Coping Styles in Pregnancy, Their Demographic and Psychological Influences, and Their Association with Postpartum Depression: A Longitudinal Study of Women in China


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting
2.3. Participants and Recruitment
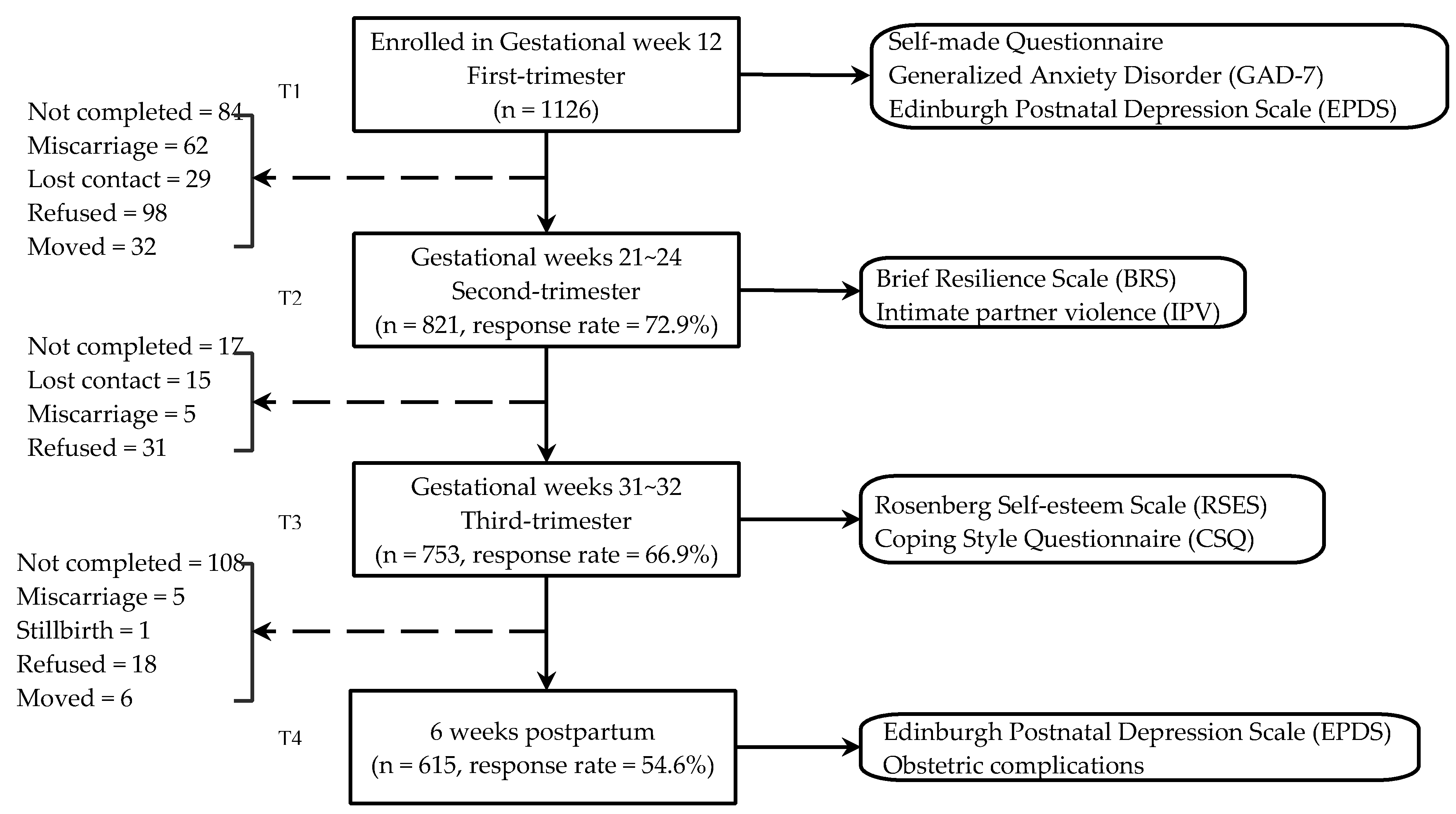
2.4. Data Collection
2.5. Measures
2.5.1. Coping Styles
2.5.2. Demographic Information
2.5.3. Intimate Partner Violence
2.5.4. Anxiety
2.5.5. Resilience
2.5.6. Self-Esteem
2.5.7. Obstetric Complications
2.5.8. Antenatal and Postpartum Depression
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Coping Styles
3.3. Simple and Multiple Linear Regression Including Factors Related to Coping Styles
3.4. Correlation between Coping Style and Postpartum Depression
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Folkman, S.; Lazarus, R.S.; Dunkelschetter, C.; Delongis, A.; Gruen, R.J. Dynamics of a stressful encounter: Cognitive appraisal, coping, and encounter outcomes. J. Personal. Soc. Psychol. 1986, 50, 992. [Google Scholar] [CrossRef]
- Susan, B.; Jayne, C. Responding to fear of childbirth. Lancet 2002, 359, 2128–2129. [Google Scholar]
- Geller, P.A. Pregnancy as a Stressful Life Event. CNS Spectrums 2004, 9, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Van den Bergh, B.R.H.; van den Heuvel, M.I.; Lahti, M.; Braeken, M.; de Rooij, S.R.; Entringer, S.; Hoyer, D.; Roseboom, T.; Räikkönen, K.; King, S.; et al. Prenatal developmental origins of behavior and mental health: The influence of maternal stress in pregnancy. Neurosci. Biobehav. Rev. 2017. [Google Scholar] [CrossRef]
- Guardino, C.M.; Schetter, C.D. Coping during pregnancy: A systematic review and recommendations. Health Psychol. Rev. 2014, 8, 70–94. [Google Scholar] [CrossRef]
- Weyers, P.; Ising, M.; Reuter, M.; Janke, W. Comparing two approaches for the assessment of coping: Part I. Psychometric properties and intercorrelations. J. Individ. Differ. 2005, 26, 207–212. [Google Scholar] [CrossRef]
- Xie, Y. The initial exploration of reliability and validity of simplified coping styles questionnaire. Chin. J. Clin. Psychol. 1998, 6, 114–115. [Google Scholar]
