
Immune Modulation Through Stereotactic Radiotherapy: The Role of TBX21, GATA-3, FoxP3, and RORɣt


Abstract
1. Introduction
2. Materials and Methods
2.1. Treatment Protocols
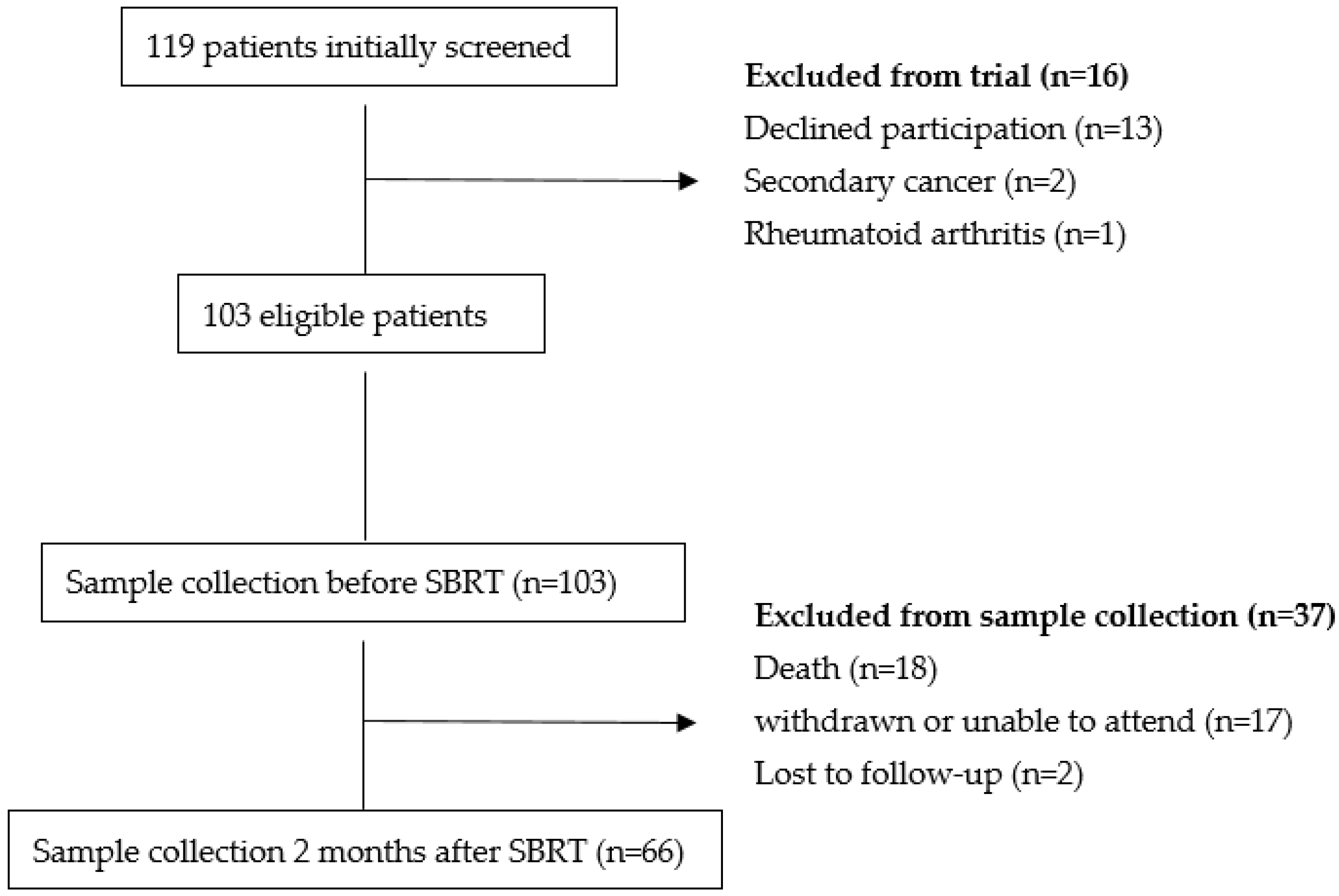
2.2. Study Flow
2.3. Serum Transcription Factor Measurements
2.4. Statistics
3. Results
3.1. Patient Characteristics
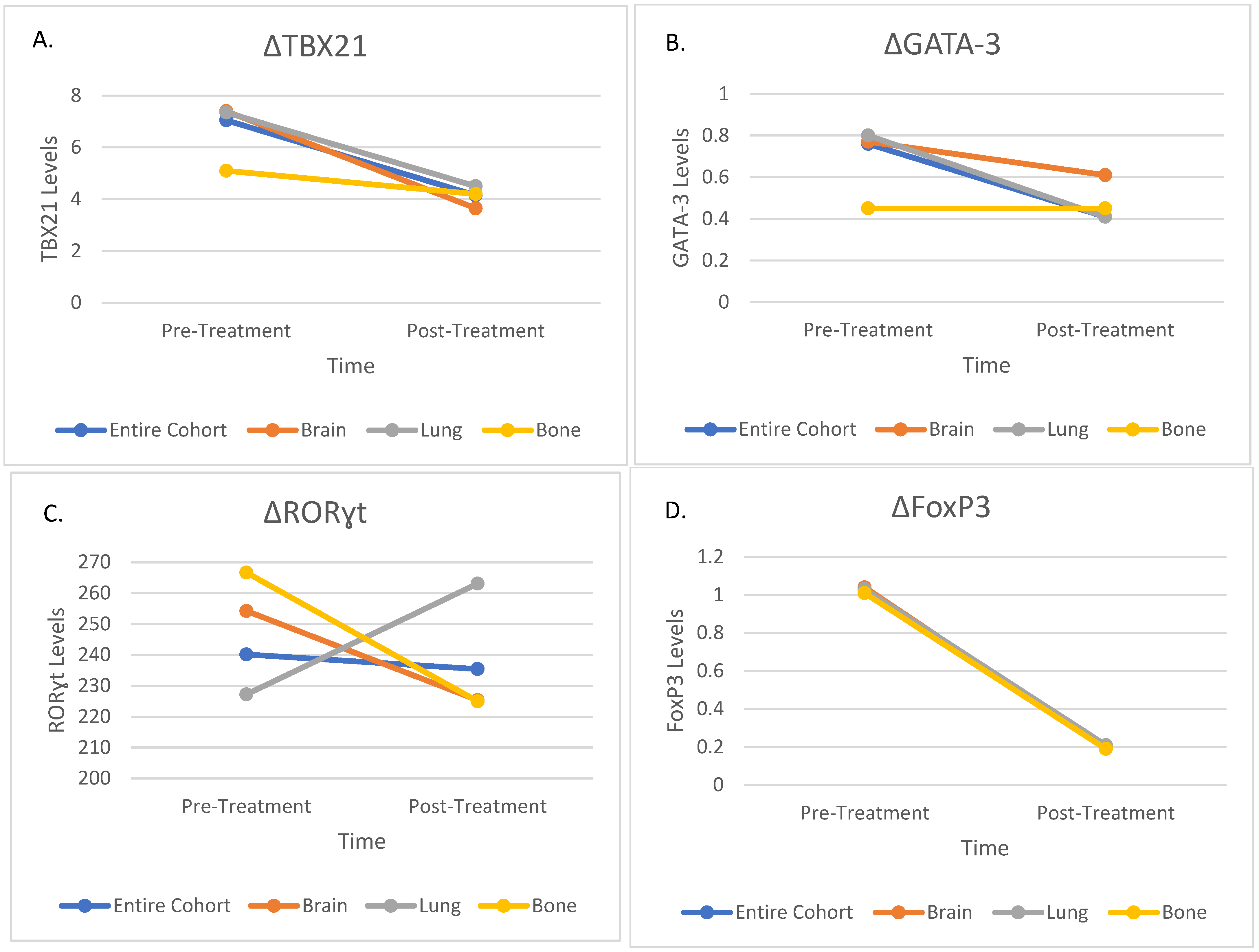
3.2. Changes in Transcription Factors
3.3. Subgroup Analyses by Treatment Region
3.4. Correlation Between Transcription Factors and Clinicopathological Parameters
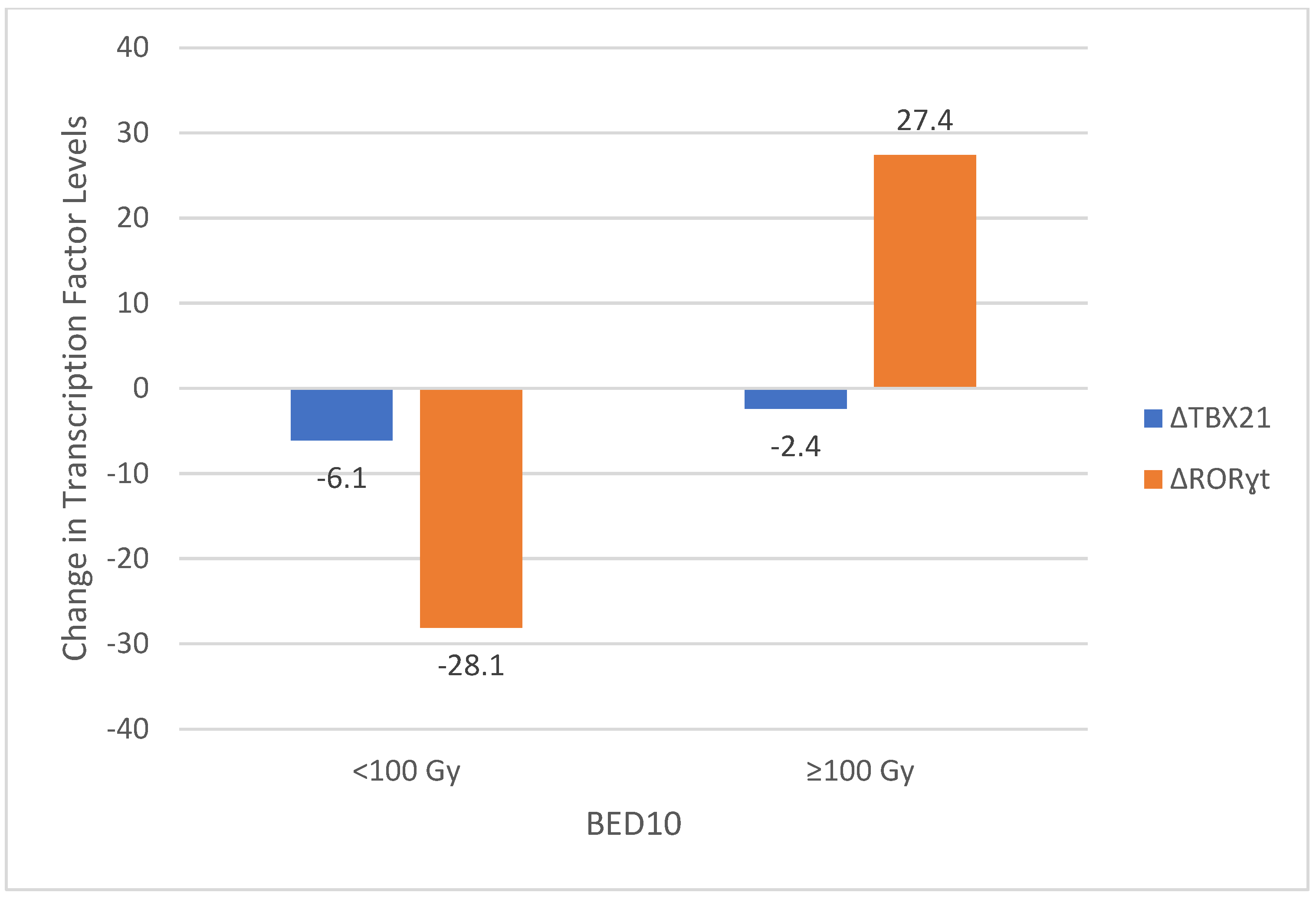
3.5. Correlation Between Transcription Factors and Dosimetric Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benedict, S.H.; Yenice, K.M.; Followill, D.; Galvin, J.M.; Hinson, W.; Kavanagh, B.; Keall, P.; Lovelock, M.; Meeks, S.; Papiez, L.; et al. Stereotactic body radiation therapy: The report of AAPM Task Group 101. Med. Phys. 2010, 37, 4078–4101. [Google Scholar] [CrossRef] [PubMed]
- Potters, L.; Steinberg, M.; Rose, C.; Timmerman, R.; Ryu, S.; Hevezi, J.M.; Welsh, J.; Mehta, M.; Larson, D.A.; Janjan, N.A. American Society for Therapeutic Radiology and Oncology and American College of Radiology practice guideline for the performance of stereotactic body radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 1026–1032. [Google Scholar] [CrossRef]
- Troost, E.G.C. Die stereotaktische Strahlentherapie unterstützt die Immunantwort. Strahlenther. Onkol. 2016, 192, 70–71. [Google Scholar] [CrossRef]
- Mole, R.H. Whole body irradiation; radiobiology or medicine? Br. J. Radiol. 1953, 26, 234–241. [Google Scholar] [CrossRef]
- Zhu, J.; Paul, W.E. Peripheral CD4+ T-cell differentiation regulated by networks of cytokines and transcription factors. Immunol. Rev. 2010, 238, 247–262. [Google Scholar] [CrossRef]
