

The Cyst of the Canal of Nuck: Anatomy, Diagnostic and Treatment of a Very Rare Diagnosis—A Case Report of an Adult Woman and Narrative Review of the Literature

 ,
,
Abstract
1. Introduction
2. Methodology
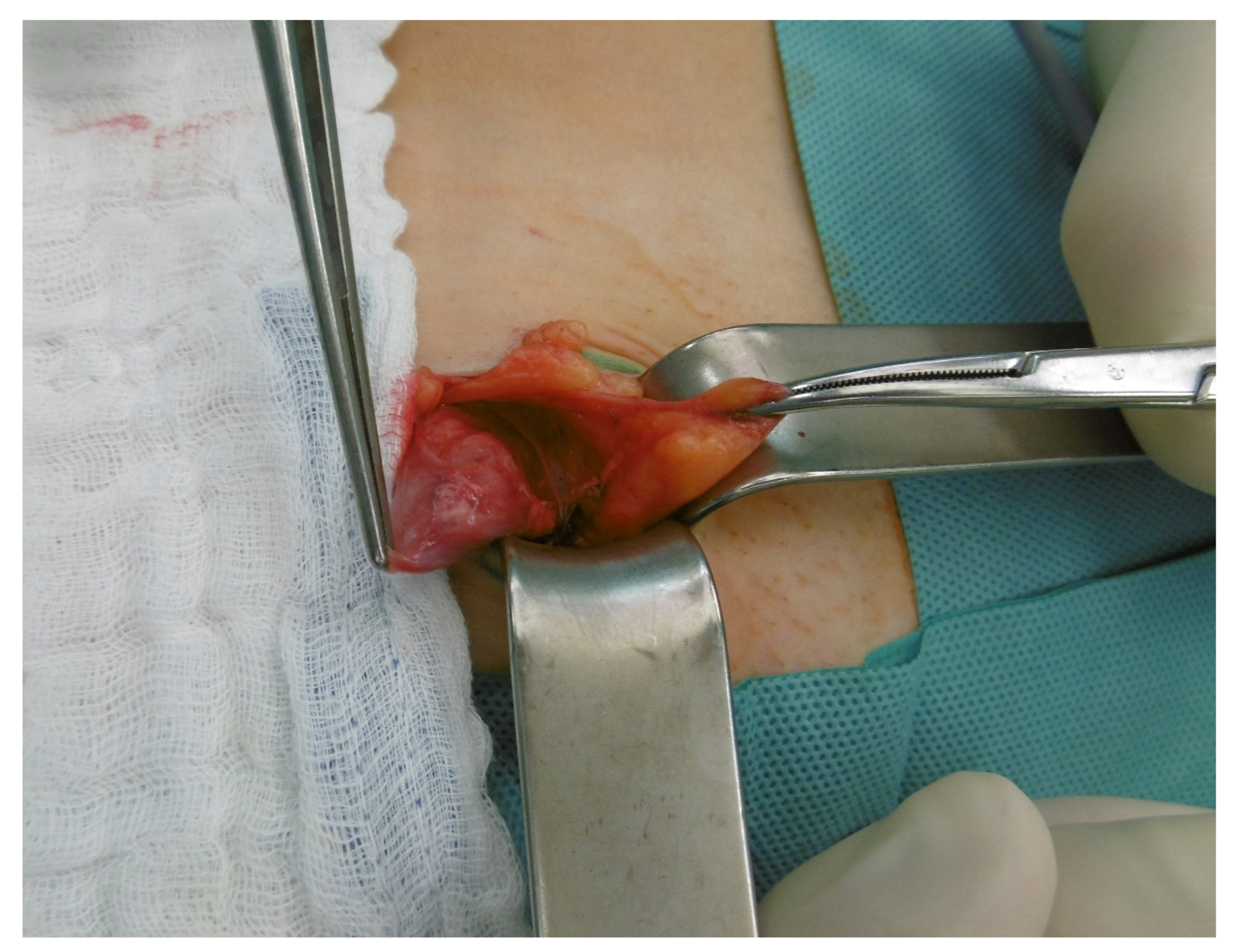
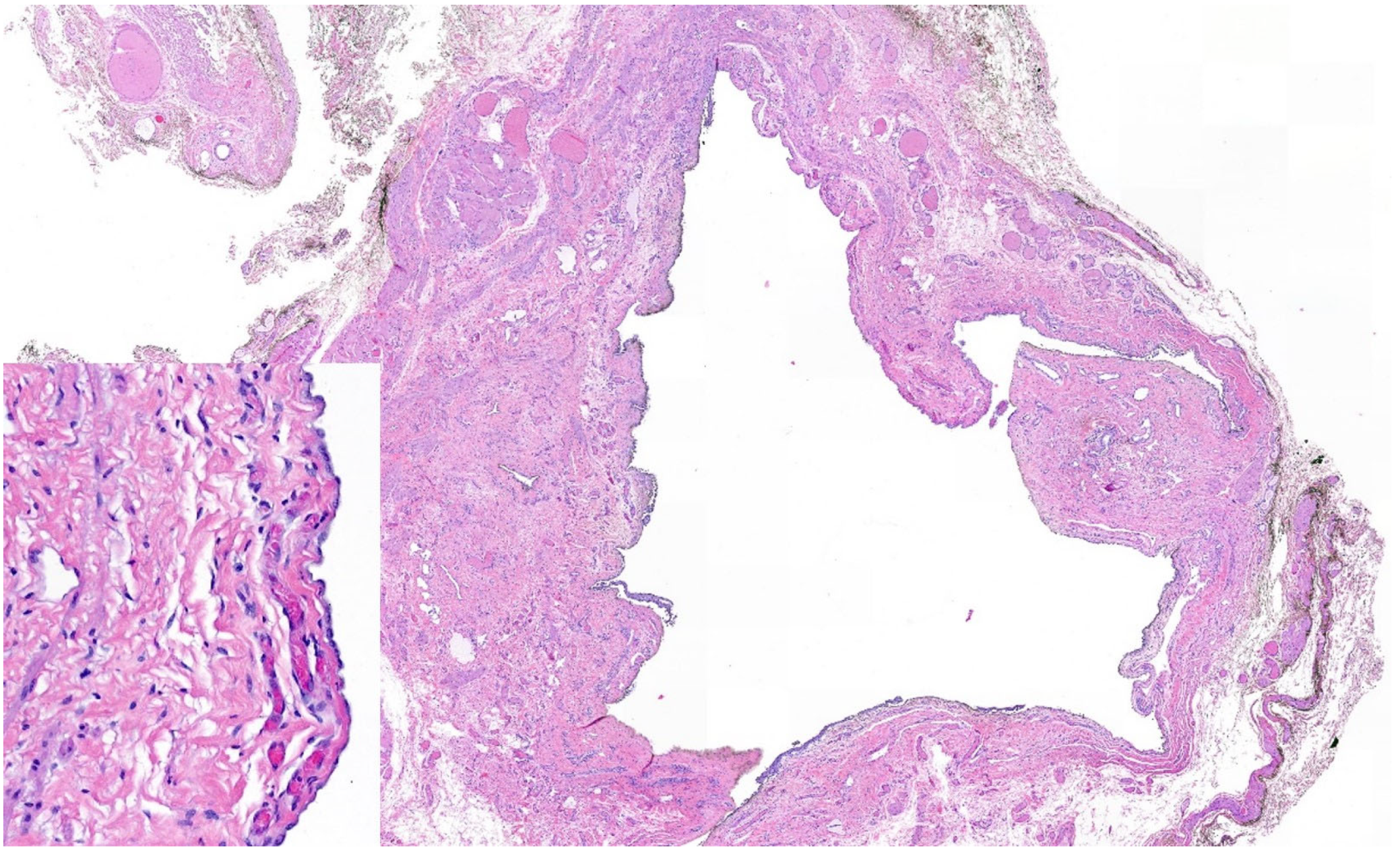
3. Case Report
4. Review of Literature
4.1. Anatomical and Pathological Background
4.2. Prevalence
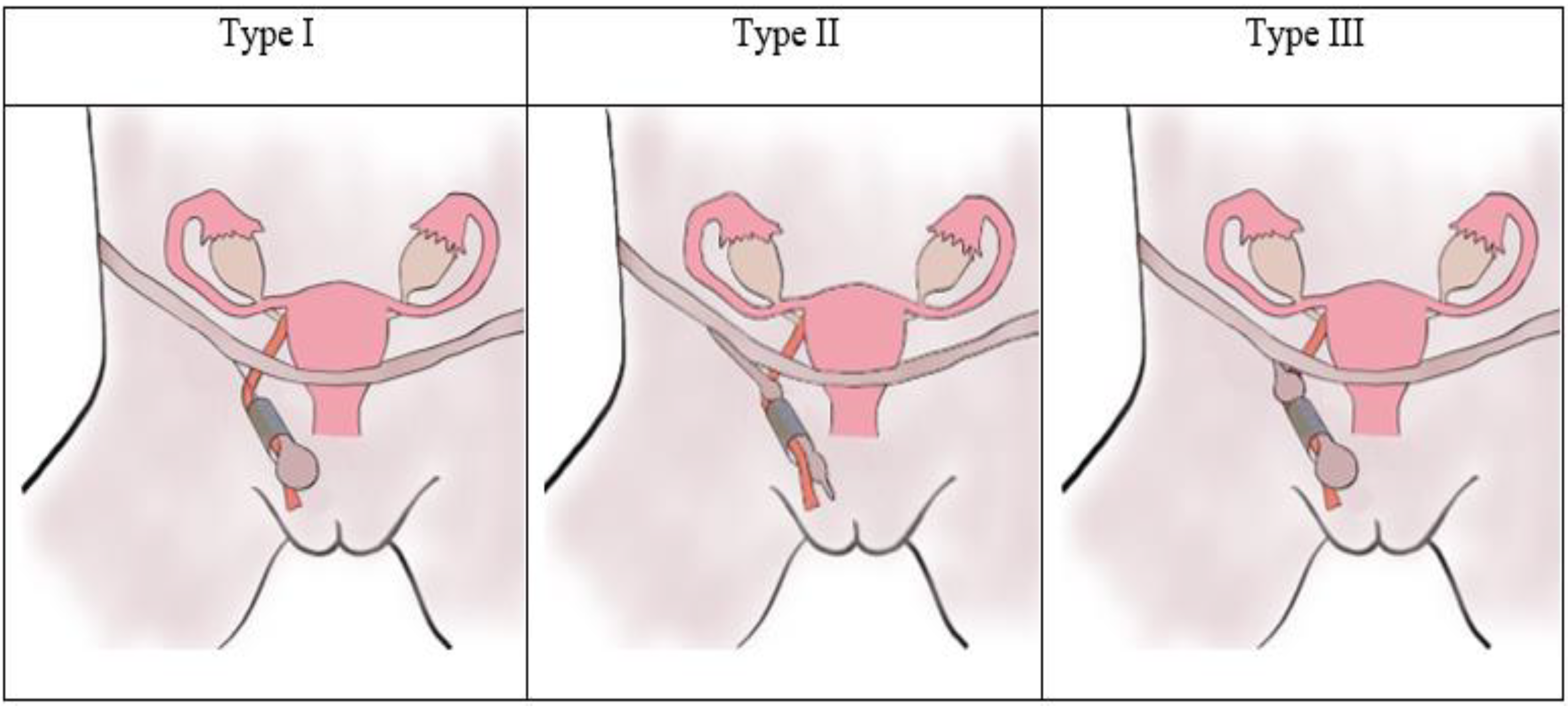
4.3. Classification
4.4. Clinical Presentation and Diagnostic Methods
4.5. Treatment
5. Discussion
6. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prodromidou, A.; Paspala, A.; Schizas, D.; Spartalis, E.; Nastos, C.; Machairas, N. Cyst of the canal of Nuck in adult females: A case report and systematic review. Biomed. Rep. 2020, 12, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Fikatas, P.; Megas, I.F.; Mantouvalou, K.; Alkatout, I.; Chopra, S.S.; Biebl, M.; Pratschke, J.; Raakow, J. Hydroceles of the canal of nuck in adults—Diagnostic, treatment and results of a rare condition in females. J. Clin. Med. 2020, 9, 4026. [Google Scholar] [CrossRef] [PubMed]
- Nasser, H.; King, M.; Rosenberg, H.K.; Rosen, A.; Wilck, E.; Simpson, W.L. Anatomy and pathology of the canal of Nuck. Clin. Imaging 2018, 51, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Holley, A. Pathologies of the canal of Nuck. Sonography 2018, 5, 29–35. [Google Scholar] [CrossRef]
- Okoshi, K.; Mizumoto, M.; Kinoshita, K. Endometriosis-associated hydrocele of the canal of Nuck with immunohistochemical confirmation: A case report. J. Med. Case Rep. 2017, 11, 354. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, A.F.; Marques, J.P.; Falcão, F. Hydrocele of the canal of Nuck presenting as a sausage-shaped mass. BMJ Case Rep. 2017, 2017, bcr-2017-221024. [Google Scholar] [CrossRef]
- Pandey, A.; Jain, S.; Verma, A.; Jain, M.; Srivastava, A.; Shukla, R.C. Hydrocele of the canal of Nuck-Rare differential for vulval swelling. Indian J. Radiol. Imaging 2014, 24, 175–177. [Google Scholar] [CrossRef]
- Matsumoto, T.; Hara, T.; Hirashita, T.; Kubo, N.; Hiroshige, S.; Orita, H. Laparoscopic diagnosis and treatment of a hydrocele of the canal of Nuck extending in the retroperitoneal space: A case report. Int. J. Surg. Case Rep. 2014, 5, 861–864. [Google Scholar] [CrossRef]
- Uzun, I.; İnan, C.; Varol, F.; Erzincan, S.; Sütcü, H.; Sayin, C. Hemorrhagic cyst of the canal of Nuck after vaginal delivery presenting as a painful inguinal mass in the early postpartum period. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 213, 147–148. [Google Scholar] [CrossRef]
- Walter, H.; Stickel, M.D.; Martin Manner, M. Female hydrocele of canal of nuck. J. Ultrasound Med. 2010, 107, 38–39. [Google Scholar]
