The Influence of Lifestyle on the Incidence of Dental Caries among 3-Year-Old Japanese Children

Abstract
:1. Introduction
2. Subjects and Methods
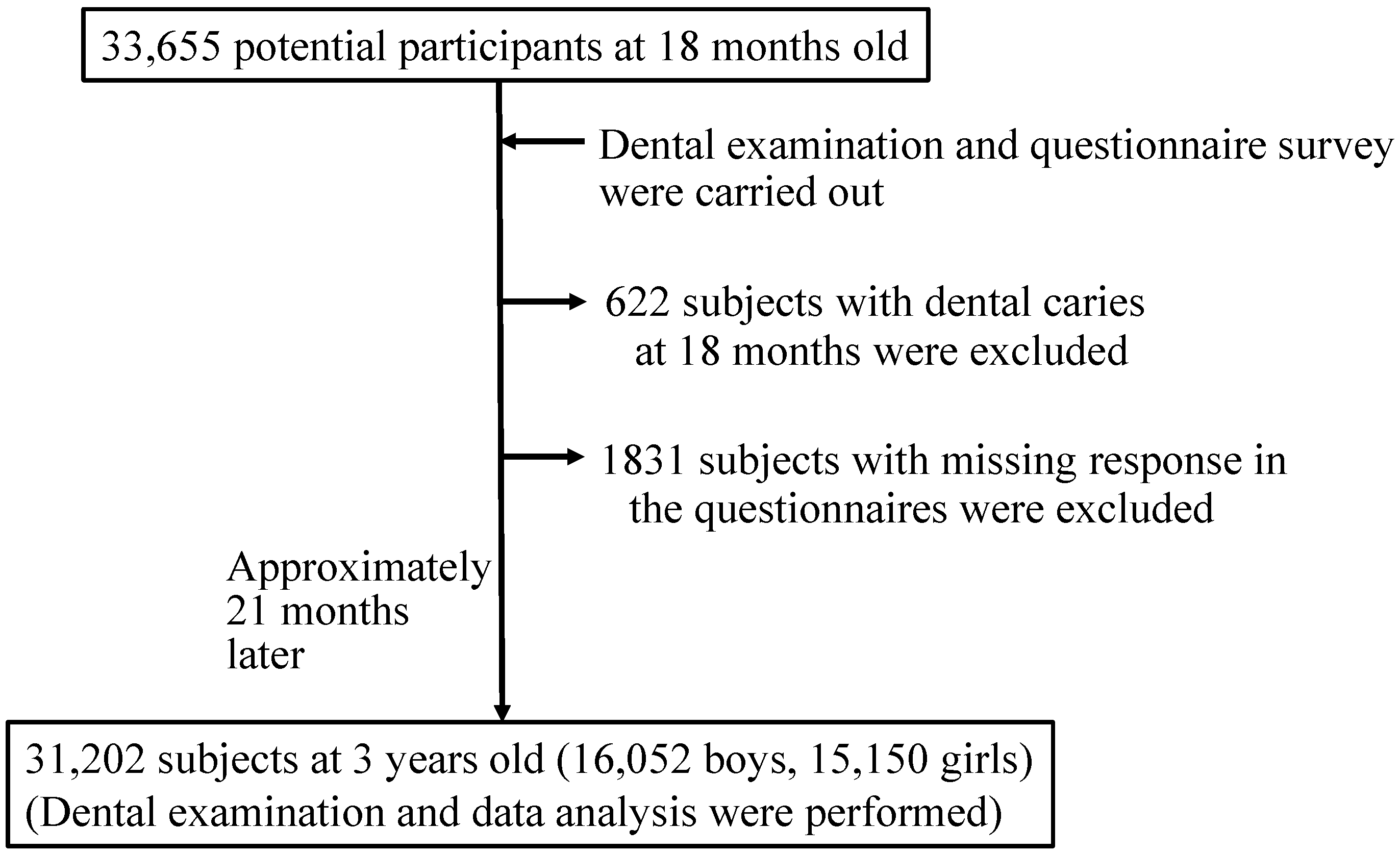
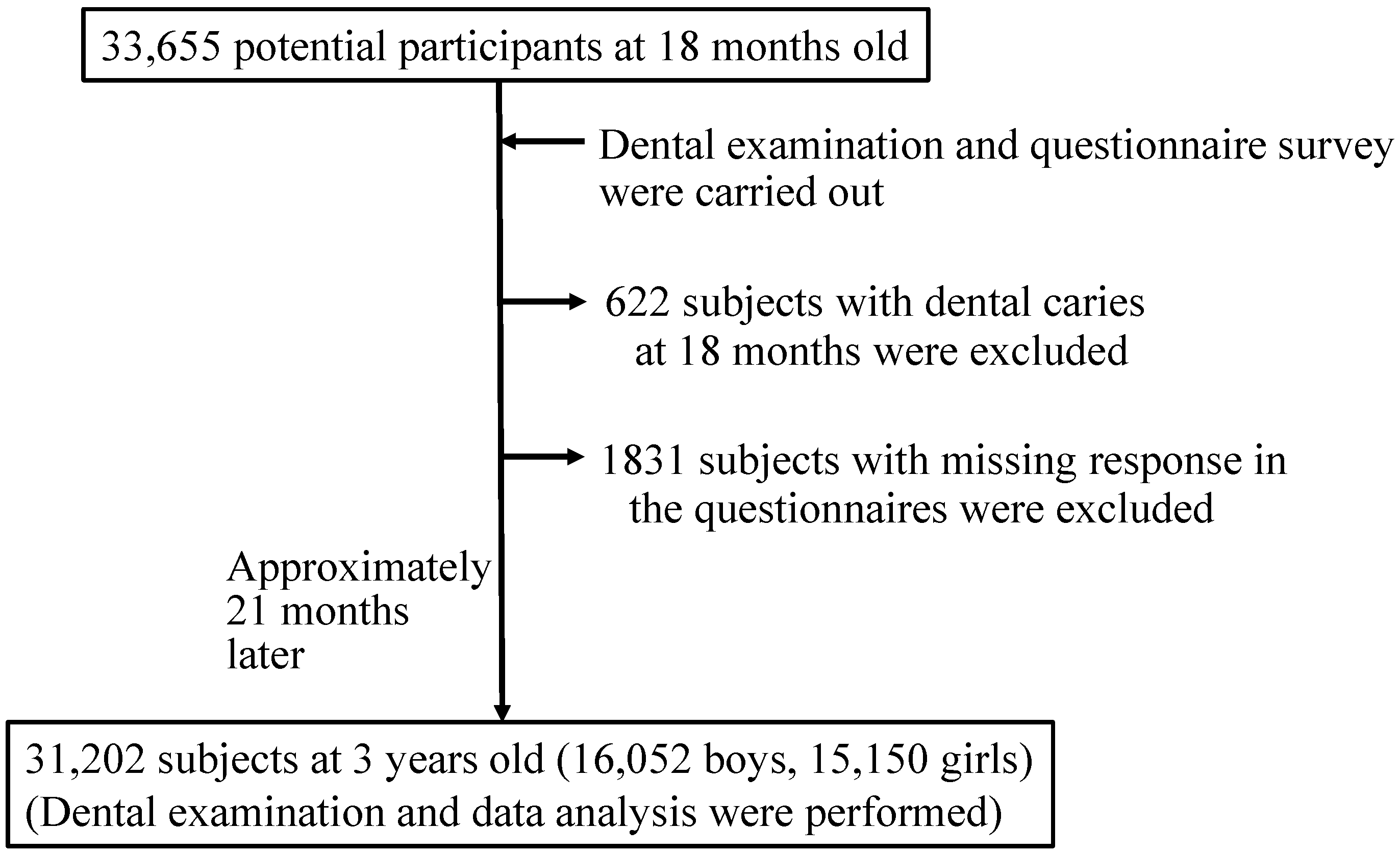
2.1. Participants
2.2. Information on Lifestyle and Household Environment on Children Aged 1.5 Years Old
2.3. Dental Examination
2.4. Caries Activity Test (Cariostat)
2.5. Statistical Analysis
3. Results and Discussion
3.1. Characteristics of Caries-Free Subjects at Age 1.5 Years

{kind=link}
| Variable | All (n = 31,202) | Boy (n = 16,052) | Girl (n = 15,150) |
|---|---|---|---|
| n (%) | n (%) | n (%) | |
| Breastfeeding | 6834 (21.9) | 3416 (21.3) | 3418 (22.6) |
| Daily frequency of sweet snack intake | |||
| 0 | 764 (2.4) | 423 (2.6) | 341 (2.3) |
| 1 | 15,270 (48.9) | 7843 (48.9) | 7427 (49.0) |
| 2 | 13,529 (43.4) | 6944 (43.3) | 6585 (43.5) |
| 3 | 1639 (5.3) | 842 (5.2) | 797 (5.3) |
| Daily sugar sweetened-beverage consumption | 13,661 (43.8) | 7097 (44.2) | 6564 (43.3) |
| Child’s bedtime | |||
| Before 9 p.m. | 7081 (22.7) | 3732 (23.2) | 3349 (22.1) |
| 9~11 p.m. | 19,580 (62.8) | 10,082 (62.8) | 9498 (62.7) |
| After 11 p.m. | 1921 (6.2) | 914 (5.7) | 1007 (6.6) |
| Irregular | 2620 (8.4) | 1324 (8.2) | 1296 (8.6) |
| Daily toothbrushing by parents | 19,733 (63.2) | 9936 (61.9) | 9797 (64.7) |
| Varnish of fluoride | 26,990 (86.5) | 13,886 (86.5) | 13,104 (86.5) |
| Smoking of family members | 13,994 (44.8) | 7199 (44.8) | 6795 (44.9) |
| Order of birth | |||
| 1st | 15,323 (49.1) | 7945 (49.5) | 7378 (48.7) |
| 2nd | 11,981 (38.4) | 6084 (37.9) | 5897 (38.9) |
| 3rd or more | 3898 (12.5) | 2023 (12.6) | 1875 (12.4) |
| Cariostat score | |||
| 0.0 | 1583 (5.1) | 759 (4.7) | 824 (5.4) |
| 1.0 | 17,195 (55.1) | 8905 (55.5) | 8290 (54.7) |
| 2.0 | 11,693 (37.5) | 5990 (37.3) | 5703 (37.6) |
| 3.0 | 731 (2.3) | 398 (2.5) | 333 (2.2) |
3.2. Incidence of Dental Caries in 3-Year-Old Subjects
| Variables | All subjects (n = 31,202) | Boy (n = 16,052) | Girl (n = 15,150) | |||
|---|---|---|---|---|---|---|
| n (%) | p a | n (%) | p a | n (%) | p a | |
