
Epidemiology and Risk Factors of Table-Tennis-Related Injuries: Findings from a Scoping Review of the Literature

 ,
,  ,
,  , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
- ▸
- P (population): male and female TT players at any age category and competitive level; in case the study also included other sports and disciplines, only data concerning TT players were extracted and retained in the present scoping review. If this was not possible (i.e., data were presented aggregated and were hard to disaggregate), the article was excluded;
- ▸
- E (exposure): reporting sports-related injuries;
- ▸
- C (comparison/comparator): between male and female TT players, various age categories, competitive levels, etc.;
- ▸
- O: the type of injury, its epidemiology (incidence/prevalence rate), and determinants of injuries;
- ▸
- S (study design): original peer-reviewed articles of any type (clinical case report, case series, observational study—incidence, prevalence or case-control investigation, randomized controlled trial, etc.) except for expert commentaries, editorials, and review articles, which were excluded but were scanned for potential articles to be included in the present scoping review;
- ▸
- Languages: all languages available.
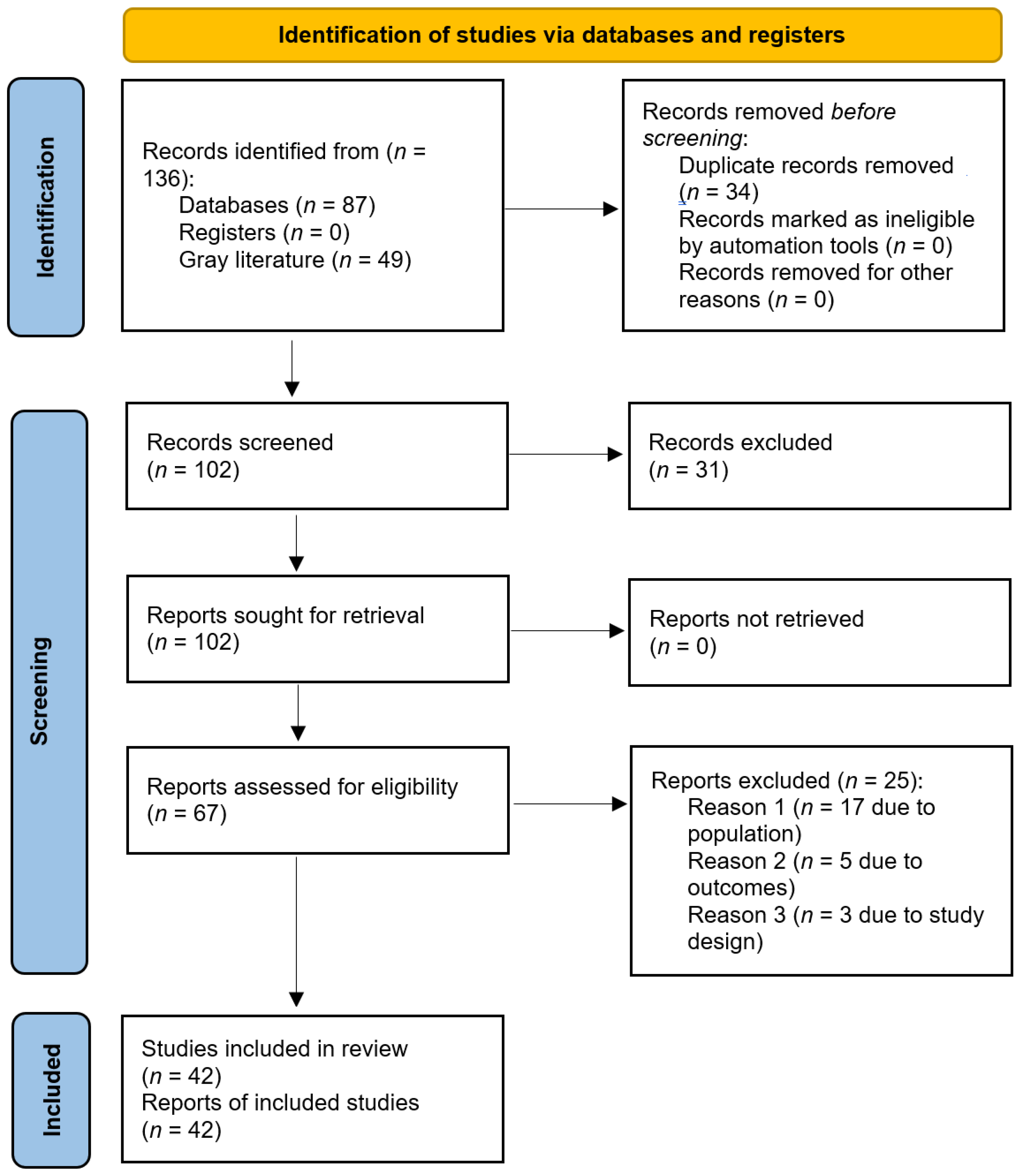
3. Results
3.1. Risk of Bias Assessment
3.2. Injury Rate
3.3. Orthopedic Injuries by Competitive Level, Gender, and Type of Contest (Training vs. Competition), and Location of Injuries
3.4. Dental and Facial Injuries
3.5. Dermatological Lesions
3.6. Ocular Lesions
3.7. Neurological Lesions and TT-Related Tumors
3.8. Injury Risk Perception and Risk Management Strategies
4. Discussion
