Abstract
Vitreoretinal surgeries require the administration of general anesthesia (GA) in selected groups of patients. The administration of intraoperative rescue narcotic analgesia (IRNA) during GA poses the risk of postoperative nausea and vomiting (PONV). The surgical pleth index (SPI), a crucial component of the adequacy of anesthesia (AoA) guidance of GA, optimizes the intraoperative titration of IRNA. The current analysis evaluated the risk factors for the occurrence of PONV and the oculo-cardiac reflex (OCR) in patients undergoing pars plana vitrectomy (PPV) under AoA guidance. In total, 175 patients undergoing PPV were randomly allocated to receive either GA with SPI-guided IRNA administration using fentanyl alone or in addition to different preoperative analgesia techniques. Any incidence of PONV or OCR was recorded. Obesity, overweight, smoking status, motion sickness, postoperative intolerable pain perception, female gender, fluid challenge and arterial hypertension did not correlate with an increased incidence of PONV or OCR under AoA guidance. Diabetes mellitus, regardless of insulin dependence, was found to correlate with the increased incidence of PONV. The AoA regimen including SPI guidance of IRNA presumably created similar conditions for individual subjects, so no risk factors of the occurrence of PONV or OCR were found, except for diabetes mellitus. We recommend using AoA guidance for GA administration to reduce OCR and PONV rates.
1. Introduction
Vitreoretinal surgeries (VRS) are increasingly common operations in ophthalmology due to the expansion of the geriatric and diabetic populations. Although in many centers VRS are performed under regional anesthesia (RA) accompanied by monitored anesthesia care (MAC) [1,2], there is a growing number of patients (especially among the elderly) who require immobilization on the operating table under general anesthesia (GA) [3]. GA alone is, however, very often associated with adverse complications due to the use of intraoperative rescue narcotic analgesia (IRNA), which was identified as a risk factor for postoperative nausea and vomiting (PONV) in the first 24 h after VRS. Therefore, the use of IRNA should be avoided when possible, as any incidence of PONV can reduce patients’ comfort and satisfaction, and anesthesia may also lead to increases in intraocular pressure and blood pressure, deteriorating the effect of the performed VRS (wound dehiscence, iris prolapse and intraocular bleeding) [4]. On the other hand, insufficient intraoperative analgesia is supposed to lead to life-threatening hemodynamic disturbances, the occurrence of oculo-cardiac reflex (OCR) and increased postoperative pain perception. Therefore, in order to minimize this negative impact, different techniques of pre-emptive analgesia (PA) are employed, which can minimize the necessity of IRNA administration.
The use of IRNA should be rational but monitoring the efficacy of analgesia remains a challenge during GA, as volatile anesthetics have been proven to blunt the hemodynamic effect of surgical stimulation expressed as increases in heart rate and blood pressure [5]. Bergmann et al. [6] reported fewer adverse events, a reduced demand for IRNA and shorter emergence from anesthesia when the titration of IRNA was based upon the observance of Surgical Pleth Index (SPI) fluctuations, which is a crucial component of the adequacy of anesthesia (AoA) concept of the guidance on general anesthesia (GA) [7]. SPI is derived from the photoplethysmography waveform amplitude and the heartbeat-to-beat interval. Several studies have proven that fluctuations in the SPI value reflect the nociceptive–anti-nociceptive balance [8,9]. Changes in the SPI value are reported to correspond to the serum opioid concentration [10], so SPI guidance seems to be an excellent tool for the administration of intraoperative RNA as the display of its fluctuations on a monitor in digital form (0—no pain; 100—maximum pain) facilitates its intraoperative use and interpretation [5,6].
In our previous studies, we investigated the influence of the AoA guidance on GA in patients undergoing pars plana vitrectomy (PPV) on the rate of incidence of postoperative intolerable pain perception (PIPP), hemodynamic stability [11], and the rate of incidence of OCR and PONV [12]. The current analysis aimed to identify risk factors for the occurrence of OCR or PONV when AoA guidance for GA alone or combined with different PA techniques was utilized.
