Social Participation in Relation to Technology Use and Social Deprivation: A Mixed Methods Study Among Older People with and without Dementia

 ,
,
Abstract
1. Introduction
Social Participation. Everyday Technology Use and Social Deprivation of the Living Environment: A Review of Key Issues
- In what ways does social participation, as reported by older participants living with and without dementia, relate to total ET use outside home and social deprivation of the living environment?
- What are the motivators, considerations that require extra attention and, strategies for managing social participation of older people with and without dementia, in relation to the role of ET use outside home?
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Participants
2.3. Data Collection Procedure
- (1)
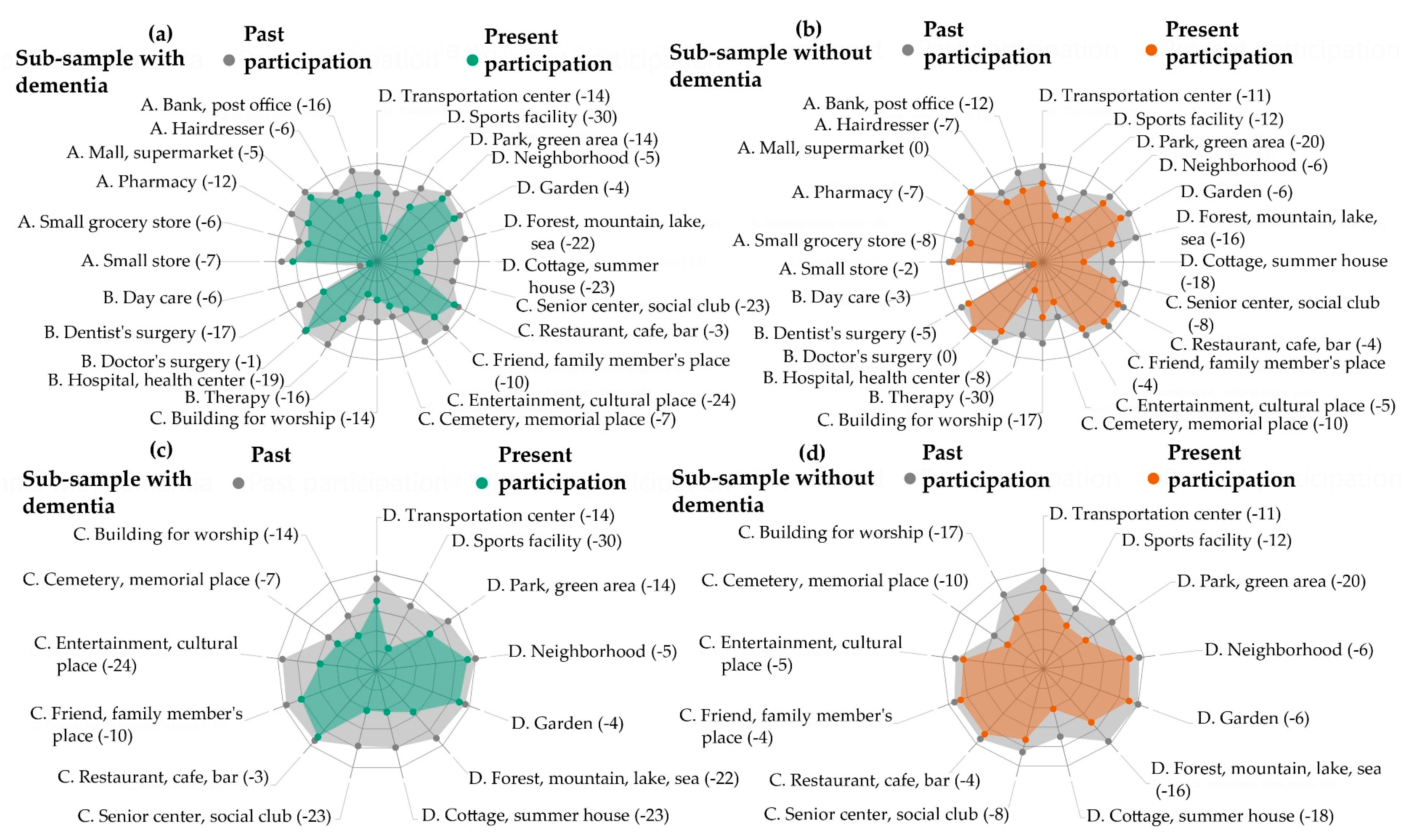
- Part one of the ACT-OUT maps self-reported present participation in four domains: (A) places for purchasing, administration, and self-care, e.g., supermarket; (B) places for medical care, e.g., doctor’s surgery; (C) places for social, spiritual, and cultural activities, e.g., friend’s home; (D) places for recreation and physical activity, e.g., neighborhood. This study used the ACT-OUT to focus on domains C and D. A dichotomous yes or no answer was recorded for whether a person participated in the place or not. In part two of the ACT-OUT, the participant was asked to report in more detail about the activity they perform in one place, for each domain. This was based on a place where there had been no change in their participation. To capture detailed information about the activity performed in a place and the journey to and from the place, open-ended questions were