
Cancer Pain and Non-Invasive Brain Stimulation—A Narrative Review

Abstract
:1. Introduction
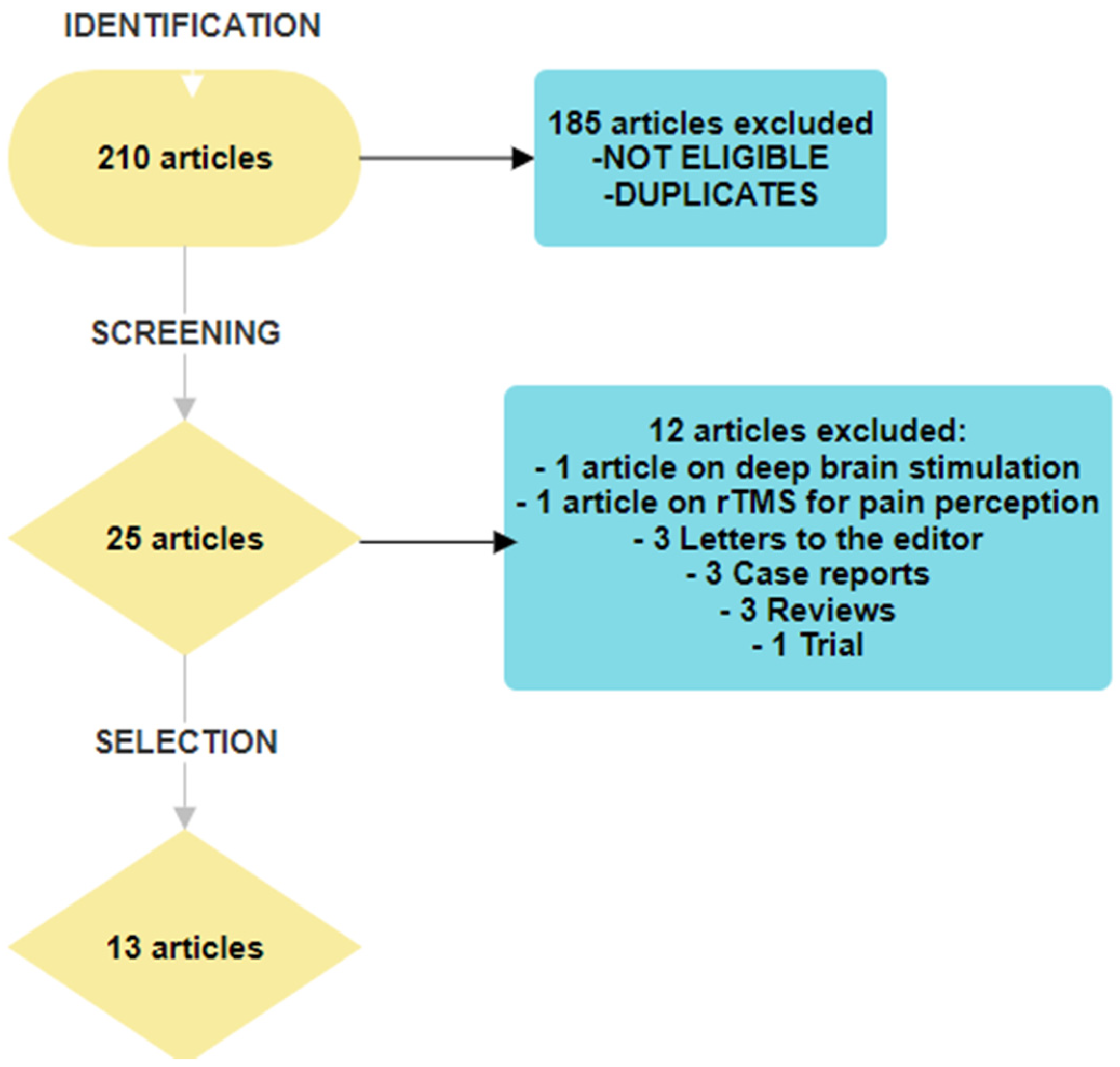
2. Materials and Methods
- Articles involving adult patients with histological confirmed cancer and cancer-related pain (both tumour- or treatment-related pain)
- Articles describing studies that used non-invasive brain stimulation, including the following:
- –
- transcranial direct current stimulation (tDCS) or
- –
- transcranial magnetic stimulation (rTMS) or
- –
- cranial electric stimulation (CES)
as a method of treating cancer-related pain.