- Morling, B.; Kitayama, S.; Miyamoto, Y. American and Japanese Women Use Different Coping Strategies During Normal Pregnancy. Personal. Soc. Psychol. Bull. 2003, 29, 1533–1546. [Google Scholar] [CrossRef]
- Azale, T.; Fekadu, A.; Medhin, G.; Hanlon, C. Coping strategies of women with postpartum depression symptoms in rural Ethiopia: A cross-sectional community study. BMC Psychiatry 2018, 18, 41. [Google Scholar] [CrossRef]
- See, C.M.; Essau, C.A. Coping Strategies in Cross-Cultural Comparison. In Psychologie–Kultur–Gesellschaft; Mayer, B., Kornadt, H.-J., Eds.; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2010; pp. 161–173. [Google Scholar]
- Ngai, F.-W.; Chan, S.W.-C.; Holroyd, E. Maternal Coping during Early Motherhood among First-time Chinese Mothers. J. Health Psychol. 2012, 17, 189–196. [Google Scholar] [CrossRef]
- Li, Y.; Zeng, Y.; Zhu, W.; Cui, Y.; Li, J. Path model of antenatal stress and depressive symptoms among Chinese primipara in late pregnancy. BMC Pregnancy Childbirth 2016, 16, 180. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.; Jiang, X.; Yao, J.; Li, X.; Liu, X.; Pang, M.; Chiang, C.L.V. Depression, Social Support, and Coping Styles among Pregnant Women after the Lushan Earthquake in Ya’an, China. PLoS ONE 2015, 10, e0135809. [Google Scholar] [CrossRef] [PubMed]
- Ockhuijsen, H.; van den Hoogen, A.; Eijkemans, M.; Macklon, N.; Boivin, J. Clarifying the benefits of the positive reappraisal coping intervention for women waiting for the outcome of IVF. Hum. Reprod. 2014, 29, 2712–2718. [Google Scholar] [CrossRef] [PubMed]
- Mcmillan, S.C.; Small, B.J.; Weitzner, M.; Schonwetter, R.; Tittle, M.; Moody, L.; Haley, W.E. Impact of coping skills intervention with family caregivers of hospice patients with cancer: A randomized clinical trial. Cancer 2010, 106, 214–222. [Google Scholar] [CrossRef] [PubMed]
- National Bureau of Statistics. China Statistical Yearbook; National Bureau of Statistics: Beijing, China, 2018.
- WJX.cn. Questionnaire Survey/Online Examination. 2006. Available online: https://www.wjx.cn/ (accessed on 20 February 2020).