Strengths and Limitations of the Present Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- de la Torre Combarros, A.; Carrasco Páez, L.; Pradas de la Fuente, F. Injury Incidence among Young Table Tennis Players during 2005 Spanish National Championship. In Proceedings of the 10th International Table Tennis Sports Science Congress, Zagreb, Croatia, 18–20 May 2007; Available online: http://www.ittf.com/ittf_science/SSCenter/10ITTSSC_Zagreb_07/docs/08-de%20la%20torre_injury%20incidence.pdf (accessed on 31 December 2021).
- Kondrič, M.; Zagatto, A.M.; Sekulić, D. The physiological demands of table tennis: A review. J. Sport. Sci. Med. 2013, 12, 362–370. [Google Scholar]
- Zagatto, A.M.; De Mello Leite, J.V.; Papoti, M.; Beneke, R. Energetics of table tennis and table tennis–specific exercise testing. Int. J. Sport. Physiol. Perform. 2016, 11, 1012–1017. [Google Scholar] [CrossRef] [PubMed]
- Zagatto, A.M.; Morel, E.A.; Gobatto, C.A. Physiological responses and characteristics of table tennis matches determined in official tournaments. J. Strength Cond. Res. 2010, 24, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.H.; Haskell, W.L.; Raven, P.B. Classification of sports. J. Am. Coll. Cardiol. 1994, 24, 864–866. [Google Scholar] [CrossRef]
- Le Floch, A.; Vidailhet, M.; St, C.F.-R.; Grabli, D.; Mayer, J.-M.; Gonce, M.; Broussolle, E.; Roze, E. Table tennis dystonia. Mov. Disord. 2010, 25, 394–397. [Google Scholar] [CrossRef]
- Correa Mesa, J.F. Prevalencia de Lesiones Osteomusculares en Tenimesistas de alto Rendimiento de la Federación Colombiana de Tenis de Mesa. 2014. Available online: https://repositorio.unal.edu.co/bitstream/handle/unal/56085/1037576078.pdf?sequence=1&isAllowed=y (accessed on 31 December 2021).