3. Results and Discussions
- ✧
- Transcranial magnetic stimulation (rTMS)—four articles
- ✧
- Transcranial direct current stimulation (tDCS)—six articles
- ✧
- Cranial electric stimulation (CES)—three articles
3.1. Transcranial Magnetic Stimulation
3.1.1. Brief Technique Overview
3.1.2. Begining of rTMS in Cancer Pain
3.1.3. Studies Using rTMS for Cancer Pain Treatment
3.1.4. Conclusion Regarding rTMS in Cancer Pain
3.2. Transcranial Direct Current Stimulation—tDCS
3.2.1. Brief Technique Overview
3.2.2. First Data on tDCS Efficacy in Cancer Pain
3.2.3. Studies on tDCS and Cancer Pain
3.2.4. Conclusion Regarding tDCS in Cancer Pain
3.3. Cranial Electrical Stimulation
3.3.1. Brief Technique Overview
3.3.2. Studies Using CES in Cancer Pain
3.3.3. Conclusion Regarding CES in Cancer Pain
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- van den Beuken-van Everdingen, M.H.J.; Hochstenbach, L.M.J.; Joosten, E.A.J.; Tjan-Heijnen, V.C.G.; Janssen, D.J.A. Update on Prevalence of Pain in Patients with Cancer: Systematic Review and Meta-Analysis. J. Pain Symptom Manag. 2016, 51, 1070–1090.e9. [Google Scholar] [CrossRef]
- WHO. Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Smith, T.J.; O’Neil, J. Fundamentals of Cancer Pain Management. In Supportive Cancer Care; Springer: Cham, Switzerland, 2016; pp. 111–126. [Google Scholar] [CrossRef]
- Meldrum, M. The ladder and the clock: Cancer pain and public policy at the end of the twentieth century. J. Pain Symptom Manag. 2005, 29, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Mamdani, H.; Matosevic, S.; Khalid, A.B.; Durm, G.; Jalal, S.I. Immunotherapy in Lung Cancer: Current Landscape and Future Directions. Front. Immunol. 2022, 13, 823618. [Google Scholar] [CrossRef] [PubMed]
- Greco, M.T.; Roberto, A.; Corli, O.; Deandrea, S.; Bandieri, E.; Cavuto, S.; Apolone, G. Quality of Cancer Pain Management: An Update of a Systematic Review of Undertreatment of Patients with Cancer. J. Clin. Oncol. 2014, 32, 4149–4154. [Google Scholar] [CrossRef]
- Wiffen, P.J.; Wee, B.; Derry, S.; Bell, R.F.; Moore, R.A. Opioids for cancer pain—An overview of Cochrane reviews. Cochrane Database Syst. Rev. 2017, 7, CD012592. [Google Scholar] [CrossRef] [PubMed]
- Corli, O.; Floriani, I.; Roberto, A.; Montanari, M.; Galli, F.; Greco, M.T.; Caraceni, A.; Kaasa, S.; Dragani, T.A.; Azzarello, G.; et al. Are strong opioids equally effective and safe in the treatment of chronic cancer pain? A multicenter randomized phase IV ‘real life’ trial on the variability of response to opioids. Ann. Oncol. 2016, 27, 1107–1115. [Google Scholar] [CrossRef]
- Bruera, E.; Paice, J.A. Cancer pain management: Safe and effective use of opioids. Am. Soc. Clin. Oncol. Educ. Book 2015, 35, e593–e599. [Google Scholar] [CrossRef] [PubMed]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef]
- Puretić, M.B.; Demarin, V. Neuroplasticity mechanisms in the pathophysiology of chronic pain. Acta Clin. Croat. 2012, 51, 425–429. [Google Scholar] [PubMed]
- Prinsloo, S.; Gabel, S.; Lyle, R.; Cohen, L. Neuromodulation of cancer pain. Integr. Cancer Ther. 2013, 13, 30–37. [Google Scholar] [CrossRef]
- International Neuromodulation Society [Internet]. Available online: https://www.neuromodulation.com./about-neuromodulation (accessed on 9 July 2023).
