
Comparative Analysis of Corneal Morphological and Optical Parameters in Predicting DSAEK Surgery Outcome

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| EK | Endothelial Keratoplasty |
| FECD | Fuchs Endothelial Corneal Dystrophy |
| BK | Bullous Keratopathy |
| PKP | Penetrating Keratoplasty |
| DSAEK | Descemet Stripping Automated Endothelial Keratoplasty |
| IOL | Intraocular Lens |
| HOAs | Higher-Order Aberrations |
| DMEK | Descemet’s Membrane Endothelial Keratoplasty |
| UT-DSAEK | Ultrathin Descemet Stripping Automated Endothelial Keratoplasty |
| CD | Corneal Densitometry |
| AS-OCT | Anterior Segment Optical Coherence Tomography |
| BCVA | Best-Corrected Visual Acuity |
| PBK | Pseudophakic Bullous Keratopathy |
| GSU | Grayscale Unit |
| RMS | Root-Mean-Square |
| logMAR | Logarithm of the Minimum Angle of Resolution |
| CI | Confidence Interval |
| Rho | Spearman’s Rank Correlation Coefficient |
References
- Giglio, R.; Vinciguerra, A.L.; Grotto, A.; Milan, S.; Tognetto, D. Hitting the refractive target in corneal endothelial transplantation triple procedures: A systematic review. Surv. Ophthalmol. 2024, 69, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Yamagami, S.; Hayashi, T. The progress and future of corneal endothelial transplantation. Jpn. J. Ophthalmol. 2024, 68, 429–442. [Google Scholar] [CrossRef]
- Machalińska, A.; Kuligowska, A.; Kowalska, B.; Safranow, K. Comparative Analysis of Corneal Parameters in Swept-Source Imaging between DMEK and UT-DSAEK Eyes. J. Clin. Med. 2021, 10, 5119. [Google Scholar] [CrossRef]
- Tourabaly, M.; Knoeri, J.; Georgeon, C.; Borderie, V. Review of the Literature: Surgery Indications for Fuchs’ Endothelial Corneal Dystrophy. J. Clin. Med. 2025, 14, 2365. [Google Scholar] [CrossRef] [PubMed]
- Bahar, I.; Kaiserman, I.; Levinger, E.; Sansanayudh, W.; Slomovic, A.R.; Rootman, D.S. Retrospective contralateral study comparing descemet stripping automated endothelial keratoplasty with penetrating keratoplasty. Cornea 2009, 28, 485–488. [Google Scholar] [CrossRef]
- Melles, G.R.; Lander, F.; Rietveld, F.J. Transplantation of Descemet’s membrane carrying viable endothelium through a small scleral incision. Cornea 2002, 21, 415–418. [Google Scholar] [CrossRef]
- Terry, M.A. Endothelial keratoplasty: Why aren’t we all doing Descemet membrane endothelial keratoplasty? Cornea 2012, 31, 469–471. [Google Scholar] [CrossRef]
- Price, M.O.; Giebel, A.W.; Fairchild, K.M.; Price, F.W., Jr. Descemet’s membrane endothelial keratoplasty: Prospective multicenter study of visual and refractive outcomes and endothelial survival. Ophthalmology 2009, 116, 2361–2368. [Google Scholar] [CrossRef] [PubMed]
- Guerra, F.P.; Anshu, A.; Price, M.O.; Giebel, A.W.; Price, F.W. Descemet’s membrane endothelial keratoplasty: Prospective study of 1-year visual outcomes, graft survival, and endothelial cell loss. Ophthalmology 2011, 118, 2368–2373. [Google Scholar] [CrossRef]