| Incidence of dental caries | 5106 (16.4) | 2777 (17.3) | 2329 (15.4) | <0.001 | ||
| Breastfeeding | <0.001 | <0.001 | <0.001 | |||
| No | 3422 (14.2) | 1856 (14.7) | 1566 (13.3) | |||
| Yes | 1684 (24.6) | 921 (27.0) | 763 (22.3) | |||
| Daily frequency of sweet snack intake | <0.001 | <0.001 | <0.001 | |||
| 0 | 43 (5.6) | 22 (5.2) | 21 (6.2) | |||
| 1 | 1925 (12.6) | 1054 (13.4) | 871 (11.7) | |||
| 2 | 2733 (20.2) | 1482 (21.3) | 1251 (19.0) | |||
| 3 | 405 (24.7) | 219 (26.0) | 186 (23.3) | |||
| Daily sugar-sweetened beverage consumption | <0.001 | <0.001 | <0.001 | |||
| No | 2324 (13.2) | 1254 (14.0) | 1070 (12.5) | |||
| Yes | 2782 (20.4) | 1523 (21.5) | 1259 (19.2) | |||
| Child’s bedtime | <0.001 | <0.001 | <0.001 | |||
| Before 9 p.m. | 852 (12.0) | 480 (12.9) | 372 (11.1) | |||
| 9~11 p.m. | 3256 (16.6) | 1789 (17.7) | 1467 (15.4) | |||
| After 11 p.m. | 430 (22.4) | 195 (21.3) | 235 (23.3) | |||
| Irregular | 568 (21.7) | 313 (23.6) | 255 (19.7) | |||
| Daily toothbrushing by parents | <0.001 | <0.001 | <0.001 | |||
| Yes | 2708 (13.7) | 1439 (14.5) | 1269 (13.0) | |||
| No | 2398 (20.9) | 1338 (21.9) | 1060 (19.8) | |||
| Varnish of fluoride | <0.001 | <0.001 | <0.001 | |||
| Yes | 4130 (15.3) | 2240 (16.1) | 1890 (14.4) | |||
| No | 976 (23.2) | 537 (24.8) | 439 (21.5) | |||
| Smoking of family members | <0.001 | <0.001 | <0.001 | |||
| No | 2317 (13.5) | 1266 | (14.3) | 1051 (12.6) | ||
| Yes | 2789 (19.9) | 1511 | (21.0) | 1278 (18.8) | ||
| Order of birth | <0.001 | <0.001 | <0.001 | |||
| 1st | 1933 (12.6) | 1085 (13.7) | 848 (11.5) | |||
| 2nd | 2121 (17.7) | 1125 (18.5) | 996 (16.9) | |||
| 3rd or more | 1052 (27.0) | 567 (28.0) | 485 (25.4) | |||
| Cariostat score | <0.001 | <0.001 | <0.001 | |||
| 0.0 | 155 (9.8) | 79 (10.4) | 76 (9.2) | |||
| 1.0 | 2347 (13.6) | 1288 (14.5) | 1059 (12.8) | |||
| 2.0 | 2339 (20.0) | 1259 (21.0) | 1080 (18.9) | |||
| 3.0 | 265 (36.3) | 151 (37.9) | 114 (34.2) | |||
3.3. Breastfeeding Was Positively Associated with Dental Caries in Children
3.4. Consumption of Sweet Snacks and Sugar-Sweetened Beverages Increased the Risk of Developing Dental Caries in Children