- Padulo, J.; Di Giminiani, R.; Iacono, A.D.; Zagatto, A.M.; Migliaccio, G.M.; Grgantov, Z.; Ardigò, L.P. Lower arm muscle activation during indirect-localized vibration: The influence of skill levels when applying different acceleration loads. Front. Physiol. 2016, 7, 242. [Google Scholar] [CrossRef]
- Zagatto, A.M.; Gobatto, C.A. Relationship between anaerobic parameters provided from MAOD and critical power model in specific table tennis test. Int. J. Sport. Med. 2012, 33, 613–620. [Google Scholar] [CrossRef]
- Zagatto, A.M.; Papoti, M.; Gobatto, C.A. Anaerobic capacity may not be determined by critical power model in elite table tennis players. J. Sport. Sci. Med. 2008, 7, 54–59. [Google Scholar]
- Martinent, G.; Ferrand, C. A Naturalistic study of the directional interpretation process of discrete emotions during high-stakes table tennis matches. J. Sport Exerc. Psychol. 2009, 31, 318–336. [Google Scholar] [CrossRef]
- Martinent, G.; Ferrand, C. A field study of discrete emotions: Athletes’ cognitive appraisals during competition. Res. Q. Exerc. Sport 2015, 86, 51–62. [Google Scholar] [CrossRef]
- Barczyk-Pawelec, K.; Bankosz, Z.; Derlich, M. Body postures and asymmetries in frontal and transverse planes in the trunk area in table tennis players. Biol. Sport 2012, 29, 127–132. [Google Scholar] [CrossRef]
- Folorunso, O.M.; Ademola, O.A. The playing posture, activities and health of the table tennis player. Int. J. Table Tennis Sci. 2010, 6, 99–104. [Google Scholar]
- Rajabi, R.; Johnson, G.M.; Alizadeh, M.H.; Meghdadi, N. Radiographic knee osteoarthritis in ex-elite table tennis players. BMC Musculoskelet. Disord. 2012, 13, 12. [Google Scholar] [CrossRef]
- McAfee, R.E. Table Tennis: Steps to Success; Human Kinetics: Champaign, IL, USA, 2009. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Nillius, S.A.; Nilsson, B.E.; Westlin, N.E.; Niixius, S.A. The incidence of Achilles tendon rupture. Acta Orthop. Scand. 1976, 47, 118–121. [Google Scholar] [CrossRef]
- Shimazaki, T.; Almeida, E.d.; Vanderlei, F.M.; Cintra Filho, D.d.A.; Vanderlei, L.C.M.; Pastre, C.M.; Bastos, F.N. Exploração de fatores de risco para lesões desportivas em atletas de tênis de mesa. Fisioter. Pesqui. 2012, 19, 158–164. [Google Scholar] [CrossRef]
- Correa-Mesa, J.F.; Correa-Morales, J.C. Prevalencia de lesiones musculoesqueléticas en jugadores de tenis de mesa. Rev. Cienc. Bioméd. 2020, 5, 48–54. [Google Scholar] [CrossRef]
- Fong, D.T.-P.; Man, C.-Y.; Yung, P.S.-H.; Cheung, S.-Y.; Chan, K.-M. Sport-related ankle injuries attending an accident and emergency department. Injury 2008, 39, 1222–1227. [Google Scholar] [CrossRef]
- Di Carlo, M.; Formigoni, M.; Peña, S.; Fernández Palazzi, F. Biomecánica y lesiones del hombro aplicadas al tenis de mesa. Cent. Méd. 1997, 42, 18–21. [Google Scholar]
- Fernández Córdova, L.S.; Barrios González, J. Lesiones más frecuentes en atletas del equipo nacional cubano de tenis de mesa en el período 2005–2008. Rev. Digital B. Aires 2010, 151. [Google Scholar]
- Majewski, M.; Susanne, H.; Klaus, S. Epidemiology of athletic knee injuries: A 10-year study. Knee 2006, 13, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Lo, Y.P.; Hsu, Y.C.; Chan, K.M. Epidemiology of shoulder impingement in upper arm sports events. Br. J. Sport. Med. 1990, 24, 173–177. [Google Scholar] [CrossRef]
- Kondric, M.; Matković, B.R.; Furjan-Mandić, G.; Hadzić, V.; Dervisević, E. Injuries in racket sports among Slovenian players. Coll. Antropol. 2011, 35, 413–417. [Google Scholar] [PubMed]
- Junge, A.; Engebretsen, L.; Mountjoy, M.L.; Alonso, J.M.; Renström, P.A.F.H.; Aubry, M.J.; Dvorak, J. Sports injuries during the summer Olympic games 2008. Am. J. Sport. Med. 2009, 37, 2165–2172. [Google Scholar] [CrossRef] [PubMed]
- Engebretsen, L.; Soligard, T.; Steffen, K.; Alonso, J.M.; Aubry, M.; Budgett, R.; Dvorak, J.; Jegathesan, M.; Meeuwisse, W.H.; Mountjoy, M.; et al. Sports injuries and illnesses during the London Summer Olympic Games 2012. Br. J. Sport. Med. 2013, 47, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Linderoth, M. Kan man bli Skadad i Pingis?: En Studie om Förekomsten av Skador i Svensk Elitbordtennis. Institutionen för Idrotts-och Hälsovetenskap. 2006. Available online: http://www.diva-portal.org/smash/get/diva2:852/FULLTEXT01.pdf (accessed on 31 December 2021).