- Stanton, S.E.; Disis, M.L. Clinical significance of tumor-infiltrating lymphocytes in breast cancer. J. Immunother. Cancer 2016, 4, 59. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Yoshikawa, K.; Suzuki, S.; Gosho, M.; Ueda, R.; Kazaoka, Y. Tumor-infiltrating FoxP3+ T cells are associated with poor prognosis in oral squamous cell carcinoma. Clin. Exp. Dent. Res. 2022, 8, 152–159. [Google Scholar] [CrossRef]
- Cunha, L.L.; Morari, E.C.; Nonogaki, S.; Bufalo, N.E.; da Assumpção, L.V.M.; Soares, F.A.; Vassallo, J.; Ward, L.S. RORγt may Influence the Microenvironment of Thyroid Cancer Predicting Favorable Prognosis. Sci. Rep. 2020, 10, 4142. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Shen, W.; Yu, J.; Wang, L. TBX21 predicts prognosis of patients and drives cancer stem cell maintenance via the TBX21-IL-4 pathway in lung adenocarcinoma. Stem Cell Res. Ther. 2018, 9, 89. [Google Scholar] [CrossRef]
- Gkika, E.; Firat, E.; Adebahr, S.; Graf, E.; Popp, I.; Radicioni, G.; Lo, S.S.; Nestle, U.; Nicolay, N.H.; Niedermann, G.; et al. Systemic immune modulation by stereotactic radiotherapy in early-stage lung cancer. NPJ Precis. Oncol. 2023, 7, 24. [Google Scholar] [CrossRef]
- Novikov, S.N.; Baldueva, I.A.; Zozulya, A.Y.; Emelyanova, N.V.; Girdyuk, D.V.; Arsenyev, A.I.; Alexandrovna, E.; Tyuryaeva, E.I.; Antipov, E.; Girshovich, M.M.; et al. Peripheral blood lymphocyte changes after stereotactic ablative body radiotherapy to lung or liver metastases in patients with oligometastatic cancers. Radiat. Oncol. J. 2023, 41, 23–31. [Google Scholar] [CrossRef]
- van der Woude, L.L.; Gorris, M.A.J.; Wortel, I.M.N.; Creemers, J.H.A.; Verrijp, K.; Monkhorst, K.; Grünberg, K.; van den Heuvel, M.M.; Textor, J.; Figdor, C.G.; et al. Tumor microenvironment shows an immunological abscopal effect in patients with NSCLC treated with pembrolizumab-radiotherapy combination. J. Immunother. Cancer 2022, 10, e005248. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Martín, A.; Galiana, I.L.; Berenguer Frances, M.A.; Cacicedo, J.; Cañas Cortés, R.; Comas Anton, S.; Padrones Sánchez, S.; Bolívar Cuevas, S.; Parry, R.; Guedea Edo, F. Preliminary Study of the Effect of Stereotactic Body Radiotherapy (SBRT) on the Immune System in Lung Cancer Patients Unfit for Surgery: Immunophenotyping Analysis. Int. J. Mol. Sci. 2018, 19, 3963. [Google Scholar] [CrossRef]
