
Updates in the Diagnosis and Management of Linear IgA Disease: A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
3. Results
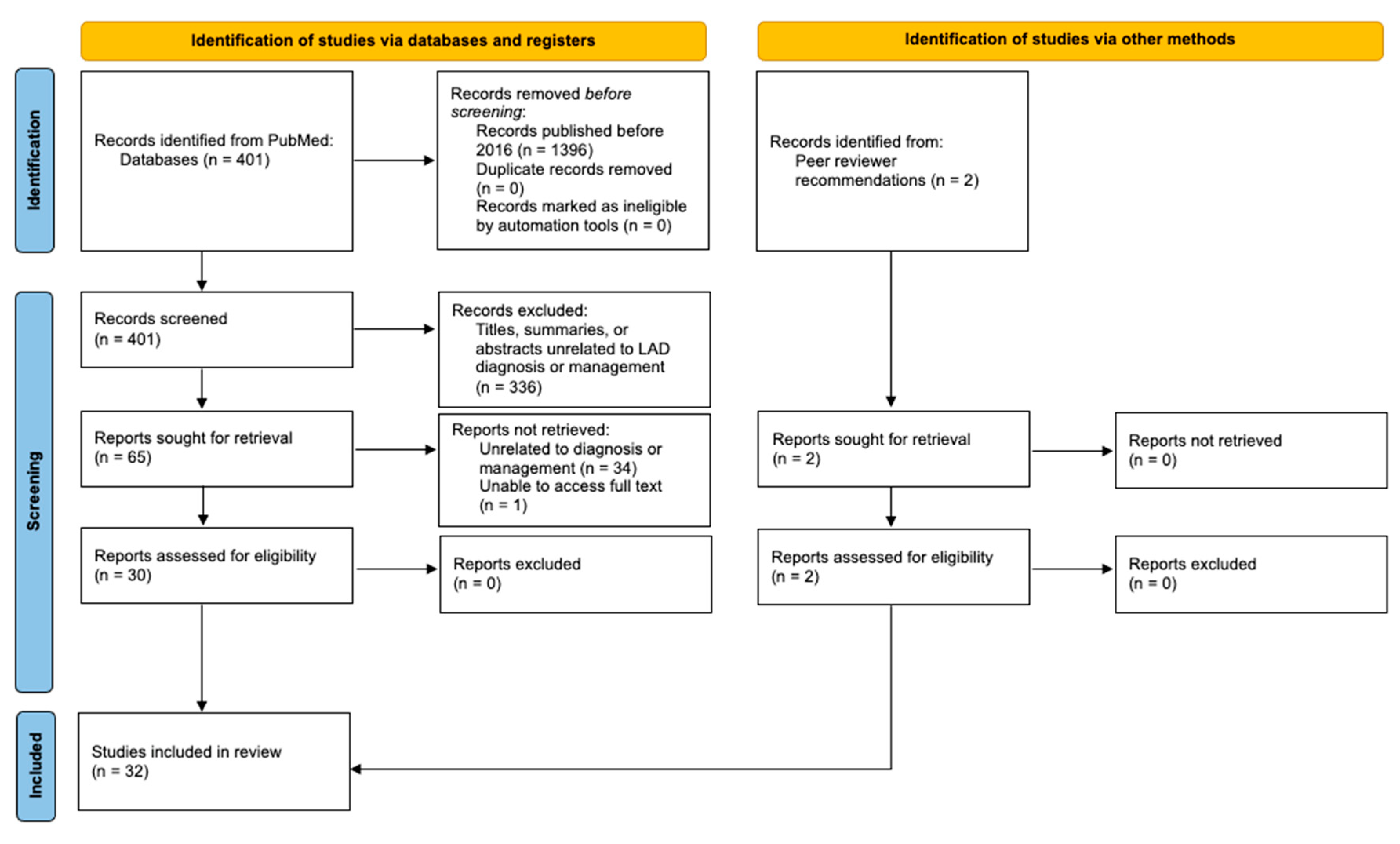
3.1. Literature Search
3.2. Diagnosis
3.3. Treatment
3.3.1. Rituximab
3.3.2. Methotrexate
3.3.3. Sulfonamides
3.3.4. IVIg
3.3.5. Topical Corticosteroids
3.3.6. Systemic Corticosteroids
3.3.7. Nicotinamide
3.3.8. Amoxicillin-Clavulanate
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bernett, C.N.; Fong, M.; Rosario-Collazo, J.A.; Linear, I.G.A. Dermatosis. [Updated 2021 Jan 15]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK526113/ (accessed on 29 June 2021).