- Pieper, H.-G.; Quack, G.; Krahl, H. Impingement of the rotator cuff in athletes caused by instability of the shoulder joint. Knee Surg. Sport. Traumatol. Arthrosc. 1993, 1, 97–99. [Google Scholar] [CrossRef]
- Nicolini, A.P.; De Carvalho, R.T.; Matsuda, M.M.; Filho, J.S.; Cohen, M. Common injuries in athletes’ knee: Experience of a specialized center. Acta Ortop. Bras. 2014, 22, 127–131. [Google Scholar] [CrossRef]
- Li, Y. Tenosynovitis of table tennis players and its treatment. Sport. Sci./Tiyu Kexue 1996, 16, 67–70. [Google Scholar]
- Pintore, E.; Maffulli, N. Osteochondritis dissecans of the lateral humeral condyle in a table tennis player. Med. Sci. Sport. Exerc. 1991, 23, 889–891. [Google Scholar] [CrossRef]
- Ron, D.; Alkalay, D.; Torok, G. Simultaneous closed dislocation of both interphalangeal joints in one finger. J. Trauma Inj. Infect. Crit. Care 1983, 23, 66–67. [Google Scholar] [CrossRef] [PubMed]
- Dufek, P.; Ostendorf, U.; Thormählen, F. Stress fracture of the ulna in a table tennis player. Sportverletz. Sportschaden Organ Der Ges. Fur Orthop.-Traumatol. Sportmed. 1999, 13, 62–64. [Google Scholar] [CrossRef] [PubMed]
- Petschnig, R.; Wurnig, C.; Rosen, A.; Baron, R. Stress fracture of the ulna in a female table tennis tournament player. J. Sport. Med. Phys. Fit. 1997, 37, 225–227. [Google Scholar]
- Laoruengthana, A.; Poosamsai, P.; Fangsanau, T.; Supanpaiboon, P.; Tungkasamesamran, K. The epidemiology of sports injury during the 37th Thailand National Games 2008 in Phitsanulok. J. Med. Assoc. Thail. 2009, 92, S204–S210. [Google Scholar]
- Hill, C.M.; Crosher, R.F.; Mason, D.A. Dental and facial injuries following sports accidents: A study of 130 patients. Br. J. Oral Maxillofac. Surg. 1985, 23, 268–274. [Google Scholar] [CrossRef]
- Andrade, R.A.; Evans, P.L.S.; Almeida, A.L.S.; Silva, J.D.J.R.D.; Guedes, A.M.L.; Guedes, F.R.; Ranalli, D.N.; Modesto, A.; Tinoco, E.M.B. Prevalence of dental trauma in Pan American Games athletes. Dent. Traumatol. 2010, 26, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Scott, M.J., Jr.; Scott, M.J., 3rd. Ping pong patches. Cutis 1989, 43, 363–364. [Google Scholar]
- Barrell, G.V.; Cooper, P.J.; Elkington, A.R.; Macfadyen, J.M.; Powell, R.G.; Tormey, P. Squash ball to eye ball: The likelihood of squash players incurring an eye injury. Br. Med. J. (Clin. Res. Ed.) 1981, 283, 893–895. [Google Scholar] [CrossRef]
- Chandran, S. Ocular hazards of playing badminton. Br. J. Ophthalmol. 1974, 58, 757–760. [Google Scholar] [CrossRef]
- Jeffers, J.B. The role of organized ophthalmology in preventing ocular injuries. Int. Ophthalmol. Clin. 1988, 28, 255–258. [Google Scholar] [CrossRef]
- Kelly, S.; Nolan, J. Eye injuries in organised sport in a rural area. Br. J. Ophthalmol. 1983, 67, 837–839. [Google Scholar] [CrossRef] [PubMed]
- Lovell, G. The diagnosis of chronic groin pain in athletes: A review of 189 cases. Aust. J. Sci. Med. Sport 1995, 27, 76–79. [Google Scholar] [PubMed]
- Shida, Y.; Shida, S.; Suzuki, S.; Murakami, H.; Yuza, N. Injuries and systemic disorders of table tennis players: Results of a survey. Int. J. Table Tennis Sci. 1992, 1, 11–16. [Google Scholar]
- Shida, Y.; Shida, S.; Suzuki, S.; Murakami, H.; Youza, N. Injuries and systematic disorders of table tennis players. Int. J. Table Tennis Sci. 1994, 2, 121–122. [Google Scholar]
