
Prevalence and Associated Factors of Dynapenia, Pre-Sarcopenia, and Sarcopenia in Korean Adults: A Cross-Sectional Epidemiological Study


Abstract
1. Introduction
2. Materials and Methods
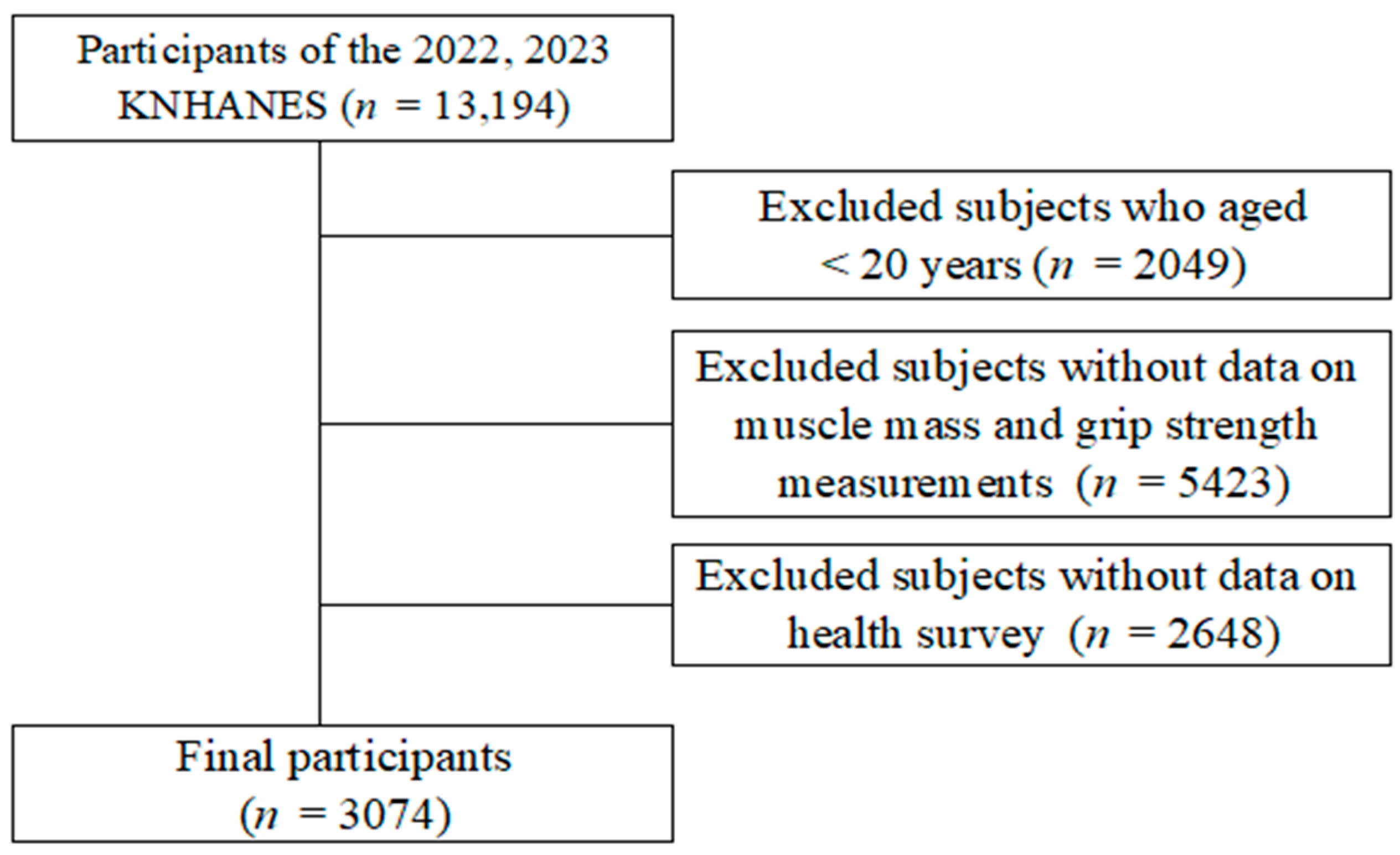
2.1. Study Design and Participants
2.2. Definitions of Dynapenia, Pre-Sarcopenia, and Sarcopenia
2.2.1. Sociodemographic Factors
2.2.2. Health Status and Behavior Factors
2.2.3. Comorbid Health Conditions
2.3. Statistical Analysis
3. Results
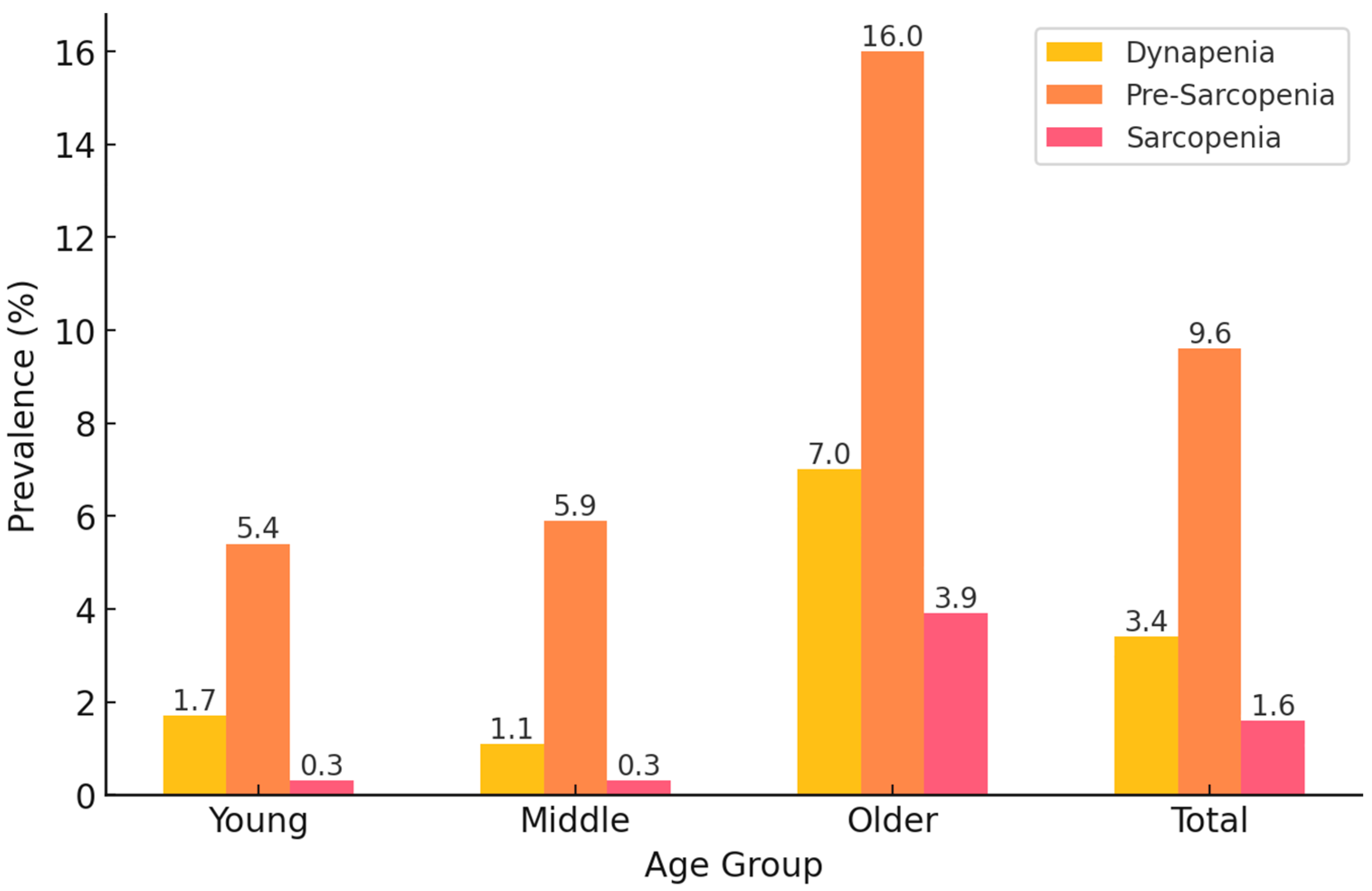
3.1. Prevalence of Dynapenia, Pre-Sarcopenia, and Sarcopenia
3.2. Sociodemographic Characteristics of Participants
3.3. Health Status and Health Behavior Characteristics of Participants
3.4. Factors Associated with Dynapenia, Pre-Sarcopenia, and Sarcopenia
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walston, J.D. Sarcopenia in older adults. Curr. Opin. Rheumatol. 2012, 24, 623–627. [Google Scholar] [CrossRef]
- Lee, D.Y.; Shin, S. Association of Sarcopenia with Osteopenia and Osteoporosis in Community-Dwelling Older Korean Adults: A Cross-Sectional Study. J. Clin. Med. 2021, 11, 129. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.Y.; Shin, S. Sarcopenia Is Associated with Metabolic Syndrome in Korean Adults Aged over 50 Years: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 1330. [Google Scholar] [CrossRef] [PubMed]
- Zuo, X.; Li, X.; Tang, K.; Zhao, R.; Wu, M.; Wang, Y.; Li, T. Sarcopenia and cardiovascular diseases: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2023, 14, 1183–1198. [Google Scholar] [CrossRef] [PubMed]
- Liao, M.C.; Yen, C.C.; Lin, Y.T.; Huang, F.D.; Chang, Y.T. Sarcopenia is associated with mortality in non-critical elderly patients visiting the emergency department. Front. Med. 2022, 9, 1027503. [Google Scholar] [CrossRef]
- Clark, B.C.; Manini, T.M. What is dynapenia? Nutrition 2012, 28, 495–503. [Google Scholar] [CrossRef]
- Keller, K.; Engelhardt, M. Strength and muscle mass loss with aging process. Age and strength loss. Muscles Ligaments Tendons J. 2013, 3, 346–350. [Google Scholar] [CrossRef]
- Santilli, V.; Bernetti, A.; Mangone, M.; Paoloni, M. Clinical definition of sarcopenia. Clin. Cases Miner. Bone Metab. Off. J. Ital. Soc. Osteoporos. Miner. Metab. Skelet. Dis. 2014, 11, 177–180. [Google Scholar]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef]