used. Responses were written down verbatim by the interviewer and consisted of a couple of sentences. Examples of the questions include: “Picture yourself in a senior center or social club: what do you have to be careful about or pay extra attention to?” and “Imagine getting there: what do you have to be careful or pay extra attention to?”. Information about the development of the ACT-OUT and the functioning of its rating scale is described in earlier research [34].
- (2)
- The MoCA [35] was performed with all participants in order to assess current levels of cognitive function to describe the sample.
- (3)
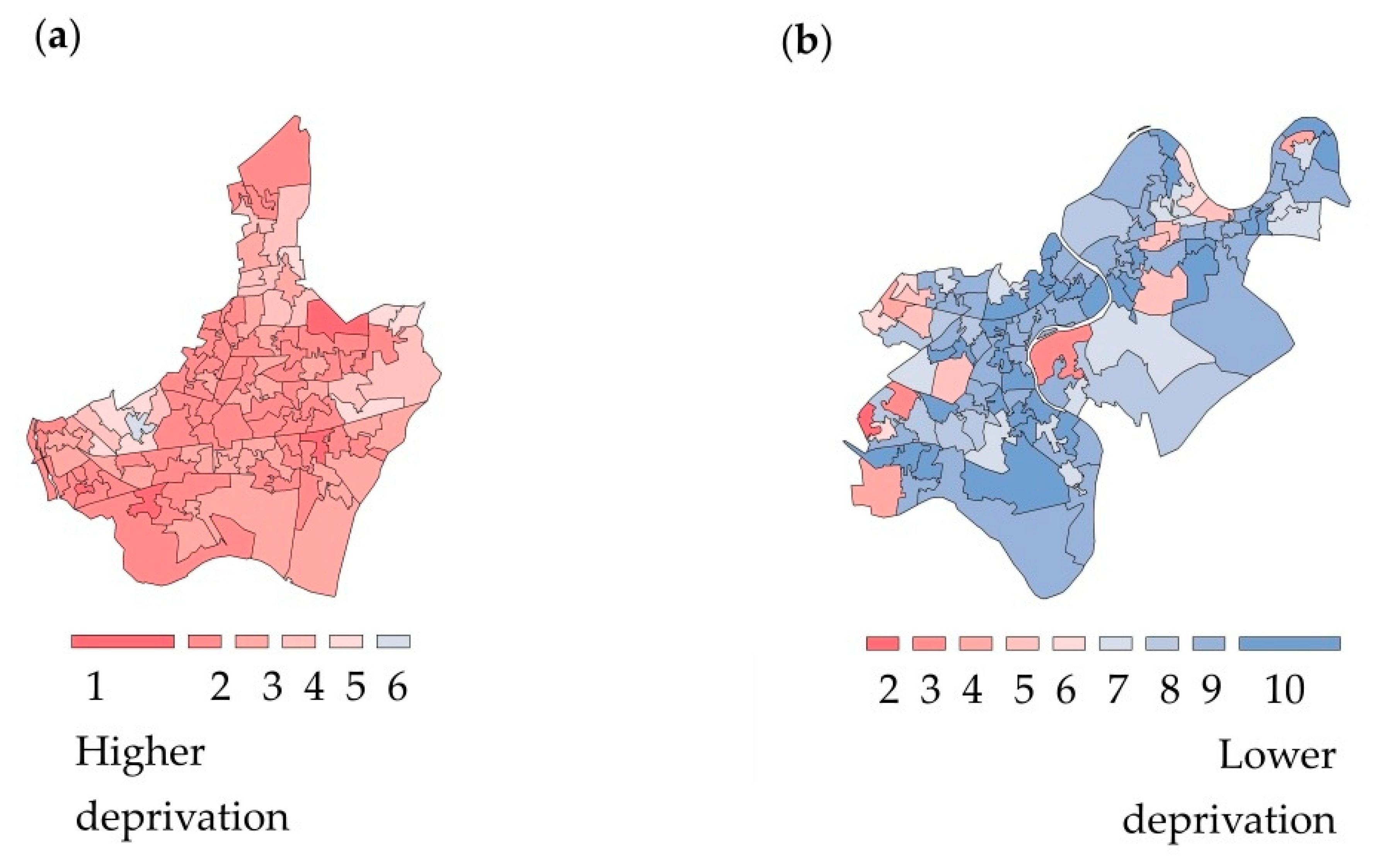
- A non-standardized demographic questionnaire was used to gather information about participants, with respect to a range of demographic factors that may be relevant according to earlier research [36]. This included asking whether participants were living with a functional impairment (e.g., reduced fine motor skills or medical diagnoses such as diabetes). An Index of Multiple Deprivation (IMD) score was determined according to information about where the participants lived, which was checked according to LSOA listings on the Ministry of Housing, Community and Local Government website [37]. The IMD is a spatially disaggregated measure of relative deprivation applied to small geographic areas or neighborhoods in England, which are referred to as Lower-Super Output Areas (LSOAs) [37]. The IMD score comprises a weighted sum of seven sub-domains of deprivation: (1) income; (2) employment; (3) education, skills, and training; (4) health and disability; (5) crime; (6) access to housing and services; and (7) living environment. The IMD was used to contextualize the living environment of participants into ten equal groups (deciles), with one corresponding to the most deprived 10% of neighborhoods in England and ten representing the least deprived 10% of neighborhoods in England [37].
- (4)
- The ETUQ was used to gather information about the total ET use outside home variable according to 49 ETs, including 16 ET which can be used outside home (e.g., ATM, self-service checkout) in addition to 33 portable ET that can be used both at home and outside home (e.g., smartphone, pedometer, eBook reader) [20]. The focus of this study is on the total ET use outside home; however, other studies provide descriptions about the use of each of the different types of ET [19]. In-depth information about the rating scale and validation of the ETUQ among different populations, including older people living with dementia, is available in earlier research [38,39].
2.4. Data Analysis
3. Results
3.1. Statistical Results
3.1.1. Participants
3.1.2. Social Participation in Relation to Total ET Use outside Home
3.1.3. Social Participation in Relation to Social Deprivation of the Living Environment
3.2. Content Analysis Results
3.2.1. Purposeful Activity as a Motivator for Social Participation
3.2.2. Doing the Journey and/or Activity with Other People as a Motivator for Social Participation
3.2.3. Contextual Factors that Require Extra Attention for Managing Social Participation
3.2.4. Preparation and Wayfinding Involving ET Use for Managing Social Participation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Social Determinants of Health. Available online: http://www.who.int/social_determinants/thecommission/countrywork/within/socialparticipation/en/index.html (accessed on 16 April 2020).