2. Results
The analysis in this study involved a total of 175 patients: 97 (55.4%) women and 78 (44.6%) men. The patients were divided into five equal groups: patients who received general anesthesia (GA); patients who received preoperative analgesia (PA) using metamizole (M); patients who exhibited preprocedural peribulbar block (PBB group) using a mixture of lignocaine and bupivacaine with Hamilton’s technique 1 min before induction of GA; patients who exhibited preprocedural peribulbar block (PBB group) using paracetamol (P); patients who received preventive topical analgesia by triple instillation of 2% proparacaine (T). Each group contained 35 patients (20%). The detailed characteristics of patients’ anthropometric data are shown in the supplementary materials (Table S1). The statistical analysis showed no statistically significant differences in the anthropometric data (p > 0.05).
In the first step of our study, we analyzed the rate of postoperative pain perception, OCR and PONV in patients in accordance with their group allocation. It was observed that the highest number of patients with NRS > 3 was in the M and T groups (eight patients; 22.9%), whereas in the GA and P groups, this was six patients (17.1%), and five patients in the PBB group (14.3%). The differences were not statistically significant (p > 0.05). The statistical analysis showed significantly higher fentanyl (FNT) values in the M group (165.7 ± 116.8 mg) in comparison to other groups (GA—144.3 ± 102.7 mg; p—95.7 ± 81.7 mg; PBB—95.1 ± 101.3 mg; T—148.6 ± 120.3 mg; p < 0.05). In addition, the performed analysis indicated that regardless of the PA technique used there were relatively small and statistically insignificant negative postoperative reactions—PONV and OCR. The rate of OCR was assessed in each group (M—six patients; GA group—four patients; P and PBB groups—four patients; T—three patients; p > 0.05) as well as PONV (M—six patients; GA, P and T group—four patients; T—three patients; p > 0.05).
The mean demand for IRNA had no significant impact on the occurrence of PONV and OCR, despite the group allocation, although a significantly higher demand for intraoperative IRNA using FNT was recorded among patients in the M group as compared to the PBB group (Table 1).

Table 1.
Comparison of intraoperative FNT requirement in patients with incidence of PONV and OCR according to group allocation.
In the last stage of our research, we analyzed whether gender, BMI, diabetes mellitus, motion sickness or smoking status had any influence on the occurrence of PONV, OCR and NRS > 3. The data are shown in Table 2 and Figure 1. The performed statistical analysis indicated that only the relationship between diabetes mellitus and PONV risk was statistically significant (p < 0.05). We did not observe any significantly different correlations between the analyzed parameters (p > 0.05).
Table 2.
Crude odds ratio and its 95% confidence interval (CI) for occurrence of OCR and PONV according to analyzed risk factors, despite group allocation.
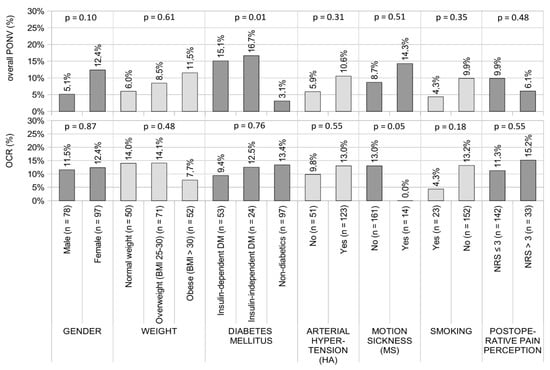
Figure 1.
Results of the relationship between gender, BMI, diabetes mellitus, arterial hypertension, motion sickness, smoking status, NRS > 3 and the occurrence of PONV and OCR. Results presented as percentages for nominal variables. p-values obtained by the X2 test for nominal variables; pairwise comparison of proportions: significant differences in percentages between the non-DM and DM groups (p < 0.05). Abbreviations: PONV—postoperative nausea and vomiting; OCR—oculocardiac reflex; NRS—numeric pain rating scale.
3. Discussion
Incidences of intraoperative OCR and PONV both constitute a challenge for the anesthesiologist intraoperatively and in the PACU, as well as for the staff of the department of ophthalmology postoperatively. Therefore, there have been attempts made to optimize the anesthetic regimen in order to minimize their occurrence and identify the risk factors for their presence in order to provide the individuals at risk with even more extensive care and supervision [13].