- Rutkowski, J.; Ślebioda, T.; Kmieć, Z.; Zaucha, R. Changes in systemic immune response after stereotactic ablative radiotherapy; Preliminary results of a prospective study in patients with early lung cancer. Pol. Arch. Intern. Med. 2017, 127, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Bezjak, A.; Paulus, R.; Gaspar, L.E.; Timmerman, R.D.; Straube, W.L.; Ryan, W.F.; Garces, Y.I.; Pu, A.T.; Singh, A.K.; Videtic, G.M.; et al. Safety and Efficacy of a Five-Fraction Stereotactic Body Radiotherapy Schedule for Centrally Located Non-Small-Cell Lung Cancer: NRG Oncology/RTOG 0813 Trial. J. Clin. Oncol. 2019, 37, 1316–1325. [Google Scholar] [CrossRef]
- Chang, J.Y.; Mehran, R.J.; Feng, L.; Verma, V.; Liao, Z.; Welsh, J.W.; Lin, S.H.; O’Reilly, M.S.; Jeter, M.D.; Balter, P.A.; et al. Stereotactic ablative radiotherapy for operable stage I non-small-cell lung cancer (revised STARS): Long-term results of a single-arm, prospective trial with prespecified comparison to surgery. Lancet Oncol. 2021, 22, 1448–1457. [Google Scholar] [CrossRef] [PubMed]
- Shaw, E.; Scott, C.; Souhami, L.; Dinapoli, R.; Kline, R.; Loeffler, J.; Farnan, N. Single dose radiosurgical treatment of recurrent previously irradiated primary brain tumors and brain metastases: Final report of RTOG protocol 90-05. Int. J. Radiat. Oncol. Biol. Phys. 2000, 47, 291–298. [Google Scholar] [CrossRef]
- Brown, P.D.; Ballman, K.V.; Cerhan, J.H.; Anderson, S.K.; Carrero, X.W.; Whitton, A.C.; Greenspoon, J.; Parney, I.F.; Laack, N.N.I.; Ashman, J.B.; et al. Postoperative stereotactic radiosurgery compared with whole brain radiotherapy for resected metastatic brain disease (NCCTG N107C/CEC·3): A multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2017, 18, 1049–1060. [Google Scholar] [CrossRef]