- Soligard, T.; Steffen, K.; Palmer, D.; Alonso, J.M.; Bahr, R.; Lopes, A.; Dvorak, J.; Grant, M.-E.; Meeuwisse, W.; Mountjoy, M.; et al. Sports injury and illness incidence in the Rio de Janeiro 2016 Olympic Summer Games: A prospective study of 11274 athletes from 207 countries. Br. J. Sport. Med. 2017, 51, 1265–1271. [Google Scholar] [CrossRef] [PubMed]
- Tin Oo, M.M.; Razali, R. Sport-related oral injuries and mouthguard use among athletes in Kelantan, Malaysia. Arch. Orofac. Sci. 2012, 7, 21–27. [Google Scholar]
- Copcu, E. Sport-induced lipoma. Int. J. Sport. Med. 2004, 25, 182–185. [Google Scholar]
- Fujiwara, M.; Asakuma, S.; Nakamura, K.; Nakamura, T.; Yasutomi, N.; Iwasaki, T. Acute myocardial infarction during sport. J. Cardiol. 1995, 26. [Google Scholar]
- Avery, J.G.; Harper, P.; Ackroyd, S. Do we pay too dearly for our sport and leisure activities? An investigation into fatalities as a result of sporting and leisure activities in England and Wales, 1982–1988. Public Health 1990, 104, 417–423. [Google Scholar] [CrossRef]
- Turk, E.E.; Riedel, A.; Pueschel, K. Natural and traumatic sports-related fatalities: A 10-year retrospective study. Br. J. Sport. Med. 2008, 42, 604–608. [Google Scholar] [CrossRef]
- Chen-Liang, C.; Wen-Guu, L. Sport Injuries and Risk Management regarding Table Tennis Club Members. 2010. Available online: https://people.dyu.edu.tw/paper/9901192_c.pdf (accessed on 31 December 2021). (In Chinese).
- Farì, G.; Fischetti, F.; Zonno, A.; Marra, F.; Maglie, A.; Bianchi, F.; Messina, G.; Ranieri, M.; Megna, M. Musculoskeletal pain in gymnasts: A retrospective analysis on a cohort of professional athletes. Int. J. Environ. Res. Public Health 2021, 18, 5460. [Google Scholar] [CrossRef] [PubMed]
- Farì, G.; Santagati, D.; Macchiarola, D.; Ricci, V.; Di Paolo, S.; Caforio, L.; Invernizzi, M.; Notarnicola, A.; Megna, M.; Ranieri, M. Musculoskeletal pain related to surfing practice: Which role for sports rehabilitation strategies? A cross-sectional study. J. Back Musculoskelet. Rehabil. 2022; preprint. [Google Scholar] [CrossRef]
- Farì, G.; Notarnicola, A.; Di Paolo, S.; Covelli, I.; Moretti, B. Epidemiology of injuries in water board sports: Trauma versus overuse injury. J. Sport. Med. Phys. Fit. 2021, 61, 707–711. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Marotta, N.; Lippi, L.; Scaturro, D.; Farì, G.; Liccardi, A.; Moggio, L.; Mauro, G.L.; Ammendolia, A.; Invernizzi, M. Pharmacological treatment for acute traumatic musculoskeletal pain in athletes. Medicina 2021, 57, 1208. [Google Scholar] [CrossRef] [PubMed]
- Hassan, I.H.I.; Elgammal, M.A. Common injuries in racket sports: A mini review. Ortho. Surg. Ortho. Care Int. J. 2018, 1, 1–3. [Google Scholar] [CrossRef]
- Wang, Y.P.; Chen, G. Table Tennis, 2nd ed.; XanEdu Publishing Company: Ann Arbor, MI, USA, 2006. [Google Scholar]
- Steffen, K.; Engebretsen, L. More data needed on injury risk among young elite athletes. Br. J. Sport. Med. 2010, 44, 485–489. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Search Strategy Items | Search Strategy Details |
|---|---|
| Used keywords | “tennis table” AND (injuries OR lesion OR trauma OR traumatism OR risk factor) |
| Searched databases | PubMed/MEDLINE, ISI/WoS, ProQuest accessed via Ex libris platform at University of Genoa, Genoa, Italy |
| Inclusion criteria | Original article (of any type: case report, case series, observational study, randomized trial) |