The utility of the adequacy of anesthesia (AoA) technique of intraoperative monitoring (SPI alongside SE and e-NMT) created a comparable anesthetic regimen for each individual patient included in the current study. The utility of monitoring the depth of anesthesia using state entropy (SE) meant that every patient was subjected to almost the same concentration of volatile anesthetic (leading to similar suppression of brain activity).
As a result of the steady suppression of brain activity expressed using SE within the target value of 40–45, each patient was expected to perceive the painful surgical stimulation during PPV with the same intensity; when the intravenous or regional PA was insufficient, ∆SPI > 15. The utility of SPI to guide IRNA administration, contrary to IRNA guidance based on the anesthesiologic intuition and observance of hemodynamic changes, created comparable conditions to administer IRNA to individual patients, as IRNA administration based on changes in the SPI value was proven to correspond to the serum opioid concentration [10]. Therefore, the employment of AoA enabled the analysis of risk factors of the occurrence of PONV and OCR, as under such an anesthetic regimen only individual characteristics could presumably be responsible for their presence and enabled a reliable risk factor analysis. Numerous reliable PA regimens were successfully undertaken to eradicate PONV and ensure a smooth postoperative recovery [1,13,14,15,16].
Based on the current literature, numerous studies were performed to identify the risk factors of the occurrence of PONV. Female gender, smoking status, motion sickness, the predictive use of narcotic analgesics (constituting Apfel score), history of DM (insulin dependent or insulin independent), obesity, and anesthetic regimen were considered to be potential risk factors for the occurrence of PONV [17].
In the study of Nitahara et al. [18] concerning risk factors for the occurrence of PONV after PPV, female gender, lower BMI and inhalational anesthesia were found to constitute the main risk factors for the occurrence of PONV after PPV performed in adults. In their study, female patients were also found to have a 3.1–5.8 times higher risk of the occurrence of PONV in comparison to male patients, and this gender difference was found to constitute the only factor influencing the incidence of PONV throughout the period of observation in their study. They observed the incidence of nausea in 16 males and 41 females and incidences of vomiting in 11 males and 26 females out of 247 patients, meeting the inclusion criteria for this study, as compared to 4 males and 12 females out of 175 patients in the current study, which was not statistically significant.
In the study of Iwamoto et al. [19], female gender was found to be a risk factor of PONV, regardless of the type of ophthalmic surgery, similar to the findings of several other studies [20,21,22], and they found droperidol to be an efficient antiemetic agent in the group of female patients. Similar to the observations of Apfel et al. [23], they also found that inhalational anesthesia correlated with increased incidence of nausea, observed in 24 cases compared to 6 incidences in propofol anesthesia. Propofol was found to reduce the rate of incidence of PONV due to its direct antiemetic properties [24] that are widely used to prevent PONV in patients undergoing thyroidectomy [25], cesarean section [26] and laparoscopic cholecystectomy [27]. Nevertheless, during maintenance of GA we used sevoflurane due to its pre-conditioning properties of ameliorating myocardial ischemia/reperfusion injury in diabetic patients [28] who constituted about 44% of patients in our study.
Despite the group allocation, in the current study, sevoflurane was used to conduct GA, resulting in an overall incidence of PONV in a total of 9% of patients, which is a relatively satisfying result.
There are conflicting data regarding the influence of overweight or obesity on the rate of incidence of PONV. Watcha et al. [29] hypothesized the incidence of PONV to be increased in obese subjects due to possible causative factors, such as a larger volume of adipose tissue, larger residual gastric volume and difficulties in mask ventilation, contrary to the findings of Apfel et al. [23] and Kranke et al. [25], who did not observe any relationship between increased BMI and the rate of incidence of PONV [25]. As only 1.6% of subjects were obese in the study of Nitahara et al. [18], which showed a decreased incidence of PONV in this group of patients, in contrast to 10.1% in the review of Kranke et al. [30], the conclusion regarding no influence of BMI > 30 on the rate of PONV is convincing. Kim et al. [31], in their study of 113,881 patients who underwent GA, showed that an increased BMI reduced the incidence of PONV [26], whereas being underweight did not. In the current study, the number of overweight patients was 72 (41.4%), whereas obesity was noted in 52 (29.9%). Therefore, the relatively high percentage of patients with abnormally increased weight, as compared to the abovementioned literature, might have contributed to the final low incidence of low overall PONV, supporting the theory of Kim et al. [31].