- Cox, B.W.; Spratt, D.E.; Lovelock, M.; Bilsky, M.H.; Lis, E.; Ryu, S.; Sheehan, J.; Gerszten, P.C.; Chang, E.; Gibbs, I.; et al. International Spine Radiosurgery Consortium consensus guidelines for target volume definition in spinal stereotactic radiosurgery. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, e597–e605. [Google Scholar] [CrossRef]
- Prasanna, P.G.; Stone, H.B.; Wong, R.S.; Capala, J.; Bernhard, E.J.; Vikram, B.; Coleman, C.N. Normal tissue protection for improving radiotherapy: Where are the Gaps? Transl. Cancer Res. 2012, 1, 35–48. [Google Scholar]
- Ricardi, U.; Badellino, S.; Filippi, A.R. Stereotactic body radiotherapy for early stage lung cancer: History and updated role. Lung Cancer 2015, 90, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Folkert, M.R.; Timmerman, R.D. Stereotactic ablative body radiosurgery (SABR) or Stereotactic body radiation therapy (SBRT). Adv. Drug Deliv. Rev. 2017, 109, 3–14. [Google Scholar] [CrossRef]
- Popp, I.; Grosu, A.L.; Niedermann, G.; Duda, D.G. Immune modulation by hypofractionated stereotactic radiation therapy: Therapeutic implications. Radiother. Oncol. 2016, 120, 185–194. [Google Scholar] [CrossRef]
- Zeng, J.; Harris, T.J.; Lim, M.; Drake, C.G.; Tran, P.T. Immune modulation and stereotactic radiation: Improving local and abscopal responses. Biomed. Res. Int. 2013, 2013, 658126. [Google Scholar] [CrossRef]
- Snyder, A.R. Review of radiation-induced bystander effects. Hum. Exp. Toxicol. 2004, 23, 87–89. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, S.E.; Timmerman, R.; McBride, W.H.; Schaue, D.; Hoffe, S.E.; Mantz, C.A.; Wilson, G.D. The confluence of stereotactic ablative radiotherapy and tumor immunology. Clin. Dev. Immunol. 2011, 2011, 439752. [Google Scholar] [CrossRef]