- O’Connell, N.E.; Wand, B.M.; Marston, L.; Spencer, S.; DeSouza, L.H. Non-invasive brain stimulation techniques for chronic pain. Cochrane Database Syst. Rev. 2018, 4, CD008208. [Google Scholar] [CrossRef]
- Baptista, A.F.; Fernandes, A.M.B.; Sá, K.N.; Okano, A.H.; Brunoni, A.R.; Lara-Solares, A.; Iskandar, A.J.; Guerrero, C.; Amescua-García, C.; Kraychete, D.C.; et al. Latin American and Caribbean consensus on noninvasive central nervous system neuromodulation for chronic pain management (LAC2-NIN-CP). Pain Rep. 2019, 4, e692. [Google Scholar] [CrossRef]
- Fregni, F.; El-Hagrassy, M.M.; Pacheco-Barrios, K.; Carvalho, S.; Leite, J.; Simis, M.; Brunelin, J.; Nakamura-Palacios, E.M.; Marangolo, P.; Venkatasubramanian, G.; et al. Evidence-Based Guidelines and Secondary Meta-Analysis for the Use of Transcranial Direct Current Stimulation in Neurological and Psychiatric Disorders. Int. J. Neuropsychopharmacol. 2020, 24, 256–313. [Google Scholar] [CrossRef]
- Lefaucheur, J.-P.; Aleman, A.; Baeken, C.; Benninger, D.H.; Brunelin, J.; Di Lazzaro, V.; Filipović, S.R.; Grefkes, C.; Hasan, A.; Hummel, F.C.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): An update (2014–2018). Clin. Neurophysiol. 2020, 131, 474–528. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Yin, Y.; Yang, H.; Pei, Z.; Molassiotis, A. Evaluating the safety, feasibility, and efficacy of non-invasive neuromodulation techniques in chemotherapy-induced peripheral neuropathy: A systematic review. Eur. J. Oncol. Nurs. 2022, 58, 102124. [Google Scholar] [CrossRef]
- Kahan, B. Cancer pain and current theory for pain control. Phys. Med. Rehabil. Clin. N. Am. 2014, 25, 439–456. [Google Scholar] [CrossRef]
- Chwistek, M. Recent advances in understanding and managing cancer pain. F1000Research 2017, 6, 945. [Google Scholar] [CrossRef]
- Chien, Y.-J.; Chang, C.-Y.; Wu, M.-Y.; Wu, H.-C.; Horng, Y.-S. Noninvasive Brain Stimulation for Cancer Pain Management in Nonbrain Malignancy: A Meta-Analysis. Eur. J. Cancer Care 2023, 2023, 5612061. [Google Scholar] [CrossRef]
- Green, B.N.; Johnson, C.D.; Adams, A. Writing narrative literature reviews for peer-reviewed journals: Secrets of the trade. J. Chiropr. Med. 2006, 5, 101–117. [Google Scholar] [CrossRef] [PubMed]
- Turk, D.C.; Dworkin, R.H.; Burke, L.B.; Gershon, R.; Rothman, M.; Scott, J.; Allen, R.R.; Atkinson, H.J.; Chandler, J.; Cleeland, C.; et al. Developing patient-reported outcome measures for pain clinical trials: IMMPACT recommendations. Pain 2006, 125, 208–215. [Google Scholar] [CrossRef]
- Khedr, E.; Kotb, H.; Mostafa, M.; Mohamad, M.; Amr, S.; Ahmed, M.; Karim, A.; Kamal, S. Repetitive transcranial magnetic stimulation in neuropathic pain secondary to malignancy: A randomized clinical trial. Eur. J. Pain 2014, 19, 519–527. [Google Scholar] [CrossRef]
- Khedr, E.M.; Mostafa, M.G.; Kotb, H.I.; Mohamad, M.F.; Bakry, R.; Kamal, S.M.M. Effect of Repetitive Transcranial Magnetic Stimulation on Malignant Visceral Pain. Neuroenterology 2015, 3, 1–8. [Google Scholar] [CrossRef]
- Goto, Y.; Hosomi, K.; Shimokawa, T.; Shimizu, T.; Yoshino, K.; Kim, S.J.; Mano, T.; Kishima, H.; Saitoh, Y. Pilot study of repetitive transcranial magnetic stimulation in patients with chemotherapy-induced peripheral neuropathy. J. Clin. Neurosci. 2020, 73, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Chen, H.; Zhou, Y.; Tan, M.-L.; Xiong, S.-L.; Li, Y.; Ji, X.-H.; Li, Y.-S. Analgesic Effects of Repetitive Transcranial Magnetic Stimulation in Patients with Advanced Non-Small-Cell Lung Cancer: A Randomized, Sham-Controlled, Pilot Study. Front. Oncol. 2022, 12, 840855. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, N.M.; Abdelhameed, K.M.; Kamal, S.M.M.; Khedr, E.M.H.; Kotb, H.I.M. Effect of Transcranial Direct Current Stimulation of the Motor Cortex on Visceral Pain in Patients with Hepatocellular Carcinoma. Pain Med. 2017, 19, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Stamenkovic, D.M.; Mladenovic, K.; Rancic, N.; Cvijanovic, V.; Maric, N.; Neskovic, V.; Zeba, S.; Karanikolas, M.; Ilic, T.V. Effect of Transcranial Direct Current Stimulation Combined with Patient-Controlled Intravenous Morphine Analgesia on Analgesic Use and Post-Thoracotomy Pain. A Prospective, Randomized, Double-Blind, Sham-Controlled, Proof-of-Concept Clinical Trial. Front. Pharmacol. 2020, 11, 125. [Google Scholar] [CrossRef] [PubMed]
- Hanna, M.H.Z.; RezkAllah, S.S.; Shalaby, A.S.; Hanna, M.Z. Efficacy of transcranial direct current stimulation (tDCS) on pain and shoulder range of motion in post-mastectomy pain syndrome patients: A randomized-control trial. Bull. Fac. Phys. Ther. 2023, 28, 7. [Google Scholar] [CrossRef]
- Lyon, D.E.; Schubert, C.; Taylor, A.G. Pilot study of cranial stimulation for symptom management in breast cancer. Oncol. Nurs. Forum 2010, 37, 476–483. [Google Scholar] [CrossRef]
- Lyon, D.; Kelly, D.; Walter, J.; Bear, H.; Thacker, L.; Elswick, R.K. Randomized sham controlled trial of cranial microcurrent stimulation for symptoms of depression, anxiety, pain, fatigue and sleep disturbances in women receiving chemotherapy for early-stage breast cancer. SpringerPlus 2015, 4, 369. [Google Scholar] [CrossRef]
- Yennurajalingam, S.; Kang, D.-H.; Hwu, W.-J.; Padhye, N.S.; Masino, C.; Dibaj, S.S.; Liu, D.D.; Williams, J.L.; Lu, Z.; Bruera, E. Cranial Electrotherapy Stimulation for the Management of Depression, Anxiety, Sleep Disturbance, and Pain in Patients with Advanced Cancer: A Preliminary Study. J. Pain Symptom Manag. 2017, 55, 198–206. [Google Scholar] [CrossRef]
- Boivie, J.; Meyerson, B.A. A correlative anatomical and clinical study of pain suppression by deep brain stimulation. Pain 1982, 13, 113–126. [Google Scholar] [CrossRef] [PubMed]
- Kakigi, R.; Inui, K.; Tamura, Y. Electrophysiological studies on human pain perception. Clin. Neurophysiol. 2005, 116, 743–763. [Google Scholar] [CrossRef] [PubMed]
- Xiong, H.-Y.; Zheng, J.-J.; Wang, X.-Q. Non-invasive Brain Stimulation for Chronic Pain: State of the Art and Future Directions. Front. Mol. Neurosci. 2022, 15, 888716. [Google Scholar] [CrossRef]
- Nizard, J.; Levesque, A.; Denis, N.; De Chauvigny, E.; Lepeintre, A.; Raoul, S.; Labat, J.-J.; Bulteau, S.; Maillard, B.; Buffenoir, K.; et al. Interest of repetitive transcranial magnetic stimulation of the motor cortex in the management of refractory cancer pain in palliative care: Two case reports. Palliat. Med. 2015, 29, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Larrea, L.; Peyron, R. Motor cortex stimulation for neuropathic pain: From phenomenology to mechanisms. NeuroImage 2007, 37, S71–S79. [Google Scholar] [CrossRef]
- Maarrawi, J.; Peyron, R.; Mertens, P.; Costes, N.; Magnin, M.; Sindou, M.; Laurent, B.; Garcia-Larrea, L. Motor cortex stimulation for pain control induces changes in the endogenous opioid system. Neurology 2007, 69, 827–834. [Google Scholar] [CrossRef]
- Nijs, J.; Meeus, M.; Versijpt, J.; Moens, M.; Bos, I.; Knaepen, K.; Meeusen, R. Brain-derived neurotrophic factor as a driving force behind neuroplasticity in neuropathic and central sensitization pain: A new therapeutic target? Expert Opin. Ther. Targets 2014, 19, 565–576. [Google Scholar] [CrossRef]