Numerous studies report the incidence of PONV to be decreased in patients with smoking status [20,32,33,34,35]. In the current study, only one smoker and 13 non-smokers developed PONV, as compared to 22 and 139 who did not, respectively, out of 175 subjects, which was not statistically insignificant. Our study findings are in concordance with the conclusion of Nitahara et al. [18] that smoking status has no predictive value for the occurrence of PONV when undergoing PPV. In their study, 42 non-smokers had nausea and 27 experienced vomiting out of 247 subjects, which was not statistically significant [18].
There are conflicting data concerning the influence of the administration of IRNA on the rate of incidence of PONV and OCR. Some reports identify IRNA as increasing the risk of the presence of PONV [36,37], as after IRNA administration approximately 40% of patients were found by some authors to be likely to experience nausea whereas 15–25% of patients experienced vomiting [14,38,39]. In other reports, meanwhile. such a correlation was not found, irrespective of the IRNA in question [40].
In ophthalmic surgery, the use of IRNA was identified as a risk factor for the presence of PONV by Mandelcorn et al. [41], who observed that postoperative nausea occurred almost three times more frequently among patients undergoing PPV under RA with conscious sedation who received IRNA as compared to patients who presented no such requirement. They concluded that the utility of IRNA was the only factor responsible for nausea in the postoperative period [41]. In the current study, such a correlation was not found. In our study, no correlation was found between the demand for IRNA and the incidence of PONV and OCR. To our surprise, the demand for IRNA was the highest among patients receiving metamizole, but the rate of incidence of PONV was the lowest in this group, similarly to patients receiving paracetamol, whose demand for IRNA was much lower, but a statistically significant difference was not found.
The declaration of PIPP, as understood by NRS > 3, also did not correlate with the rate of incidence of PONV in the current analysis. Contrary to our study findings, the reduction in the rate of incidence of PONV correlated significantly with the reduction in the pain score and not with reduced opioid use related to paracetamol application in the study of Apfel et al. [41]. They suggested either a direct link between the analgesic effect and PONV reduction or a direct effect of paracetamol on PONV, similarly to the observation made by Cok et al. [42] in children undergoing strabismus surgery who recorded a decreased rate of incidence of PONV during the first 24 h of receiving intraoperative intravenous paracetamol. Additionally, motion sickness did not correlate with the rate of incidence of PONV in the current analysis.
We also analyzed the possibility of coincidence between the two most common comorbidities of patients undergoing vitreoretinal surgeries, arterial hypertension and DM, in relation to the incidence of PONV [43,44,45]. Diabetic patients benefit from enhanced vision and improved lifestyle from the introduction of vitreoretinal surgeries [46].
In the current study, the history of DM, regardless of dependence on insulin, was identified as an independent risk factor for the incidence of PONV. Symptoms of PONV are classic and frequent gastroparesis following DM [47]. We suppose that this due to the fact that diabetic patients mainly suffer from nausea in the morning before eating, during the night and when not eating [48], which resembles a perioperative fasting regimen. PONV in these patients might have occurred either as a coincidence or as an immediate postoperative adverse event, induced by the delayed effect of IRNA in individual cases with diabetic autonomic neural imbalance progressing to diabetic autonomic neuropathy, delaying gastric emptying [49]. No correlation between the presence of HA and incidence of PONV was found, regardless of the group allocation.
According to the current literature, there are conflicting data concerning the influence of fluid management in the perioperative period on the rate of presence of PONV [50,51,52]. The perioperative administration of an adequate volume of intravenous fluid was reported to be able to correct the intravascular volume deficits, finally reducing PONV [53,54].
Apfel et al. [53] concluded in their review that the supplemental intravenous administration of crystalloids played a key preventive role in the management of PONV, which is an inexpensive and non-pharmacological modality that reduces the incidence rate of PONV that is free from the observable side effects of pharmacological therapy [53]. Mallick-Searle et al. [37], in their study concerning children undergoing strabismus surgery, observed the superiority of combined dexamethasone and super-hydration over each therapy alone in terms of reducing the rate of incidence of PONV [37].