- Muroyama, Y.; Nirschl, T.R.; Kochel, C.M.; Lopez-Bujanda, Z.; Theodros, D.; Mao, W.; Carrera-Haro, M.A.; Ghasemzadeh, A.; Marciscano, A.E.; Velarde, E.; et al. Stereotactic Radiotherapy Increases Functionally Suppressive Regulatory T Cells in the Tumor Microenvironment. Cancer Immunol. Res. 2017, 5, 992–1004. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Auh, S.L.; Wang, Y.; Burnette, B.; Wang, Y.; Meng, Y.; Beckett, M.; Sharma, R.; Chin, R.; Tu, T.; et al. Therapeutic effects of ablative radiation on local tumor require CD8+ T cells: Changing strategies for cancer treatment. Blood 2009, 114, 589–595. [Google Scholar] [CrossRef]
- Liu, C.; Hu, Q.; Xu, B.; Hu, X.; Su, H.; Li, Q.; Zhang, X.; Yue, J.; Yu, J. Peripheral memory and naïve T cells in non-small cell lung cancer patients with lung metastases undergoing stereotactic body radiotherapy: Predictors of early tumor response. Cancer Cell Int. 2019, 19, 121. [Google Scholar] [CrossRef]
- Liu, C.; Hu, Q.; Hu, K.; Su, H.; Shi, F.; Kong, L.; Zhu, H.; Yu, J. Increased CD8+CD28+ T cells independently predict better early response to stereotactic ablative radiotherapy in patients with lung metastases from non-small cell lung cancer. J. Transl. Med. 2019, 17, 120. [Google Scholar] [CrossRef]
- Mirjolet, C.; Charon-Barra, C.; Ladoire, S.; Arbez-Gindre, F.; Bertaut, A.; Ghiringhelli, F.; Leroux, A.; Peiffert, D.; Borg, C.; Bosset, J.F.; et al. Tumor lymphocyte immune response to preoperative radiotherapy in locally advanced rectal cancer: The LYMPHOREC study. Oncoimmunology 2018, 7, e1396402. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | |
|---|---|---|
| Age, y, median (range) | 62 (31–85) | |
| Sex, male/female | 38/28 (%57.6/%42.4) | |
| ECOG Performance Score | 0 | 18 (%27.3) |
| 1 | 40 (%60.6) | |
| 2 | 8 (%12.1) | |
| Smoke | No | 35 (%53) |
| Yes | 31 (%47) | |
| Primary Disease Site and Histology | Lung | 29 (%43.9) |
| Adenocarcinoma | 20 (%30.2) | |
| SCC | 5 (%7.6) | |
| Small Cell Carcinoma | 4 (%6.1) | |
