
Treatment Outcomes of Langerhans Cell Histiocytosis: A Retrospective Study

 ,
,
Abstract
1. Introduction
2. Patients and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fletcher, C.D.; Lazar, A.J. WHO classification of tumors of soft tissue and bone. In Soft Tissue and Bone Tumours, 5th ed.; IARC Publications: Lyon, France, 2020; pp. 492–494. [Google Scholar]
- Krooks, J.; Minkov, M.; Weatherall, A.G. Langerhans cell histiocytosis in children: History, classification, pathobiology, clinical manifestations, and prognosis. J. Am. Acad. Dermatol. 2018, 78, 1035–1044. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.K.; Park, C.J.; Jang, S.; Cho, Y.U.; Park, S.H.; Koh, K.N.; Im, H.J.; Seo, J.J. Bone marrow involvement of Langerhans cell histiocytosis: Immunohistochemical evaluation of bone marrow for CD1a, langerin, and S100 expression. Histopathology 2014, 65, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Islinger, R.B.; Kuklo, T.R.; Owens, B.D.; Horan, P.J.; Choma, T.J.; Murphey, M.D.; Temple, H. Langerhans’ cell histiocytosis in patients older than 21 years. Clin. Orthop. Relat. Res. 2000, 379, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Ando, S.; Kawamata, T.; Makiyama, J.; Yokoyama, K.; Imai, Y.; Tojo, A. Clinical features and outcomes of adult Langerhans cell histiocytosis: A single-center experience. Int. J. Hematol. 2020, 112, 185–192. [Google Scholar] [CrossRef]
- Minkov, M. Multisystem Langerhans cell histiocytosis in children: Current treatment and future directions. Pediatr. Drugs 2011, 13, 75–86. [Google Scholar] [CrossRef]
- Radzikowska, E. Pulmonary Langerhans’ cell histiocytosis in adults. Adv. Respir. Med. 2017, 85, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Kilpatrick, S.E.; Wenger, D.E.; Gilchrist, G.S.; Shives, T.C.; Wollan, P.C.; Unni, K.K. Langerhans’ cell histiocytosis (histiocytosis X) of bone. A clinicopathologic analysis of 263 pediatric and adult cases. Cancer 1995, 76, 2471–2484. [Google Scholar] [CrossRef]