Although the mechanism underlying the reduction in PONV achieved by supplemental fluid therapy remains unclear, Ismail et al. [55], in their study concerning the prophylaxis of PONV, hypothesized that during elective surgery overnight fasting in addition to intraoperative fluid loss results in hypovolemia and a subsequent reduction in blood flow to the gut. In their opinion, the correction of gut ischemia suppresses the excessive serotonin release, which can possibly become a trigger of PONV. Therefore, the improvement of mesenteric perfusion by the prevention of gut ischemia and a decrease in serotonin release may possibly add to the reduction in the rate of presence of PONV [55].
In the current study, there were no statistically significant differences in perioperative fluid challenge between studied groups and no correlation between fluid challenge and the abovementioned risk factors was found. First, all patients received a fixed volume of crystalloids (10 mL/kg of body weight) to balance the overnight fluid loss, which was estimated to be approximately 40 mL/hour. Intraoperatively, when the depth of anesthesia using spectral entropy EEG (SE) was fixed at [40,41,42,43,44,45] in all patients and the IRNA was kept under SPI guidance levels (in accordance with AoA regimen), the use of anesthetic agents had a presumably similar impact on the intraoperative fluid requirement in individual patients, despite the group allocation. We hypothesize that the intraoperative monitoring of the depth of anesthesia using SE and analgesia using SPI could have created comparable conditions for all patients to direct fluid challenge according to their needs based on the intraoperative hemodynamic changes in response to the anesthetic regimen required to perform PPV.
The OCR is defined as an HR decrease of 20% from the baseline value or if dysrhythmias or sinoatrial arrest occurs during ocular manipulation [29] requiring atropine administration if the HR fails to increase to a baseline value after the release of surgical stimulation on the demand of the anesthesiologist. In the current study, the total rate of incidence of OCR was 12% (21 subjects out of 175), regardless of group allocation. Contrary to the observations of Ruta et al. [56] and Sajedi et al. [57], who observed a reduced rate of incidence of OCR when topical anesthesia was added to GA in patients undergoing PPV, in our study AoA guidance of GA completely blunted the effect of pre-emptive analgesia techniques. Moreover, no correlation between the rate of incidence of OCR and the abovementioned risk factors of its incidence was found. We presume that the employment of an anesthetic modality based on AoA guidance was responsible for the elimination of any cofounding factors of its incidence, similar to the case of PONV.
There are some limitations to the current analysis. First, nausea is a subjective phenomenon, which may be underreported by patients, especially in the population of diabetic patients, who may either misinterpret nausea as general illness after GA or may be so habituated to everyday nausea that they do not report it postoperatively. Second, despite the group allocation, patients were premedicated using midazolam as a part of the anesthetic regimen, which was proven to decrease the rate of PONV after PPV [58]. Its administration could have proportionally affected the final rate of incidence of PONV. Third, as shown in the current literature, there is no consistent algorithm for the titration of IRNA available, which could be due to the on-line observation of fluctuations in the SPI value [59]; therefore, we adopted a methodology of IRNA titration from our previous studies [60,61,62,63,64].
4. Materials and Methods
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the Bioethical Committee of the Medical University of Silesia (protocol code KNW/0022/KB1/101/15 and date of approval 29 September 2015). The project was registered in the Clinical Trial Registry (SilesianMUKOAiIT2, NCT02973581) and received the same approval as previous studies [11,12,60,61]. Informed consent was obtained from all patients recruited. This section builds upon our previous work [11,12,60,61].