| Variables | All (n = 31,202) | Boy (n = 16,052) | Girl (n = 15,150) | |||
|---|---|---|---|---|---|---|
| OR a (95% CI b) | p | OR c (95% CI b) | p | OR c (95% CI b) | p | |
| Breastfeeding | ||||||
| No | 1.0 | 1.0 | 1.0 | |||
| Yes | 2.06 (1.93, 2.21) | <0.001 | 2.21 (2.01, 2.43) | <0.001 | 1.91 (1.73, 2.11) | <0.001 |
| Daily frequency of sweet snack intake | ||||||
| 0 | 1.0 | 1.0 | 1.0 | |||
| 1 | 2.00 (1.46, 2.74) | <0.001 | 2.35 (1.51, 3.65) | <0.001 | 1.65 (1.05, 2.60) | <0.001 |
| 2 | 3.21 (2.34, 4.40) | <0.001 | 3.78 (2.43, 5.87) | <0.001 | 2.64 (1.68, 4.16) | <0.05 |
| 3 | 3.90 (2.79, 5.45) | <0.001 | 4.61 (2.90, 7.35) | <0.001 | 3.20 (1.97, 5.17) | <0.001 |
| Daily sugar-sweetened beverage consumption | ||||||
| No | 1.0 | 1.0 | 1.0 | |||
| Yes | 1.56 (1.46, 1.65) | <0.001 | 1.55 (1.42, 1.69) | <0.001 | 1.55 (1.41, 1.70) | <0.001 |
| Child’s bedtime | ||||||
| Before 9 p.m. | 1.0 | 1.0 | 1.0 | |||
| 9~11 p.m. | 1.33 (1.23, 1.45) | <0.001 | 1.33 (1.19, 1.49) | <0.001 | 1.34 (1.18, 1.51) | <0.001 |
| After 11 p.m. | 1.85 (1.61, 2.12) | <0.001 | 1.59 (1.30, 1.93) | <0.001 | 2.13 (1.75, 2.58) | <0.001 |
| Irregular | 1.71 (1.51, 1.93) | <0.001 | 1.74 (1.47, 2.06) | <0.001 | 1.67 (1.39, 2.01) | <0.001 |
| Daily toothbrushing by parents | ||||||
| Yes | 1.0 | 1.0 | 1.0 | |||
| No | 1.32 (1.24, 1.41) | <0.001 | 1.30 (1.19, 1.42) | <0.001 | 1.35 (1.23, 1.49) | <0.001 |
| Varnish of fluoride | ||||||
| Yes | 1.0 | 1.0 | 1.0 | |||
| No | 1.49 (1.37, 1.62) | <0.001 | 1.53 (1.37, 1.72) | <0.001 | 1.44 (1.27, 1.63) | <0.001 |
| Smoking of family members | ||||||
| No | 1.0 | 1.0 | 1.0 | |||
| Yes | 1.43 (1.34, 1.52) | <0.001 | 1.41 (1.29, 1.54) | <0.001 | 1.45 (1.32, 1.59) | <0.001 |
3.5. Late Bedtime Contributes to the Development of Dental Caries
3.6. Daily Tooth Brushing Decreased Dental Caries in Children
3.7. Fluoride Varnish
3.8. Household Smoking Is a Risk Factor for Development of Early Childhood Caries
3.9. Main Strengths and Limitations of the Study