- Rattanasupar, A.; Prateepchaiboon, T.; Akarapatima, K.; Songjamrat, A.; Pakdeejit, S.; Chang, A. Impact of pre-sarcopenia on outcomes of transarterial chemoembolization in unresectable hepatocellular carcinoma. Sci. Rep. 2024, 14, 19249. [Google Scholar] [CrossRef]
- von Haehling, S.; Morley, J.E.; Anker, S.D. An overview of sarcopenia: Facts and numbers on prevalence and clinical impact. J. Cachexia Sarcopenia Muscle 2010, 1, 129–133. [Google Scholar] [CrossRef]
- Huang, J.; He, F.; Gu, X.; Chen, S.; Tong, Z.; Zhong, S. Estimation of sarcopenia prevalence in individuals at different ages from Zheijang province in China. Aging 2021, 13, 6066–6075. [Google Scholar] [CrossRef]
- Sun, S.; Lee, H.; Yim, H.W.; Won, H.S.; Ko, Y.H. The impact of sarcopenia on health-related quality of life in elderly people: Korean National Health and Nutrition Examination Survey. Korean J. Intern. Med. 2019, 34, 877–884. [Google Scholar] [CrossRef]
- Yeung, S.S.Y.; Reijnierse, E.M.; Pham, V.K.; Trappenburg, M.C.; Lim, W.K.; Meskers, C.G.M.; Maier, A.B. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2019, 10, 485–500. [Google Scholar] [CrossRef]
- Xia, L.; Zhao, R.; Wan, Q.; Wu, Y.; Zhou, Y.; Wang, Y.; Cui, Y.; Shen, X.; Wu, X. Sarcopenia and adverse health-related outcomes: An umbrella review of meta-analyses of observational studies. Cancer Med. 2020, 9, 7964–7978. [Google Scholar] [CrossRef]
- Murphy, C.H.; McCarthy, S.N.; Roche, H.M. Nutrition strategies to counteract sarcopenia: A focus on protein, LC n-3 PUFA and precision nutrition. Proc. Nutr. Soc. 2023, 82, 419–431. [Google Scholar] [CrossRef]
- Robinson, S.; Cooper, C.; Aihie Sayer, A. Nutrition and sarcopenia: A review of the evidence and implications for preventive strategies. J. Aging Res. 2012, 2012, 510801. [Google Scholar] [CrossRef]
- Shen, Y.; Shi, Q.; Nong, K.; Li, S.; Yue, J.; Huang, J.; Dong, B.; Beauchamp, M.; Hao, Q. Exercise for sarcopenia in older people: A systematic review and network meta-analysis. J. Cachexia Sarcopenia Muscle 2023, 14, 1199–1211. [Google Scholar] [CrossRef]
- Lee, D.Y. Sex-Specific Sarcopenia Prevalence and Risk Factors in the Korean Population: A Cross-Sectional Epidemiological Study. Medicina 2024, 60, 899. [Google Scholar] [CrossRef]