- Hashimoto, T.; Yamagami, J.; Zone, J.J. History, Diagnosis, Pathogenesis, and Nomenclature in Sublamina Dense-Type Linear IgA Disease. JAMA Dermatol. 2021. [Google Scholar] [CrossRef]
- Winn, A.E.; Spillane, E.L.; Peterson, D.J.; Sperling, L.C.; Meyerle, J.H. False-negative direct immunofluorescence testing in vancomycin-induced linear IgA bullous dermatosis: A diagnostic pitfall. J. Cutan. Pathol. 2016, 43, 802–804. [Google Scholar] [CrossRef] [Green Version]
- Yamagami, J.; Nakamura, Y.; Nagao, K.; Funakoshi, T.; Takahashi, H.; Tanikawa, A.; Hachiya, T.; Yamamoto, T.; Ishida-Yamamoto, A.; Tanaka, T.; et al. Vancomycin Mediates IgA Autoreactivity in Drug-Induced Linear IgA Bullous Dermatosis. J. Investig. Dermatol. 2018, 138, 1473–1480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vale, E.C.S.D.; Dimatos, O.C.; Porro, A.M.; Santi, C.G. Consensus on the treatment of autoimmune bullous dermatoses: Dermatitis herpetiformis and linear IgA bullous dermatosis—Brazilian Society of Dermatology. An. Bras. Dermatol. 2019, 94, 48–55. [Google Scholar] [CrossRef]
- Yang, Z.; Liu, Z.; Sun, C.; Shen, H. Successful treatment of a case of idiopathic linear IgA bullous dermatosis with oral sulfasalazine. Dermatol. Ther. 2020, 33, e13210. [Google Scholar] [CrossRef]
- Cui, Y.X.; Yang, B.Q.; Zhou, G.Z.; Zhang, F.R. Childhood linear IgA bullous dermatosis successfully treated with oral nicotinamide. Clin. Exp. Dermatol. 2016, 41, 816–818. [Google Scholar] [CrossRef] [PubMed]
- Pinard, C.; Hebert, V.; Lecuyer, M.; Sacre, L.; Joly, P. Linear IgA bullous dermatosis treated with rituximab. JAAD Case Rep. 2019, 5, 124–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islamoğlu, Z.G.K.; Akyürek, F.T. A case of recalcitrant linear IgA bullous dermatosis: Successfully treated with rituximab. Dermatol. Ther. 2019, 32, e12911. [Google Scholar] [CrossRef]
- Lamberts, A.; Euverman, H.I.; Terra, J.B.; Jonkman, M.F.; Horváth, B. Effectiveness and Safety of Rituximab in Recalcitrant Pemphigoid Diseases. Front. Immunol. 2018, 9, 248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nedosekin, D.; Wilson, K.D.; Campbell, K.; Shalin, S.; Wong, H.K. Immunologic overlap in a case of linear IgG/IgA bullous dermatosis responsive to rituximab. JAAD Case Rep. 2021, 9, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Steger, B.; Madhusudan, S.; Kaye, S.B.; Stylianides, A.; Romano, V.; Maqsood, S.E.; Harper, J.; Ahmad, S. Combined Use of Rituximab and Intravenous Immunoglobulin for Severe Autoimmune Cicatricial Conjunctivitis—An Interventional Case Series. Cornea 2016, 35, 1611–1614. [Google Scholar] [CrossRef]
- Maalouf, N.S.; Hanna, D. Linear IgA bullous dermatosis successfully treated with omalizumab: A case report. JAAD Case Rep. 2019, 5, 966–969. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.H.; Padhiyar, J.K.; Patel, T.D.; Trivedi, N.S.; Chandibhamar, V.S.; Raval, R. A case of linear IgA bullous dermatosis successfully treated with omalizumab. Indian J. Dermatol. 2020, 65, 543–545. [Google Scholar] [CrossRef]