- Xu, J.; Kang, Q.; Song, Z.; Clarke, C.P. Applications of Mobile Social Media: WeChat among Academic Libraries in China. J. Acad. Librariansh. 2015, 41, 21–30. [Google Scholar] [CrossRef]
- Zhang, N.; Gao, Y.; Wu, R.; Qiu, P.Y. Validity and reliability of the short form of the revised Conflict Tactics Scales in women suffering from domestic violence in rural areas. Chin. Ment. Health J. 2014, 28, 381–384. [Google Scholar]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Zeng, Q.-Z.; He, Y.-L.; Liu, H.; Miao, J.-M.; Chen, J.-X.; Xu, H.-N.; Wang, J.-Y. Reliability and validity of Chinese version of the Generalized Anxiety Disorder 7-item (GAD-7) scale in screening anxiety disorders in outpatients from traditional Chinese internal department. [Reliability and validity of Chinese version of the Generalized Anxiety Disorder 7-item (GAD-7) scale in screening anxiety disorders in outpatients from traditional Chinese internal department.]. Chin. Ment. Health J. 2013, 27, 163–168. [Google Scholar]
- Tong, X.; An, D.; McGonigal, A.; Park, S.-P.; Zhou, D. Validation of the Generalized Anxiety Disorder-7 (GAD-7) among Chinese people with epilepsy. Epilepsy Res. 2016, 120, 31–36. [Google Scholar] [CrossRef]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef]
- Lai, J.C.L.; Yue, X. Using the Brief Resilience Scale to Assess Chinese People’s Ability to Bounce Back from Stress. SAGE Open 2014, 4, 2158244014554386. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; Princeton University Press: Princeton, NJ, USA, 2015. [Google Scholar]
- Wang, M.; Cai, B.; Wu, Y.; Dai, X. The Factor Structure of Chinese Rosenberg’Self-esteem Scale Affected by Item Statement Method. Psychol. Explor. 2010, 30, 63–68. [Google Scholar]
- Yang, Y.; Wang, D. Retest of the Bidimensional Model of Rosenberg Self-Esteem Scale. Chin. Ment. Health J. 2007, 21, 603–605. [Google Scholar]
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry J. Ment. Sci. 1987, 150, 782–786. [Google Scholar] [CrossRef]
- Murray, D.; Cox, J.L. Screening for depression during pregnancy with the edinburgh depression scale (EDDS). J. Reprod. Infant Psychol. 1990, 8, 99–107. [Google Scholar] [CrossRef]
- Lee, D.T.; Yip, S.; Chiu, H.F.; Leung, T.Y.; Chan, K.P.; Chau, I.O.; Leung, H.C.; Chung, T.K. Detecting postnatal depression in Chinese women: Validation of the Chinese version of the Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1998, 172, 433–437. [Google Scholar] [CrossRef]
- Cox, J.; Holden, J.; Henshaw, C. Perinatal Mental Health: The Edinburgh Postnatal Depression Scale (EPDS) Manual, 2nd ed.; RCPsych Publications: London, UK, 2014. [Google Scholar]
- Wang, Y.; Guo, X.; Lau, Y.; Chan, K.S.; Yin, L.; Chen, J. Psychometric evaluation of the Mainland Chinese version of the Edinburgh Postnatal Depression Scale. Int. J. Nurs. Stud. 2009, 46, 813–823. [Google Scholar] [CrossRef]
- Alin, A. Multicollinearity. Wiley Interdiscip. Rev. Comput. Stat. 2010, 2, 370–374. [Google Scholar] [CrossRef]
- Hu, Q.; Bernardo, A.B.I.; Lam, S.W.; Cheang, P.K. Individualism-Collectivism Orientations and Coping Styles of Cyberbullying Victims in Chinese Culture. Curr. Psychol. 2018, 37, 65–72. [Google Scholar] [CrossRef]