- Won, C.W. Management of Sarcopenia in Primary Care Settings. Korean J. Fam. Med. 2023, 44, 71–75. [Google Scholar] [CrossRef]
- Ooi, H.; Welch, C. Obstacles to the Early Diagnosis and Management of Sarcopenia: Current Perspectives. Clin. Interv. Aging 2024, 19, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.Y. Association Between Chronic Obstructive Pulmonary Disease and Low Muscle Mass in Korean Adults. J. Clin. Med. 2025, 14, 1134. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.Y.; Shin, S. Sarcopenia and Anemia in Elderly Koreans: A Nationwide Population-Based Study. Healthcare 2023, 11, 2428. [Google Scholar] [CrossRef]
- Purnamasari, D.; Tetrasiwi, E.N.; Kartiko, G.J.; Astrella, C.; Husam, K.; Laksmi, P.W. Sarcopenia and Chronic Complications of Type 2 Diabetes Mellitus. Rev. Diabet. Stud. RDS 2022, 18, 157–165. [Google Scholar] [CrossRef]
- Meng, S.; He, X.; Fu, X.; Zhang, X.; Tong, M.; Li, W.; Zhang, W.; Shi, X.; Liu, K. The prevalence of sarcopenia and risk factors in the older adult in China: A systematic review and meta-analysis. Front. Public Health 2024, 12, 1415398. [Google Scholar] [CrossRef]
- Kao, T.W.; Peng, T.C.; Chen, W.L.; Han, D.S.; Chen, C.L.; Yang, W.S. Impact of adiposity on muscle function and clinical events among elders with dynapenia, presarcopenia and sarcopenia: A community-based cross-sectional study. Aging 2021, 13, 7247–7258. [Google Scholar] [CrossRef]
- Lee, D.-Y. Incidence of low grip strength and related factors in the elderly korean. J. Korean Soc. Phys. Med. 2024, 19, 81–89. [Google Scholar] [CrossRef]
- Park, S.; Lee, J.H. Joint association of sedentary behavior and physical activity domains with depression in Korean adults: Cross-sectional study combining four biennial surveys (2016–2022). PLoS ONE 2024, 19, e0312029. [Google Scholar] [CrossRef]
- Lee, D.-Y. The association between sarcopenia and pulmonary function in Koreans: A cross-sectional study. Int. J. Gerontol 2021, 15, 319–323. [Google Scholar]
- Wilkinson, D.J.; Piasecki, M.; Atherton, P.J. The age-related loss of skeletal muscle mass and function: Measurement and physiology of muscle fibre atrophy and muscle fibre loss in humans. Ageing Res. Rev. 2018, 47, 123–132. [Google Scholar] [CrossRef]