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Do, L.G. Distribution of caries in children: Variations between and within populations. J. Dent. Res. 2012, 91, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Burt, B.A.; Eklund, S.A.; Morgan, K.J.; Larkin, F.E.; Guire, K.E.; Brown, L.O.; Weintraub, J.A. The effects of sugars intake and frequency of investigation on dental caries increment in a three-year longitudinal study. J. Dent. Res. 1998, 67, 1422–1429. [Google Scholar] [CrossRef]
- Burt, B.A.; Pai, S. Sugar consumption and caries risk: A systematic review. J. Dent. Educ. 2001, 65, 1017–1023. [Google Scholar] [PubMed]
- Johansson, I.; Holgerson, P.L.; Kressin, N.R.; Nunn, M.E.; Tanner, A.C. Snacking habits and caries in young children. Caries Res. 2010, 44, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Tahmassebi, J.F.; Duggal, M.S.; Malik-Kotru, G.; Curzon, M.E. Soft drinks and dental health: A review of the current literature. J. Dent. 2006, 34, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Armfield, J.M.; Spencer, A.J.; Roberts-Thomson, K.F.; Plastow, K. Water fluoridation and the association of sugar-sweetened beverage consumption and dental caries in Australian children. Am. J. Public Health 2013, 103, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Hanioka, T.; Ojima, M.; Tanaka, K.; Yamamoto, M. Does secondhand smoke affect the development of dental caries in children? A systematic review. Int. J. Environ. Res. Public Health 2011, 8, 1503–1519. [Google Scholar] [CrossRef] [PubMed]
- Leroy, R.; Hoppenbrouwers, K.; Jara, A.; Declerck, D. Parental smoking behavior and caries experience in preschool children. Community Dent. Oral Epidemiol. 2008, 36, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Hanioka, T.; Nakamura, E.; Ojima, M.; Tanaka, K.; Aoyama, H. Dental caries in 3-year-old children and smoking status of parents. Pediatr. Perinat. Epidemiol. 2008, 22, 546–550. [Google Scholar] [CrossRef]
- Tanaka, K.; Miyake, Y.; Arakawa, M.; Sasaki, S.; Ohya, Y. Household smoking and dental caries in school children: the Ryukyus Child Health Study. BMC Public Health. 2010, 10. [Google Scholar] [CrossRef] [PubMed]
- Valatis, R.; Hesch, R.; Passarelli, C.; Sheehan, D.; Sinton, J. A systematic review of the relationship between breastfeeding and early childhood caries. Can. J. Public Health 2000, 91, 411–417. [Google Scholar] [PubMed]
