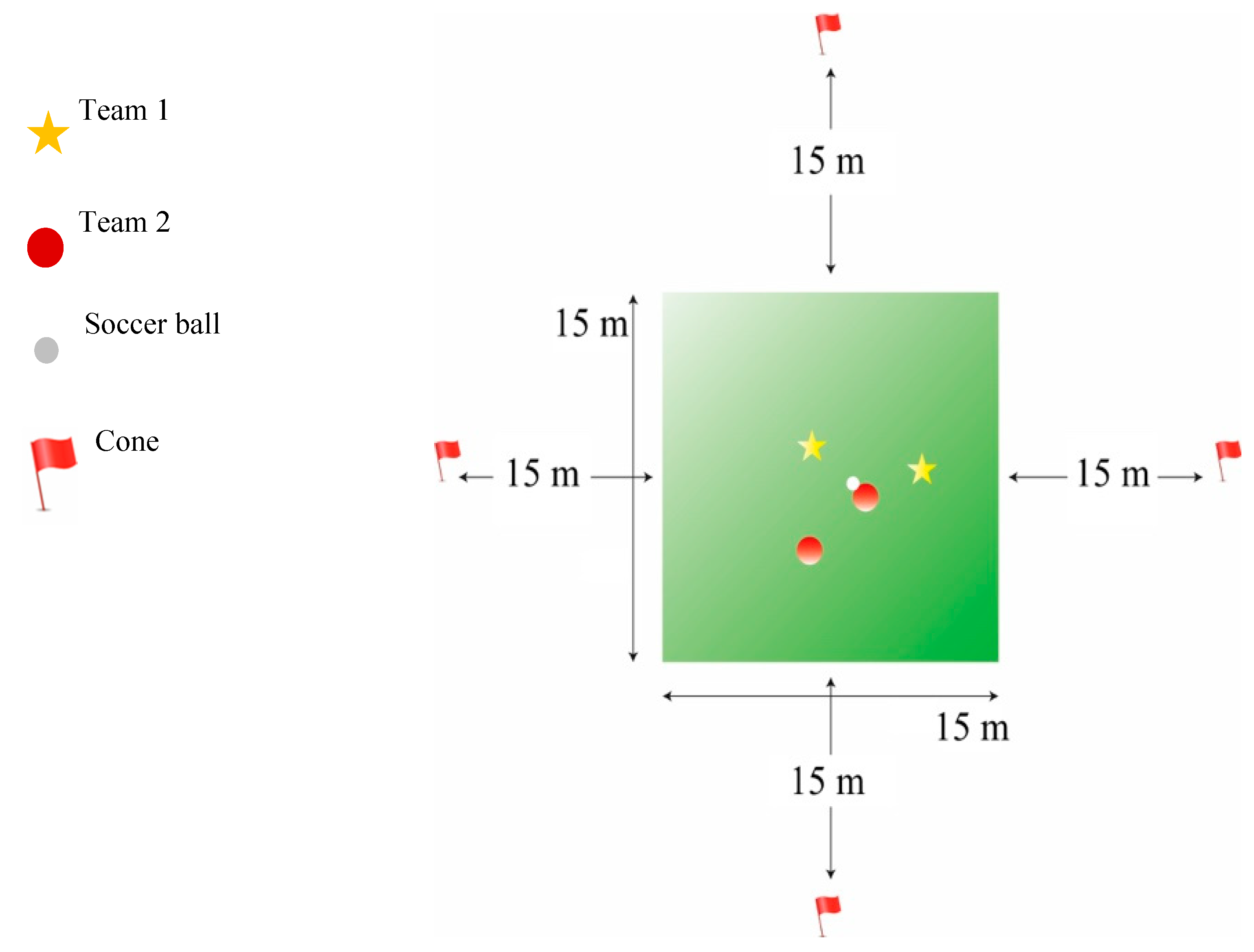
2.2.3. Soccer-Specific Fatigue Protocol (SSFP)
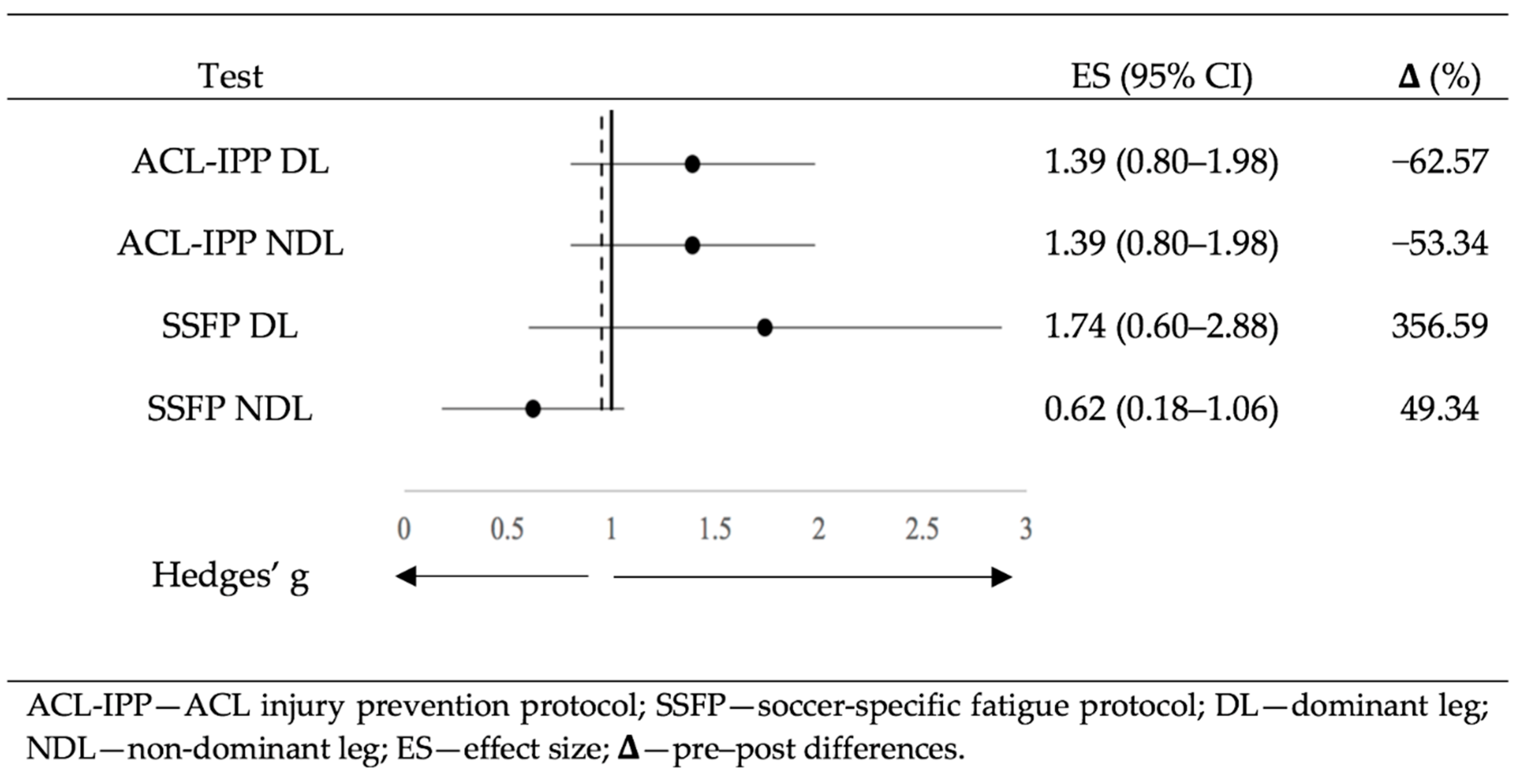
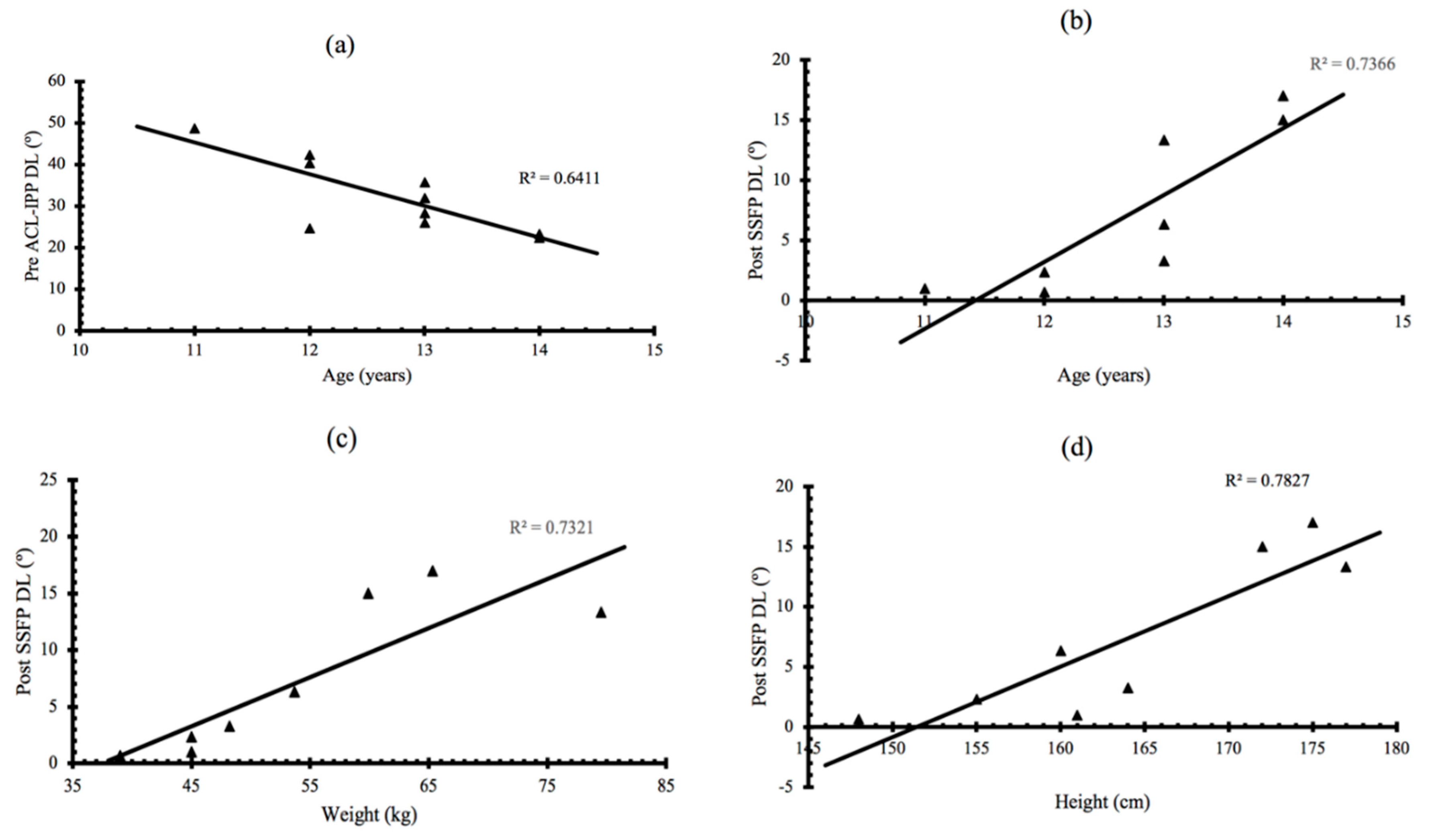
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Reilly, T.; Bangsbo, J.; Franks, A. Anthropometric and physiological predispositions for elite soccer. J. Sports Sci. 2000, 18, 669–683. [Google Scholar] [CrossRef] [PubMed]
- Niu, W.; Feng, T.; Jiang, C.; Zhang, M. Peak vertical ground reaction force during two-leg landing: A systematic review and mathematical modeling. Biomed Res. Int. 2014, 2014, 126860. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Heidt, R.S., Jr.; Colosimo, A.J.; McLean, S.G.; van den Bogert, A.J.; Paterno, M.V.; Succop, P. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am. J. Sports Med. 2005, 33, 492–501. [Google Scholar] [CrossRef]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of muscle injuries in professional football (soccer). Am. J. Sports Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Inklaar, H.; Bol, E.; Schmikli, S.; Mosterd, W. Injuries in male soccer players: Team risk analysis. Int. J. Sports Med. 1996, 17, 229–234. [Google Scholar] [CrossRef] [PubMed]
- Peterson, L.; Junge, A.; Chomiak, J.; Graf-Baumann, T.; Dvorak, J. Incidence of football injuries and complaints in different age groups and skill-level groups. Am. J. Sports Med. 2000, 28, S51–S57. [Google Scholar] [CrossRef] [PubMed]
- Bjordal, J.M.; Arnły, F.; Hannestad, B.; Strand, T. Epidemiology of anterior cruciate ligament injuries in soccer. Am. J. Sports Med. 1997, 25, 341–345. [Google Scholar] [CrossRef]
- Chahla, J.; Sherman, B.; Cinque, M.; Miranda, A.; Garrett, W.E.; Chiampas, G.; O’Malley, H.; Gerhardt, M.B.; Mandelbaum, B.R. Epidemiological findings of soccer injuries during the 2017 Gold Cup. Orthop. J. Sports Med. 2018, 6, 8. [Google Scholar] [CrossRef]
- Gianotti, S.M.; Marshall, S.W.; Hume, P.A.; Bunt, L. Incidence of anterior cruciate ligament injury and other knee ligament injuries: A national population-based study. J. Sci. Med. Sport 2009, 12, 622–627. [Google Scholar] [CrossRef]
- Agel, J.; Arendt, E.A.; Bershadsky, B. Anterior cruciate ligament injury in national collegiate athletic association basketball and soccer: A 13-year review. Am. J. Sports Med. 2005, 33, 524–530. [Google Scholar] [CrossRef]
- Boden, B.P.; Dean, C.S.; Feagin, J.A.; Garrett, W.E. Mechanisms of anterior cruciate ligament injury. Orthopedics 2000, 23, 573–578. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Clarsen, B.; Ekstrand, J. Why we should focus on the burden of injuries and illnesses, not just their incidence. Br. J. Sports Med. 2018, 52, 1018–1021. [Google Scholar] [CrossRef] [PubMed]