- Ballesteros-Sánchez, A.; Peraza-Nieves, J.; Casablanca-Piñera, A.; Rodríguez-Calvo-De-Mora, M.; Catalán-Coronado, S.; Torras-Sanvicens, J.; Borroni, D.; Sánchez-González, J.M.; Rocha-De-Lossada, C. Scheimpflug Corneal Densitometry Patterns at the Graft-Host Interface in DMEK and DSAEK: A 12-Month Longitudinal Comparative Study. J. Clin. Med. 2023, 12, 7133. [Google Scholar] [CrossRef]
- Chamberlain, W.; Austin, A.; Terry, M.; Jeng, B.H.; Rose-Nussbaumer, J. Survey of Experts on Current Endothelial Keratoplasty Techniques. J. Clin. Exp. Ophthalmol. 2016, 7, 608. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Terry, M.A.; Shamie, N.; Chen, E.S.; Phillips, P.M.; Hoar, K.L.; Friend, D.J. Precut tissue for Descemet’s stripping automated endothelial keratoplasty: Vision, astigmatism, and endothelial survival. Ophthalmology 2009, 116, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Neokleous, A.; Michail, N.; Herodotou, F.; Athanasiadou, A.; Christodoulou, S.; Kola, D.; Panayidou, K.; Hadjilouka, G.; Palioura, S. Long-Term Monitoring of Corneal Grafts Via Anterior Segment OCT Pachymetry Maps. Ophthalmol. Sci. 2025, 5, 100724. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ivarsen, A.; Hjortdal, J. Recipient corneal thickness and visual outcome after Descemet’s stripping automated endothelial keratoplasty. Br. J. Ophthalmol. 2014, 98, 30–34. [Google Scholar] [CrossRef]
- Phillips, P.M.; Phillips, L.J.; Maloney, C.M. Preoperative graft thickness measurements do not influence final BSCVA or speed of vision recovery after descemet stripping automated endothelial keratoplasty. Cornea 2013, 32, 1423–1427. [Google Scholar] [CrossRef]
- Lin, C.C.; Chamberlain, W.D.; Kakigi, C.; Arnold, B.F.; Rose-Nussbaumer, J. Mediators of Visual Acuity in Descemet Membrane Endothelial Keratoplasty and Ultrathin Descemet Stripping Automated Endothelial Keratoplasty. Cornea 2024, 43, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Shilova, N.F.; Anisimova, N.S.; Antonova, O.P.; Anisimov, S.I.; Malyugin, B.E. Comparative study of corneal densitometry values after posterior lamellar keratoplasty. Vestn. Oftalmol. 2020, 136, 25–31. [Google Scholar] [CrossRef]
- Hirabayashi, K.E.; Chamberlain, W.; Rose-Nussbaumer, J.; Austin, A.; Stell, L.; Lin, C.C. Corneal Light Scatter After Ultrathin Descemet Stripping Automated Endothelial Keratoplasty Versus Descemet Membrane Endothelial Keratoplasty in Descemet Endothelial Thickness Comparison Trial: A Randomized Controlled Trial. Cornea 2020, 39, 691–696. [Google Scholar] [CrossRef]
- Arora, R.; Gupta, P.; Sahu, J.; Jain, P.; Vishwanath, S.; Shroff, R. Analysis of Corneal Scheimpflug Densitometry and Ocular Wavefront Aberrations Post Descemet Stripping Automated Endothelial Keratoplasty. Eye Contact Lens. 2022, 48, 242–249. [Google Scholar] [CrossRef]
- Dhubhghaill, S.N.; Rozema, J.J.; Jongenelen, S.; Ruiz Hidalgo, I.; Zakaria, N.; Tassignon, M.-J. Normative Values for Corneal Densitometry Analysis by Scheimpflug Optical Assessment. Investig. Ophthalmol. Vis. Sci. 2014, 55, 162–168. [Google Scholar]
- EQUATOR Network. Available online: https://www.equator-network.org/ (accessed on 3 March 2025).