- Nilsson, I.; Löfgren, B.; Fisher, A.G.; Bernspång, B. Focus on Leisure Repertoire in the Oldest Old: The Umeå 85+ Study. J. Appl. Gerontol. 2006, 25, 391–405. [Google Scholar] [CrossRef]
- Evans, I.E.; Martyr, A.; Collins, R.; Brayne, C.; Clare, L. Social Isolation and Cognitive Function in Later Life: A Systematic Review and Meta-Analysis. J. Alzheimer’s Dis. 2019, 70, S119–S144. [Google Scholar] [CrossRef]
- Bai, Z.; Wang, Z.; Shao, T.; Qin, X.; Hu, Z. Relationship between Individual Social Capital and Functional Ability among Older People in Anhui Province, China. Int. J. Environ. Res. Public Health 2020, 17, 2775. [Google Scholar] [CrossRef]
- Fallahpour, M.; Borell, L.; Luborsky, M.; Nygård, L. Leisure-activity participation to prevent later-life cognitive decline: a systematic review. Scand. J. Occup. Ther. 2015, 23, 1–36. [Google Scholar] [CrossRef] [PubMed]
- Yamada, M.; Hapsari, E.D.; Matsuo, H. Behaviors toward Noncommunicable Diseases Prevention and Their Relationship with Physical Health Status among Community-dwelling, Middle-aged and Older Women in Indonesia. Int. J. Environ. Res. Public Health 2020, 17, 2332. [Google Scholar] [CrossRef] [PubMed]
- Turcotte, P.-L.; Carrier, A.; Roy, V.; Levasseur, M. Occupational therapists’ contributions to fostering older adults’ social participation: A scoping review. Br. J. Occup. Ther. 2018, 81, 427–449. [Google Scholar] [CrossRef]
- Nygård, L. The meaning of everyday technology as experienced by people with dementia who live alone. Dementia 2008, 7, 481–502. [Google Scholar] [CrossRef]
- Neves, B.B.; Franz, R.; Judges, R.; Beermann, C.; Baecker, R. Can Digital Technology Enhance Social Connectedness Among Older Adults? A Feasibility Study. J. Appl. Gerontol. 2017, 38, 49–72. [Google Scholar] [CrossRef]
- Bruggencate, T.T.; Luijkx, K.G.; Sturm, J. Friends or Frenemies? The Role of Social Technology in the Lives of Older People. Int. J. Environ. Res. Public Health 2019, 16, 4969. [Google Scholar] [CrossRef]
- Pinto-Bruno, Á.C.; García-Casal, A.; Csipke, E.; Jenaro, C.; Franco-Martín, M.A. ICT-based applications to improve social health and social participation in older adults with dementia. A systematic literature review. Aging Ment. Health 2016, 21, 58–65. [Google Scholar] [CrossRef]
- Thordardottir, B.; Fänge, A.M.; Lethin, C.; Gatta, D.R.; Chiatti, C. Acceptance and Use of Innovative Assistive Technologies among People with Cognitive Impairment and Their Caregivers: A Systematic Review. BioMed. Res. Int. 2019, 2019, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Fischl, C.; Lindelöf, N.; Lindgren, H.; Nilsson, I. Older adults’ perceptions of contexts surrounding their social participation in a digitalized society—an exploration in rural communities in Northern Sweden. Eur. J. Ageing 2020, 1–10. [Google Scholar] [CrossRef]
- Barakovic, S.; Husic, J.B.; Van Hoof, J.; Krejcar, O.; Maresova, P.; Akhtar, Z.; Melero, F.J. Quality of Life Framework for Personalised Ageing: A Systematic Review of ICT Solutions. Int. J. Environ. Res. Public Health 2020, 17, 2940. [Google Scholar] [CrossRef] [PubMed]
- Mannheim, I.; Schwartz, E.; Xi, W.; Buttigieg, S.C.; McDonnell-Naughton, M.; Wouters, E.; Van Zaalen, Y. Inclusion of Older Adults in the Research and Design of Digital Technology. Int. J. Environ. Res. Public Health 2019, 16, 3718. [Google Scholar] [CrossRef] [PubMed]
- Levasseur, M.; Richard, L.; Gauvin, L.; Raymond, É. Inventory and analysis of definitions of social participation found in the aging literature: Proposed taxonomy of social activities. Soc. Sci. Med. 2010, 71, 2141–2149. [Google Scholar] [CrossRef]