- Caraffa, A.; Cerulli, G.; Projetti, M.; Aisa, G.; Rizzo, A. Prevention of anterior cruciate ligament injuries in soccer: A prospective controlled study of proprioceptive training. Knee Surg. Sports Traumatol. Arthrosc. 1996, 4, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Rekik, R.N.; Tabben, M.; Eirale, C.; Landreau, P.; Bouras, R.; Wilson, M.G.; Gillogly, S.; Bahr, R.; Chamari, K. ACL injury incidence, severity and patterns in professional male soccer players in a Middle Eastern league. BMJ Open Sport Exerc. Med. 2018, 4, e000461. [Google Scholar] [CrossRef] [PubMed]
- Ingersoll, C.D.; Grindstaff, T.L.; Pietrosimone, B.G.; Hart, J.M. Neuromuscular consequences of anterior cruciate ligament injury. Clin. Sports Med. 2008, 27, 383–404. [Google Scholar] [CrossRef]
- Salmon, L.; Russell, V.; Musgrove, T.; Pinczewski, L.; Refshauge, K. Incidence and risk factors for graft rupture and contralateral rupture after anterior cruciate ligament reconstruction. Arthrosc. J. Arthrosc. Relat. Surg. 2005, 21, 948–957. [Google Scholar] [CrossRef] [PubMed]
- Friel, N.A.; Chu, C.R. The role of ACL injury in the development of Posttraumatic knee osteoarthritis. Clin. Sports Med. 2013, 32, 1–12. [Google Scholar] [CrossRef]
- Mather, R.C.; Koenig, L.; Kocher, M.S.; Dall, T.M.; Gallo, P.; Scott, D.J.; Bach, B.R.; Spindler, K.P. Societal and economic impact of anterior cruciate ligament tears. J. Bone Jt. Surg. Am. Vol. 2013, 95, 1751–1759. [Google Scholar] [CrossRef]
- Kvist, J.; Ek, A.; Sporrstedt, K.; Good, L. Fear of re-injury: A hindrance for returning to sports after anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2005, 13, 393–397. [Google Scholar] [CrossRef]
- Brophy, R.H.; Wright, R.W.; Matava, M.J. Cost analysis of converting from single-bundle to double-bundle anterior cruciate ligament reconstruction. Am. J. Sports Med. 2009, 37, 683–687. [Google Scholar] [CrossRef]
- Beck, N.A.; Lawrence, J.T.R.; Nordin, J.D.; DeFor, T.A.; Tompkins, M. ACL tears in school-aged children and adolescents over 20 years. Pediatrics 2017, 139, e20161877. [Google Scholar] [CrossRef] [PubMed]
- Werner, B.C.; Yang, S.; Looney, A.M.; Gwathmey, F.W. Trends in pediatric and adolescent anterior cruciate ligament injury and reconstruction. J. Pediatr. Orthop. 2016, 36, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Kocher, M.S.; Saxon, H.S.; Hovis, W.D.; Hawkins, R.J. Management and complications of anterior cruciate ligament injuries in skeletally immature patients: Survey of The Herodicus Society and The ACL Study Group. J. Pediatr. Orthop. 2002, 22, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Quatman, C.E.; Quatman-Yates, C.C.; Hewett, T.E. A ‘plane’ explanation of anterior cruciate ligament injury mechanisms: A systematic review. Sports Med. 2010, 40, 729–746. [Google Scholar] [CrossRef]