4.1. Subjects
A total of 200 patients with indications for vitrectomy were invited to take part in the study. Patient data were stored in accordance with applicable laws in the Department of Anesthesiology and Intensive Therapy of the 5th Regional Hospital in Sosnowiec, Poland. Randomization was conducted via opening sealed envelopes after acquiring written informed consent. Before starting the analysis, the patients’ data were deleted so that individual patients could not be identified. The group size was estimated on the basis of the total number of vitrectomy procedures performed at the 5th Regional Hospital in Sosnowiec, Poland, which is 333 per year, and the confidence level of 95% and margin of error of 5%. Finally, 175 patients who underwent vitrectomy were enrolled in this study. They were divided into five groups according to the anesthesia used during the procedure. According to our previous articles, the groups were characterized as (1) the GQ group, including patients who received general anesthesia alone; (2) the T group, including patients who received preventive topical analgesia by the triple instillation of 2% proparacaine (alcaine, propacaine hydrochloride ophthalmic solution USP 0.5%, 15 mL, Sandoz a Novartis Company, Warszawa, Poland) 15 min before the induction of GA; (3) the PBB group, including patients who received PBB using a mixture of 3.5 mL each of 2% lignocaine (Lignocainum hydrochloricum WZF 2% solution, 20 mg/mL, 2 mL, Polfa Warszawa S.A, Warszawa, Poland) and 0.5% bupivacaine (Bupivacainum hydrochloricum WZF 0.5%, 5 mg/mL, 10 mL, Polfa Warszawa S.A) with Hamilton’s technique 1 min before the induction of GA [40]; (4) the M group, including patients who received PA using a single dose of 1 g of metamizole (Pyralgin 0.5 g/mL, 5 mL solution; Polpharma SA, Starogard Gdański, Poland) in 100 mL of saline solution intravenously 30 min before arrival at the operating room; and (5) the P group, including patients who received PA using a single dose of 1 g of acetaminophen (Paracetamol Kabi 10 mg/mL, solution 100 mL; Fresenius Kabi, Kutno, Poland) in 100 mL of saline solution intravenously 30 min before arrival at the operating room. The following vital parameters were monitored both during induction of anesthesia and throughout the surgical procedure: (1) non-invasive arterial pressure (NIBP), (2) HR, (3) standard electrocardiography, (4) pulse oximetry (SaO2), (5) fraction of inspired oxygen in the gas mixture, (6) fraction of inspired sevoflurane (FiAA), (7) fraction of expired sevoflurane, (8) EtCO2, and (9) minimal alveolar concentration of sevoflurane. [11,12,60,61].
4.2. Assessment of the Surgical Pleth Index
EEG entropy (state and response) was used to monitor the depth of anesthesia, while the SPI index was used to assess intraoperative analgesia. In addition, the neuromuscular blockade (Carescape B650, GE, Helsinki, Finland) was analyzed. The average SPI value and the calibration of the SPI sensor was possible thanks to the monitoring of the SPI value, which started 5 min after putting on the laryngeal mask and continued until the orbital sterilization began. At the intraoperative stage, the SPI value was read at 1 min intervals. In a situation where the SPI value increased by more than 15 compared to the value in the preoperative stage (∆SPI > 15), the patient was administered 1 µg/kg of FNT intravenously every 5 min, until the SPI value dropped to the mean value from the preoperative stage. We took a ∆SPI of >15 as the threshold at which emergency analgesia should be applied. The adoption of a difference value ∆SPI > 15 as an indication for emergency analgesia allowed us to minimize the risk of administering too much FNT, which may result from fluctuations in the SPI value and possible incorrect SPI calculations [11,12,60,61].
4.3. Assessment of the Occurrence of OCR and PONV
OCR incidence was monitored during vitrectomy, while PONV incidence was monitored both during surgery and for the first 24 h after surgery. “In the event of bradycardia, 0.5 mg of atropine (Atropinum sulfuricum WZF 1 mg/mL, solution 1 mL, Polfa Warszawa SA) was used, and in the case of hypotension, 5 mL of crystalloid per kg of body weight and a single dose of 5 mg of ephedrine (Ephedrinum hydrochloricum WZF 25 mg/mL, 1 mL of solution, Polfa Warszawa SA) [11,65]”. The indicators of SPI, HR, systolic arterial pressure (SAP), mean arterial pressure (MAP), diastolic blood pressure (DAP) and SaO2 were used to monitor the health of patients in the postoperative period, in accordance with the recommendations of Abouammoh et al. [66]. A numeric pain rating scale (NRS) was used for each patient’s pain rating. When the NRS score was below 3, standard non-steroidal anti-inflammatory drugs were administered in accordance with the Polish Society of Anaesthesiologists [67]. As mentioned in the previous work, “both NRS and SPI values were noted for severe (NRS 7–10), moderate (NRS 4–6), or mild pain (NRS 0–3) perception intervals [11]”. The risk of PONV was also assessed using the Apfel scale, which considers the following risk factors: female gender, history of motion sickness or PONV, no smoking, and postoperative opioid use. The Apfel score was determined before the anesthetic procedure. Depending on the absence of 1–4 of these risk factors, the incidence of PONV is 10%, 21%, 39%, 61% and 79%, respectively [11,45,59].