| Brain (Glioblastoma Multiforme) | 2 (%3) | |
| Breast | 9 (%13.6) | |
| Head and Neck | 7 (%10.6) | |
| SCC | 1 (%1.5) | |
| Glomus | 5 (%7.6) | |
| Schwannoma | 1 (%1.5) | |
| Genitourinary System | 8 (%12.1) | |
| Renal Cell Carcinoma | 5 (%7.6) | |
| Prostate Adenocarcinoma | 2 (%3) | |
| Urothelial Carcinoma | 1 (%1.5) | |
| Gastrointestinal System | 5 (%7.6) | |
| Colorectal Adenocarcinoma | 4 (%6.1) | |
| Pancreatic Adenocarcinoma | 1 (%1.5) | |
| Endometrial Adenocarcinoma | 1 (%1.5) | |
| Soft Tissue Sarcoma | 2 (%3) | |
| Kordoma | 2 (%3) | |
| Peritoneal Mezothelioma | 1 (%1.5) | |
| SBRT Site | Lung | 22 (%33.3) |
| Brain | 20 (%30.3) | |
| Bone | 13 (%19.7) | |
| Neck | 6 (%9.1) | |
| Surrenal | 2 (%3) | |
| Liver | 1 (%1.5) | |
| Pancreas | 1 (%1.5) | |
| Prostate | 1 (%1.5) | |
| Previous Chemotherapy | No | 15 (%22.7) |
| Yes | 51 (%77.3) | |
| Previous Immunotherapy | No | 61 (%92.4) |
| Yes | 5 (%7.6) | |
| Previous Radiotherapy | No | 34 (%51.5) |
| Yes | 32 (%48.5) | |
| Chemotherapy after SBRT | No | 39 (%59.1) |
| Yes | 27 (%40.9) | |
| Immunotherapy after SBRT | No | 59 (%89.4) |
| Yes | 7 (%10.6) | |
| Radiotherapy after SBRT | No | 48 (%72.7) |
| Yes | 18 (%27.3) | |
| Concomitant Treatment with SBRT | No | 43 (%65.2) |
| Yes | 23 (%34.8) | |
| Chemotherapy | 18 (%27.3) | |
| Immunotherapy | 5 (%7.5) | |
| Parameter | Pre-Treatment Levels | Post-Treatment Levels | p Value |
|---|---|---|---|
| TBX21 | 7.05 (2.3–16) | 4.15 (1.8–16) | p < 0.001 |
| GATA 3 | 0.76 (0.19–20) | 0.41 (0.19–19.83) | p = 0.005 |
| TBX21/GATA3 | 8.89 (0.8–84.21) | 11.46 (0.15–84.21) | p = 0.76 |
| RORɣt | 240.15 (115.9–1500) | 235.45 (169.7–1500) | p = 0.49 |
| FoxP3 | 1.03 (0.19–3.08) | 0.19 (0.19–11.44) | p < 0.001 |
| FoxP3/RORɣt | 0.004 (0–0.02) | 0.001 (0–0.05) | p < 0.001 |
| WBC | 6.83 (2–15.5) | 7.08 (2.2–18.8) | p = 0.51 |
| ALC | 1.46 (0.4–2.9) | 1.36 (0.4–3) | p = 0.092 |