- Koga, H.; Nakamae, A.; Shima, Y.; Iwasa, J.; Myklebust, G.; Engebretsen, L.; Bahr, R.; Krosshaug, T. Mechanisms for noncontact anterior cruciate ligament injuries: Knee joint kinematics in 10 injury situations from female team handball and basketball. Am. J. Sports Med. 2010, 38, 2218–2225. [Google Scholar] [CrossRef]
- Faigenbaum, A.D.; Myer, G.D. Resistance training among young athletes: Safety, efficacy and injury prevention effects. Br. J. Sports Med. 2010, 44, 56–63. [Google Scholar] [CrossRef]
- Ford, K.R.; Myer, G.D.; Hewett, T.E. Valgus knee motion during landing in high school female and male basketball players. Med. Sci. Sports Exerc. 2003, 35, 1745–1750. [Google Scholar] [CrossRef]
- Russell, K.A.; Palmieri, R.M.; Zinder, S.M.; Ingersoll, C.D. Sex differences in valgus knee angle during a single-leg drop jump. J. Athl. Train. 2006, 41, 166–171. [Google Scholar]
- Donnell-Fink, L.A.; Klara, K.; Collins, J.E.; Yang, H.Y.; Goczalk, M.G.; Katz, J.N.; Losina, E. Effectiveness of knee injury and anterior cruciate ligament tear prevention programs: A meta-analysis. PLoS ONE 2015, 10, e0144063. [Google Scholar] [CrossRef]
- Lima, Y.L.; Ferreira, V.M.L.M.; de Paula Lima, P.O.; Bezerra, M.A.; de Oliveira, R.R.; Almeida, G.P.L. The association of ankle dorsiflexion and dynamic knee valgus: A systematic review and meta-analysis. Phys. Ther. Sport 2018, 29, 61–69. [Google Scholar] [CrossRef]
- Claiborne, T.L.; Armstrong, C.W.; Gandhi, V.; Pincivero, D.M. Relationship between hip and knee strength and knee valgus during a single leg squat. J. Appl. Biomech. 2006, 22, 41–50. [Google Scholar] [CrossRef]
- Suzuki, H.; Omori, G.; Uematsu, D.; Nishino, K.; Endo, N. The influence of hip strength on knee kinematics during a single-leggged medial drop landing among competitive collegiate basketball players. Int. J. Sports Phys. Ther. 2015, 10, 592–601. [Google Scholar] [PubMed]
- Bodendorfer, B.M.; Arnold, N.R.; Shu, H.T.; Leary, E.V.; Cook, J.L.; Gray, A.D.; Guess, T.M.; Sherman, S.L. Do neoprene sleeves and prophylactic knee braces affect neuromuscular control and cutting agility? Phys. Ther. Sport 2019, 39, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Cinque, M.E.; Bodendorfer, B.M.; Shu, H.T.; Arnold, N.R.; Gray, A.D.; Summerhays, B.J.; Guess, T.M.; Sherman, S.L. The effect of silicone ankle sleeves and lace-up ankle braces on neuromuscular control, joint torque, and cutting agility. J. Orthop. 2020, 20, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.B.; Waxman, J.P.; Richter, S.J.; Shultz, S.J. Evaluation of the effectiveness of anterior cruciate ligament injury prevention programme training components: A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 79–87. [Google Scholar] [CrossRef]