- Gonzalez-Freire, M.; de Cabo, R.; Studenski, S.A.; Ferrucci, L. The Neuromuscular Junction: Aging at the Crossroad between Nerves and Muscle. Front. Aging Neurosci. 2014, 6, 208. [Google Scholar] [CrossRef]
- Trombetti, A.; Reid, K.F.; Hars, M.; Herrmann, F.R.; Pasha, E.; Phillips, E.M.; Fielding, R.A. Age-associated declines in muscle mass, strength, power, and physical performance: Impact on fear of falling and quality of life. Osteoporos. Int. 2016, 27, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Alexandre, T.D.S.; Duarte, Y.A.O.; Santos, J.L.F.; Lebrão, M.L. Prevalence and associated factors of sarcopenia, dynapenia, and sarcodynapenia in community-dwelling elderly in São Paulo—SABE Study. Rev. Bras. De Epidemiol. Braz. J. Epidemiol. 2019, 21 (Suppl. S2), e180009. [Google Scholar] [CrossRef]
- Neves, T.; Ferriolli, E.; Lopes, M.B.M.; Souza, M.G.C.; Fett, C.A.; Fett, W.C.R. Prevalence and factors associated with sarcopenia and dynapenia in elderly people. J. Frailty Sarcopenia Falls 2018, 3, 194–202. [Google Scholar] [CrossRef]
- Choi, Y.A.; Lee, J.S.; Kim, Y.H. Association between physical activity and dynapenia in older adults with COPD: A nationwide survey. Sci. Rep. 2022, 12, 7480. [Google Scholar] [CrossRef]
- Andreo-López, M.C.; Zarco-Martín, M.T.; Contreras-Bolívar, V.; Fernández-Soto, M.L. Prevalence of Sarcopenia and Dynapenia and Related Clinical Outcomes in Patients with Type 1 Diabetes Mellitus. Nutrients 2023, 15, 4914. [Google Scholar] [CrossRef]
- Mitchell, W.K.; Williams, J.; Atherton, P.; Larvin, M.; Lund, J.; Narici, M. Sarcopenia, dynapenia, and the impact of advancing age on human skeletal muscle size and strength; a quantitative review. Front. Physiol. 2012, 3, 260. [Google Scholar] [CrossRef]
- Della Peruta, C.; Lozanoska-Ochser, B.; Renzini, A.; Moresi, V.; Sanchez Riera, C.; Bouché, M.; Coletti, D. Sex Differences in Inflammation and Muscle Wasting in Aging and Disease. Int. J. Mol. Sci. 2023, 24, 4651. [Google Scholar] [CrossRef]
- Hwang, J.; Park, S. Gender-Specific Risk Factors and Prevalence for Sarcopenia among Community-Dwelling Young-Old Adults. Int. J. Environ. Res. Public Health 2022, 19, 7232. [Google Scholar] [CrossRef]
- Lu, L.; Tian, L. Postmenopausal osteoporosis coexisting with sarcopenia: The role and mechanisms of estrogen. J. Endocrinol. 2023, 259, E230116. [Google Scholar] [CrossRef]