- Zawaideh, J.P.; Trambaiolo Antonelli, C.; Massarotti, C.; Remorgida, V.; Derchi, L.E. Cyst of Nuck: A Disregarded Pathology. J. Minim. Invasive Gynecol. 2018, 25, 376–377. [Google Scholar] [CrossRef] [PubMed]
- Bunting, D.; Szczebiot, L.; Cota, A. Laparoscopic hernia repair-When is a hernia not a hernia? J. Soc. Laparoendosc. Surg. 2013, 17, 654–656. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Choi, J.H.; Kim, H.M.; Kim, K.P.; Kwon, Y.J.; Hwang, J.H.; Lee, S.Y. Hydrocele of the canal of nuck in a female adult. Arch. Plast. Surg. 2016, 43, 476–478. [Google Scholar] [CrossRef] [PubMed]
- Bagley, J.E.; Davis, M.B. Cyst of canal of nuck. J. Diagn. Med. Sonogr. 2015, 31, 111–114. [Google Scholar] [CrossRef]
- Patnam, V.; Narayanan, R.; Kudva, A. A cautionary approach to adult female groin swelling: Hydrocoele of the canal of Nuck with a review of the literature. BMJ Case Rep. 2016, 2016, bcr2015212547. [Google Scholar] [CrossRef]
- Ozel, A.; Kirdar, O.; Halefoglu, A.M.; Erturk, S.M.; Karpat, Z.; Lo Russo, G.; Maldur, V.; Cantisani, V. Cysts of the canal of Nuck: Ultrasound and magnetic resonance imaging findings. J. Ultrasound 2009, 12, 125–127. [Google Scholar] [CrossRef] [PubMed]
- Caviezel, A.; Montet, X.; Schwartz, J.; Egger, J.F.; Iselin, C.E. Female hydrocele: The cyst of nuck. Urol. Int. 2009, 82, 242–245. [Google Scholar] [CrossRef]
- Ryan, J.D.; Joyce, M.R.; Pierce, C.; Brannigan, A.; O’Connell, P.R. Haematoma in a hydrocele of the canal of Nuck mimicking a Richter’s hernia. Hernia 2009, 13, 643–645. [Google Scholar] [CrossRef]
- Sethi, V.; Patel, H. Hydrocele in the canal of nuck—CT appearance of a developmental groin anomaly. J. Radiol. Case Rep. 2016, 10, 29–33. [Google Scholar] [CrossRef]
- Hwang, B.; Bultitude, J.; Diab, J.; Bean, A. Cyst and endometriosis of the canal of Nuck: Rare differentials for a female groin mass. J. Surg. Case Rep. 2022, 2022, rjab626. [Google Scholar] [CrossRef]
- Jagdale, R.; Agrawal, S.; Chhabra, S.; Jewan, S.Y. Hydrocele of the canal of Nuck: Value of radiological diagnosis. J. Radiol. Case Rep. 2012, 6, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Kono, R.; Terasaki, H.; Murakami, N.; Tanaka, M.; Takeda, J.; Abe, T. Hydrocele of the canal of Nuck: A case report with magnetic resonance hydrography findings. Surg. Case Rep. 2015, 1, 86. [Google Scholar] [CrossRef] [PubMed]
- Akkoyun, I.; Kucukosmanoglu, I.; Yalinkilinc, E. Cyst of the canal of Nuck in pediatric patients. N. Am. J. Med. Sci. 2013, 5, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Nuck, A. Adenographia curiosa et uteri foeminei anatome nova. Am. J. Obstet. Gynecol. 1975, 123, 66. [Google Scholar] [CrossRef]
- Coley, W.B., II. Hydrocele in the Female: With a Report of Fourteen Cases. Ann. Surg. 1892, 16, 42–59. [Google Scholar] [CrossRef]