- Piškur, B.; Daniëls, R.; Jongmans, M.J.; Ketelaar, M.; Smeets, R.J.; Norton, M.; Beurskens, A.J.H.M. Participation and social participation: Are they distinct concepts? Clin. Rehabil. 2014, 28, 211–220. [Google Scholar] [CrossRef]
- Donkers, H.W.; Vernooij-Dassen, M.; Van Der Veen, D.; Van Der Sanden, M.N.; Graff, M. Social participation perspectives of people with cognitive problems and their care-givers: A descriptive qualitative study. Ageing Soc. 2018, 39, 1–27. [Google Scholar] [CrossRef]
- Gaber, S.N.; Nygård, L.; Kottorp, A.; Charlesworth, G.; Wallcook, S.; Malinowsky, C. Perceived risks, concession travel pass access and everyday technology use for out-of-home participation: Cross-sectional interviews among older people in the UK. BMC Geriatr. 2019, in press. [Google Scholar]
- Gaber, S.; Nygård, L.; Brorsson, A.; Kottorp, A.; Malinowsky, C. Everyday technologies and public space participation among people with and without dementia. Can. J. Occup. Ther. 2019, 86, 400–411. [Google Scholar] [CrossRef] [PubMed]
- Margot-Cattin, I.; Kuhne, N.; Kottorp, A.; Cutchin, M.; Öhman, A.; Nygård, L. Participation in activities and places outside home among people with and without dementia: Reflections on an unevenly shrinking world. Can. J. Occup. 2020. under review. [Google Scholar]
- Nygård, L.; Rosenberg, L.; Kottorp, A. User’s Manual: Everyday Technology Use Questionnaire (ETUQ) Everyday Technology in Activities at Home and in Society; Technical Report; Karolinska Institutet: Stockholm, Sweden, 2016; pp. 1–31. [Google Scholar]
- Lindqvist, E.; Persson Vasiliou, A.; Gomersall, T.; Astelle, A.; Mihailidis, A.; Sixsmith, A.; Nygård, L. Activities people with cognitive deficits want to continue mastering–A scoping study. Brit. J. Occup. Ther. 2016, 79, 399–408. [Google Scholar] [CrossRef]
- Brorsson, A.; Nygard, L.; Ohman, A. Access to Everyday Activities in Public Space-Views of People with Dementia. Innov. Aging 2019, 3, S774–S775. [Google Scholar] [CrossRef]
- Innes, A.; Page, S.J.; Cutler, C. Barriers to leisure participation for people with dementia and their carers: An exploratory analysis of carer and people with dementia’s experiences. Dementia 2016, 15, 1643–1665. [Google Scholar] [CrossRef] [PubMed]
- Longley, P.; Singleton, A. Linking Social Deprivation and Digital Exclusion in England. Urban Stud. 2009, 46, 1275–1298. [Google Scholar] [CrossRef]
- Demakakos, P.; Nunn, S.; Nazroo, J. Loneliness, relative deprivation and life satisfaction. In Retirement, Health and Relationships of the Older Population in England: The 2004 English Longitudinal Study of Ageing; Banks, J., Breeze, E., Lessof, C., Nazroo, J., Eds.; Institute for Fiscal Studies: London, UK, 2006; pp. 297–318. [Google Scholar]
- Creswell, J.W.; Creswell, J.D. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches, 5th ed.; SAGE: Los Angeles, CA, USA, 2018. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR); American Psychiatric Association Publishing: Washington, WA, USA, 2000. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Available online: https://www.psychiatry.org/psychiatrists/practice/dsm (accessed on 3 June 2020).
- National Institute for Health Research. Going the Extra Mile: Improving the Nation’s Health and Wellbeing through Public Involvement in Research. Available online: https://www.nihr.ac.uk/documents/about-us/our-contribution-to-research/how-we-involve-patients-carers-and-the-public/Going-the-Extra-Mile.pdf (accessed on 1 March 2020).
- World Health Organization. Age-Friendly Environments in Europe. A Handbook of Domains for Policy Action. Available online: http://www.euro.who.int/__dataassets/pdf_file/0011/359543/AFEE-handbook.PDF?ua=1 (accessed on 27 May 2020).