- Armitage, P.; Perry, G. Statistical Methods in Medical Research; Wiley-Blackwell: Oxford, UK, 2001. [Google Scholar]
- Busin, M.; Madi, S.; Santorum, P.; Scorcia, V.; Beltz, J. Ultrathin descemet’s stripping automated endothelial keratoplasty with the microkeratome double-pass technique: Two-year outcomes. Ophthalmology 2013, 120, 1186–1194. [Google Scholar] [CrossRef] [PubMed]
- Busin, M.; Albé, E. Does thickness matter: Ultrathin Descemet stripping automated endothelial keratoplasty. Curr. Opin. Ophthalmol. 2014, 25, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Muftuoglu, O.; Prasher, P.; Bowman, R.W.; McCulley, J.P.; Mootha, V.V. Corneal higher-order aberrations after Descemet’s stripping automated endothelial keratoplasty. Ophthalmology 2010, 117, 878–884. [Google Scholar] [CrossRef]
- Alqudah, A.A.; Bauer, A.J.; Straiko, M.D.; Sanchez, P.J.; Terry, M.A. Descemet Stripping Automated Endothelial Keratoplasty: The influence of preoperative endothelial cell density and triple procedures on grafts at 5 years postoperative. Medicine 2020, 99, e23139. [Google Scholar] [CrossRef] [PubMed]
- Heinzelmann, S.; Böhringer, D.; Maier, P.C.; Reinhard, T. Correlation between visual acuity and interface reflectivity measured by Pentacam following DSAEK. Acta Ophthalmol. 2014, 92, e1–e4. [Google Scholar] [CrossRef]
- Nielsen, E.; Ivarsen, A.; Kristensen, S.; Hjortdal, J. Fuchs’ endothelial corneal dystrophy: A controlled prospective study on visual recovery. Acta Ophthalmol. 2016, 94, 780–787. [Google Scholar] [CrossRef]