- Howarth, D.M.; Gilchrist, G.S.; Mullan, B.P.; Wiseman, G.A.; Edmonson, J.H.; Schomberg, P.J. Langerhans cell histiocytosis: Diagnosis, natural history, management, and outcome. Cancer 1999, 85, 2278–2290. [Google Scholar] [CrossRef]
- Kim, B.E.; Koh, K.N.; Suh, J.K.; Im, H.J.; Song, J.S.; Lee, J.W.; Kang, H.J.; Park, K.D.; Shin, H.Y.; Choi, H.S.; et al. Korea Histiocytosis Working Party. Clinical features and treatment outcomes of Langerhans cell histiocytosis: A nationwide survey from Korea Histiocytosis Working Party. J. Pediatr. Hematol. Oncol. 2014, 36, 125–133. [Google Scholar] [CrossRef]
- Weitzman, S.; Egeler, R.M. Langerhans cell histiocytosis: Update for the pediatrician. Curr. Opin. Pediatr. 2008, 20, 23–29. [Google Scholar] [CrossRef]
- Van Nieuwenhuyse, J.P.; Clapuyt, P.; Malghem, J.; Everarts, P.; Melin, J.; Pauwels, S.; Brichard, B.; Ninane, J.; Vermylen, C.; Cornu, G. Radiographic skeletal survey and radionuclide bone scan in Langerhans cell histiocytosis of bone. Pediatr. Radiol. 1996, 26, 734–738. [Google Scholar] [CrossRef]
- Azouz, E.M.; Saigal, G.; Rodriguez, M.M.; Podda, A. Langerhans’ cell histiocytosis: Pathology, imaging and treatment of skeletal involvement. Pediatr. Radiol. 2005, 35, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Haupt, R.; Minkov, M.; Astigarraga, I.; Schäfer, E.; Nanduri, V.; Jubran, R.; Egeler, R.M.; Janka, G.; Micic, D.; Rodriguez-Galindo, C.; et al. Langerhans cell histiocytosis (LCH): Guidelines for diagnosis, clinical work-up, and treatment for patients till the age of 18 years. Pediatr. Blood Cancer 2013, 60, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.R.; Yoon, H.M.; Jung, A.Y.; Cho, Y.A.; Seo, J.J.; Lee, J.S. Comparison of whole-body MRI, bone scan, and radiographic skeletal survey for lesion detection and risk stratification of Langerhans cell histiocytosis. Sci. Rep. 2019, 9, 317. [Google Scholar] [CrossRef] [PubMed]