- Harmer, B.J.; Orrell, M. What is meaningful activity for people with dementia living in care homes? A comparison of the views of older people with dementia, staff and family carers. Aging Ment. Health 2008, 12, 548–558. [Google Scholar] [CrossRef]
- Margot-Cattin, I.; Kuhne, N.; Kottorp, A.; Cutchin, M.; Öhman, A.; Nygård, L. Development of a Questionnaire to Evaluate Out-of-Home Participation for People With Dementia. Am. J. Occup. Ther. 2019, 73, 7301205030p1–7301205030p10. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H.; Bédirian, V. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Kottorp, A.; Nygård, L.; Hedman, A.; Öhman, A.; Malinowsky, C.; Rosenberg, L.; Lindqvist, E.; Ryd, C. Access to and use of everyday technology among older people: An occupational justice issue—but for whom? J. Occup. Sci. 2016, 23, 382–388. [Google Scholar] [CrossRef]
- Ministry of Housing, Community & Local Government. National Statistics. English Indices of Deprivation 2015. Available online: https://www.gov.uk/government/statistics/english-indices-of-deprivation-2015 (accessed on 1 March 2020).
- Malinowsky, C.; Kottorp, A.; Wallin, A.; Nordlund, A.; Björklund, E.; Melin, I.; Pernevik, A.; Rosenberg, L.; Nygård, L. Differences in the use of everyday technology among persons with MCI, SCI and older adults without known cognitive impairment. Int. Psychogeriatr. 2017, 29, 1193–1200. [Google Scholar] [CrossRef]
- Nygård, L.; Pantzar, M.; Uppgard, B.; Kottorp, A. Detection of activity limitations in older adults with MCI or Alzheimer’s disease through evaluation of perceived difficulty in use of everyday technology: A replication study. Aging Ment. Health 2012, 16, 361–371. [Google Scholar] [CrossRef]
- Guetterman, T.C.; Fetters, M.D.; Creswell, J.W. Integrating Quantitative and Qualitative Results in Health Science Mixed Methods Research Through Joint Displays. Ann. Fam. Med. 2015, 13, 554–561. [Google Scholar] [CrossRef]
- Healy, M.J.R.; Hoaglin, D.C.; Mosteller, F.; Tukey, J.W. Understanding Robust and Exploratory Data Analysis. Biometrics 1983, 39, 1126. [Google Scholar] [CrossRef]
- R Core Team. The R Project for Statistical Computing. Available online: http://www.r-project.org/ (accessed on 13 February 2012).
- Microsoft. Power BI, Version 2.76.5678.782. Available online: https://powerbi.microsoft.com/sv-se/ (accessed on 8 February 2020).
- Trafford Data Lab. Available online: https://www.trafforddatalab.io/deprivation.html (accessed on 12 February 2020).
- Brewer, C.; Harrower, M. COLORBREWER 2.0: Color Advice for Cartography; The Pennsylvania State University: State College, PA, USA, 2020; Available online: https://colorbrewer2.org/ (accessed on 7 May 2020).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- ATLAS.ti Scientific Software Development GmbH. ATLAS.ti, Version 8; GmbH: Berlin, Germany, 2017. [Google Scholar]
- Shelley, M.; Krippendorff, K. Content Analysis: An Introduction to its Methodology. J. Am. Stat. Assoc. 1984, 79, 240. [Google Scholar] [CrossRef]
- Office of National Statistics. Urban and Rural Area Definitions for Policy Purposes in England and Wales: Methodology (v1.0). Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/239477/RUC11methodologypaperaug_28_Aug.pdf (accessed on 1 March 2020).
- Office of National Statistics. 2011 Census Analysis: Ethnicity and Religion of the Non-UK Born Population in England and Wales: 2011. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/culturalidentity/ethnicity/articles/2011censusanalysisethnicityandreligionofthenonukbornpopulationinenglandandwales/2015-06-18 (accessed on 1 March 2020).
- Oxford Poverty & Human Development Initiative. Walls of Glass: Measuring Deprivation in Social Participation. Available online: https://www.ophi.org.uk/wp-content/uploads/OPHIWP117.pdf (accessed on 24 April 2020).