- Koh, S.; Maeda, N.; Nakagawa, T.; Nishida, K. Quality of vision in eyes after selective lamellar keratoplasty. Cornea 2012, 31 (Suppl. 1), S45–S49. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Male recipient [n (%)] | 6/17 (35%) |
| Female recipient [n (%)] | 11/17 (65%) |
| Male donor [n (%)] | 8/17 (47%) |
| Female donor [n (%)] | 9/17 (53%) |
| Recipient age [years, median (IQR)] | 66 (62–74) |
| Donor age [years, median (IQR)] | 64 (58–69) |
| Right operated eye [n (%)] | 9/17 (53%) |
| Left operated eye [n (%)] | 8/17 (47%) |
| Time from surgery to follow-up [months, median (IQR)] | 11 (9–15) |
| Follow-up 3–6 months after surgery [n (%)] | 3/17 (18%) |
| Follow-up 8–9 months aftersurgery [n (%)] | 3/17 (18%) |
| Follow-up 10–11 months after surgery [n (%)] | 3/17 (18%) |
| Follow-up 12–15 months after surgery [n (%)] | 5/17 (28%) |
| Follow-up > 2 years after surgery [n (%)] | 3/17 (18%) |
| FECD [n (%)] | 10/17 (59%) |
| PBK [n (%)] | 7/17 (41%) |
| DSAEK [n (%)] | 10/17 (59%) |
| Triple DSAEK [n (%)] | 7/17 (41%) |
| Visual Acuity Measure | Preoperative Median (IQR) | Postoperative Median (IQR) | Difference | 95% CI | p * |
|---|---|---|---|---|---|
| Snellen | 0.10 (0.04–0.23) | 0.50 (0.30–0.63) | 0.33 | 0.25 to 0.43 | <0.001 |
| logMAR | 1.0 (0.66–1.4) | 0.30 (0.21–0.52) | −0.64 | −0.90 to −0.44 | <0.001 |
| Median (IQR) by Follow-Up Time | 3–6 Months | 8–9 Months | 10–11 Months | 12–15 Months | >2 Years | p Value * |
|---|---|---|---|---|---|---|
| Postoperative visual acuity (Snellen) | 0.40 (0.33–0.48) | 0.30 (0.23–0.53) | 0.90 (0.60–0.98) | 0.40 (0.30–0.63) | 0.50 (0.43–0.80) | 0.22 |
| Postoperative visual acuity (logMAR) | 0.40 (0.33–0.49) | 0.52 (0.30–0.66) | 0.05 (0.01–0.24) | 0.40 (0.20–0.52) | 0.30 (0.11–0.38) | 0.22 |