| Exclusion criteria | Letter to editor, editorial, review articles |
| Time filter | None applied |
| Language filter | None applied |
| Target journals | BMC Musculoskeletal Disorders; British Journal of Ophthalmology; British Journal of Sports Medicine; British Medical Journal; Cutis; Dental Traumatology; Injury; International Journal Of Sports Medicine; International Journal of Table Tennis Science; Journal of Physical Education, Recreation & Dance; Journal of Sports Sciences; Knee; Knee Surgery, Sports Traumatology, Arthroscopy; Revista Brasileira de Medicina do Esporte; Sports Medicine |
| Authors | Year | Country | Study Population | Age | Injury Rate | Risk Factors/Determinants |
|---|---|---|---|---|---|---|
| Anders Niixius et al. [19] | 1976 | Sweden | A series of 229 cases of Achilles tendon rupture | Nr | 134 (121 m, 13 f) were due to sports activities, 5 (3.7%) of which were due to table tennis | Nr |
| Andrade et al. [40] | 2010 | Pan American Games (XV Pan Am) held in Rio de Janeiro, Brazil in July of 2007 | 5 table tennis players | Nr | 0% (dental injuries) | Nr |
| Barrell et al. [42] | 1981 | United Kingdom | A series of 118 ocular lesions | Nr | 1 case (0.8%) due to table tennis | Nr |
| Chandran [43] | 1974 | Malaysia | A series of 63 cases of ocular lesions | Nr | 2 cases (3.2%) due to table tennis | Nr |
| Correa-Mesa and Correa-Morales [21] | 2015 | Colombia | 50 athletes (9 f, 41 m) out of 52 athletes initially recruited | Nr | Shoulder (28%), knee (26%), and lumbosacral region (10%) | No risk factors found |
| Correa-Mesa [7] | 2015 | Colombia | 178 athletes (141 m, 37 f) | 21.77 y | 44% (129 injuries), with rotator cuff syndrome being the most common disorder (10.6%). Shoulder (17%), knee (16%), back (9.3%) and elbow (9.3%) were the most affected sites. The most prevalent type of injury was tendinopathy (38.2%), followed by benign muscle injuries (17.1%) and sprain lesions (10.9%). | Higher BMI, female gender, older age, and longer training time were found to be significantly associated with an increased injury frequency. |
| de la Torre Combarros et al. [1] | 2007 | Spain | 355 athletes (198 m, 157 f) | 9–21 y | 2.8% | 66.6% during the first day of the championship, 60% during the first hour of the afternoon |
| Di Carlo et al. [23] | 1997 | Venezuela | 26 athletes (18 m, 8 f) | 10–50 y | Shoulder (84.6%), lumbago (100%), supraspinatus tendinitis (63.6%), biceps tendinitis (36.4%) | 54.6% of injured subjects in the range 10–20 y |
| Engebretsen et al. [29] | 2012 | 2012 Olympic Games | 174 athletes (88 f, 86 m) | Nr | 11 (6.3%) reported injuries. Seven (4.0%) and 2 (1.1%) injuries led to time loss ≥1 day and >7 days. | Seven (70.0%) occurred during the competition and 3 (30.0%) during training. |
| Fernández Córdova and Barrios González [24] | 2008 | Cuba | 16 players (8 f, 8 m) | 21 y, range 16–26 y | Bursitis and synovitis (88%), lumbago (75%), tendinitis (25.21%), sacrolumbalgia (10.08%), tenosynovitis (8.40%), chondromalacia and insertion impairment (7.56%), other injuries such as fasciitis, ganglionitis, capsulitis, subluxations, Osgood–Schlatter disease, herniated disc, and residual meniscus (7.56%) | International competitions, practice |
| Folorunso et al. [14] | 2010 | Nigeria | 40 athletes (24 m, 16 f) | 8 < 20 y, 32 > 20 y | 25% (upper limb chronic pain) | Nr |