4.4. Statistical Analysis
Statistical analysis was performed using the STATISTICA 13PL software (StatSoft Sp. z o.o., Cracow, Poland) with a statistical significance threshold of p < 0.05. We performed one-way analysis of variance (ANOVA) and if the test showed statistically significant differences between variables, Tukey’s post hoc test was used. On the other hand, when the assumptions of the Shapiro–Wilk test were not met we used the non-parametric Kruskal–Wallis test followed by Dunn’s post hoc test. The Chi-square (X2) Test was used to analyze the independence of data expressed on a nominal scale. Moreover, to assess the relationship between the occurrence of OCR, PONV and analyzed risk factors, the crude OR (odds ratio), and 95%CI (confidence interval) with Fisher’s exact test were used.
5. Conclusions
The analysis in the current study revealed that DM, regardless of insulin dependence, constituted the only risk factor of the incidence of PONV. Female gender, smoking status, motion sickness, overweight and obesity, declaration of PIPP (NRS > 3), dose of IRNA and arterial hypertension were not found to correlate with the presence of intraoperative OCR and/or PONV. We assume that the utility of AoA monitoring created comparable conditions in the anesthetic regimen for each patient in the study, which blunted the influence of already-identified risk factors for the incidence of PONV in the current literature.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/ph15020237/s1. Table S1: Characteristics of the patients who participated in the study.
Author Contributions
Conceptualization, A.P. and M.J.S.; methodology, M.K., A.L.-B. and D.D.; software, S.K.; validation, M.J.S.; formal analysis, S.K.; investigation, A.L.-B. and D.D.; resources, E.N. and J.Ż.; data curation, E.N., R.R. and J.Ż.; writing—original draft preparation, A.P., A.M., M.J.S. and I.S.; writing—review and editing, L.K. and M.J.S.; supervision, M.J.S. and M.J.K.; project administration, B.O.G. and P.J. All authors have read and agreed to the published version of the manuscript.
Funding
A Medical University of Silesia scientific grant (No. KNW-1-183/N/9/K) covered the cost of analytic equipment, data collection and analysis and manuscript preparation.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the Bioethical Committee of the Medical University of Silesia (protocol code KNW/0022/KB1/101/15 and date of approval 29 September 2015). The project was registered in the Clinical Trial Registry (SilesianMUKOAiIT2, NCT02973581) and received the same approval as that from previous studies [11,12,60,61].
Informed Consent Statement
Informed consent was obtained from all patients recruited.
Data Availability Statement
Data is contained within the article.
Acknowledgments
The authors sincerely thank Teresa Paczyńska (the anesthetic nurse who assisted every GA for PPV) of Regional Hospital no. 5 in Sosnowiec for her enthusiastic co-operation with the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Reibaldi, M.; Fallico, M.; Longo, A.; Avitabile, T.; Astuto, M.; Murabito, P.; Minardi, C.; Bonfiglio, V.; Boscia, F.; Furino, C.; et al. Efficacy of Three Different Prophylactic Treatments for Postoperative Nausea and Vomiting after Vitrectomy: A Randomized Clinical Trial. J. Clin. Med. 2019, 8, 391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heinke, W.; Frank, T.; Meier, P.; Wiegel, M.; Korth, D. Postoperative vomiting after pars plana vitrectomy. Anesthesiol. Reanim. 1996, 21, 47–50. [Google Scholar]