- Orprayoon, N.; Wainipitapong, P.; Champaiboon, J.; Wattanachanya, L.; Jaisamrarn, U.; Chaikittisilpa, S. Prevalence of pre-sarcopenia among postmenopausal women younger than 65 years. Menopause 2021, 28, 1351–1357. [Google Scholar] [PubMed]
- Kim, J.H.; Choi, S.H.; Lim, S.; Yoon, J.W.; Kang, S.M.; Kim, K.W.; Lim, J.Y.; Cho, N.H.; Jang, H.C. Sarcopenia and obesity: Gender-different relationship with functional limitation in older persons. J. Korean Med. Sci. 2013, 28, 1041–1047. [Google Scholar] [CrossRef]
- Noh, H.M.; Park, Y.S. Handgrip strength, dynapenia, and mental health in older Koreans. Sci. Rep. 2020, 10, 4004. [Google Scholar] [CrossRef]
- Petersen, A.M.; Magkos, F.; Atherton, P.; Selby, A.; Smith, K.; Rennie, M.J.; Pedersen, B.K.; Mittendorfer, B. Smoking impairs muscle protein synthesis and increases the expression of myostatin and MAFbx in muscle. Am. J. Physiol. Endocrinol. Metab. 2007, 293, E843–E848. [Google Scholar] [CrossRef]
- Yang, L.; Ran, Q.; Yeo, Y.H.; Wen, Z.; Tuo, S.; Li, Y.; Yuan, J.; Dai, S.; Wang, J.; Ji, F.; et al. Sex disparity in the association between alcohol consumption and sarcopenia: A population-based study. Front. Nutr. 2025, 12, 1536488. [Google Scholar] [CrossRef]
- Steffl, M.; Bohannon, R.W.; Sontakova, L.; Tufano, J.J.; Shiells, K.; Holmerova, I. Relationship between sarcopenia and physical activity in older people: A systematic review and meta-analysis. Clin. Interv. Aging 2017, 12, 835–845. [Google Scholar] [CrossRef]
- Caan, B.J.; Cespedes Feliciano, E.M.; Kroenke, C.H. The importance of body composition in explaining the overweight paradox in cancer—Counterpoint. Cancer Res. 2018, 78, 1906–1912. [Google Scholar]
- Abramowitz, M.K.; Hall, C.B.; Amodu, A.; Sharma, D.; Androga, L.; Hawkins, M. Muscle mass, BMI, and mortality among adults in the United States: A population-based cohort study. PLoS ONE 2018, 13, e0194697. [Google Scholar] [CrossRef]
- Qiao, Y.S.; Chai, Y.H.; Gong, H.J.; Zhuldyz, Z.; Stehouwer, C.D.A.; Zhou, J.B.; Simó, R. The Association Between Diabetes Mellitus and Risk of Sarcopenia: Accumulated Evidences From Observational Studies. Front. Endocrinol. 2021, 12, 782391. [Google Scholar] [CrossRef]