| Fong et al. [22] | 2008 | Hong Kong | A series of 240 ankle injuries out of a total of 1715 sports-related lesions and injuries | Nr | 6 due to table tennis: 3 (1.3%) were ankle injuries, 3 (1.5%) ligamentous sprains | Lower ankle injury rate with respect to other sports, such as basketball or soccer. |
| Hill et al. [39] | 1985 | United Kingdom | 130 patients with dental injuries related to 21 sports activities | Nr | Few table tennis-related injuries | Nr |
| Jeffers [44] | 1988 | USA | A series of 203 ocular lesions | Nr | 2 cases due to table tennis | Nr |
| Junge et al. [28] | 2009 | Summer Olympic Games 2008 | 10,977 registered athletes | Nr | 9 athletes (5.2%) were injured, with an estimated 2.6% of athletes reporting time-loss injuries. One injury was a fracture and 1 a dislocation/rupture of the tendon or ligament. | Five athletes (83.3%) reported injuries during training, only 1 (16.7%) during competition. |
| Kelly and Nolan [45] | 1983 | Ireland | A series of 45 consecutive patients (37 m, 8 f; 5 cases lost at follow-up) | 25 y | 1 case due to table tennis | Nr |
| Kondric et al. [27] | 2011 | Slovenia | 83 athletes of which 29 table tennis players | 19.52 ± 4.21 y | Shoulder girdle (17.3%), spine (16.6%), ankle (15.8%), foot (10.1%), and wrist (12.2%) | No risk factors found (training and competition reporting equal injury rates, also comparing females and males). |
| Laoruengthana et al. [38] | 2009 | 37th Thailand National Games 2008 in Phitsanulok, Thailand | 276 athletes (124 m, 152 f) | Nr | 0% | Nr |
| Linderoth et al. [30] | 2006 | Sweden | 85 athletes (only 44 taking part in the study) | Nr | 79.5% (strain injuries 75%, upper limb 40%, lower extremity 35%, back injuries 22%, neck injuries 3%) | Poor warm-up and stretching, gender (women reporting more injuries to the upper extremity), poor resting after injuries |
| Lo et al. [26] | 1990 | Hong Kong | 373 students (242 m, 130 f) | Nr | Shoulder impingement (1.3%) | Nr |
| Lovell et al. [46] | 1995 | Australia | A series of 189 chronic injuries | Nr | 1 case of chronic groin pain | Nr |
| Majewski et al. [25] | 2006 | Switzerland | A 10-year survey of 123,653 athletes | Nr | 37 cases of knee joint traumas | Nr |
| Rajabi et al. [15] | 2012 | Iran | 52 m athletes, of which 22 took part in the study | 57 ± 5 y | Osteoarthritis (78.3%) | Nr |
| Shida et al. [47] | 1992 | Japan | 303 university students (166 m, 137 f) | 13–21 y | 59.4% (lumbago 23.5%, knee joint injury 13.4%, tenosynovitis, and sprains being the most common injuries) | Age (70% of injuries in high school), practice for more than 5 years, more than 20 h per week, poor training program |
| Shida et al. [48] | 1994 | Japan | 210 athletes (111 m, 99 f), with 100 taking part in the study | Nr | 64.8% (lumbago, 25.1%, shoulder 15.7%, knee 14.1%) | Nr |
| Shimazaki et al. [20] | 2012 | Brazil | 111 athletes | 23 ± 9 y | Injury rate of 0.5 injuries per athlete | International/national players (52.9%) versus regional players (48.8%), most injuries during training |
| Soligard et al. [49] | 2017 | Brazil, XXXI Olympic Games, hosted by Rio de Janeiro from 5 to 21 August 2016 | 11,274 athletes (6185 m, 5089 f) from all disciplines (nr for table tennis) | Nr | 0–3% | No risk factors identified |
| Tin-Oo and Razali [50] | 2012 | Malaysia | 180 athletes | 12–27 y | 0% (oral injuries) | Nr |
| Case Report/Case Series | Type of Injury |
|---|---|
| Avery et al., 1990 [53] | Catastrophic injuries |