| Parameter | Median (Interquartile Range) | Minimum–Maximum |
|---|---|---|
| Total corneal thickness on AS-OCT [µm]—postoperative | 578 (526–617.5) | 486–696 |
| Total corneal thickness on Pentacam [µm]—postoperative | 557 (512.5–598) | 473–676 |
| Graft thickness on AS-OCT [µm]—postoperative | 95 (80–106) | 62–129 |
| Parameter | logMAR BCVA (Rho, p) | Time Since Surgery (Rho, p) |
|---|---|---|
| Recipient age | 0.654 (<0.001) | −0.417 (0.10) |
| Donor age | 0.060 (0.82) | −0.246 (0.34) |
| Postoperative graft thickness (AS-OCT) | 0.051 (0.85) | 0.188 (0.47) |
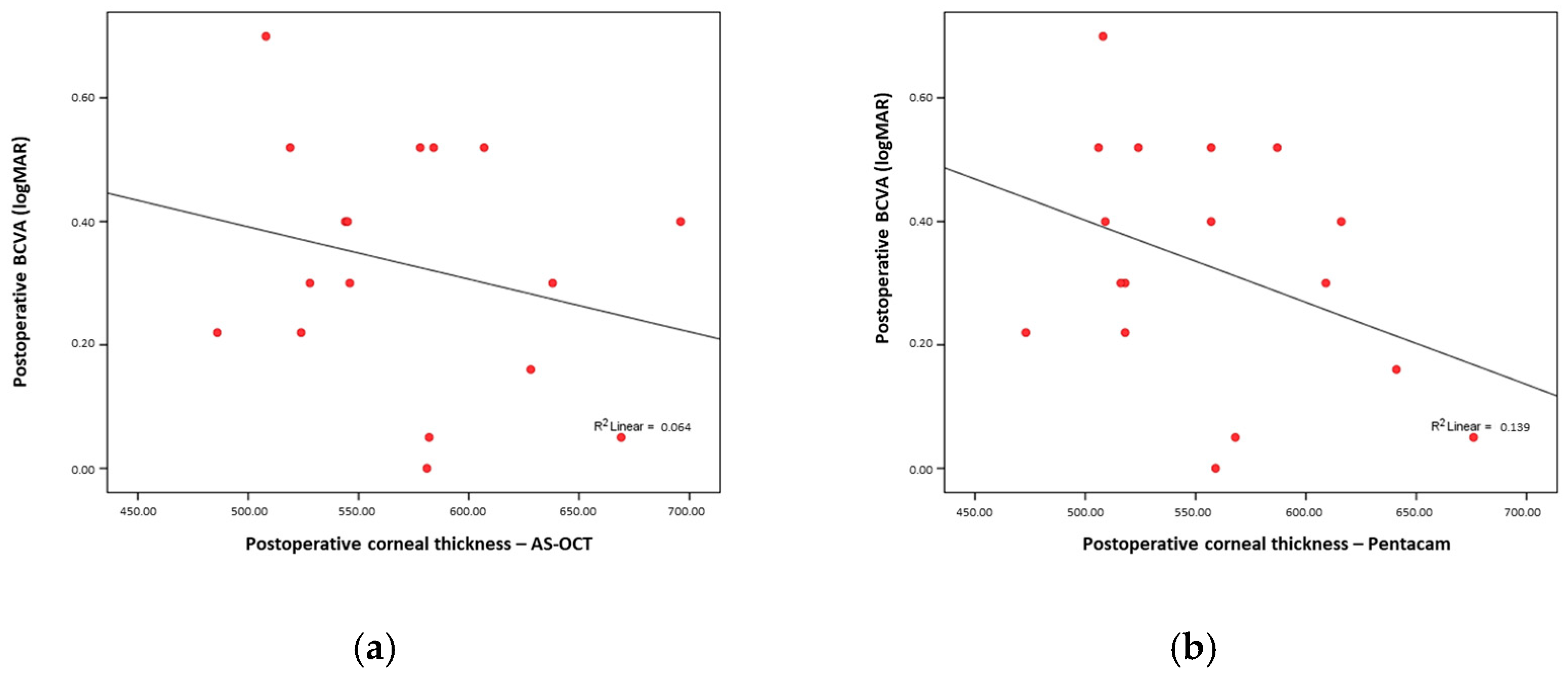
| Postoperative total corneal thickness (AS-OCT) | −0.227 (0.38) | 0.156 (0.55) |
| Postoperative total corneal thickness (Pentacam) | −0.369 (0.14) | 0.085 (0.75) |
| CD total | 0.551 (0.02) | −0.119 (0.65) |
| CD anterior total | 0.418 (0.10) | 0.039 (0.88) |
| CD central total | 0.556 (0.02) | −0.208 (0.42) |
| CD posterior total | 0.584 (0.01) | −0.132 (0.61) |
| CD 0–2 mm total | 0.660 (<0.001) | −0.072 (0.78) |
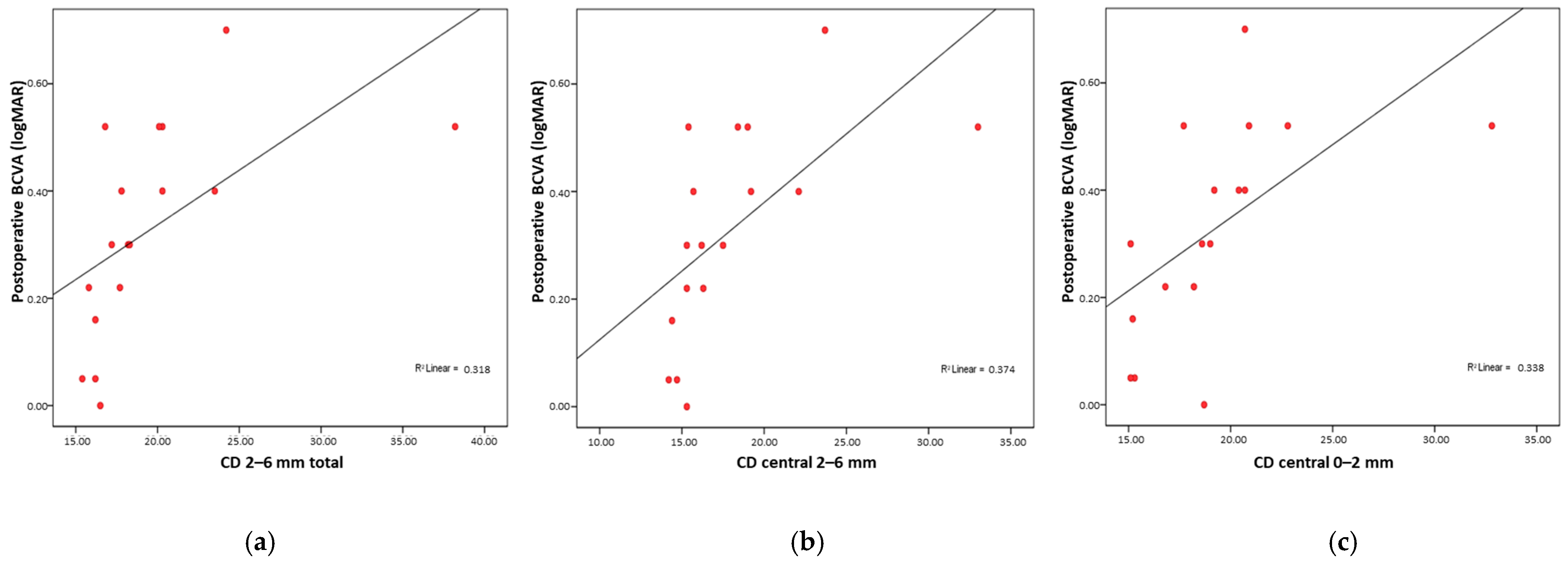
| CD 2–6 mm total | 0.795 (<0.001) | −0.192 (0.46) |
| CD 6–10 mm total | 0.649 (<0.001) | −0.215 (0.41) |
| CD 10–12 mm total | −0.117 (0.65) | −0.072 (0.78) |
| CD anterior 0–2 mm | 0.333 (0.19) | 0.474 (0.05) |
| CD anterior 2–6 mm | 0.590 (0.01) | 0.301 (0.24) |
| CD anterior 6–10 mm | 0.677 (<0.001) | −0.215 (0.41) |
| CD anterior 10–12 mm | −0.148 (0.57) | −0.036 (0.89) |
| CD central 0–2 mm | 0.730 (<0.001) | −0.024 (0.93) |
| CD central 2–6 mm | 0.791 (<0.001) | −0.286 (0.27) |
| CD central 6–10 mm | 0.654 (<0.001) | −0.289 (0.26) |
| CD central 10–12 mm | −0.027 (0.92) | −0.162 (0.53) |