- Boland, E.G.; Selvarajah, D.; Hunter, M.; Ezaydi, Y.; Tesfaye, S.; Ahmedzai, S.H.; Snowden, J.A.; Wilkinson, I.D. Central pain processing in chronic chemotherapy-induced peripheral neuropathy: A functional magnetic resonance imaging study. PLoS ONE 2014, 9, e96474. [Google Scholar] [CrossRef]
- Lefaucheur, J.-P.; Drouot, X.; Cunin, P.; Bruckert, R.; Lepetit, H.; Créange, A.; Wolkenstein, P.; Maison, P.; Keravel, Y.; Nguyen, J.-P. Motor cortex stimulation for the treatment of refractory peripheral neuropathic pain. Brain 2009, 132, 1463–1471. [Google Scholar] [CrossRef]
- Cha, M.; Um, S.W.; Kwon, M.; Nam, T.S.; Lee, B.H. Repetitive motor cortex stimulation reinforces the pain modulation circuits of peripheral neuropathic pain. Sci. Rep. 2017, 7, 7986. [Google Scholar] [CrossRef]
- Attal, N.; Poindessous-Jazat, F.; De Chauvigny, E.; Quesada, C.; Mhalla, A.; Ayache, S.S.; Fermanian, C.; Nizard, J.; Peyron, R.; Lefaucheur, J.-P.; et al. Repetitive transcranial magnetic stimulation for neuropathic pain: A randomized multicentre sham-controlled trial. Brain 2021, 144, 3328–3339. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, J.-P.; André-Obadia, N.; Poulet, E.; Devanne, H.; Haffen, E.; Londero, A.; Cretin, B.; Leroi, A.-M.; Radtchenko, A.; Saba, G.; et al. Recommandations françaises sur l’utilisation de la stimulation magnétique transcrânienne répétitive (rTMS): Règles de sécurité et indications thérapeutiques. Neurophysiol. Clin. 2011, 41, 221–295. [Google Scholar] [CrossRef]
- Lefaucheur, J.-P.; André-Obadia, N.; Antal, A.; Ayache, S.S.; Baeken, C.; Benninger, D.H.; Cantello, R.M.; Cincotta, M.; de Carvalho, M.; De Ridder, D.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS). Clin. Neurophysiol. 2014, 125, 2150–2206. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.D.J.P. Value of Repetitive Transcranial Magnetic Stimulation of the Motor Cortex in the Management of Refractory Cancer Pain in Palliative Care: A Case Report. J. Palliat. Care Med. 2013, 3, 147. [Google Scholar] [CrossRef]
- Antal, A.; Alekseichuk, I.; Bikson, M.; Brockmöller, J.; Brunoni, A.; Chen, R.; Cohen, L.; Dowthwaite, G.; Ellrich, J.; Flöel, A.; et al. Low intensity transcranial electric stimulation: Safety, ethical, legal regulatory and application guidelines. Clin. Neurophysiol. 2017, 128, 1774–1809. [Google Scholar] [CrossRef] [PubMed]
- Woods, A.J.; Antal, A.; Bikson, M.; Boggio, P.S.; Brunoni, A.R.; Celnik, P.; Cohen, L.G.; Fregni, F.; Herrmann, C.S.; Kappenman, E.S.; et al. A technical guide to tDCS, and related non-invasive brain stimulation tools. Clin. Neurophysiol. 2016, 127, 1031–1048. [Google Scholar] [CrossRef]
- DaSilva, A.F.; Truong, D.Q.; DosSantos, M.F.; Toback, R.L.; Datta, A.; Bikson, M. State-of-art neuroanatomical target analysis of high-definition and conventional tDCS montages used for migraine and pain control. Front. Neuroanat. 2015, 9, 89. [Google Scholar] [CrossRef]
- Hu, X.-S.; Fisher, C.A.; Munz, S.M.; Toback, R.L.; Nascimento, T.D.; Bellile, E.L.; Rozek, L.; Eisbruch, A.; Worden, F.P.; Danciu, T.E.; et al. Feasibility of Non-invasive Brain Modulation for Management of Pain Related to Chemoradiotherapy in Patients with Advanced Head and Neck Cancer. Front. Hum. Neurosci. 2016, 10, 466. [Google Scholar] [CrossRef]
- Dos Santos, M.F.; Love, T.M.; Martikainen, I.K.; Nascimento, T.D.; Fregni, F.; Cummiford, C.; Deboer, M.D.; Zubieta, J.-K.; DaSilva, A.F.M. Immediate effects of tDCS on the μ-opioid system of a chronic pain patient. Front. Psychiatry 2012, 3, 93. [Google Scholar] [CrossRef]
- Lefaucheur, J.-P.; Antal, A.; Ayache, S.S.; Benninger, D.H.; Brunelin, J.; Cogiamanian, F.; Cotelli, M.; De Ridder, D.; Ferrucci, R.; Langguth, B.; et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin. Neurophysiol. 2016, 128, 56–92. [Google Scholar] [CrossRef]