- Liu, X.; Heras, G.; Lauschke, V.M.; Mi, J.; Tian, G.; Gastaldello, S. High glucose-induced oxidative stress accelerates myogenesis by altering SUMO reactions. Exp. Cell Res. 2020, 395, 112234. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Factors | Categories | Normal (n = 2527) | Dynapenia (n = 140) | Pre-Sarcopenia (n = 335) | Sarcopenia (n = 72) | p |
|---|---|---|---|---|---|---|
| M or % | M or % | M or % | M or % | |||
| Age | Young | 15.1 | 7.1 | 7.9 | 2.9 | <0.001 |
| Middle | 53.2 | 15.5 | 30.1 | 8.8 | ||
| Older | 31.7 | 77.3 | 62.0 | 88.3 | ||
| Sex | Male | 44.6 | 27.8 | 56.7 | 31.6 | <0.001 |
| Female | 53.6 | 72.2 | 43.3 | 68.4 | ||
| Education level | Elementary | 11.1 | 37.8 | 23.1 | 46.5 | <0.001 |
| Middle | 9.9 | 13.0 | 16.6 | 17.9 | ||
| High | 29.4 | 21.8 | 31.9 | 19.9 | ||
| University | 49.6 | 27.4 | 28.8 | 15.7 | ||
| Marital status | With | 85.9 | 68.5 | 82.5 | 62.5 | <0.001 |
| Without | 14.1 | 31.5 | 17.5 | 37.5 | ||
| Individual income | Q1 (Lowest) | 19.5 | 23.3 | 23.9 | 25.1 | 0.801 |
| Q2 | 24.3 | 24.2 | 24.8 | 27.7 | ||
| Q3 | 26.3 | 25.1 | 24.0 | 20.8 | ||
| Q4 (Highest) | 29.8 | 27.4 | 27.4 | 26.5 | ||
| Residential area | Urban | 84.9 | 77.4 | 84.4 | 81.0 | 0.256 |
| Rural | 15.1 | 22.6 | 15.6 | 19.0 |
| Factors | Categories | Normal (n = 2527) | Dynapenia (n = 140) | Pre-Sarcopenia (n = 335) | Sarcopenia (n = 72) | p |
|---|---|---|---|---|---|---|
| M or % | M or % | M or % | M or % | |||
| Subjective health status | Good | 37.0 | 26.1 | 28.0 | 16.6 | <0.001 |
| Moderate | 47.7 | 53.0 | 46.7 | 49.8 | ||
| Bad | 15.3 | 20.9 | 25.3 | 33.6 | ||
| Stress level | High | 21.7 | 26.5 | 15.5 | 24.1 | 0.037 |
| Low | 78.3 | 73.5 | 84.5 | 75.9 | ||
| Smoking status | Current | 14.6 | 4.8 | 19.6 | 5.3 | <0.001 |
| Past | 26.8 | 20.5 | 27.7 | 18.3 | ||
| Non | 58.5 | 74.7 | 52.7 | 76.4 | ||
| Alcohol status | Yes | 54.7 | 33.8 | 42.6 | 20.0 | <0.001 |
| No | 45.3 | 66.2 | 57.4 | 80.0 | ||
| Physical activity | LPA | 88.8 | 95.5 | 97.5 | 97.9 | <0.001 |
| MVPA | 11.2 | 4.5 | 2.5 | 2.1 | ||
| Comorbidity conditions | ||||||
| Hypertension | 28.4 | 31.9 | 34.2 | 29.1 | 0.204 | |
| Diabetes | 41.6 | 51.1 | 45.8 | 58.7 | 0.011 | |
| High triglyceride | 26.8 | 23.9 | 17.1 | 23.2 | 0.006 | |
| Low HDL-C | 22.1 | 26 | 16.2 | 29.8 | 0.047 | |