- Hewett, T.E.; Ford, K.R.; Myer, G.D. Anterior cruciate ligament injuries in female athletes: Part 2, a meta-analysis of neuromuscular interventions aimed at injury prevention. Am. J. Sports Med. 2006, 34, 490–498. [Google Scholar] [CrossRef]
- Myer, G.D.; Ford, K.R.; McLean, S.G.; Hewett, T.E. The effects of plyometric versus dynamic stabilization and balance training on lower extremity biomechanics. Am. J. Sports Med. 2006, 34, 445–455. [Google Scholar] [CrossRef]
- Nessler, T.; Denney, L.; Sampley, J. ACL injury prevention: What does research tell us? Curr. Rev. Musculoskelet. Med. 2017, 10, 281–288. [Google Scholar] [CrossRef]
- Herman, K.; Barton, C.; Malliaras, P.; Morrissey, D. The effectiveness of neuromuscular warm-up strategies, that require no additional equipment, for preventing lower limb injuries during sports participation: A systematic review. BMC Med. 2012, 10, 1–12. [Google Scholar] [CrossRef]
- Mehl, J.; Diermeier, T.; Herbst, E.; Imhoff, A.B.; Stoffels, T.; Zantop, T.; Petersen, W.; Achtnich, A. Evidence-based concepts for prevention of knee and ACL injuries. 2017 guidelines of the ligament committee of the German Knee Society (DKG). Arch. Orthop. Trauma Surg. 2018, 138, 51–61. [Google Scholar] [CrossRef]
- Voskanian, N. ACL Injury prevention in female athletes: Review of the literature and practical considerations in implementing an ACL prevention program. Curr. Rev. Musculoskelet. Med. 2013, 6, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Ueno, R.; Navacchia, A.; DiCesare, C.A.; Ford, K.R.; Myer, G.D.; Ishida, T.; Tohyama, H.; Hewett, T.E. Knee abduction moment is predicted by lower gluteus medius force and larger vertical and lateral ground reaction forces during drop vertical jump in female athletes. J. Biomech. 2020, 103, 109669. [Google Scholar] [CrossRef] [PubMed]
- Small, K.; McNaughton, L.; Greig, M.; Lovell, R. The effects of multidirectional soccer-specific fatigue on markers of hamstring injury risk. J. Sci. Med. Sport 2010, 13, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Behrens, M.; Mau-Moeller, A.; Wassermann, F.; Plewka, A.; Bader, R.; Bruhn, S. Repetitive jumping and sprinting until exhaustion alters hamstring reflex responses and tibial translation in males and females. J. Orthop. Res. 2015, 33, 1687–1692. [Google Scholar] [CrossRef]
- Borotikar, B.S.; Newcomer, R.; Koppes, R.; McLean, S.G. Combined effects of fatigue and decision making on female lower limb landing postures: Central and peripheral contributions to ACL injury risk. Clin. Biomech. 2008, 23, 81–92. [Google Scholar] [CrossRef]
- McLean, S.G.; Felin, R.E.; Suedekum, N.; Calabrese, G.; Passerallo, A.; Joy, S. Impact of fatigue on gender-based high-risk landing strategies. Med. Sci. Sports Exerc. 2007, 39, 502–514. [Google Scholar] [CrossRef]