- Silva, G.; Miksad, R.; Freedman, S.D.; Pascual-Leone, A.; Jain, S.; Gomes, D.L.; Amancio, E.J.; Boggio, P.S.; Correa, C.F.; Fregni, F. Treatment of cancer pain with noninvasive brain stimulation. J. Pain Symptom Manag. 2007, 34, 342–345. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, J.-P.; Esnault, J.; Suarez, A.; Dixneuf, V.; Lepeintre, A.; Levesque, A.; Meignier, M.; Lefaucheur, J.-P.; Nizard, J. Value of transcranial direct-current stimulation of the motor cortex for the management of refractory cancer pain in the palliative care setting: A case report. Clin. Neurophysiol. 2016, 127, 2773–2774. [Google Scholar] [CrossRef]
- Nguyen, J.-P.; Gaillard, H.; Suarez, A.; Terzidis-Mallat, É.; Constant-David, D.; Van Langhenhove, A.; Evin, A.; Malineau, C.; Tan, S.V.O.; Mhalla, A.; et al. Bicentre, randomized, parallel-arm, sham-controlled trial of transcranial direct-current stimulation (tDCS) in the treatment of palliative care patients with refractory cancer pain. BMC Palliat. Care 2023, 22, 15. [Google Scholar] [CrossRef]
- Kamal, S.M.; Elhusseini, N.M.; Sedik, M.F.; Mohamad, M.F.; Khedr, E.M.H.; Kotb, H.I.M. Effect of Transcranial Direct Current Brain Stimulation of the Motor Cortex on Chemotherapy-Induced Nausea and Vomiting in Female Patients with Breast Cancer. Pain Med. 2021, 23, 571–578. [Google Scholar] [CrossRef] [PubMed]
- Lowson, E.; Holmes, L.; Addingtonhall, J.; Grande, G.; Payne, S.; Seymour, J.; Hanratty, B. Abstracts of the 7th World Research Congress of the European Association for Palliative Care (EAPC). Palliat. Med. 2012, 26, 384–674. [Google Scholar] [CrossRef]
- Moura, B.d.S.; Hu, X.-S.; DosSantos, M.F.; DaSilva, A.F. Study Protocol of tDCS Based Pain Modulation in Head and Neck Cancer Patients Under Chemoradiation Therapy Condition: An fNIRS-EEG Study. Front. Mol. Neurosci. 2022, 15, 859988. [Google Scholar] [CrossRef] [PubMed]
- Painless Project. Horizon-HLTH-2021-DISEASE-04(2022-2027) Project ID: 101057367. [INTERNET]. Available online: https://palliativeprojects.ru/painless/ (accessed on 18 April 2023).

{kind=link}
| First author | Khedr [24] | Khedr [25] | Goto [26] | Tang [27] | ||||
| Country of origin | Egipt | Egipt | Japan | China | ||||
| Year of publication | 2015 | 2015 | 2020 | 2022 | ||||
| Type of study | Randomized clinical trial. | Preliminary randomized trial. | Pilot randomized controlled, single-blind, four-way crossover study. | Randomized double-blind, parallel-group, sham-controlled, clinical trial. | ||||
| IMMPACT Recommendations Score | 4/6 | 4/6 | 3/6 | 4/6 | ||||
| Type of pain | Neuropathic pain with a score ≥ 4 on the Douleur Neuropathique 4 questionnaire. | Visceral pain. | Neuropathic pain with a minimum grade 2 severity based on the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE, version 4.0) scale. | Lung cancer pain. | ||||
| Inclusion criteria |
|
|
|
| ||||
| Exclusion criteria |
|
|
|
| ||||
| Period of study | January 2010–May 2013 | January 2010–January 2012 | April 2015–October 2016 | January 2020–March2021 | ||||
| Study patients | Intervention group | Control group | Intervention group | Control group | Pilot study, no control group | Intervention group | Control group | |
| Initial number of patients | 17 | 17 | 17 | 17 | 11 | 21 | 21 | |
| Final number of patients | 15 | 15 | 15 | 15 | 11 | 20 | 19 | |
| Losses (no/%) | 2 (11.7%) | 2 (11.7%) | 2 (11.7%) | 2 (11.7%) | 0 | 1 (4.7%) | 2 (9.5%) | |
| Age (years) mean ± SD | 47 ± 9.2 | 48 ± 9.7 | 51 ± 9.7 | 57.8 ± 3.9 | 64.8 ± 7.8 | 58.5 ± 8.9 | 59.6 ± 7.7 | |
| Gender | ||||||||
| Male | 1 | 2 | 10 | 8 | 0 | 12 | 10 | |
| Female | 16 | 15 | 7 | 9 | 11 | 8 | 9 | |
| Duration of disease (months) | 15.4 ± 15.9 | 16.8 ± 16.3 | 15 ± 19.6 | 12.3 ± 14.9 | Unknown | Unknown | ||
| Oncologic pathology/Cancer (no patients) | Post mastectomy 14 Soft tissue sarcoma 1 Giant cell glioma 1 Femoral mass 1 | Post mastectomy 15 Soft tissue sarcoma 2 | Pancreas 4 Hepatic 7 Gall bladder 2 Stomach 1 NH lymphoma 1 Peritoneal mesothelioma 1 | Pancreas 5 Hepatic 6 Gall Bladder 2 Stomach 2 Oesophagus 1 NH lymphoma 1 | Breast 9 Gynecologic 2 | Lung cancer 42 | ||
| Treatment analgesic | Tramadol 100 mg bid Pregabalin 75 mg bid Gabapentin 400 mg bid Amitriptyline 25 mg bid | Tramadol 100 mg bid Pregabalin 75 mg bid Gabapentin 400 mg bid Amitriptyline 25 mg bid | Tramadol 100 mg bid Scopolamina 20 mg tid Amitriptilina 25 mg bid | Tramadol 100 mg bid Scopolamina 20 mg tid Amitriptilina 25 mg bid | Unknown | Morphine sulfate controlled-release tablets or oxycodone hydrochloride sustained-release tablets | ||
| STIMULATION DETAILS | Target/ Coil type/ Orientation/ Stimulation Frequency/ Intensity/ Time/ | Contralateral to pain M1 hand; F8 coil/AP; 20 Hz (10 s, 10 trains, with intertrain interval 30 s); 80% RMT; 10 min. | Contralateral side of pain M1 hand or dominant hemishpere for epigastric pain; F8 coil/AP; 20 Hz (10 s, 10 trains, with intertrain of 30 s); 80% RMT; 10 min. | 5 Hz, 10 s, 10 trains, with intertrain of 50 s, F8 coil; Stimulation types: 1. PA 90%: PA coil direction with 90% RMT target M1 stimulation, 2. PA 100%: PA coil direction with 100% RMT target M1 stimulation, 3. Ipsilateral PA 90%: PA coil direction with 90% RMT stimulation ipsilateral to the target M1 (if the target M1 was “the right-hand area”, then ipsilateral target M1 was “the right leg area”), 4. LM 90%: LM coil direction with 90% RMT target M1 stimulation. | DLPFC left side; F8 coil; 10 Hz (15 pulse trains (1.5 s), with intertrain of 3 s); 80% RMT. | |||
| No of pulses/sessions No of sessions | 2000 pulses; 10 sessions; daily; 2 weeks. | 2000 pulses; 10 session; daily; 2 weeks. | 500 pulses; 4 sessions in 2 months. | 1500 pulses; 15 sessions; daily; 3 weeks. | ||||
| Endpoints | Primary VAS after 10th session and 1 month later; Secondary VDS, LANSS, and HAM-D after 10th session and 1 month later. | Primary VAS after 10th session and 1 month later; Secondary VDS and HAM-D after 10th session and 1 month later; Serum Dynorphin. | P-VAS; SF-MPQ2; D-VAS. | NRS; OME, Quality of life; HAM-A; HAM-D. | ||||
| Adverse events | No | No | No | two patients with transient scalp numbness or facial muscle twitching | ||||
| Results |
|
|
|
| ||||
| First author | Ibrahim [28] | Stamenkovic [29] | Hanna [30] | ||||
| Country of origin | Egipt | Serbia | Egipt | ||||
| Year of publication | 2018 | 2020 | 2022 | ||||
| Type of study | Prospective, randomized, double-blind sham-controlled. | Prospective, randomized, double-blind sham-controlled. | Prospective, randomized, sham-controlled. | ||||
| IMMPACT Recommendations Score | 4/6 | 4/6 | 3/6 | ||||
| Type of pain | HCC; Chronic abdominal/visceral pain. | Lung cancer; Acute pain post thoracotomy. | Post mastectomy pain syndrome scored ≥ 4 in DN4. | ||||
| Inclusion criteria |
|
|
| ||||
| Exclusion criteria |
|
|
| ||||
| Period of study | April 2015 to February 2016 | 15 June 2016 to 27 March 2018. | Unknown | ||||
| Study patients | Intervention group | Control group | Intervention group | Control group | Intervention grpup | Control group | |
| Initial number of patients | 24 | 24 | 30 | 31 | 20 | 18 | |
| Final number of patients | 20 | 20 | 27 | 28 | 15 | 15 | |
| Losses (no/%) | 4 (16%) | 4 (16%) | 3 (10%) | 3 (9.6%) | 5 (20%) | 3 (6%) | |