| CD posterior 0–2 mm | 0.644 (0.01) | −0.256 (0.32) |
| CD posterior 2–6 mm | 0.613 (0.01) | −0.332 (0.19) |
| CD posterior 6–10 mm | 0.590 (0.01) | 0.027 (0.92) |
| CD posterior 10–12 mm | −0.065 (0.80) | 0.002 (0.99) |
| HOA total | 0.171 (0.51) | 0.073 (0.78) |
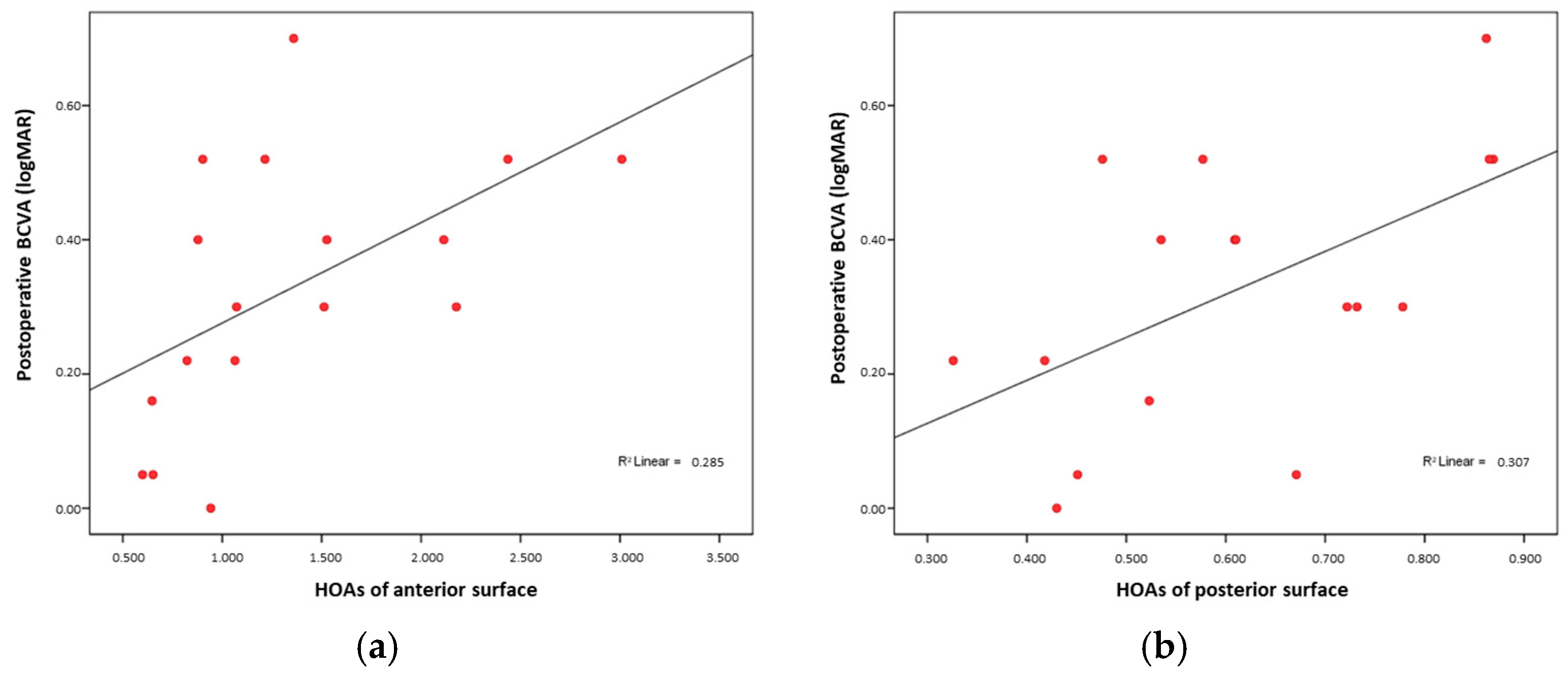
| HOA anterior | 0.624 (0.01) | −0.043 (0.87) |
| HOA posterior | 0.556 (0.02) | 0.064 (0.81) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geber, A.; Masnec, S.; Kalauz, M.; Bešlić, I.; Škegro, I.; Gaćina, D.L.; Jandroković, S.; Meter, A.; Kuzman, T. Comparative Analysis of Corneal Morphological and Optical Parameters in Predicting DSAEK Surgery Outcome. Medicina 2025, 61, 1022. https://doi.org/10.3390/medicina61061022
Geber A, Masnec S, Kalauz M, Bešlić I, Škegro I, Gaćina DL, Jandroković S, Meter A, Kuzman T. Comparative Analysis of Corneal Morphological and Optical Parameters in Predicting DSAEK Surgery Outcome. Medicina. 2025; 61(6):1022. https://doi.org/10.3390/medicina61061022
Chicago/Turabian StyleGeber, Antonela, Sanja Masnec, Miro Kalauz, Iva Bešlić, Ivan Škegro, Dina Lešin Gaćina, Sonja Jandroković, Ana Meter, and Tomislav Kuzman. 2025. "Comparative Analysis of Corneal Morphological and Optical Parameters in Predicting DSAEK Surgery Outcome" Medicina 61, no. 6: 1022. https://doi.org/10.3390/medicina61061022
APA StyleGeber, A., Masnec, S., Kalauz, M., Bešlić, I., Škegro, I., Gaćina, D. L., Jandroković, S., Meter, A., & Kuzman, T. (2025). Comparative Analysis of Corneal Morphological and Optical Parameters in Predicting DSAEK Surgery Outcome. Medicina, 61(6), 1022. https://doi.org/10.3390/medicina61061022