- Barber-Westin, S.D.; Noyes, F.R. Effect of fatigue protocols on lower limb neuromuscular function and implications for anterior cruciate ligament injury prevention training: A systematic review. Am. J. Sports Med. 2017, 45, 3388–3396. [Google Scholar] [CrossRef]
- Briem, K.; Jónsdóttir, K.V.; Árnason, Á.; Sveinsson, Þ. Effects of sex and fatigue on biomechanical measures during the Drop-jump task in children. Orthop. J. Sports Med. 2017, 5. [Google Scholar] [CrossRef]
- Fort-Vanmeerhaeghe, A.; Benet, A.; Mirada, S.; Montalvo, A.M.; Myer, G.D. Sex and maturation differences in performance of functional jumping and landing deficits in youth athletes. J. Sport Rehabil. 2019, 28, 606–613. [Google Scholar] [CrossRef]
- Pappas, E.; Hagins, M.; Sheikhzadeh, A.; Nordin, M.; Rose, D. Biomechanical differences between unilateral and bilateral landings from a jump: Gender differences. Clin. J. Sport Med. 2007, 17, 263–268. [Google Scholar] [CrossRef]
- Ugalde, V.; Brockman, C.; Bailowitz, Z.; Pollard, C.D. Single leg squat test and its relationship to dynamic knee valgus and injury risk screening. PM R 2015, 7, 229–235. [Google Scholar] [CrossRef]
- Puig-Diví, A.; Escalona-Marfil, C.; Padullés-Riu, J.M.; Busquets, A.; Padullés-Chando, X.; Marcos-Ruiz, D. Validity and reliability of the Kinovea program in obtaining angles and distances using coordinates in 4 perspectives. PLoS ONE 2019, 14, e0216448. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Atkinson, G.; Nevill, A.M. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Med. 1998, 26, 217–238. [Google Scholar] [CrossRef] [PubMed]
- Horton, M.G.; Hall, T.L. Quadriceps femoris muscle angle: Normal values and relationships with gender and selected skeletal measures. Phys. Ther. 1989, 69, 897–901. [Google Scholar] [CrossRef] [PubMed]
- Agresta, C.; Church, C.; Henley, J.; Duer, T.; O’Brien, K. Single-leg squat performance in active adolescents aged 8-17 years. J. Strength Cond. Res. 2017, 31, 1187–1191. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Rhea, M.R. Determining the magnitude of treatment effects in strength training research through the use of the effect size. J. Strength Cond. Res. 2004, 18, 918–920. [Google Scholar] [CrossRef]
- Barendrecht, M.; Lezeman, H.C.A.; Duysens, J.; Smits-Engelsman, B.C.M. Neuromuscular training improves knee kinematics, in particular in valgus aligned adolescent team handball players of both sexes. J. Strength Cond. Res. 2011, 25, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Emamvirdi, M.; Letafatkar, A.; Khaleghi Tazji, M. The effect of valgus control instruction exercises on pain, strength, and functionality in active females with patellofemoral pain sndrome. Sports Health 2019, 11, 223–237. [Google Scholar] [CrossRef]