- Dagur, G.; Gandhi, J.; Suh, Y.; Weissbart, S.; Sheynkin, Y.R.; Smith, N.L.; Joshi, G.; Khan, S.A. Classifying Hydroceles of the Pelvis and Groin: An Overview of Etiology, Secondary Complications, Evaluation, and Management. Curr. Urol. 2017, 10, 1–14. [Google Scholar] [CrossRef]
- Papparella, A.; Vaccaro, S.; Accardo, M.; DE Rosa, L.; Ronchi, A.; Noviello, C. Nuck cyst: A rare cause of inguinal swelling in infancy. Minerva Pediatr. 2021, 73, 180–183. [Google Scholar] [CrossRef]
- Huang, C.S.; Luo, C.C.; Chao, H.C.; Chu, S.M.; Yu, Y.J.; Yen, J.B. The presentation of asymptomatic palpable movable mass in female inguinal hernia. Eur. J. Pediatr. 2003, 162, 493–495. [Google Scholar] [CrossRef]
- Counseller, V.S.; Black, B.M. Hydrocele of the canal of Nuck. Report of seventeen cases. Ann. Surg. 1941, 113, 625–630. [Google Scholar] [CrossRef]
- Wang, L.; Maejima, T.; Fukahori, S.; Shun, K.; Yoshikawa, D.; Kono, T. Laparoscopic surgical treatment for hydrocele of canal of Nuck: A case report and literature review. Surg. Case Rep. 2021, 7, 121. [Google Scholar] [CrossRef]
- Manenti, G.; D’Amato, D.; Ranalli, T.; Marsico, S.; Castellani, F.; Salimei, F.; Floris, R. Cyst of canal of Nuck in a young woman affected by kniest syndrome: Ultrasound and MRI features. Radiol. Case Rep. 2019, 14, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Topal, U.; Sarıtaş, A.G.; Ülkü, A.; Akçam, A.T.; Doran, F. Cyst of the canal of Nuck mimicking inguinal hernia. Int. J. Surg. Case Rep. 2018, 52, 117–119. [Google Scholar] [CrossRef]
- Scott, M.; Helmy, A.H. Rare encounter: Hydrocoele of canal of Nuck in a Scottish rural hospital during the COVID-19 pandemic. BMJ Case Rep. 2020, 13, 13–16. [Google Scholar] [CrossRef] [PubMed]
- Jamadar, D.A.; Jacobson, J.A.; Morag, Y.; Girish, G.; Ebrahim, F.; Gest, T.; Franz, M. Sonography of inguinal region hernias. Am. J. Roentgenol. 2006, 187, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Shakil, A.; Aparicio, K.; Barta, E.; Munez, K. Inguinal Hernias: Diagnosis and Management. Am. Fam. Physician 2020, 102, 487–492. [Google Scholar] [PubMed]
- Van den Berg, J. Inguinal Hernias: MRI and Ultrasound. Semin. Ultrasound CT MRI 2002, 23, 156–173. [Google Scholar] [CrossRef]
- Simons, M.P.; Smietanski, M.; Bonjer, H.J.; Bittner, R.; Miserez, M.; Aufenacker, T.J.; Fitzgibbons, R.J.; Chowbey, P.K.; Tran, H.M.; Sani, R.; et al. International guidelines for groin hernia management. Hernia 2018, 22, 1–165. [Google Scholar] [CrossRef]
- Mohseni, S.; Shojaiefard, A.; Khorgami, Z.; Alinejad, S.; Ghorbani, A.; Ghafouri, A. Peripheral lymphadenopathy: Approach and diagnostic tools. Iran. J. Med. Sci. 2014, 39, 158–170. [Google Scholar]
- Torabi, M.; Aquino, S.L.; Harisinghani, M.G. Current Concepts in Lymph Node Imaging Continuing Education. J. Nucl. Med. 2004, 45, 1509–1518. [Google Scholar]