- Wiles, J.; Leibing, A.; Guberman, N.; Reeve, J.; Allen, R.E.S. The Meaning of “Aging in Place” to Older People. Gerontologist 2011, 52, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Forgays, D.K.; Hyman, I.; Schreiber, J. Texting everywhere for everything: Gender and age differences in cell phone etiquette and use. Comput. Hum. Behav. 2014, 31, 314–321. [Google Scholar] [CrossRef]
- Leone, T.; Hessel, P. The effect of social participation on the subjective and objective health status of the over-fifties: Evidence from SHARE. Ageing Soc. 2015, 36, 968–987. [Google Scholar] [CrossRef]
- Patomella, A.-H.; Lovarini, M.; Lindqvist, E.; Kottorp, A.; Nygård, L. Technology use to improve everyday occupations in older persons with mild dementia or mild cognitive impairment: A scoping review. Br. J. Occup. Ther. 2018, 81, 555–565. [Google Scholar] [CrossRef]
- Førsund, L.H.; Grov, E.K.; Helvik, A.-S.; Juvet, L.K.; Skovdahl, K.; Eriksen, S. The experience of lived space in persons with dementia: A systematic meta-synthesis. BMC Geriatr. 2018, 18, 33. [Google Scholar] [CrossRef]
- Peek, S.T.M.; Luijkx, K.G.; Rijnaard, M.D.; Nieboer, M.E.; Van Der Voort, C.S.; Aarts, S.; Van Hoof, J.; Vrijhoef, H.J.; Wouters, E. Older Adults’ Reasons for Using Technology while Aging in Place. Gerontologist 2015, 62, 226–237. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Sub-Sample with Dementia (n = 64) | Sub-Sample without Dementia (n = 64) |
|---|---|---|
| Age, Years ** | ||
| Median (Min, Max) IQR 1 | 79.0 (62.0, 96.0) 74.0–83.0 | 71.0 (55.0, 89.0) 64.0–80.8 |
| Gender, n (%) | ||
| Female | 29 (45.3) | 34 (53.1) |
| Male | 35 (54.7) | 30 (46.9) |
| Living Arrangement, n (%) | ||
| Cohabiting | 39 (60.9) | 40 (62.5) |
| Lives Alone | 25 (39.1) | 24 (37.5) |
| Geography, n (%) | ||
| Urban | 51 (79.7) | 47 (73.4) |
| Rural | 13 (20.3) | 17 (26.6) |
| Education, Years ** | ||
| Median (Min, Max) IQR | 11.0 (7.0, 21.0) 10.3–13.0 | 13.0 (9.0, 19.0) 11.0–16.0 |
| Ethnicity, n (%) | ||
| White | 56 (87.5) | 49 (76.5) |
| Mixed/Multiple Ethnic Group | 0 (0.0) | 2 (3.1) |
| Asian/Asian British | 1 (1.6) | 9 (14.1) |
| Black/African/Caribbean/ Black British | 5 (7.8) | 3 (4.7) |
| Other Ethnic Group | 2 (3.1) | 1 (1.6) |
| Driving, n (%) ** | ||
| Driving | 26 (40.6) | 46 (71.9) |
| Not Driving | 38 (59.4) | 18 (28.1) |
| Functional Impairment, n (%) | ||
| Functional Impairment | 54 (84.4) | 56 (87.5) |
| No Functional Impairment | 10 (15.6) | 8 (12.5) |
| MoCA Score ** | ||
| Median (Min, Max) IQR | 21.0 (12.0, 28.0) 18.0–23.0 | 26.0 (21.0, 30.0) 25.0–28.5 |
| Index of Multiple Deprivation (IMD) | ||
| Median (Min, Max) IQR | 5.0 (1.0, 10.0) 3.5–8.0 | 5.5 (1.0, 10.0) 4.0–7.0 |
| Domain | Variables | Participants with Dementia (n = 64) | Participants without Dementia (n = 64) | |
|---|---|---|---|---|
| Domain C (Social, Spiritual and Cultural Places) | Total social participation (places = 6) | Median: 3.0; Min–Max: 1.0–6.0; IQR: 3.0–5.0 | Median: 5.0; Min–Max: 1.0–6.0; IQR: 3.0–5.0 | |
| Places in Domain C and examples of activities performed in the places | Places: 1. Friend or family member’s place 2. Restaurant, café, bar 3. Senior center, social club 4. Building for worship 5. Cemetery, memorial place 6. Entertainment, cultural place | Activities: 1. Drive to daughter’s place, a trip 2. Going into the village, sit down, cup of tea, chat 3. Dementia care group and socialize, art group, crossword, singalong 4. Socialize, worship, church duties 5. N/A 6. Go and watch live music | Activities: 1. Socialize and see grandchildren 2. Breakfast different place each week 3. Gujarati center. 150 people go. Meet people there, see friends, prayer, pass time, enjoys herself 4. Worship, play guitar, pray, enjoy time with dear friends 5. Walk and look around cemetery 6. See a concert with a friend | |
| Association between Social participation and: i. Total Everyday Technology use outside home; ii. IMD | i. No significant association (Rs = 0.176; p = 0.164) ii. No significant association (Rs = 0.035, p = 0.785) | i. No significant association (Rs = 0.181; p = 0.152) ii. No significant association (Rs = 0.157, p = 0.214) | ||
| Domain D (Places for Recreation and Physical Activities) | Total social participation (places = 7) | Median: 5.0; Min–Max: 0.0–7.0; IQR: 3.0–6.0 | Median: 5.0; Min–Max: 1.0–7.0; IQR: 4.0–6.0 | |
| Places in Domain D and examples of activities performed in the places | Places: 1. Garden 2. Park, green area 3. Forest, mountain, lake, sea 4. Cottage, summer house 5. Neighborhood 6. Sports facility 7. Transportation center | Activities: 1. Garden, admire the garden and the birds 2. Goes with granddaughter so she can play on the swings 3. Walk the dog along the seafront for a friend 4. Visit son and grandchildren and have a break 5. Neighborhood, sometimes walk and get fresh air 6. Seated exercises 7. Traveling | Activities: 1. Sit there with wife and cat 2. Go to park, people watch, go to café, sit on bench, walk 3. Walk and enjoy the scenery and navigate 4. Has 3 days at the timeshare cottage 5. Walking around, thinking alone. Enjoy exercise, time to think, fresh air 6. Swimming, 70 lengths 7. Get underground or buses | |
| Association between Social participation and: i. Total Everyday Technology use outside home; ii. IMD | i. Small significant association (Rs = 0.247; p = 0.049) ii. Small significant association (Rs = 0.267, p = 0.033) | i. Small-medium significant association (Rs = 0.343; p =0.006) ii. No significant association (Rs = 0.014, p = 0.911) | ||
| Domain C and D | Motivators for social participation | Purposeful activity; doing the journey and/or activity with other people | ||
| Considerations that require extra attention for social participation | Contextual factors | |||
| Strategies for managing social participation | Preparation and wayfinding | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaber, S.N.; Nygård, L.; Brorsson, A.; Kottorp, A.; Charlesworth, G.; Wallcook, S.; Malinowsky, C. Social Participation in Relation to Technology Use and Social Deprivation: A Mixed Methods Study Among Older People with and without Dementia. Int. J. Environ. Res. Public Health 2020, 17, 4022. https://doi.org/10.3390/ijerph17114022
Gaber SN, Nygård L, Brorsson A, Kottorp A, Charlesworth G, Wallcook S, Malinowsky C. Social Participation in Relation to Technology Use and Social Deprivation: A Mixed Methods Study Among Older People with and without Dementia. International Journal of Environmental Research and Public Health. 2020; 17(11):4022. https://doi.org/10.3390/ijerph17114022
Chicago/Turabian StyleGaber, Sophie N., Louise Nygård, Anna Brorsson, Anders Kottorp, Georgina Charlesworth, Sarah Wallcook, and Camilla Malinowsky. 2020. "Social Participation in Relation to Technology Use and Social Deprivation: A Mixed Methods Study Among Older People with and without Dementia" International Journal of Environmental Research and Public Health 17, no. 11: 4022. https://doi.org/10.3390/ijerph17114022
APA StyleGaber, S. N., Nygård, L., Brorsson, A., Kottorp, A., Charlesworth, G., Wallcook, S., & Malinowsky, C. (2020). Social Participation in Relation to Technology Use and Social Deprivation: A Mixed Methods Study Among Older People with and without Dementia. International Journal of Environmental Research and Public Health, 17(11), 4022. https://doi.org/10.3390/ijerph17114022