| Copcu, 2004 [51] | Tumor |
| Dufek et al., 1999 [36] | Orthopedic injuries |
| Fujiwara, 1995 [52] | Cardiological injuries |
| Kexue, 1996 [33] | Orthopedic injuries |
| Le Floch et al., 2010 [6] | Neurological injuries |
| Li, 1996 [33] | Orthopedic injuries |
| Nicolini et al., 2014 [32] | Orthopedic injuries |
| Petschnig et al., 1997 [37] | Orthopedic injuries |
| Pieper et al., 1993 [31] | Orthopedic injuries |
| Pintore and Maffulli, 1991 [34] | Orthopedic injuries |
| Ron et al., 1983 [35] | Orthopedic injuries |
| Scott and Scott, 1989 [41] | Dermatological injuries |
| Turk et al., 2008 [54] | Catastrophic injuries |
| Authors | Percentage of “Yes” | Interpretation |
|---|---|---|
| Anders Niixius et al. [19] | 30.0% | High risk of bias |
| Andrade et al. [40] | 33.3% | High risk of bias |
| Barrell et al. [42] | 50.0% | Moderate risk of bias |
| Chandran [43] | 60.0% | Moderate risk of bias |
| Correa-Mesa and Correa-Morales [21] | 11.1% | High risk of bias |
| Correa-Mesa [7] | 55.6% | Moderate risk of bias |
| de la Torre Combarros et al. [1] | 90.0% | Low risk of bias |
| Di Carlo et al. [23] | 33.3% | High risk of bias |
| Engebretsen et al. [29] | 60.0% | Moderate risk of bias |
| Fernández Córdova and Barrios González [24] | 30.0% | High risk of bias |
| Folorunso et al. [14] | 22.2% | High risk of bias |
| Fong et al. [22] | 60.0% | Moderate risk of bias |
| Hill et al. [39] | 60.0% | Moderate risk of bias |
| Jeffers [44] | 40.0% | High risk of bias |
| Junge et al. [28] | 50.0% | Moderate risk of bias |
| Kelly and Nolan [45] | 60.0% | Moderate risk of bias |
| Kondric et al. [27] | 11.1% | High risk of bias |
| Laoruengthana et al. [38] | 40.0% | High risk of bias |
| Linderoth et al. [30] | 11.1% | High risk of bias |
| Lo et al. [26] | 22.2% | High risk of bias |
| Lovell et al. [46] | 70.0% | Moderate risk of bias |
| Majewski et al. [25] | 40.0% | High risk of bias |
| Rajabi et al. [15] | 100.0% | Low risk of bias |
| Shida et al. [47] | 44.4% | High risk of bias |
| Shida et al. [48] | 22.2% | High risk of bias |
| Shimazaki et al. [20] | 60.0% | Moderate risk of bias |
| Soligard et al. [49] | 60.0% | Moderate risk of bias |
| Tin-Oo and Razali [50] | 33.3% | High risk of bias |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biz, C.; Puce, L.; Slimani, M.; Salamh, P.; Dhahbi, W.; Bragazzi, N.L.; Ruggieri, P. Epidemiology and Risk Factors of Table-Tennis-Related Injuries: Findings from a Scoping Review of the Literature. Medicina 2022, 58, 572. https://doi.org/10.3390/medicina58050572
Biz C, Puce L, Slimani M, Salamh P, Dhahbi W, Bragazzi NL, Ruggieri P. Epidemiology and Risk Factors of Table-Tennis-Related Injuries: Findings from a Scoping Review of the Literature. Medicina. 2022; 58(5):572. https://doi.org/10.3390/medicina58050572
Chicago/Turabian StyleBiz, Carlo, Luca Puce, Maamer Slimani, Paul Salamh, Wissem Dhahbi, Nicola Luigi Bragazzi, and Pietro Ruggieri. 2022. "Epidemiology and Risk Factors of Table-Tennis-Related Injuries: Findings from a Scoping Review of the Literature" Medicina 58, no. 5: 572. https://doi.org/10.3390/medicina58050572
APA StyleBiz, C., Puce, L., Slimani, M., Salamh, P., Dhahbi, W., Bragazzi, N. L., & Ruggieri, P. (2022). Epidemiology and Risk Factors of Table-Tennis-Related Injuries: Findings from a Scoping Review of the Literature. Medicina, 58(5), 572. https://doi.org/10.3390/medicina58050572