- Ribeiro, N.M.; Ribeiro, M.A. Breastfeeding and early childhood caries: A critical review. J. Pediatr. (Rio. J.) 2004, 80, S199–S210. [Google Scholar] [CrossRef]
- Yonezu, T.; Ushida, N.; Yakushiji, M. Longitudinal study of prolonged breast-or bottle-feeding on dental caries in Japanese children. Bull. Tokyo Dent. Coll. 2006, 47, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Qin, M.; Li, J.; Zhang, S.; Ma, W. Risk factor for severe early childhood caries in children younger than 4 years old in Beijing, China. Pediatr. Dent. 2008, 30, 122–128. [Google Scholar] [PubMed]
- Mohebbi, S.Z.; Virtanen, J.I.; Vhid-Golpayegami, M.; Vehkalahti, M.M. Feeding habits as determinants of early childhood caries in a population where prolonged breastfeeding is the norm. Community Dent. Oral Epidemiol. 2008, 36, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Mizoguchi, K.; Kurumado, K.; Tango, T.; Minowa, M. Study on factors for caries and infant feeding characteristics in children aged 1.5–3 years in a Kanto urban area. Nihon Koshu Eisei Zasshi. 2003, 50, 867–878. (In Japanese) [Google Scholar] [PubMed]
- National Institute of Public Health. The Results of Dental Health Examination in Japanese Infants. Available online: http://www.niph.go.jp/soshiki/koku/oralhealth/infantcaries.html (accessed on 20 September 2014).
- Rodis, O.M.M.; Li, Y.; Matsumura, S.; Shimono, T.; Okazaki, Y. Comparison of plaque samples and saliva samples using the CAT21 Test® (Cariostat method). Pediatr. Dent. J. 2005, 15, 6–9. [Google Scholar] [CrossRef]
- Nishimura, M. The relationship between a caries activity test (Cariostat) and plate colony counts of mutans streptococci in human dental plaque. Pediatr. Dent. J. 1994, 4, 23–27. [Google Scholar]
- Iida, H.; Auinger, P.; Billings, R.J.; Weitzman, M. Association between infant breastfeeding and early childhood caries in the United States. Pediatrics 2007, 120, e944–e952. [Google Scholar] [CrossRef] [PubMed]