| ANC | 4.80 (1–14.2) | 4.92 (0.9–17) | p = 0.74 |
| CRP | 4.83 (1.37–81.5) | 6.45 (1.53–80) | p = 0.143 |
| Parameter | Region | Pre-Treatment Levels | Post-Treatment Levels | p Value |
|---|---|---|---|---|
| TBX21 | Brain | 7.4 (2.3–16) | 3.65 (1.8–16) | p < 0.001 |
| Lung | 7.35 (5.3–16) | 4.5 (2.4–16) | p < 0.001 | |
| Bone | 5.1 (2.4–16) | 4.2 (2.2–16) | p = 0.021 | |
| GATA-3 | Brain | 0.77 (0.19–8.34) | 0.61 (0.19–9.62) | p = 0.49 |
| Lung | 0.80 (0.19–2.13) | 0.41 (0.19–17.61) | p = 0.03 | |
| Bone | 0.45 (0.19–1.62) | 0.35 (0.19–1.02) | p = 0.047 | |
| RORɣt | Brain | 254.25 (146.1–1500) | 225.35 (169.7–1500) | p = 0.27 |
| Lung | 227.25 (154.7–1500) | 263.15 (171.2–1500) | p = 0.12 | |
| Bone | 266.7 (115.9–1500) | 225 (170.2–1500) | p = 0.48 | |
| FoxP3 | Brain | 1.04 (0.19–2.16) | 0.19 (0.19–0.93) | p = 0.002 |
| Lung | 1.03 (0.19–1.82) | 0.21 (0.19–11.44) | p = 0.003 | |
| Bone | 1.01 (0.19–1.13) | 0.19 (0.19–0.48) | p = 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ucgul, A.N.; Bora, H.; Yaz Aydin, G.; Gulbahar, O.; Koken, U.H. Immune Modulation Through Stereotactic Radiotherapy: The Role of TBX21, GATA-3, FoxP3, and RORɣt. Medicina 2025, 61, 717. https://doi.org/10.3390/medicina61040717
Ucgul AN, Bora H, Yaz Aydin G, Gulbahar O, Koken UH. Immune Modulation Through Stereotactic Radiotherapy: The Role of TBX21, GATA-3, FoxP3, and RORɣt. Medicina. 2025; 61(4):717. https://doi.org/10.3390/medicina61040717
Chicago/Turabian StyleUcgul, Aybala Nur, Huseyin Bora, Gizem Yaz Aydin, Ozlem Gulbahar, and Ummu Habibe Koken. 2025. "Immune Modulation Through Stereotactic Radiotherapy: The Role of TBX21, GATA-3, FoxP3, and RORɣt" Medicina 61, no. 4: 717. https://doi.org/10.3390/medicina61040717
APA StyleUcgul, A. N., Bora, H., Yaz Aydin, G., Gulbahar, O., & Koken, U. H. (2025). Immune Modulation Through Stereotactic Radiotherapy: The Role of TBX21, GATA-3, FoxP3, and RORɣt. Medicina, 61(4), 717. https://doi.org/10.3390/medicina61040717