- Phillips, M.; Allen, C.; Gerson, P.; McClain, K. Comparison of FDG-PET scans to conventional radiography and bone scans in management of Langerhans cell histiocytosis. Pediatr. Blood Cancer 2009, 52, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Binkovitz, L.A.; Olshefski, R.S.; Adler, B.H. Coincidence FDG-PET in the evaluation of Langerhans’ cell histiocytosis: Preliminary findings. Pediatr. Radiol. 2003, 33, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Kaste, S.C.; Rodriguez-Galindo, C.; McCarville, M.E.; Shulkin, B.L. PET-CT in pediatric Langerhans cell histiocytosis. Pediatr. Radiol. 2007, 37, 615–622. [Google Scholar] [CrossRef]
- Khung, S.; Budzik, J.F.; Amzallag-Bellenger, E.; Lambilliote, A.; Soto Ares, G.; Cotten, A.; Boutry, N. Skeletal involvement in Langerhans cell histiocytosis. Insights Imaging 2013, 4, 569–579. [Google Scholar] [CrossRef]
- Oh, B.; Lee, S.; Ke, Y.; Kimpo, M.; Yeoh, A.; Quah, T.C. A “wait-and-see” approach to quiescent single-system Langerhans cell histiocytosis to spare children from chemotherapy. Front. Pediatr. 2020, 8, 466. [Google Scholar] [CrossRef]
- Gadner, H.; Minkov, M.; Grois, N.; Pötschger, U.; Thiem, E.; Aricò, M.; Astigarraga, I.; Braier, J.; Donadieu, J.; Henter, J.I.; et al. Histiocyte Society. Therapy prolongation improves outcome in multi-system Langerhans cell histiocytosis. Blood 2013, 121, 5006–5014. [Google Scholar] [CrossRef]
- Morimoto, A.; Shimazaki, C.; Takahashi, S.; Yoshikawa, K.; Nishimura, R.; Wakita, H.; Kobayashi, Y.; Kanegane, H.; Tojo, A.; Imamura, T.; et al. Therapeutic outcome of multifocal Langerhans cell histiocytosis in adults treated with the Special C regimen formulated by the Japan LCH Study Group. Int. J. Hematol. 2013, 97, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Donadieu, J.; Bernard, F.; van Noesel, M.; Barkaoui, M.; Bardet, O.; Mura, R.; Arico, M.; Piguet, C.; Gandemer, V.; Armari Alla, C.; et al. Cladribine and cytarabine in refractory multi-system Langerhans cell histiocytosis: Results of an international phase 2 study. Blood 2015, 126, 1415–1423. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient No. | Age (Years) | Sex | Site | Imaging Tool for Diagnosis | Symptom | Comorbidity | Biopsy Site | Treatment | Outcome | Follow-Up Period (Months) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 24 | F | Rt tibia, left seventh rib | Radiography, scintigraphy, PET-CT | Pain and swelling | None | Tibia | Spontaneous regression | CDF | 13 |
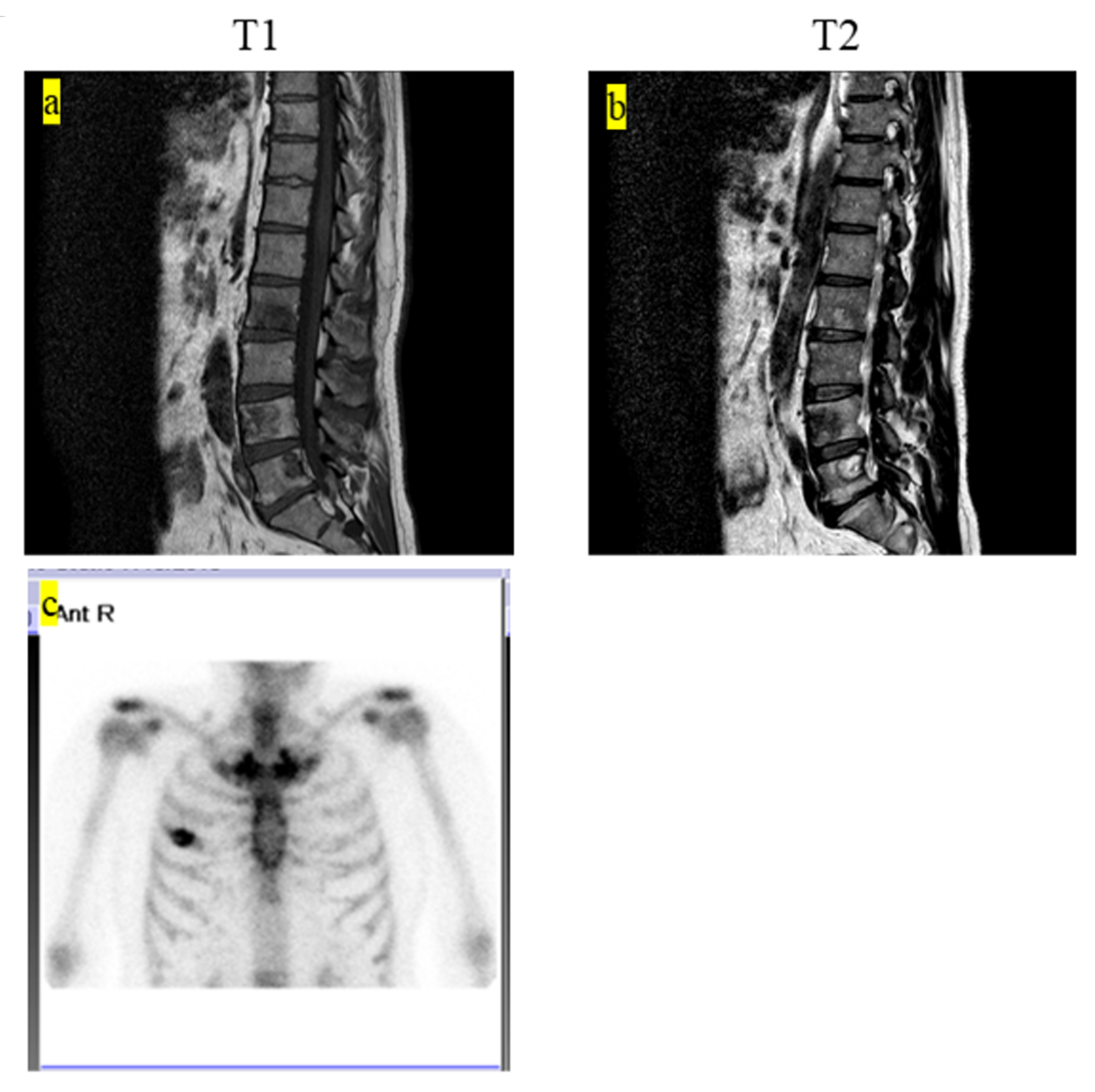
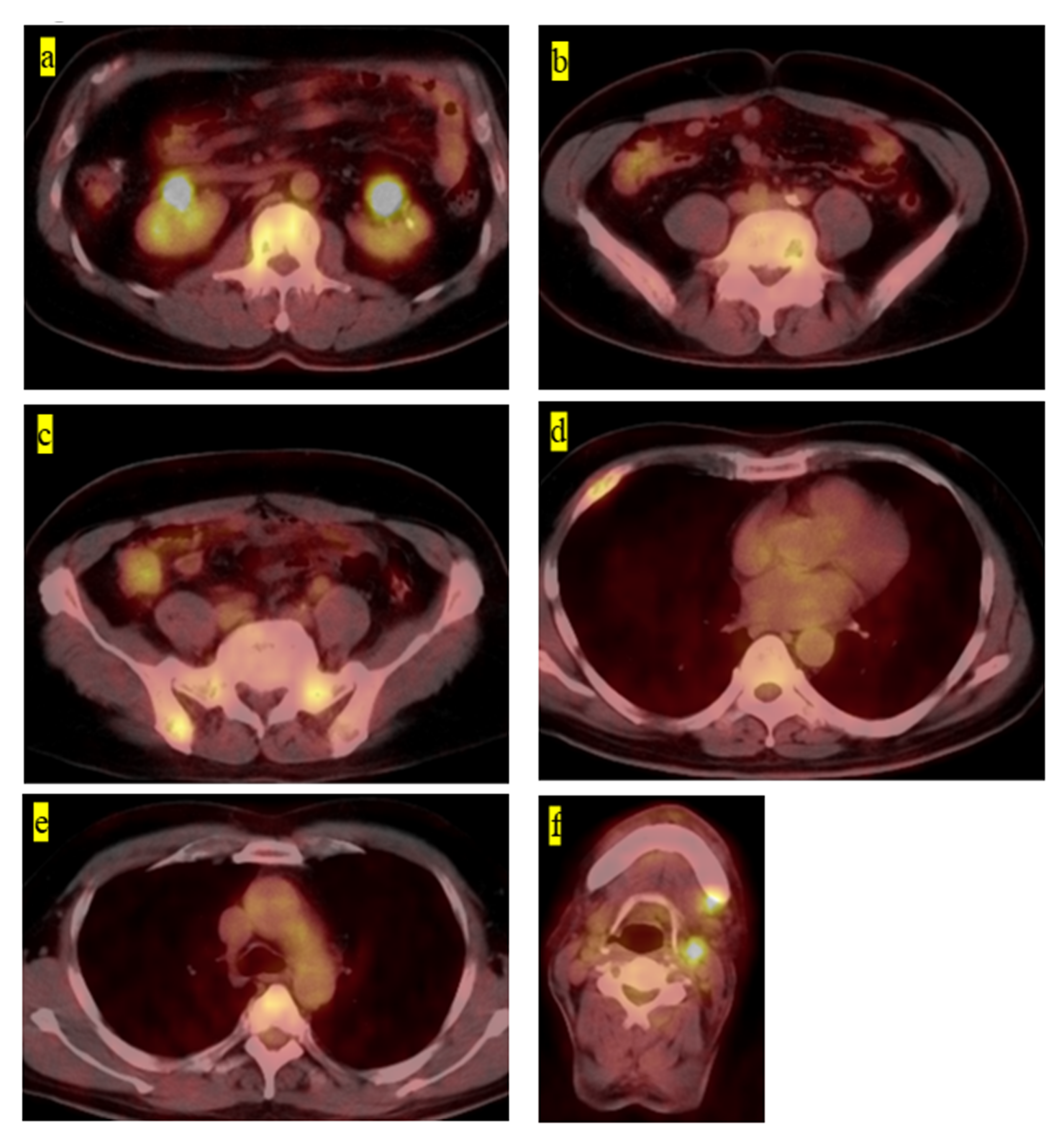
| 2 | 60 | M | Second, third, fourth, fifth lumbar, Th10, rt fourth rib, sacrum, pelvic | Radiography, MRI, PET-CT | Without symptoms | Hepatitis B | Fifth lumbar | Chemotherapy (6-mercaptopurine 110 mg, MTX 2.5 mg, PSL 5 mg) | CDF | 63 |
| 3 | 30 | F | Rt fourth rib | Radiography, scintigraphy, CT, MRI, contrast-enhanced MRI | Pain | None | Rt fourth rib | Natural observation | AWD | 4 |
| 4 | 2 | F | Femur, eighth thoracic vertebra | Radiography, MRI | Pain and claudication | None | Femur | Spontaneous regression | CDF | 27 |
| 5 | 2 | M | Femur, temporal bone, anterior mediastinum | Radiography, scintigraphy | Pain and claudication | Autism | Femur | Chemotherapy (cladribine 5 mg/m2 and cytarabine 500 mg/m2) | CDF | 55 |
| 6 | 3 | M | Elbow | Radiography, Scintigraphy | Pain | None | Radius | Spontaneous regression | CDF | 73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hashimoto, K.; Nishimura, S.; Sakata, N.; Inoue, M.; Sawada, A.; Akagi, M. Treatment Outcomes of Langerhans Cell Histiocytosis: A Retrospective Study. Medicina 2021, 57, 356. https://doi.org/10.3390/medicina57040356
Hashimoto K, Nishimura S, Sakata N, Inoue M, Sawada A, Akagi M. Treatment Outcomes of Langerhans Cell Histiocytosis: A Retrospective Study. Medicina. 2021; 57(4):356. https://doi.org/10.3390/medicina57040356
Chicago/Turabian StyleHashimoto, Kazuhiko, Shunji Nishimura, Naoki Sakata, Masami Inoue, Akihisa Sawada, and Masao Akagi. 2021. "Treatment Outcomes of Langerhans Cell Histiocytosis: A Retrospective Study" Medicina 57, no. 4: 356. https://doi.org/10.3390/medicina57040356
APA StyleHashimoto, K., Nishimura, S., Sakata, N., Inoue, M., Sawada, A., & Akagi, M. (2021). Treatment Outcomes of Langerhans Cell Histiocytosis: A Retrospective Study. Medicina, 57(4), 356. https://doi.org/10.3390/medicina57040356