- Mattila, M.L.; Rautava, P.; Paunio, P.; Ojanlatva, A.; Hyssälä, L.; Helenius, H.; Sillanpää, M. Caries experience and caries increments at 10 years of age. Caries Res. 2001, 35, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Lingstrom, P.; van Houte, J.; Kashket, S. Food starches and dental caries. Crit. Rev. Oral Biol. Med. 2000, 11, 366–380. [Google Scholar] [CrossRef] [PubMed]
- Firestone, A.R.; Schmid, R.; Muhlemann, H.R. Cariogenic effects of cooked wheat starch alone or with sucrose and frequency-controlled feeding in rats. Arch. Oral Biol. 1982, 27, 759–763. [Google Scholar] [CrossRef] [PubMed]
- Bellini, H.T.; Arnberg, P.; von der Fehr, F.R. Oral hygiene and caries. A review. Acta. Odontol. Scand. 1981, 39, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Fogels, H.R.; Cancro, L.P.; Bianco, J.; Fischman, S.L. The anticaries effect of supervised tooth brushing with a nonfluoride dentifrice. ASDC J. Dent. Child. 1982, 49, 424–427. [Google Scholar] [PubMed]
- Andlaw, R.J. Oral hygiene and dental caries—A review. Int. Dent. J. 1978, 28, 1–6. [Google Scholar] [PubMed]
- De Bruyn, H.; Arends, J. Fluoride varnishes—A review. J. Biol. Buccale 1987, 15, 71–82. [Google Scholar] [PubMed]
- Twetman, S.; Petersson, L.G.; Pakhomov, G.N. Caries incidence in relation to salivary mutans streptococci and fluoride varnish applications in preschool children from low- and optimal-fluoride areas. Caries Res. 1996, 30, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Seppä, L. Fluoride varnishes in caries prevention. Med. Princ. Pract. 2004, 13, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Recommendations for using fluoride to prevent and control dental caries in the United States. MMWR Recomm. Rep. 2001, 50, 1–42. [Google Scholar]
- Rosen, S.; Frea, J.I.; Hsu, S.M. Effect of fluoride-resistant microorganisms on dental caries. J. Dent. Res. 1978, 57. [Google Scholar] [CrossRef]
- Marquis, R.E. Diminished acid tolerance of plaque bacteria caused by fluoride. J. Dent. Res. 1990, 69, 672–675. [Google Scholar] [PubMed]
- Lindemeyer, R.G.; Baum, R.H.; Hsu, S.C.; Going, R.E. In vitro effect of tobacco on the growth of oral cariogenic streptococci. J. Am. Dent. Assoc. 1981, 103, 719–722. [Google Scholar] [PubMed]