- Herrington, L. The effects of 4 weeks of jump training on landing knee valgus and crossover hop performance in female basketball players. J. Strength Cond. Res. 2010, 24, 3427–3432. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E.; Stroupe, A.L.; Nance, T.A.; Noyes, F.R. Plyometric training in female athletes: Decreased impact forces and increased hamstring torques. Am. J. Sports Med. 1996, 24, 765–773. [Google Scholar] [CrossRef] [PubMed]
- Lim, B.O.; Lee, Y.S.; Kim, J.G.; An, K.O.; Yoo, J.; Kwon, Y.H. Effects of sports injury prevention training on the biomechanical risk factors of anterior cruciate ligament injury in high school Female basketball players. Am. J. Sports Med. 2009, 37, 1728–1734. [Google Scholar] [CrossRef] [PubMed]
- Myer, G.D.; Ford, K.R.; Palumbo, J.P.; Hewett, T.E. Neuromuscular training improves performance and lower-extremity biomechanics in female athletes. J. Strength Cond. Res. 2005, 19, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Noyes, F.R.; Barber-Westin, S.D.; Tutalo Smith, S.T.; Campbell, T. A training program to improve neuromuscular and performance indices in female high school soccer players. J. Strength Cond. Res. 2013, 27, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Carcia, C.; Eggen, J.; Shultz, S. Hip-abductor fatigue, frontal-plane landing angle, and excursion during a drop jump. J. Sport Rehabil. 2005, 14, 321–331. [Google Scholar] [CrossRef]
- Chappell, J.D.; Herman, D.C.; Knight, B.S.; Kirkendall, D.T.; Garrett, W.E.; Yu, B. Effect of fatigue on knee kinetics and kinematics in stop-jump tasks. Am. J. Sports Med. 2005, 33, 1022–1029. [Google Scholar] [CrossRef]
- Cortes, N.; Quammen, D.; Lucci, S.; Greska, E.; Onate, J. A functional agility short-term fatigue protocol changes lower extremity mechanics. J. Sports Sci. 2012, 30, 797–805. [Google Scholar] [CrossRef]
- Dickin, D.C.; Johann, E.; Wang, H.; Popp, J.K. Combined effects of drop height and fatigue on landing mechanics in active females. J. Appl. Biomech. 2015, 31, 237–243. [Google Scholar] [CrossRef]
- Fidai, M.S.; Okoroha, K.R.; Meldau, J.; Meta, F.; Lizzio, V.A.; Borowsky, P.; Redler, L.H.; Moutzouros, V.; Makhni, E.C. Fatigue increases dynamic knee valgus in youth athletes: Results from a field-based drop-jump test. Arthrosc. J. Arthrosc. Relat. Surg. 2020, 36, 214–222. [Google Scholar] [CrossRef]
- Greig, M. The influence of soccer-specific activity on the kinematics of an agility sprint. Eur. J. Sport Sci. 2009, 9, 23–33. [Google Scholar] [CrossRef]
- Lucci, S.; Cortes, N.; Van Lunen, B.; Ringleb, S.; Onate, J. Knee and hip sagittal and transverse plane changes after two fatigue protocols. J. Sci. Med. Sport 2011, 14, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Cashman, G.E. The effect of weak hip abductors or external rotators on knee valgus kinematics in healthy subjects: A systematic review. J. Sport Rehabil. 2012, 21, 273–284. [Google Scholar] [CrossRef] [PubMed]
- Sanna, G.; O’Connor, K.M. Fatigue-related changes in stance leg mechanics during sidestep cutting maneuvers. Clin. Biomech. 2008, 23, 946–954. [Google Scholar] [CrossRef]
- Chavez, A.; Knudson, D.; Harter, R.; McCurdy, K. Activity-specific effects of fatigue protocols may influence landing kinematics: A pilot study. Int. J. Exerc. Sci. 2013, 6, 242–249. [Google Scholar]
- Daneshjoo, A.; Mohseni, M. Comparing the knee joint kinematic parameters during landing at different minutes of soccer game. J. Sport Biomech. 2019, 5, 2–13. [Google Scholar] [CrossRef]
- Ludwig, O.; Simon, S.; Piret, J.; Becker, S.; Marschall, F. Differences in the dominant and non-dominant dnee valgus angle in junior elite and amateur soccer players after unilateral landing. Sports 2017, 5, 14. [Google Scholar] [CrossRef]
- Read, P.J.; Oliver, J.L.; De Ste Croix, M.B.A.; Myer, G.D.; Lloyd, R.S. Landing kinematics in elite male youth soccer players of different chronologic ages and stages of maturation. J. Athl. Train. 2018, 53, 372–378. [Google Scholar] [CrossRef]
- Barber-Westin, S.D.; Noyes, F.R.; Galloway, M. Jump-land characteristics and muscle strength development in young athletes: A gender comparison of 1140 athletes 9 to 17 years of age. Am. J. Sports Med. 2006, 34, 375–384. [Google Scholar] [CrossRef]
- Rogol, A.D.; Roemmich, J.N.; Clark, P.A. Growth at puberty. J. Adolesc. Health 2002, 31, 192–200. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Test | n | pre (°) (Mean ± SD) | post (°) (Mean ± SD) | 95% CI | p-Value | |
|---|---|---|---|---|---|---|
| LL | UL | |||||
| ACL-IPP DL | 10 | 32.67 ± 9.39 | 12.23 ± 13.91 | 11.04 | 29.82 | 0.007 ** |
| ACL-IPP NDL | 10 | 28.93 ± 7.04 | 13.50 ± 10.53 | 8.36 | 22.50 | 0.005 ** |
| SSFP DL | 8 | 3.11 ± 1.93 | 14.20 ± 6.52 | 6.15 | 16.03 | 0.012 * |
| SSFP NDL | 8 | 8.37 ± 3.71 | 12.50 ± 6.00 | 1.18 | 9.43 | 0.123 |
| Variables | Age | Weight | Height | BMI | pre-ACL-IPP DL | pre-ACL-IPP NDL | post-ACL-IPP DL | post-ACL-IPP NDL | |
|---|---|---|---|---|---|---|---|---|---|
| Age | r | 1 | 0.617 | 0.845 ** | 0.286 | −0.778 ** | 0.029 | −0.267 | 0.465 |
| p | – | 0.058 | 0.002 | 0.423 | 0.008 | 0.937 | 0.456 | 0.175 | |
| Weight | r | 1 | 0.462 | 0.903 ** | −0.419 | 0.043 | −0.139 | 0.225 | |
| p | – | 0.179 | 0.000 | 0.228 | 0.907 | 0.701 | 0.532 | ||
| Height | r | 1 | 0.195 | −0.546 | 0.116 | −0.140 | 0.332 | ||
| p | – | 0.590 | 0.103 | 0.750 | 0.700 | 0.348 | |||
| BMI | r | 1 | −0.158 | −0.103 | −0.224 | −0.158 | |||
| p | – | 0.663 | 0.776 | 0.533 | 0.663 | ||||