- Yetto, T.; Burns, C. Linear IgA bullous dermatosis associated with ulcerative proctitis: Treatment challenge. Derm. Online J. 2018, 24, 14. [Google Scholar] [CrossRef]
- Tate, C.; Christian, W.; Newell, L. Chronic Bullous Dermatosis of Childhood and the String of Pearls Sign. J. Pediatr. 2018, 202, 325–325.e1. [Google Scholar] [CrossRef] [Green Version]
- Prieto-Barrios, M.; Velasco-Tamariz, V.; Tous-Romero, F.; Burillo-Martinez, S.; Zarco-Olivo, C.; Rodriguez-Peralto, J.; Ortiz-Romero, P. Linear immunoglobulin A dermatosis mimicking toxic epidermal necrolysis: A case report of etanercept treatment. Br. J. Dermatol. 2017, 178, 786–789. [Google Scholar] [CrossRef]
- Patsatsi, A.; Lamprou, F.; Kokolios, M.; Stylianidou, D.; Trigoni, A.; Kalampalikis, D.; Sotiriadis, D. Spectrum of Autoimmune Bullous Diseases in Northern Greece. A 4-year Retrospective Study and Review of the Literature. Acta Dermatovenerol. Croat. 2017, 25, 195–201. [Google Scholar]
- Scarpone, R.; Meier, K.; Ghoreschi, K.; Worm, M. Intravenous Immunoglobulins in a Series of 32 Rare and Recalcitrant Immune Dermatoses. Acta Derm. Venereol. 2020, 100, adv00298. [Google Scholar] [CrossRef] [PubMed]
- Gil Sáenz, F.J.; Urdániz, G.D.; Galar, M.F.; Ballester, J.G.; Varasa, A.H.; Bordege, R.G. Corticoides tópicos como alternativa terapéutica en la dermatosis ampollosa por inmunoglobulina A lineal de la infancia. Caso clínico. Arch. Argent. Pediatr. 2016, 114, e440–e443. [Google Scholar] [CrossRef]
- Mazurek, M.T.; Banihani, R.; Wong, J.; Weinstein, M.; Alnutayfi, A.; Etoom, Y. Uncomplicated Neonatal Linear IgA Bullous Dermatosis: A Case Report. J. Cutan. Med. Surg. 2018, 22, 431–434. [Google Scholar] [CrossRef]
- Fulton, E.; Jan, F.; Zimarowski, M.J. Flame figures in linear IgA bullous dermatosis: A novel histopathologic finding. Dermatol. Online J. 2017, 23, 17. [Google Scholar] [CrossRef]
- Shetty, V.M.; Pai, S.B.; Rao, R. Linear IgA bullous dermatosis presenting as chronic prurigo: Unveiling of the diagnosis by serrated pattern analysis. Int. J. Dermatol. 2018, 57, e147–e149. [Google Scholar] [CrossRef]
- Becker, M.; Schumacher, N.; Schmidt, E.; Zillikens, D.; Sadik, C.D. Evaluation and Comparison of Clinical and Laboratory Characterstics of Patients With IgA Epidermolysis Bullosa Acquisita, Linear IgA Bullous Dermatosis, and IgG Epidermolysis Bullosa Acquisita. JAMA Dermatol. 2021. [Google Scholar] [CrossRef]
- Fernandes, K.D.A.P.; Galvis, K.H.; Gomes, A.C.D.M.S.; Nogueira, O.M.; Felix, P.A.O.; Vargas, T.J.D.S. Linear IgA and IgG bullous dermatosis. An. Bras. Dermatol. 2016, 91 (Suppl. 1), 32–34. [Google Scholar] [CrossRef] [Green Version]
- Lim, G.H.; Cai, S.C.S.; Lee, J.S.S.; Chen, Q. Rare case of linear IgA bullous dermatosis showing IgA, IgG and IgM reactivity. Australas. J. Dermatol. 2021, 62, e361–e362. [Google Scholar] [CrossRef] [PubMed]
- Ohata, C.; Ishii, N.; Koga, H.; Nakama, T. A clinical and serological study of linear IgA bullous dermatosis without linear immunoglobulin deposition other than IgA at the basement membrane zone using direct immunofluorescence. Br. J. Dermatol. 2016, 177, 152–157. [Google Scholar] [CrossRef]
- Nanda, A.; Lazarevic, V.; Rajy, J.M.; Almasry, I.M.; AlSabah, H.; AlLafi, A. Spectrum of autoimmune bullous diseases among children in Kuwait. Pediatr. Dermatol. 2020, 38, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Machado, T.Y.S.; Enokihara, M.M.S.E.S.; Iida, T.M.; Porro, A.M. Adult linear IgA bullous dermatosis: Report of three cases. An. Bras. Dermatol. 2018, 93, 435–437. [Google Scholar] [CrossRef] [PubMed]
- Varo, R.; Fernández-Luis, S.; Sitoe, A.; Bassat, Q. Suspected case of chronic bullous disease of childhood in a rural area of Southern Mozambique. BMJ Case Rep. 2017, 2017, bcr2016218315. [Google Scholar] [CrossRef] [Green Version]
- Giraud, L.; Welfringer-Morin, A.; Boccara, O.; Frassati-Biaggi, A.; Leclerc-Mercier, S.; Grootenboer-Mignot, S.; Bodemer, C.; Hadj-Rabia, S. Neonatal and self-healing linear immunoglobulin A dermatosis. J. Eur. Acad. Dermatol. Venereol. 2019, 34, e86–e87. [Google Scholar] [CrossRef]
- Egami, S.; Suzuki, C.; Kurihara, Y.; Yamagami, J.; Kubo, A.; Funakoshi, T.; Nishie, W.; Matsumura, K.; Matsushima, T.; Kawaida, M.; et al. Neonatal Linear IgA Bullous Dermatosis Mediated by Breast Milk–Borne Maternal IgA. JAMA Dermatol. 2021. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Drug | Dose | Age (Years) | Drug-Induced LAD (Y/N) | Time to Clearance (yrs/m/w/d) | Relapse (Y/N) | Side Effects of Treatment |
|---|---|---|---|---|---|---|
| Rituximab + prednisone + MMF [11] | Rituximab: 375 mg/m2 weekly × 4 w Prednisone: 0.5 mg/kg (80 mg) tapered over 1 m MMF: 500 mg | 43 | N | 1 m | Y, 9 m later | NS |
| Rituximab + dapsone + topical corticosteroids + MMF [8] | Rituximab: 2 infusions of 1 g 2 w apart × 2 Dapsone: unspecified Topical corticosteroids: unspecified MMF: 3 g/d to 500 mg/d | 35 | Unknown | 14 m | Y, 6 m later | NS |
| Rituximab + dapsone + IVIg [9] | Rituximab: 1 g × 2 cycles Dapsone: 100 mg to 50 mg IVIg: 2 g/kg/cycle | 33 | N | 7 w | N | None |
| Rituximab + dapsone + prednisone + doxycycline + MMF [8] | Rituximab: 2 infusions of 1 g 2 w apart × 2 Dapsone: 200 mg/d Prednisone: 0.1 mg/kg/d Doxycycline: 200 mg/d MMF: 1 g/d | 30 | Unknown | 20 m | N | NS |
| Rituximab + IVIg [12] | Rituximab: 2 infusions of 1 g 2 w apart IVIg: 2 g/kg/cycle divided over 3 d × 2 | 21 | Unknown | 17 m follow-up showed improvement in visual acuity and less conjunctival cicatrization | N | None * |
| Omalizumab | Dose regimen 1: Subcutaneous 300 mg every m × 6 m [13] Dose regimen 2: Subcutaneous 300 mg every m × 3 m [14] | 55 40 | N Unknown | 3 w 4.5 m | Y, within 1 m of cessation N | NS NS |
| Etanercept [17] | 50 mg × 1 | 65 | Y | 4 d | NS | None |
| Methotrexate + mesalamine ** after high dose prednisone + IV methylprednisolone [15] | Methotrexate: 22.5 mg/w Mesalamine: unspecified Prednisone: unspecified Methylprednisone: 3 d course | 58 | N | NS, but near clearance achieved | NS | NS |
| Sulfasalazine [6] | 40–60 mg/kg daily | 17 | N | 2 m | N | None |
| Sulfamethoxypyridazine [28] | 250 mg–1 g/d | 7 | N | 60 m | N | NS |
| IVIg + prednisolone [19] | IVIg: 2 g/kg or 0.4 g/kg for a median of 6 doses over 2–5 d + Prednisolone: 5–10 mg/d | Unspecified, range of 64–84 | Unknown | NS | N | None *** |
| IVIg + prednisolone [28] | IVIg: 2 g/kg/cycle × 8 Prednisolone: 0.5–1 mg/kg/d | 13 | N | 30 m | N | NS |
| IVIg [28] | 2 g/kg/cycle × 8 cycles | 9, 1.7 | N | 96 m, 7 m | N | NS |
| IVIg + prednisolone + clarithromycin [28] | IVIg: 2 g/kg/cycle monthly × 5 Prednisolone: 1 mg/kg/d Clarithromycin: 30 mg/kg/d over 3 doses | 1 | N | 6 m | N | NS |
| Dapsone + prednisone [29] | Dapsone: 50 mg/d Prednisone: 0.6 mg/kg (60 mg/d) | 51 | N | 2.5 yrs | N | NS |
| Dapsone + prednisone [29] | Dapsone: 50 mg/d Prednisone: 1 mg/kg/d (60 mg/d) tapered to 10 mg/d | 44 | N | Clearance not achieved | Clearance not achieved | Glaucoma, arterial hypertension, osteoporosis, Cushingoid facies |
| Prednisone [29] | 20 mg/d monthly dose tapering | 30 | Unknown | NS | Y | NS |
| Dapsone + prednisolone [28] | Dapsone: 1–2 mg/kg/d Prednisolone: 0.5–1 mg/kg/d in tapering doses | 13, 9, 7, 1 | N | 60 m, 156 m, 108 m, 24 m | N | NS |
| Oral corticosteroids [30] | Unspecified | 8 | NS | 4 m | NS | NS |
| Oral prednisolone + corticosteroid eye drops [25] | 0.5 mg/kg/d | 7 | NS | NS, but had eyelid adhesion despite clinical control | NS | NS |
| Dapsone + prednisolone + cyclosporine [16] | Dapsone: 0.5–2 mg/kg; Prednisolone: 0.5–1 mg/kg Cyclosporine: dose unspecified | 5 | N | NS, but is well-controlled | NS | NS |
| Topical triamcinolone + vancomycin cessation [3] | Triamcinolone 0.1% ointment | 74 | Y | NS, but clearance was achieved | NS | NS |
| Topical methylprednisolone + clobetasol shampoo [20] | Methylprednisolone: 0.1% BID × 8 w | 6 | N | 5–8 w | N | NS |
| Topical corticosteroids + clarithromycin [28] | Topical corticosteroids: mid-potency, unspecified Clarithromycin: 30 mg/kg/d over 3 doses × 1 m | 5 | N | 2.5 m | N | NS |
| Topical corticosteroids [28] | Mid-potency, unspecified | 4 | N | 2.5 m | N | NS |
| Betamethasone valerate [21] | 0.05% | 4 d | N | 21 d | NS | NS |
| Nicotinamide [7] | 300 mg/d | 22 m | N | 7 d | N | None |
| Amoxicillin-clavulanate [31] | Infusion × 7 d | 7 d | N | 7 d | N | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, L.; Gardner, J.T., II; Dao, H., Jr. Updates in the Diagnosis and Management of Linear IgA Disease: A Systematic Review. Medicina 2021, 57, 818. https://doi.org/10.3390/medicina57080818
Shin L, Gardner JT II, Dao H Jr. Updates in the Diagnosis and Management of Linear IgA Disease: A Systematic Review. Medicina. 2021; 57(8):818. https://doi.org/10.3390/medicina57080818
Chicago/Turabian StyleShin, Leah, Jeffrey T. Gardner, II, and Harry Dao, Jr. 2021. "Updates in the Diagnosis and Management of Linear IgA Disease: A Systematic Review" Medicina 57, no. 8: 818. https://doi.org/10.3390/medicina57080818
APA StyleShin, L., Gardner, J. T., II, & Dao, H., Jr. (2021). Updates in the Diagnosis and Management of Linear IgA Disease: A Systematic Review. Medicina, 57(8), 818. https://doi.org/10.3390/medicina57080818