| Abdominal obesity | 40.7 | 53.7 | 9.5 | 15.4 | <0.001 | |
| Categories | Dynapenia | Pre-Sarcopenia | Sarcopenia | ||||
|---|---|---|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | ||
| Age | Young | 1 (reference) | 1 (reference) | 1 (reference) | |||
| Middle | 0.646 (0.202–2.068) | 0.010 | 0.923 (0.510–1.670) | 0.009 | 0.635 (0.115–3.490) | 0.010 | |
| Older | 5.426 (1.509–19.518) | <0.001 | 2.354 (1.239–4.471) | <0.001 | 7.695 (1.634–36.233) | <0.001 | |
| Sex | Male | 0.588 (0.313–1.102) | 0.098 | 2.375 (1.582–3.565) | <0.001 | 1.52 (0.654–3.533) | 0.331 |
| Female | 1 (reference) | 1 (reference) | 1 (reference) | ||||
| Education level | Elementary | 1.094 (0.54–2.217) | 0.803 | 2.065 (1.264–3.375) | 0.004 | 2.273 (0.838–6.165) | 0.107 |
| Middle | 0.598 (0.276–1.297) | 0.192 | 1.997 (1.212–3.29) | 0.007 | 1.424 (0.558–3.636) | 0.460 | |
| High | 0.786 (0.429–1.439) | 0.433 | 1.58 (1.045–2.391) | 0.031 | 1.197 (0.455–3.152) | 0.716 | |
| University | 1 (reference) | 1 (reference) | 1 (reference) | ||||
| Marital status | With | 0.711 (0.442–2.219) | 0.159 | 0.937 (0.648–1.354) | 0.726 | 0.535 (0.286–1.001) | 0.051 |
| Without | 1 (reference) | 1 (reference) | 1 (reference) | ||||
| Individual income | Q1 (Lowest) | 1.233 (0.685–2.219) | 0.485 | 1.132 (0.741–1.729) | 0.568 | 1.242 (0.599–2.579) | 0.561 |
| Q2 | 1.241 (0.673–2.289) | 0.490 | 1.031 (0.671–1.585) | 0.892 | 1.424 (0.726–2.794) | 0.303 | |
| Q3 | 1.060 (0.600–1.872) | 0.843 | 0.952 (0.609–1.488) | 0.828 | 0.918 (0.423–1.991) | 0.828 | |
| Q4 (Highest) | 1 (reference) | 1 (reference) | 1 (reference) | ||||
| Residential area | Urban | 0.687 (0.42–1.123) | 0.134 | 1.308 (0.952–1.796) | 0.098 | 1.076 (0.495–2.343) | 0.854 |
| Rural | 1 (reference) | 1 (reference) | 1 (reference) | ||||
| Subjective health status | Good | 1 (reference) | 1 (reference) | 1 (reference) | |||
| Moderate | 1.349 (0.846–2.15) | 0.209 | 1.409 (0.971–2.045) | 0.072 | 2.079 (0.995–4.344) | 0.052 | |
| Bad | 1.173 (0.653–2.108) | 0.594 | 2.626 (1.682–4.102) | 0.001 | 3.412 (1.434–8.121) | 0.006 | |
| Stress level | High | 2.084 (1.338–3.247) | 0.002 | 0.799 (0.55–1.162) | 0.239 | 1.828 (0.948–3.524) | 0.072 |
| Low | 1 (reference) | 1 (reference) | 1 (reference) | ||||
| Smoking status | Current | 0.495 (0.204–1.198) | 0.119 | 1.621 (1.026–2.562) | 0.039 | 0.436 (0.135–1.406) | 0.164 |
| Past | 0.933 (0.503–1.732) | 0.825 | 0.792 (0.538–1.166) | 0.236 | 0.606 (0.261–1.409) | 0.244 | |
| Non | 1 (reference) | 1 (reference) | 1 (reference) | ||||
| Alcohol status | Yes | 0.903 (0.552–1.478) | 0.684 | 0.67 (0.476–0.942) | 0.022 | 0.448 (0.236–0.852) | 0.015 |
| No | 1 (reference) | 1 (reference) | 1 (reference) | ||||
| Physical activity | Low | 1.413 (0.596–3.351) | 0.432 | 4.958 (1.941–12.664) | 0.001 | 3.029 (0.394–23.304) | 0.287 |
| Moderate–Vigorous | 1 (reference) | 1 (reference) | 1 (reference) | ||||
| Comorbidities conditions | |||||||
| Hypertension | 0.731 (0.491–1.088) | 0.122 | 1.175 (0.847–1.63) | 0.336 | 0.646 (0.373–1.121) | 0.120 | |
| Diabetes | 1.13 (0.798–1.6) | 0.491 | 1.085 (0.817–1.44) | 0.575 | 1.614 (0.929–2.805) | 0.090 | |
| High triglyceride | 1.093 (0.653–1.83) | 0.735 | 0.655 (0.437–0.981) | 0.040 | 0.993 (0.474–2.077) | 0.983 | |
| Low HDL-C | 0.854 (0.536–1.362) | 0.505 | 0.785 (0.501–1.231) | 0.291 | 1.126 (0.588–2.155) | 0.722 | |
| Abdominal obesity | 1.228 (0.817–1.846) | 0.325 | 0.107 (0.073–0.157) | 0.001 | 0.134 (0.065–0.28) | 0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the author. Published by MDPI on behalf of the Lithuanian University of Health Sciences. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.-Y. Prevalence and Associated Factors of Dynapenia, Pre-Sarcopenia, and Sarcopenia in Korean Adults: A Cross-Sectional Epidemiological Study. Medicina 2025, 61, 575. https://doi.org/10.3390/medicina61040575
Lee D-Y. Prevalence and Associated Factors of Dynapenia, Pre-Sarcopenia, and Sarcopenia in Korean Adults: A Cross-Sectional Epidemiological Study. Medicina. 2025; 61(4):575. https://doi.org/10.3390/medicina61040575
Chicago/Turabian StyleLee, Do-Youn. 2025. "Prevalence and Associated Factors of Dynapenia, Pre-Sarcopenia, and Sarcopenia in Korean Adults: A Cross-Sectional Epidemiological Study" Medicina 61, no. 4: 575. https://doi.org/10.3390/medicina61040575
APA StyleLee, D.-Y. (2025). Prevalence and Associated Factors of Dynapenia, Pre-Sarcopenia, and Sarcopenia in Korean Adults: A Cross-Sectional Epidemiological Study. Medicina, 61(4), 575. https://doi.org/10.3390/medicina61040575