- Kohler, B.; Andreen, I.; Jonsson, B. The earlier the colonization by mutans streptococci, the higher the caries prevalence at 4 years of age. Oral Microbiol. Immunol. 1988, 3, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Costa, S.M.; Vasconcelos, M.; Abreu, M.H. High dental caries among adults aged 35 to 44 years: Case-control study of distal and proximal factors. Int. J. Environ. Res. Public Health 2013, 10, 2401–2411. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, K.; Miyake, Y.; Sasaki, S.; Hirota, Y. Socioeconomic status and risk of dental caries in Japanese preschool children: The Osaka Maternal and child health study. J. Public Health Dent. 2013, 73, 217–223. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watanabe, M.; Wang, D.-H.; Ijichi, A.; Shirai, C.; Zou, Y.; Kubo, M.; Takemoto, K.; Masatomi, C.; Ogino, K. The Influence of Lifestyle on the Incidence of Dental Caries among 3-Year-Old Japanese Children. Int. J. Environ. Res. Public Health 2014, 11, 12611-12622. https://doi.org/10.3390/ijerph111212611
Watanabe M, Wang D-H, Ijichi A, Shirai C, Zou Y, Kubo M, Takemoto K, Masatomi C, Ogino K. The Influence of Lifestyle on the Incidence of Dental Caries among 3-Year-Old Japanese Children. International Journal of Environmental Research and Public Health. 2014; 11(12):12611-12622. https://doi.org/10.3390/ijerph111212611
Chicago/Turabian StyleWatanabe, Masako, Da-Hong Wang, Akihiro Ijichi, Chika Shirai, Yu Zou, Masayuki Kubo, Kei Takemoto, Chie Masatomi, and Keiki Ogino. 2014. "The Influence of Lifestyle on the Incidence of Dental Caries among 3-Year-Old Japanese Children" International Journal of Environmental Research and Public Health 11, no. 12: 12611-12622. https://doi.org/10.3390/ijerph111212611
APA StyleWatanabe, M., Wang, D.-H., Ijichi, A., Shirai, C., Zou, Y., Kubo, M., Takemoto, K., Masatomi, C., & Ogino, K. (2014). The Influence of Lifestyle on the Incidence of Dental Caries among 3-Year-Old Japanese Children. International Journal of Environmental Research and Public Health, 11(12), 12611-12622. https://doi.org/10.3390/ijerph111212611