| Age (years) mean ± SD | 58.9 ± 5.6 | 56.85 ± 9.16 | 61.44 ± 7.98 | 61.89 ± 5.79 | 40.5 ± 2.8 | 40.2 ± 3.1 | |
| Gender | |||||||
| Male | 14 | 13 | 16 | 23 | 0 | 0 | |
| Female | 6 | 7 | 11 | 5 | 15 | 15 | |
| Oncologic pathology | HCC | Lung cancer | Breast cancer | ||||
| Treatment analgesic | Tramadol hydrochloride 50 mg twice daily. | Unknown | Unknown | ||||
| Endpoints | VAS; VDS; HAM-D. | Morphine dose; VAS—pain rest, movement, and couch; VAS—anxiety; Beck depression inventory; PRO. | VAS; Beck depression inventory; ROM. | ||||
| Stimulation details | Anode location | Primary motor cortex of the contralateral most painful abdominal area. | Left primary motor cortex. | Bilateral M1. | |||
| Cathode location | Contralateral supraorbital region. | Contralateral supraorbital region. | Supraorbital region. | ||||
| Stimulation details | Duration: 10 sessions/2 weeks; | Duration: 5 daily sessions; | Duration: 5 daily sessions; | ||||
| Intensity: 2 mA; | Intensity: 1.2 mA; | Intensity: 2 mA; | |||||
| Duration of a session: 30 min; | Duration of a session: 20 min; | Duration of a session: 20 min × 2 (20 min each side); | |||||
| Device: neuroConn Germany. | Device: neuroelectrics. | Device: unknown. | |||||
| Side effects | Slight burning sensation in three patients; Skin redness under the active electrode in two patients. | None declared. | None declared. | ||||
| Outcome |
|
|
| ||||
| First author | Lyon [31] | Lyon [32] | Yennurajalingam [33] | |||
| Country of origin | USA | USA | USA | |||
| Year of publication | 2010 | 2015 | 2018 | |||
| Type of study | Pilot feasibility study. | Randomized, sham-controlled trial. | Preliminary study, one group, open label. | |||
| IMMPACT Recommendation Score | 4/6 | 4/6 | 4/6 | |||
| Inclusion criteria |
|
|
| |||
| Exclusion criteria |
|
|
| |||
| Stimulation details | Alpha-Stim Stress Control System | Alpha-Stim Stress Control System | Alpha-Stim M | |||
| Intensity: 100 μA; | Intensity: 100 μA; | Intensity: 100 μA; | ||||
| Frequency: 0.5 Hz; | Frequency: 0.5 Hz; | Frequency: 0.5 Hz; | ||||
| Duration: 60 min; | Duration: 60 min; | Duration: 60 min; | ||||
| Period of stimulation | Daily for 6–8 weeks depending on chemotherapy schedule. | Daily for the chemotherapy period and 2 weeks after; (6–32 weeks). | Daily for 4 weeks. | |||
| Outcomes | Feasability; HADS; BPI; BFI; GSDS. | HADS; BPI; BFI; GSDS. | ESAS; HADS; PSQI; BPI; MDAS; NCCN Distress Thermometer Safety. | |||
| Groups | Active | Sham | Standard | Active | Sham | Not sham-controlled |
| Number of patients initially | 36 | 84 | 83 | 36 | ||
| Number of patients analyzed | 13 | 10 | 12 | 77 | 75 | 33 |
| Losses number (%) | 0% | 0% | 0% | 7 (8.33%) | 8 (10.6%) | 3 (8.33%) |
| Age (years) ± SD | 47.54 ± 9.1 | 46.6 ± 5.64 | 50.5 ± 18.28 | 51.04 ± 1.21 | 51.91 ± 0.97 | 59 |
| Results |
|
|
| |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiriac, V.-F.; Ciurescu, D.; Moșoiu, D.-V. Cancer Pain and Non-Invasive Brain Stimulation—A Narrative Review. Medicina 2023, 59, 1957. https://doi.org/10.3390/medicina59111957
Chiriac V-F, Ciurescu D, Moșoiu D-V. Cancer Pain and Non-Invasive Brain Stimulation—A Narrative Review. Medicina. 2023; 59(11):1957. https://doi.org/10.3390/medicina59111957
Chicago/Turabian StyleChiriac, Valentina-Fineta, Daniel Ciurescu, and Daniela-Viorica Moșoiu. 2023. "Cancer Pain and Non-Invasive Brain Stimulation—A Narrative Review" Medicina 59, no. 11: 1957. https://doi.org/10.3390/medicina59111957
APA StyleChiriac, V.-F., Ciurescu, D., & Moșoiu, D.-V. (2023). Cancer Pain and Non-Invasive Brain Stimulation—A Narrative Review. Medicina, 59(11), 1957. https://doi.org/10.3390/medicina59111957