- Sun, T.; Horn, M.; Merritt, D. Values and lifestyles of individualists and collectivists: A study on Chinese, Japanese, British and US consumers. J. Consum. Mark. 2004, 21, 318–331. [Google Scholar] [CrossRef]
- Renae Stancil, T.; Hertz-Picciotto, I.; Schramm, M.; Watt-Morse, M. Stress and pregnancy among African-American women. Paediatr. Perinat. Epidemiol. 2000, 14, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Dunkel Schetter, C. Psychological Science on Pregnancy: Stress Processes, Biopsychosocial Models, and Emerging Research Issues. Annu. Rev. Psychol. 2011, 62, 531–558. [Google Scholar] [CrossRef] [PubMed]
- Rauch, S.A.; Defever, E.; Oetting, S.; Graham-Bermann, S.A.; Seng, J.S. Optimism, Coping, and Posttraumatic Stress Severity in Women in the Childbearing Year. Psychol. Trauma Theory Res. Pract. Policy 2013, 5, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Kotzé, M.; Sikkema, K.; Forsyth, B. Psychosocial Variables Associated with Coping of HIV-Positive Women Diagnosed During Pregnancy. Aids Behav. 2013, 17, 498–507. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Participants in Study (n = 615) | Participants Lost to Follow-Up (n = 511) | |||
|---|---|---|---|---|---|
| n | % | n | % | p Value 1 | |
| Advanced Age | |||||
| No | 495 | 80.5 | 411 | 80.4 | 0.981 |
| Yes | 120 | 19.5 | 100 | 19.6 | |
| Employed | |||||
| No | 157 | 25.5 | 122 | 23.9 | 0.522 |
| Yes | 458 | 74.5 | 389 | 76.1 | |
| Education status | |||||
| Middle school or lower | 57 | 9.3 | 70 | 13.7 | 0.107 |
| High school | 141 | 22.9 | 117 | 22.9 | |
| Bachelor | 366 | 59.5 | 281 | 55.0 | |
| Postgraduate or higher | 51 | 8.3 | 43 | 8.4 | |
| Income level | |||||
| <2000 | 200 | 32.5 | 168 | 32.9 | 0.099 |
| 2000~ | 322 | 52.4 | 224 | 43.8 | |
| 5000~ | 80 | 13 | 101 | 19.8 | |
| ≥10,000 | 13 | 2.1 | 18 | 3.5 | |
| Marital satisfaction | |||||
| Very satisfied | 518 | 84.2 | 405 | 79.3 | 0.031 |
| Not very satisfied | 97 | 15.8 | 106 | 20.7 | |
| Living with parents-in-law | |||||
| No | 411 | 66.8 | 332 | 65.0 | 0.512 |
| Yes | 204 | 33.2 | 179 | 35.0 | |
| Past history of mood disorders | |||||
| No | 598 | 97.2 | 506 | 99.0 | 0.031 |
| Yes | 17 | 2.8 | 5 | 1.0 | |
| First pregnancy | |||||
| No | 433 | 70.4 | 403 | 78.9 | 0.001 |
| Yes | 182 | 29.6 | 108 | 21.1 | |
| Previous miscarriage | |||||
| No | 305 | 49.6 | 269 | 52.6 | 0.308 |
| Yes | 310 | 50.4 | 242 | 47.4 | |
| Parity | |||||
| 0 | 362 | 58.9 | 277 | 54.2 | 0.117 |
| ≥1 | 253 | 41.1 | 234 | 45.8 | |
| Smoking | |||||
| No | 594 | 96.6 | 489 | 95.7 | 0.438 |
| Yes | 21 | 3.4 | 22 | 4.3 | |
| Drinking | |||||
| No | 568 | 92.4 | 472 | 92.4 | 0.995 |
| Yes | 47 | 7.6 | 39 | 7.6 | |
| Employed (partner) | |||||
| No | 17 | 2.8 | 10 | 2.0 | 0.378 |
| Yes | 598 | 97.2 | 501 | 98.0 | |
| Education status (partner) | |||||
| Middle school or lower | 73 | 11.9 | 71 | 13.9 | 0.814 |
| High school | 146 | 23.7 | 113 | 22.1 | |
| Bachelor | 343 | 55.8 | 281 | 55.0 | |
| Postgraduate or higher | 53 | 8.6 | 46 | 9.0 | |
| GAD-7 (Mean, SD) | 2.899 (2.862) | 3.147 (2.941) | 0.102 | ||
| Depression (Mean, SD) | 8.424 (3.992) | 8.787 (3.965) | 0.127 | ||
| Coping Styles | Mean (SD) | Never | Sometimes | Often | Almost Always |
|---|---|---|---|---|---|
| Positive Coping | |||||
| Take my mind off things through study, work or other activities | 1.98 (0.79) | 15 (2.4) | 152 (24.7) | 280 (45.5) | 168 (27.3) |
| Talk with others about my trouble | 2.21 (0.81) | 7 (1.1) | 129 (21.0) | 208 (33.8) | 271 (44.1) |
| Focus on good aspects of things | 2.36 (0.73) | 4 (0.7) | 80 (13.0) | 222 (36.1) | 309 (50.2) |
| Change my mind and rediscover important things in life | 2.13 (0.74) | 4 (0.7) | 119 (19.3) | 282 (45.9) | 210 (34.1) |
| Do not take problems too seriously | 2.18 (0.83) | 16 (2.6) | 118 (19.2) | 220 (35.8) | 261 (42.4) |
| Stand my ground and fight for what I want | 1.90 (0.80) | 27 (4.4) | 146 (23.7) | 302 (49.1) | 140 (22.8) |
| Come up with strategies to cope | 2.06 (0.74) | 8 (1.3) | 129 (21.0) | 298 (48.5) | 180 (29.3) |
| Get help and advice from other people | 2.08 (0.82) | 25 (4.1) | 108 (17.6) | 274 (44.6) | 208 (33.8) |
| Change some of my original practices or some of my own problems | 1.90 (0.72) | 14 (2.3) | 149 (24.2) | 337 (54.8) | 115 (18.7) |
| Learn from others to deal with the similar situation | 1.92 (0.76) | 20 (3.3) | 147 (23.9) | 312 (50.7) | 136 (22.1) |
| Seeking hobbies like taking part in cultural or sports activities | 1.80 (0.85) | 39 (6.3) | 181 (29.4) | 261 (42.4) | 134 (21.8) |
| Try to control my disappointment, regret, sadness and anger | 2.01 (0.80) | 21 (3.4) | 129 (21.0) | 286 (46.5) | 179 (29.1) |
| Negative coping | |||||
| Take a rest or vacation, put the problem aside temporarily | 1.92 (0.84) | 36 (5.9) | 133 (21.6) | 288 (46.8) | 158 (25.7) |
| Use alcohol, cigarette or other drugs to help me get through it | 0.20 (0.58) | 541 (88.0) | 35 (5.7) | 31 (5.0) | 8 (1.3) |
| Time will change the situation and the only thing I could do is waiting | 1.15 (0.84) | 131 (21.3) | 308 (50.1) | 130 (21.1) | 46 (7.5) |
| Try to forget everything | 1.25 (0.90) | 131 (21.3) | 261 (42.4) | 162 (26.3) | 61 (9.9) |
| Rely on others to solve problems | 0.87 (0.77) | 218 (35.4) | 275 (44.7) | 109 (17.7) | 13 (2.1) |
| Accept the reality | 1.27 (0.83) | 105 (17.1) | 287 (46.7) | 175 (28.5) | 48 (7.8) |
| Imagine the occurrence of miracle | 0.98 (0.83) | 191 (31.1) | 273 (44.4) | 125 (20.3) | 26 (4.2) |
| Comfort myself | 1.89 (0.83) | 22 (3.6) | 182 (29.6) | 250 (40.7) | 161 (26.2) |
| Characteristics | Mean (SD) | Crude β (95% CI) | Adjusted β (95% CI) |
|---|---|---|---|
| Advanced Age | |||
| No | 2.029 (0.503) | — | — |
| Yes | 2.040 (0.510) | 0.011 (−0.090, 0.112) | −0.003 (−0.108, 0.101) |
| Employed | |||
| No | 1.956 (0.529) | — | — |
| Yes | 2.058 (0.494) | 0.102 (0.011, 0.193) | −0.045(−0.163, 0.074) |
| Education status | |||
| Middle school or lower | 1.692 (0.571) | — | — |
| High school | 1.974 (0.509) | 0.283 (0.132, 0.433) | 0.210 (0.056, 0.364) |
| Bachelor | 2.077 (0.479) | 0.385 (0.249, 0.522) | 0.242 (0.083, 0.400) |
| Postgraduate or higher | 2.245 (0.392) | 0.553 (0.368, 0.738) | 0.353 (0.134, 0.576) |
| Income level | |||
| <2000 | 1.939 (0.519) | — | — |
| 2000~ | 2.062 (0.494) | 0.123 (0.035, 0.212) | 0.063 (−0.051, 0.177) |
| 5000~ | 2.101 (0.472) | 0.162 (0.032, 0.292) | 0.032 (−0.119, 0.183) |
| ≥10,000 | 2.276 (0.526) | 0.337 (0.056, 0.618) | 0.172 (−0.100, 0.444) |
| Marital satisfaction | |||
| Very satisfied | 2.063 (0.501) | — | — |
| Not very satisfied | 1.863 (0.492) | −0.200 (−0.309, −0.091) | −0.037 (−0.146, 0.072) |
| Living with parents-in-law | |||
| No | 2.049 (0.494) | — | — |
| Yes | 1.997 (0.525) | −0.051 (−0.136, 0.034) | 0.041 (−0.042, 0.123) |
| Past history of mood disorders | |||
| No | 2.029 (0.503) | — | — |
| Yes | 2.123 (0.542) | 0.094 (−0.149, 0.338) | 0.053 (−0.175, 0.281) |
| First pregnancy | |||
| No | 1.989 (0.512) | — | — |
| Yes | 2.132 (0.472) | 0.143 (0.056, 0.230) | 0.076 (−0.040, 0.193) |
| Previous miscarriage | |||
| No | 2.074 (0.494) | — | — |
| Yes | 2.046 (0.477) | −0.083 (−0.163, −0.004) | 0.006 (−0.090, 0.103) |
| Parity | |||
| 0 | 2.089 (0.484) | — | — |
| ≥1 | 1.949 (0.522) | −0.140 (−0.221, −0.060) | −0.039 (−0.134, 0.057) |
| Smoking | |||
| No | 2.033 (0.504) | — | — |
| Yes | 1.979 (0.511) | −0.054 (−0.274, 0.166) | −0.019 (−0.242, 0.204) |
| Drinking | |||
| No | 2.038 (0.507) | — | — |
| Yes | 1.955 (0.471) | −0.083 (−0.233, 0.067) | −0.043 (−0.195, 0.109) |
| Employed (partner) | |||
| No | 1.897 (0.500) | — | — |
| Yes | 2.035 (0.504) | 0.138 (−0.105, 0.382) | 0.050 (−0.178, 0.278) |
| Education status (partner) | |||
| Middle school or lower | 1.853 (0.488) | — | — |
| High school | 1.927 (0.538) | 0.075 (−0.065, 0.214) | −0.028 (−0.168, 0.113) |
| Bachelor | 2.087 (0.485) | 0.235 (0.109, 0.360) | 0.077 (−0.063, 0.218) |
| Postgraduate or higher | 2.206 (0.438) | 0.354 (0.179, 0.529) | 0.111 (−0.092, 0.314) |
| Intimate partner violence | |||
| No | 2.050 (0.496) | — | — |
| Yes | 1.866 (0.548) | −0.082 (−0.149, −0.015) | −0.082 (−0.209, 0.044) |
| GAD−7 (Mean, SD) | 2.899 (2.862) | −0.034 (−0.048, −0.020) | −0.013 (−0.027, 0.001) |
| Resilience (Mean, SD) | 3.498 (0.580) | 0.293 (0.228, 0.358) | 0.233 (0.163, 0.302) |
| Self-esteem (Mean, SD) | 29.385 (3.383) | 0.024 (0.007, 0.040) | 0.017 (0.001, 0.032) |
| Characteristics | Mean (SD) | Crude β (95% CI) | Adjusted β (95% CI) |
|---|---|---|---|
| Advanced Age | |||
| No | 2.029 (0.503) | — | — |
| Yes | 2.040 (0.510) | 0.001 (−0.102, 0.104) | −0.008 (−0.125, 0.108) |
| Employed | |||
| No | 1.956 (0.529) | — | — |
| Yes | 2.058 (0.494) | 0.014 (−0.079, 0.107) | −0.010 (−0.141, 0.122) |
| Education status | |||
| Middle school or lower | 1.033 (0.502) | — | — |
| High school | 1.233 (0.542) | 0.200 (0.042, 0.357) | 0.203 (0.032, 0.374) |
| Bachelor | 1.214 (0.490) | 0.181 (0.038, 0.324) | 0.174 (−0.002, 0.351) |
| Postgraduate or higher | 1.294 (0.580) | 0.261 (0.067, 0.454) | 0.267 (0.021, 0.513) |
| Income level (per month) | |||
| <2000 | 1.186 (0.521) | — | — |
| 2000~ | 1.217 (0.508) | 0.031 (−0.060, 0.122) | 0.005 (−0.123, 0.132) |
| 5000~ | 1.198 (0.489) | 0.012 (−0.122, 0.145) | −0.038 (−0.206, 0.129) |
| ≥10,000 | 1.375 (0.683) | 0.189 (−0.100, 0.478) | 0.235 (−0.068, 0.537) |
| Marital satisfaction | |||
| Very satisfied | 2.063 (0.501) | — | — |
| Not very satisfied | 1.863 (0.492) | 0.069 (−0.042, 0.181) | 0.020 (−0.101, 0.141) |
| Living with parents-in-law | |||
| No | 1.214 (0.514) | — | — |
| Yes | 1.197 (0.513) | −0.017 (−0.103, 0.070) | 0.012 (−0.079, 0.104) |
| Past history of mood disorders | |||
| No | 2.029 (0.503) | — | — |
| Yes | 2.123 (0.542) | −0.017 (−0.266, 0.231) | −0.033 (−0.286, 0.221) |
| First pregnancy | |||
| No | 1.989 (0.512) | — | — |
| Yes | 2.132 (0.472) | −0.030 (−0.119, 0.059) | −0.015 (−0.144, 0.114) |
| Previous miscarriage | |||
| No | 2.074 (0.494) | — | — |
| Yes | 2.046 (0.477) | 0.040 (−0.041, −0.121) | 0.044 (−0.063, 0.151) |
| Parity | |||
| 0 | 2.089 (0.484) | — | — |
| ≥1 | 1.949 (0.522) | −0.005 (−0.088, 0.077) | −0.004 (−0.110, 0.103) |
| Smoking | |||
| No | 2.033 (0.504) | — | — |
| Yes | 1.979 (0.511) | −0.020 (−0.244, 0.204) | −0.034 (−0.282, 0.214) |
| Drinking | |||
| No | 2.038 (0.507) | — | — |
| Yes | 1.955 (0.471) | 0.058 (−0.095, 0.211) | 0.074 (−0.095, 0.243) |
| Employed (partner) | |||
| No | 1.897 (0.500) | — | — |
| Yes | 2.035 (0.504) | −0.036 (−0.284, 0.213) | −0.030 (−0.284, 0.223) |
| Education status (partner) | |||
| Middle school or lower | 1.116 (0.514) | — | — |
| High school | 1.171 (0.510) | 0.055 (−0.089, 0.199) | −0.006 (−0.163, 0.150) |
| Bachelor | 1.235 (0.500) | 0.119 (−0.011, 0.249) | 0.072 (−0.084, 0.229) |
| Postgraduate or higher | 1.258 (0.596) | 0.142 (−0.040, 0.323) | 0.073 (−0.153, 0.299) |
| Intimate partner violence | |||
| No | 1.198 (0.508) | — | |
| Yes | 1.298 (0.554) | 0.112 (−0.026, 0.250) | 0.040 (−0.100, 0.181) |
| GAD-7 (Mean, SD) | 2.899 (2.862) | 0.014 (0.000, 0.028) | 0.008 (−0.008, 0.023) |
| Resilience (Mean, SD) | 3.498 (0.580) | −0.108 (−0.178, −0.039) | −0.106 (−0.183, −0.028) |
| Self-esteem (Mean, SD) | 29.385 (3.383) | 0.000 (−0.017, 0.017) | 0.001 (−0.017, 0.018) |
| Variables | Without Postpartum Depression (n = 453) n (%) Mean (SD) | With Postpartum Depression (n = 162) n (%) Mean (SD) | p Value 1 |
|---|---|---|---|
| Advanced Age | |||
| No | 357 (72.1) | 138 (27.9) | 0.079 |
| Yes | 96 (80.0) | 24 (20.0) | |
| Employed | |||
| No | 100 (63.7) | 75 (36.3) | 0.001 |
| Yes | 353 (77.1) | 105 (22.9) | |
| Education status | |||
| Middle school | 38 (66.7) | 19 (33.3) | 0.443 |
| High school | 103 (73.0) | 38 (27.0) | |
| Bachelor | 271 (74.0) | 95 (26.0) | |
| Postgraduate or higher | 41 (80.4) | 10 (19.6) | |
| Income level | |||
| <2000 | 137 (68.5) | 63 (31.5) | 0.010 |
| 2000~5000 | 242 (75.2) | 80 (24.8) | |
| 5001~10,000 | 61 (76.3) | 19 (23.7) | |
| >10,000 | 13 (100) | 0 (0) | |
| Marital satisfaction | |||
| Very satisfied | 396 (76.4) | 122 (23.6) | 0.001 |
| Not very satisfied | 57 (58.8) | 40 (41.2) | |
| Past history of mood disorders | |||
| No | 442 (73.9) | 156 (26.1) | 0.735 |
| Yes | 11 (64.7) | 6 (35.3) | |
| First pregnancy | |||
| No | 319 (73.7) | 114 (26.3) | 0.991 |
| Yes | 134 (73.6) | 48 (26.4) | |
| Previous miscarriage | |||
| No | 219 (71.8) | 86 (28.2) | 0.300 |
| Yes | 234 (75.5) | 76 (24.5) | |
| Parity | |||
| 0 | 261 (72.1) | 101 (27.9) | 0.294 |
| ≥1 | 192 (75.9) | 61 (24.1) | |
| Intimate partner violence | |||
| No | 421 (76.1) | 132 (23.9) | 0.001 |
| Yes | 32 (51.6) | 30 (48.4) | |
| Obstetric complications | |||
| No | 392 (66.0) | 202 (34.0) | 0.698 |
| Yes | 13 (61.9) | 8 (38.1) | |
| GAD-7 | 2.488 (2.595) | 4.048 (3.244) | 0.001 |
| Positive coping | 2.086 (0.470) | 1.878 (0.564) | 0.001 |
| Negative coping | 1.183 (0.504) | 1.278 (0.535) | 0.042 |
| Variables | B | St | β | t | p |
|---|---|---|---|---|---|
| Advanced age | −0.461 | 0.488 | −0.039 | −0.946 | 0.345 |
| Employed | −0.802 | 0.558 | −0.075 | −1.437 | 0.151 |
| Education status | |||||
| Middle school | — | — | — | — | — |
| High school | −0.267 | 0.692 | −0.024 | −0.385 | 0.700 |
| Bachelor | −0.077 | 0.666 | −0.008 | −0.115 | 0.908 |
| Postgraduate or higher | −0.041 | 0.915 | −0.002 | −0.045 | 0.964 |
| Income level | |||||
| <2000 | — | — | — | — | — |
| 2000~5000 | 0.261 | 0.540 | 0.028 | 0.483 | 0.629 |
| 5001~10,000 | 0.125 | 0.707 | 0.009 | 0.177 | 0.859 |
| >10,000 | −0.242 | 1.289 | −0.007 | −0.188 | 0.851 |
| Marital satisfaction | 1.129 | 0.506 | 0.088 | 2.231 | 0.026 |
| Past history of mood disorders | −0.602 | 1.075 | −0.021 | −0.560 | 0.576 |
| First pregnancy | 0.122 | 0.553 | 0.012 | 0.222 | 0.825 |
| Previous miscarriage | −0.539 | 0.453 | −0.058 | −1.191 | 0.234 |
| Parity | −0.123 | 0.453 | −0.013 | −0.271 | 0.787 |
| Intimate partner violence | 0.398 | 0.385 | 0.030 | 1.035 | 0.301 |
| Obstetric complications | 0.012 | 0.439 | 0.002 | 0.032 | 0.740 |
| GAD-7 | 0.438 | 0.065 | 0.268 | 6.753 | 0.000 |
| Positive coping | −0.560 | 0.245 | −0.071 | −2.282 | 0.023 |
| Negative coping | 0.491 | 0.229 | 0.063 | 2.147 | 0.032 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, M.; Gong, W.; Taylor, B.; Cai, Y.; Xu, D. Coping Styles in Pregnancy, Their Demographic and Psychological Influences, and Their Association with Postpartum Depression: A Longitudinal Study of Women in China. Int. J. Environ. Res. Public Health 2020, 17, 3654. https://doi.org/10.3390/ijerph17103654
Yu M, Gong W, Taylor B, Cai Y, Xu D. Coping Styles in Pregnancy, Their Demographic and Psychological Influences, and Their Association with Postpartum Depression: A Longitudinal Study of Women in China. International Journal of Environmental Research and Public Health. 2020; 17(10):3654. https://doi.org/10.3390/ijerph17103654
Chicago/Turabian StyleYu, Min, Wenjie Gong, Beck Taylor, Yiyuan Cai, and Dong (Roman) Xu. 2020. "Coping Styles in Pregnancy, Their Demographic and Psychological Influences, and Their Association with Postpartum Depression: A Longitudinal Study of Women in China" International Journal of Environmental Research and Public Health 17, no. 10: 3654. https://doi.org/10.3390/ijerph17103654
APA StyleYu, M., Gong, W., Taylor, B., Cai, Y., & Xu, D. (2020). Coping Styles in Pregnancy, Their Demographic and Psychological Influences, and Their Association with Postpartum Depression: A Longitudinal Study of Women in China. International Journal of Environmental Research and Public Health, 17(10), 3654. https://doi.org/10.3390/ijerph17103654