- Eppel, W.; Worda, C. Ultrasound Imaging of Bartholin’ s Cysts. Gynecol. Obstet. Investig. 2000, 49, 179–182. [Google Scholar] [CrossRef]
- López, C.; Balogun, M.; Ganesan, R.; Olliff, J.F. MRI of vaginal conditions. Clin. Radiol. 2005, 60, 648–662. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.Y.; Dalpiaz, A.; Schwamb, R.; Miao, Y.; Waltzer, W.; Khan, A. Clinical pathology of Bartholin’s glands: A review of the literature. Curr. Urol. 2014, 8, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Licheri, S.; Pisano, G.; Erdas, E.; Ledda, S.; Casu, B.; Cherchi, M.V.; Pomata, M.; Daniele, G.M. Endometriosis of the round ligament: Description of a clinical case and review of the literature. Hernia 2005, 9, 294–297. [Google Scholar] [CrossRef] [PubMed]
- Gui, B.; Valentini, A.L.; Ninivaggi, V.; Marino, M.; Iacobucci, M.; Bonomo, L. Deep pelvic endometriosis: Don’t forget round ligaments. Review of anatomy, clinical characteristics, and MR imaging features. Abdom. Imaging 2014, 39, 622–632. [Google Scholar] [CrossRef]
- Yukata, K.; Nakai, S.; Goto, T.; Ikeda, Y.; Shimaoka, Y.; Yamanaka, I.; Sairyo, K.; Hamawaki, J.I.J. Cystic lesion around the hip joint. World J. Orthop. 2015, 6, 688–704. [Google Scholar] [CrossRef]
- Angelini, A.; Zanotti, G.; Berizzi, A.; Staffa, G.; Piccinini, E.; Ruggieri, P. Synovial cysts of the hip. Acta Biomed. 2017, 88, 483–490. [Google Scholar] [CrossRef]
- Johnson, C.N.; Ha, A.S.; Chen, E.; Davidson, D. Lipomatous soft-tissue tumors. J. Am. Acad. Orthop. Surg. 2018, 26, 779–788. [Google Scholar] [CrossRef]
- Fasih, N.; Prasad Shanbhogue, A.K.; Macdonald, D.B.; Fraser-Hill, M.A.; Papadatos, D.; Kielar, A.Z.; Doherty, G.P.; Walsh, C.; McInnes, M.; Atri, M. Leiomyomas beyond the uterus: Unusual locations, rare manifestations. Radiographics 2008, 2, 1931. [Google Scholar] [CrossRef]
- Sun, C.; Zou, J.; Wang, Q.; Wang, Q.; Han, L.; Batchu, N.; Ulain, Q.; Du, J.; Lv, S.; Song, Q.; et al. Review of the pathophysiology, diagnosis, and therapy of vulvar leiomyoma, a rare gynecological tumor. J. Int. Med. Res. 2018, 46, 663–674. [Google Scholar] [CrossRef]
- Wozniak, A.; Wozniak, S. Ultrasonography of uterine leiomyomas. Menopause Rev. 2017, 16, 113–117. [Google Scholar] [CrossRef]
- Mine, Y.; Eguchi, S.; Enjouji, A.; Fukuda, M.; Yamaguchi, J.; Inoue, Y.; Fujita, F.; Tsukamoto, O.; Masuzaki, H. Round ligament varicosities diagnosed as inguinal hernia during pregnancy: A case report and series from two regional hospitals in Japan. Int. J. Surg. Case Rep. 2017, 36, 122–125. [Google Scholar] [CrossRef] [PubMed]
- Naik, S.S.; Balasubramanian, P. Round ligament varices mimicking inguinal hernia during pregnancy. Radiol. Case Rep. 2019, 14, 1036–1038. [Google Scholar] [CrossRef] [PubMed]
- Ryu, K.H.; Yoon, J.H. Ultrasonographic diagnosis of round ligament varicosities mimicking inguinal hernia: Report of two cases with literature review. Ultrasonography 2014, 33, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Tokue, H.; Aoki, J.; Tsushima, Y.; Endo, K. Characteristic of computed tomography and magnetic resonance imaging finding of thrombosed varices of the round ligament of the uterus: A case report. J. Comput. Assist. Tomogr. 2008, 32, 559–561. [Google Scholar] [CrossRef]
- Ng, C.; Wong, G.T. Round ligament varicosity thrombosis presenting as an irreducible inguinal mass in a postpartum woman. J. Clin. Imaging Sci. 2019, 9, 28. [Google Scholar] [CrossRef]
- Cornacchia, C.; Dessalvi, S.; Boccardo, F. Surgical treatment of cyst of the canal of nuck and prevention of lymphatic complications: A single-center experience. Lymphology 2019, 52, 143–148. [Google Scholar] [CrossRef]
- Qureshi, N.J.; Lakshman, K. Laparoscopic excision of cyst of canal of Nuck. J. Minim. Access Surg. 2014, 10, 87–89. [Google Scholar] [CrossRef]
- Shahid, F.; El Ansari, W.; Ben-Gashir, M.; Abdelaal, A. Laparoscopic hydrocelectomy of the canal of Nuck in adult female: Case report and literature review. Int. J. Surg. Case Rep. 2020, 66, 338–341. [Google Scholar] [CrossRef]
- Wang, L.; Maejima, T.; Fukahori, S.; Shun, K.; Yoshikawa, D.; Kono, T. Laparoscopic assisted hydrocelectomy of the canal of Nuck: A case report. Surg. Case Rep. 2021, 7. [Google Scholar] [CrossRef]
- Eker, H.H.; Hansson, B.M.E.; Buunen, M.; Janssen, I.M.C.; Pierik, R.E.G.J.M.; Hop, W.C.; Bonjer, H.J.; Jeekel, J.; Lange, J.F. Laparoscopic vs Open Incisional Hernia Repair. JAMA Surg. 2013, 148, 259. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Differential Diagnosis | Symptoms | Physical Examination | Imaging |
|---|---|---|---|
| Cyst of the canal of Nuck | Cysts of the canal of Nuck present as an inguinal or genital, painless or painful swelling with no gastrointestinal symptoms. | On clinical examination, an inguinal or genital swelling is palpable. This mass shows no increase in volume by performing the Valsalva maneuver, and may is manually reducible. | On ultrasound, an anechoic or hypoechoic lesion without changes in the Valsalva maneuver and without vascular flow can be detected. Computed tomography (CT) imaging shows the cyst of the canal of Nuck as a homogeneous fluid-filled lesion along the round ligament. On magnetic resonance imaging (MRI), it shows as a thin-walled lesion, which appears hypointense on T1-weighted and hyperintense on T2-weighted sequences. |
| Inguinal hernia [34,35,36,37] | Inguinal hernias may be asymptomatic or symptomatic along with swelling, discomfort, or pain in the groin. Activities that increase intra-abdominal pressure may increase these symptoms. Sudden severe pain, nausea and vomiting indicate possible incarceration of organs in the hernia sac. | The gold standard for hernia diagnostics is clinical examination, although diagnosis is more difficult in women. A female inguinal hernia is confirmed if a bulge is palpable with the open hand over the groin during a Valsalva maneuver. | Although it is rarely necessary, imaging may be useful in unclear situations. Ultrasound is a highly sensitive method of identifying hernias. While the herniating fat appears hyperechoic on ultrasound, the bowel may show peristalsis. Valsalva maneuver is an important examination during the sonography, to increase the swelling and show characteristic movement of the herniating tissues. When ultrasound is not sufficient, a dynamic MRI or CT can be considered. On MRI, hernias present as pathological widening of the anteroposterior inguinal canal and/or protrusion of gastro-enteric content within the inguinal canal. |
| Lymph-adenopathy [38,39] | Localized inguinal lymphadenopathy is typically caused by infection, while malignancy rarely presents itself solely in the inguinal lymph nodes. | Inguinal lymph node size over 1.5 cm should be suspected as pathological. Pain and tenderness on a lymph node is a non-specific finding. Lymphadenopathies resulting from infections are usually free moving. Acute inflammation makes nodes tauter with concomitant tenderness, while chronic inflammation leads to hard nodes. Painless and adamantine nodes, which are fixed to the surrounding tissues are usually caused by metastatic cancer or granulomatous diseases. Rubbery mobile nodes are typical of lymphoma. | On ultrasound, benign lymphadenopathies emerge as ovoid lesions with various borders, inconspicuous hilum, and isoechoic internal echogenicity, while neoplastic disorders present as round lesions with a sharp border, no hilum and a hypoechoic internal echogenicity. Most benign lymphadenopathies present as ovoid lesions with a central fatty hilum on CT and MRI. Round morphology in addition to changes in size, signal intensity, and dynamic gadolinium contrast enhancement are typical for malignant lesions. |
| Bartholin cysts [40,41,42] | Bartholin cyst can be asymptomatic or symptomatic, associated with painful swelling in not only the genital but also the inguinal region. | During examination small asymptomatic cysts may be observed as small masses, while larger cysts and abscesses are associated with cellulitis, severe pain and swelling. In addition, a Bartholin gland abscess presents with erythema, edema and sometimes ruptured skin. | On ultrasound, a Bartholin cyst is a central hypoechoic to anechoic lesion, surrounded by a stronger reflective cystic wall, which presents as increased echo enhancement on the posterior side. On MRI, it shows as a small cystic mass with a high signal intensity on T2-weighted sequences and also, depending on the mucoid content, on T1-weighted ones. |
| Endometriosis of the round ligament [43,44] | If endometriosis affects the extra pelvic portion of the round ligament it may present as a painful, palpable groin mass with or without menstrual variation. | On examination, the endometriosis of the round ligament presents as groin mass without fluctuation, which is non-reducible and possibly partially tender. There are no changes through straining, coughing or adjustments in the patient’s position. | On sonographic examination, endometriosis of the round ligament shows as an inhomogeneous hypoechoic lesion with poorly defined boundaries. On MRI scans, endometriosis of the round ligament, which usually presents as a thin hypointense structure, appears thickened, shortened and irregular. While pure fibrous lesions are hypointense on T1- and T2- weighted sequences, hemorrhagic lesions are hyperintense on T1-weighted images. |
| Ganglion cysts [45,46] | Ganglion cysts of the hip joint are usually asymptomatic but may cause pain through compression of nerves and vessels. They may present as swelling of the groin or genital region, when they become larger. | On clinical examination, ganglion cysts show as tender, non-pulsatile masses, which may limit the range of motion of the hip joint. Deeper cysts are more difficult to palpate and usually a radiological imaging is necessary to detect them. | Ganglion cysts present on ultrasound as a hypoechoic lesion without the ability to identify the exact joint connection. On CT, ganglion cysts show lower attenuation than muscles, but higher ones than fat. After contrast administration, a rim enhancement may be observed. MRI can show round or ovoid cystic masses with low signal intensities on T1- and high ones on T2-weighted sequences. Similar to CT, a rim enhancement can be observed on T1-weighted MRI sequences, after contrast administration. |
| Lipomata [47] | Lipoma presents as a painless soft-tissue mass. Deeper ones may be larger and present as asymmetrical. | On palpation, lipomata are freely movable doughy subcutaneous masses. Deeper ones, namely intramuscular lipomata move simultaneously with muscle contraction. | On ultrasonography, lipomata present as homogenous hyperechogenic masses. MRI is necessary for any deeper lipomas or lesion bigger than 5 cm. Lipomata show as homogenous lesions, isointense to fat and may contain thin fibrous septae, on MRI. CT is only the second choice, when patients are inept for MRI due to medical reasons. |
| Leiomyomata [48,49,50] | Leiomyomata may arise in unusual regions such as the vulva. Clinically, these vulvar leiomyomata usually present as painless swellings of the genital region. | On palpation a vulvar leiomyoma shows as a partially mobile mass, which is non-tender in most cases. In certain superficial lesions, a peduncle is sometimes palpable. | On ultrasound leiomyomata present as well-defined, solid, concentric, hypoechoic masses. Due to its bad soft-tissue contrast, CT has a minor role in diagnostics. Vaginal Leiomyomata are isotense to muscles on T1-weighted MRI sequences and enhance homogenously after contrast administration. On T2-weighted sequences, vulvar leiomyomata show a low signal intensity similar to that of smooth muscles. |
| Varicosity of the round ligament [51,52,53,54,55] | Varicosity of the round ligament is a further rare condition, which commonly occurs as painful or painless inguinal swelling. In most common cases, the occurrence is associated with pregnancy. | On physical examination, varicosity of the round ligament occurs as a soft groin mass. Some authors describe an increase in size of the mass in standing position and on Valsalva maneuver. | The sonographical characteristics of the round ligament varicosities are dilated veins that appear as multiple echo free serpentine tubes, some of which drain into the inferior epigastric artery, with no herniated bowel or lymphadenopathy. Doppler sonography reveals hypervascularity with a venous flow pattern which increases during Valsalva-maneuver. On both MRI and CT, the varicosity of the round ligament appears as a well-defined serpentine structure extending along the inguinal course of the round ligament of the uterus. In the case of thrombosis, the MRI will show a high T1 and a low T2 signal. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kohlhauser, M.; Pirsch, J.V.; Maier, T.; Viertler, C.; Fegerl, R. The Cyst of the Canal of Nuck: Anatomy, Diagnostic and Treatment of a Very Rare Diagnosis—A Case Report of an Adult Woman and Narrative Review of the Literature. Medicina 2022, 58, 1353. https://doi.org/10.3390/medicina58101353
Kohlhauser M, Pirsch JV, Maier T, Viertler C, Fegerl R. The Cyst of the Canal of Nuck: Anatomy, Diagnostic and Treatment of a Very Rare Diagnosis—A Case Report of an Adult Woman and Narrative Review of the Literature. Medicina. 2022; 58(10):1353. https://doi.org/10.3390/medicina58101353
Chicago/Turabian StyleKohlhauser, Michael, Julian Vinzent Pirsch, Thorsten Maier, Christian Viertler, and Roland Fegerl. 2022. "The Cyst of the Canal of Nuck: Anatomy, Diagnostic and Treatment of a Very Rare Diagnosis—A Case Report of an Adult Woman and Narrative Review of the Literature" Medicina 58, no. 10: 1353. https://doi.org/10.3390/medicina58101353
APA StyleKohlhauser, M., Pirsch, J. V., Maier, T., Viertler, C., & Fegerl, R. (2022). The Cyst of the Canal of Nuck: Anatomy, Diagnostic and Treatment of a Very Rare Diagnosis—A Case Report of an Adult Woman and Narrative Review of the Literature. Medicina, 58(10), 1353. https://doi.org/10.3390/medicina58101353