- Sallam, A.A.B.; Donachie, P.H.J.; Williamson, T.; Sparrow, J.M.; Johnston, R.L. The Royal College of Ophthalmologists’ National Ophthalmology Database Study of vitreoretinal surgery: Report 5, Anesthetic Techniques. Br. J. Ophthalmol. 2015, 100, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Cok, O.Y.; Eker, H.E.; Pelit, A.; Canturk, S.; Akin, S.; Aribogan, A.; Arslan, G. The effect of paracetamol on postoperative nausea and vomiting during the first 24 h after strabismus surgery: A prospective, randomised, double-blind study. Eur. J. Anesthesiol. 2011, 28, 836–841. [Google Scholar] [CrossRef]
- Bharti, N.; Chari, P.; Kumar, P. Effect of sevoflurane versus propofol-based anesthesia on the hemodynamic response and recovery characteristics in patients undergoing microlaryngeal surgery. Saudi J. Anesth. 2012, 6, 380–384. [Google Scholar] [CrossRef]
- Bergmann, I.; Göhner, A.; Crozier, T.A.; Hesjedal, B.; Wiese, C.H.; Popov, A.F.; Bauer, M.; Hinz, J.M. Surgical pleth index-guided remifentanil administration reduces remifentanil and propofol consumption and shortens recovery times in outpatient anesthesia. Br. J. Anesth. 2013, 110, 622–628. [Google Scholar] [CrossRef] [Green Version]
- Gruenewald, M.; Harju, J.; Preckel, B.; Molnár, Z.; Yli-Hankala, A.; Rosskopf, F.; Koers, L.; Orban, A.; Bein, B.; AoA Study Group. Comparison of adequacy of anesthesia monitoring with standard clinical practice monitoring during routine general anesthesia: An international, multicentre, single-blinded randomised controlled trial. Eur. J. Anesthesiol. 2021, 38, 73–81. [Google Scholar] [CrossRef]
- Wennervirta, J.; Hynynen, M.; Koivusalo, A.M.; Uutela, K.; Huiku, M.; Vakkuri, A. Surgical stress index as a measure of nocicep-tion/antinociception balance during general anesthesia. Acta Anesthesiol. Scand. 2008, 52, 1038–1045. [Google Scholar] [CrossRef]
- Ahonen, J.; Jokela, R.; Uutela, K.; Huiku, M. Surgical stress index reflects surgical stress in gynaecological laparoscopic day-case surgery. Br. J. Anesth. 2007, 98, 456–461. [Google Scholar] [CrossRef] [Green Version]
- Gruenewald, M.; Meybohm, P.; Ilies, C.; Höcker, J.; Hanss, R.; Scholz, J.; Bein, B. Influence of different remifentanil concentrations on the performance of the surgical stress index to detect a standardized painful stimulus during sevoflurane anesthesia. Br. J. Anesth. 2009, 103, 586–593. [Google Scholar] [CrossRef] [Green Version]
- Stasiowski, M.; Pluta, A.; Lyssek-Boroń, A.; Kawka, M.; Krawczyk, L.; Niewiadomska, E.; Dobrowolski, D.; Rejdak, R.; Król, S.; Żak, J.; et al. Preventive Analgesia, Hemodynamic Stability, and Pain in Vitreoretinal Surgery. Medicina 2021, 57, 262. [Google Scholar] [CrossRef]
- Pluta, A.; Stasiowski, M.J.; Lyssek-Boroń, A.; Król, S.; Krawczyk, L.; Niewiadomska, E.; Żak, J.; Kawka, M.; Dobrowolski, D.; Grabarek, B.O.; et al. Adverse Events during Vitrectomy under Adequacy of Anesthesia—An Additional Report. J. Clin. Med. 2021, 10, 4172. [Google Scholar] [CrossRef] [PubMed]
- Pluta, M.; Krzych, Ł.J. Użyteczność punktacji Apfel w przewidywaniu pooperacyjnych nudności i wymiotów—Doświadczenia jednego ośrodka. Ann. Acad. Med. Siles 2018, 72, 224–229. [Google Scholar] [CrossRef]
- Ali-Melkkilä, T.; Kanto, J.; Katevuo, R. Tropisetron and metoclopramide in the prevention of postoperative nausea and vomit-ing. A comparative, placebo controlled study in patients undergoing ophthalmic surgery. Anesthesia 1996, 51, 232–235. [Google Scholar]
- Bruderer, U.; Fisler, A.; Steurer, M.P.; Steurer, M.; Dullenkopf, A. Post-discharge nausea and vomiting after total intravenous anesthesia and standardised PONV prophylaxis for ambulatory surgery. