
Value of Proximal Femur Geometry in Predicting Occult Hip Fracture

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
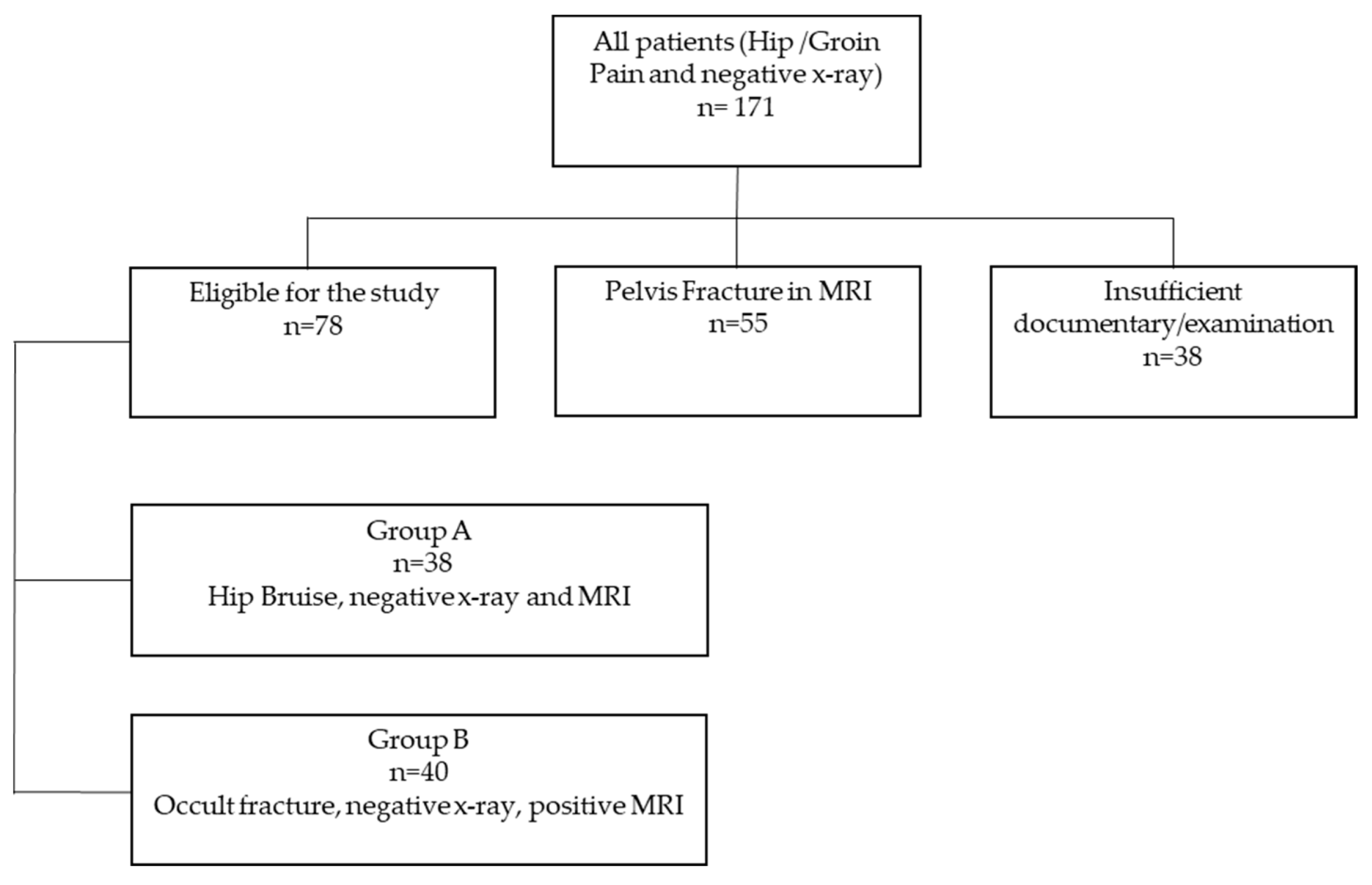
2.1. Subjects
2.2. Radiography and Radiological Indices
2.3. MRI
2.4. Statistical Analysis
3. Results
3.1. Reliability of Measurements
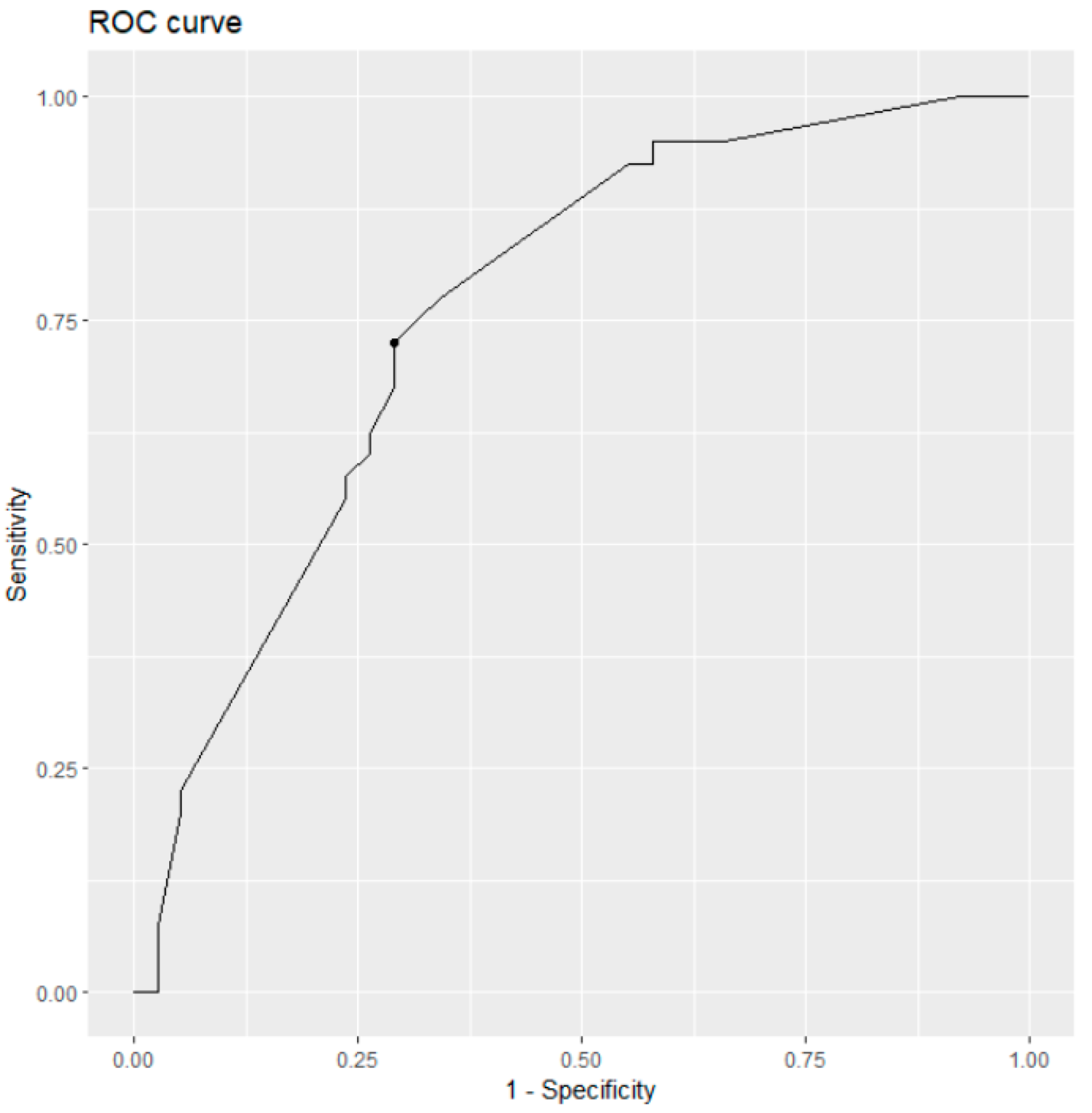
3.2. Results of ROC Curve Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schneider, E.L.; Guralnik, J.M. The aging of America. Impact on health care costs. JAMA 1990, 263, 2335–2340. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Maggi, S. Epidemiology and social costs of hip fracture. Injury 2018, 49, 1458–1460. [Google Scholar] [CrossRef] [PubMed]
- Rapp, K.; Becker, C.; Todd, C.; Rothenbacher, D.; Schulz, C.; König, H.H.; Liener, U.; Hartwig, E.; Büchele, G. The Association Between Orthogeriatric Co-Management and Mortality Following Hip Fracture. Dtsch. Arztebl. Int. 2020, 117, 53–59. [Google Scholar] [CrossRef]
- Haj-Mirzaian, A.; Eng, J.; Khorasani, R.; Raja, A.S.; Levin, A.S.; Smith, S.E.; Johnson, P.T.; Demehri, S. Use of Advanced Imaging for Radiographically Occult Hip Fracture in Elderly Patients: A Systematic Review and Meta-Analysis. Radiology 2020, 296, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Cannon, J.; Silvestri, S.; Munro, M. Imaging choices in occult hip fracture. J. Emerg. Med. 2009, 37, 144–152. [Google Scholar] [CrossRef]
- Sankey, R.A.; Turner, J.; Lee, J.; Healy, J.; Gibbons, C.E. The use of MRI to detect occult fractures of the proximal femur: A study of 102 consecutive cases over a ten-year period. J. Bone Jt. Surg. Br. 2009, 91, 1064–1068. [Google Scholar] [CrossRef] [PubMed]
- Walsh, P.J.; Farooq, M.; Walz, D.M. Occult fracture propagation in patients with isolated greater trochanteric fractures: Patterns and management. Skelet. Radiol. 2022, 51, 1391–1398. [Google Scholar] [CrossRef]
- Deleanu, B.; Prejbeanu, R.; Tsiridis, E.; Vermesan, D.; Crisan, D.; Haragus, H.; Predescu, V.; Birsasteanu, F. Occult fractures of the proximal femur: Imaging diagnosis and management of 82 cases in a regional trauma center. World J. Emerg. Surg. 2015, 10, 55. [Google Scholar] [CrossRef]
- Gill, S.K.; Smith, J.; Fox, R.; Chesser, T.J. Investigation of occult hip fractures: The use of CT and MRI. Sci. World J. 2013, 2013, 830319. [Google Scholar] [CrossRef]
- Dominguez, S.; Liu, P.; Roberts, C.; Mandell, M.; Richman, P.B. Prevalence of traumatic hip and pelvic fractures in patients with suspected hip fracture and negative initial standard radiographs—A study of emergency department patients. Acad. Emerg. Med. 2005, 12, 366–369. [Google Scholar] [CrossRef]
- Daabiss, M. American Society of Anaesthesiologists physical status classification. Indian J. Anaesth. 2011, 55, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Ulusoy, H.; Bilgici, A.; Kuru, O.; Sarica, N.; Arslan, S.; Erkorkmaz, U. A new value of proximal femur geometry to evaluate hip fracture risk: True moment arm. Hip Int. 2008, 18, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Partanen, J.; Jämsä, T.; Jalovaara, P. Influence of the upper femur and pelvic geometry on the risk and type of hip fractures. J. Bone Miner. Res. 2001, 16, 1540–1546. [Google Scholar] [CrossRef]
- Pulkkinen, P.; Partanen, J.; Jalovaara, P.; Jämsä, T. Combination of bone mineral density and upper femur geometry improves the prediction of hip fracture. Osteoporos. Int. 2004, 15, 274–280. [Google Scholar] [CrossRef]
- El-Kaissi, S.; Pasco, J.A.; Henry, M.J.; Panahi, S.; Nicholson, J.G.; Nicholson, G.C.; Kotowicz, M.A. Femoral neck geometry and hip fracture risk: The Geelong osteoporosis study. Osteoporos Int. 2005, 16, 1299–1303. [Google Scholar] [CrossRef]
- Hans, D.; Šteňová, E.; Lamy, O. The Trabecular Bone Score (TBS) Complements DXA and the FRAX as a Fracture Risk Assessment Tool in Routine Clinical Practice. Curr. Osteoporos. Rep. 2017, 15, 521–531. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.T.; Cherian, K.E.; Kapoor, N.; Jebasingh, F.K.; Asha, H.S.; Mathai, T.; Nithyananth, M.; Oommen, A.T.; Daniel, A.J.; Thomas, N.; et al. Does hip structural analysis confer additional benefit to routine BMD assessment in postmenopausal women with hip fracture? A study from a tertiary center in southern India. Arch. Osteoporos. 2022, 17, 32. [Google Scholar] [CrossRef]
- Noble, P.C.; Box, G.G.; Kamaric, E.; Fink, M.J.; Alexander, J.W.; Tullos, H.S. The effect of aging on the shape of the proximal femur. Clin. Orthop. Relat. Res. 1995, 316, 31–44. [Google Scholar] [CrossRef]
- Tawada, K.; Iguchi, H.; Tanaka, N.; Watanabe, N.; Murakami, S.; Hasegawa, S.; Otsuka, T. Is the canal flare index a reliable means of estimation of canal shape? Measurement of proximal femoral geometry by use of 3D models of the femur. J. Orthop. Sci. 2015, 20, 498–506. [Google Scholar] [CrossRef]
- Dorr, L.D.; Faugere, M.C.; Mackel, A.M.; Gruen, T.A.; Bognar, B.; Malluche, H.H. Structural and cellular assessment of bone quality of proximal femur. Bone 1993, 14, 231–242. [Google Scholar] [CrossRef]
- Dorr, L.D. Total hip replacement using APR system. Tech. Orthop. 1986, 1, 22–34. [Google Scholar] [CrossRef]
- Noble, P.C.; Alexander, J.W.; Lindahl, L.J.; Yew, D.T.; Granberry, W.M.; Tullos, H.S. The anatomic basis of femoral component design. Clin. Orthop. Relat. Res. 1988, 235, 148–165. [Google Scholar] [CrossRef]
- Spotorno, L.; Romagnoli, S. Indications for the CLS stem, The CLS uncemented total hip replacement system. Berna Protek 1991, 4. [Google Scholar]
- Yeung, Y.; Chiu, K.Y.; Yau, W.P.; Tang, W.M.; Cheung, W.Y.; Ng, T.P. Assessment of the proximal femoral morphology using plain radiograph—Can it predict the bone quality? J. Arthroplast. 2006, 21, 508–513. [Google Scholar] [CrossRef]
- Liu, Y.; Ma, W.J.; Huang, K.; Yang, J.; Zeng, Y.; Shen, B. Radiographic indexes in AP hip radiographs prior to total hip arthroplasty reveal candidates with low BMD. Osteoporos. Int. 2022, 33, 871–879. [Google Scholar] [CrossRef]
- Klestil, T.; Röder, C.; Stotter, C.; Winkler, B.; Nehrer, S.; Lutz, M.; Klerings, I.; Wagner, G.; Gartlehner, G.; Nussbaumer-Streit, B. Impact of timing of surgery in elderly hip fracture patients: A systematic review and meta-analysis. Sci. Rep. 2018, 8, 13933. [Google Scholar] [CrossRef]
- Lim, K.B.; Eng, A.K.; Chng, S.M.; Tan, A.G.; Thoo, F.L.; Low, C.O. Limited magnetic resonance imaging (MRI) and the occult hip fracture. Ann. Acad. Med. Singap. 2002, 31, 607–610. [Google Scholar] [PubMed]
- Haubro, M.; Stougaard, C.; Torfing, T.; Overgaard, S. Sensitivity and specificity of CT- and MRI-scanning in evaluation of occult fracture of the proximal femur. Injury 2015, 46, 1557–1561. [Google Scholar] [CrossRef]
- Cabarrus, M.C.; Ambekar, A.; Lu, Y.; Link, T.M. MRI and CT of insufficiency fractures of the pelvis and the proximal femur. AJR Am. J. Roentgenol. 2008, 191, 995–1001. [Google Scholar] [CrossRef]
- Expert Panel on Musculoskeletal Imaging; Ross, A.B.; Lee, K.S.; Chang, E.Y.; Amini, B.; Bussell, J.K.; Gorbachova, T.; Ha, A.S.; Khurana, B.; Klitzke, A.; et al. ACR Appropriateness Criteria® Acute Hip Pain-Suspected Fracture. J. Am. Coll. Radiol. 2019, 16, S18–S25. [Google Scholar] [CrossRef] [PubMed]
- Reddy, T.; McLaughlin, P.D.; Mallinson, P.I.; Reagan, A.C.; Munk, P.L.; Nicolaou, S.; Ouellette, H.A. Detection of occult, undisplaced hip fractures with a dual-energy CT algorithm targeted to detection of bone marrow edema. Emerg. Radiol. 2015, 22, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Sah, A.P.; Thornhill, T.S.; LeBoff, M.S.; Glowacki, J. Correlation of plain radiographic indices of the hip with quantitative bone mineral density. Osteoporos. Int. 2007, 18, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Ohnaru, K.; Sone, T.; Tanaka, K.; Akagi, K.; Ju, Y.I.; Choi, H.J.; Tomomitsu, T.; Fukunaga, M. Hip structural analysis: A comparison of DXA with CT in postmenopausal Japanese women. Springerplus 2013, 2, 331. [Google Scholar] [CrossRef]
- Beck, T.J.; Broy, S.B. Measurement of Hip Geometry—Technical Background. J. Clin. Densitom. 2015, 18, 331–337. [Google Scholar] [CrossRef]
- LaCroix, A.Z.; Beck, T.J.; Cauley, J.A.; Lewis, C.E.; Bassford, T.; Jackson, R.; Wu, G.; Chen, Z. Hip structural geometry and incidence of hip fracture in postmenopausal women: What does it add to conventional bone mineral density? Osteoporos. Int. 2010, 21, 919–929. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, B.N.; Hoshino, H.; Togawa, D.; Matsuyama, Y. Cortical Thickness Index of the Proximal Femur: A Radiographic Parameter for Preliminary Assessment of Bone Mineral Density and Osteoporosis Status in the Age 50 Years and Over Population. Clin. Orthop. Surg. 2018, 10, 149–156. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group A (n = 38) | Group B (n = 40) | |
|---|---|---|
| Age (Mean (SD)) | 84.3 (6.0) | 79.2 (11.6) |
| Gender n (%) | ||
| 35 (92%) | 24 (60%) |
| 3 (8%) | 16 (40%) |
| Residence n (%) | ||
| 23 (61%) | 12 (30%) |
| 6 (16%) | 20 (50%) |
| 7 (18%) | 6 (15%) |
| 2 (5%) | 2 (5%) |
| ASA Grade n (%) | ||
| - | - |
| 2 (5%) | 1 (2%) |
| 36 (95%) | 35 (88%) |
| - | 4 (10%) |
| CCI (median (range)) | 5 (3–9) | 6 (2–11) |
| MRI days after admission (median (range)) | 2 (0–14) | 1.5 (0–35) |
| Vitamin D (mg/mL) n | ||
| 14 | 14 |
| 5 | 9 |
| 6 | 6 |
| 13 | 9 |
| 5 | 2 |
| Variable | Hip Bruise (n = 38) | Occult Proximal Femur Fracture (n = 40) | ||
|---|---|---|---|---|
| [mean (SD)] | Rater 1 | Rater 2 | Rater 1 | Rater 2 |
| CTI | 31.1 (3.68) | 31.3 (3.13) | 32.6 (3.63) | 32.3 (4.33) |
| CFI | 3.7 (0.74) | 3.6 (0.75) | 3.5 (0.65) | 3.4 (0.73) |
| MCI | 2.6 (0.57) | 2.5 (0.51) | 2.4 (0.37) | 2.4 (0.39) |
| CBR | 0.5 (0.07) | 0.5 (0.09) | 0.5 (0.08) | 0.5 (0.07) |
| CBAR | 0.5 (0.08) | 0.5 (0.09) | 0.5 (0.07) | 0.6 (0.15) |
| CRR | 0.5 (0.12) | 0.5 (0.14) | 0.5 (0.11) | 0.5 (0.10) |
| Variable | Univariate Analysis | |
|---|---|---|
| AUC | Optimal Cut-Off | |
| CTI | 0.580 | 35.39 |
| CFI | 0.565 | 3.96 |
| MCI | 0.607 | 2.60 |
| CBR | 0.568 | 0.49 |
| CBAR | 0.630 | 0.47 |
| CRR | 0.563 | 0.55 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bökeler, U.; Liener, U.; Vogeley, N.; Mayer, B.; Horsch, C.; Tröster, F.; Eschbach, D.; Ruchholtz, S.; Knauf, T. Value of Proximal Femur Geometry in Predicting Occult Hip Fracture. Medicina 2023, 59, 1987. https://doi.org/10.3390/medicina59111987
Bökeler U, Liener U, Vogeley N, Mayer B, Horsch C, Tröster F, Eschbach D, Ruchholtz S, Knauf T. Value of Proximal Femur Geometry in Predicting Occult Hip Fracture. Medicina. 2023; 59(11):1987. https://doi.org/10.3390/medicina59111987
Chicago/Turabian StyleBökeler, Ulf, Ulrich Liener, Nils Vogeley, Benjamin Mayer, Cornelia Horsch, Fridolin Tröster, Daphne Eschbach, Steffen Ruchholtz, and Tom Knauf. 2023. "Value of Proximal Femur Geometry in Predicting Occult Hip Fracture" Medicina 59, no. 11: 1987. https://doi.org/10.3390/medicina59111987
APA StyleBökeler, U., Liener, U., Vogeley, N., Mayer, B., Horsch, C., Tröster, F., Eschbach, D., Ruchholtz, S., & Knauf, T. (2023). Value of Proximal Femur Geometry in Predicting Occult Hip Fracture. Medicina, 59(11), 1987. https://doi.org/10.3390/medicina59111987