| pre-ACL-IPP DL | r | 1 | 0.049 | 0.395 | −0.457 | ||||
| p | – | 0.894 | 0.258 | 0.184 | |||||
| pre-ACL-IPP NDL | r | 1 | 0.796 ** | 0.470 | |||||
| p | – | 0.006 | 0.171 | ||||||
| post-ACL-IPP DL | r | 1 | 0.383 | ||||||
| p | – | 0.275 | |||||||
| post-ACL-IPP NDL | r | 1 | |||||||
| p | – | ||||||||
| Variables | Age | Weight | Height | BMI | pre-SSFP DL | pre-SSFP NDL | post-SSFP DL | post-SSFP NDL | |
|---|---|---|---|---|---|---|---|---|---|
| Age | r | 1 | 0.789 * | 0.667 | 0.717 * | 0.652 | −0.049 | 0.927 ** | −0.210 |
| p | – | 0.2 | 0.071 | 0.046 | 0.079 | 0.907 | 0.001 | 0.618 | |
| Weight | r | 1 | 0.910 ** | 0.898 ** | 0.476 | 0.252 | 0.922 ** | 0.252 | |
| p | – | 0.002 | 0.002 | 0.233 | 0.548 | 0.001 | 0.548 | ||
| Height | r | 1 | 0.667 | 0.359 | 0.452 | 0.810 * | 0.333 | ||
| p | – | 0.071 | 0.382 | 0.26 | 0.015 | 0.42 | |||
| BMI | r | 1 | 0.407 | 0.095 | 0.833 * | 0.167 | |||
| p | – | 0.317 | 0.823 | 0.01 | 0.693 | ||||
| pre-SSFP DL | r | 1 | 0.275 | 0.587 | −0.156 | ||||
| p | – | 0.509 | 0.126 | 0.713 | |||||
| pre-SSFP NDL | r | 1 | 0.095 | 0.667 | |||||
| p | – | 0.823 | 0.071 | ||||||
| post-SSFP DL | r | 1 | 0.048 | ||||||
| p | – | 0.911 | |||||||
| post-SSFP NDL | r | 1 | |||||||
| p | – | ||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Luna, M.A.; Cortell-Tormo, J.M.; García-Jaén, M.; Ortega-Navarro, M.; Tortosa-Martínez, J. Acute Effects of ACL Injury-Prevention Warm-Up and Soccer-Specific Fatigue Protocol on Dynamic Knee Valgus in Youth Male Soccer Players. Int. J. Environ. Res. Public Health 2020, 17, 5608. https://doi.org/10.3390/ijerph17155608
García-Luna MA, Cortell-Tormo JM, García-Jaén M, Ortega-Navarro M, Tortosa-Martínez J. Acute Effects of ACL Injury-Prevention Warm-Up and Soccer-Specific Fatigue Protocol on Dynamic Knee Valgus in Youth Male Soccer Players. International Journal of Environmental Research and Public Health. 2020; 17(15):5608. https://doi.org/10.3390/ijerph17155608
Chicago/Turabian StyleGarcía-Luna, Marco Andrés, Juan Manuel Cortell-Tormo, Miguel García-Jaén, Manuel Ortega-Navarro, and Juan Tortosa-Martínez. 2020. "Acute Effects of ACL Injury-Prevention Warm-Up and Soccer-Specific Fatigue Protocol on Dynamic Knee Valgus in Youth Male Soccer Players" International Journal of Environmental Research and Public Health 17, no. 15: 5608. https://doi.org/10.3390/ijerph17155608
APA StyleGarcía-Luna, M. A., Cortell-Tormo, J. M., García-Jaén, M., Ortega-Navarro, M., & Tortosa-Martínez, J. (2020). Acute Effects of ACL Injury-Prevention Warm-Up and Soccer-Specific Fatigue Protocol on Dynamic Knee Valgus in Youth Male Soccer Players. International Journal of Environmental Research and Public Health, 17(15), 5608. https://doi.org/10.3390/ijerph17155608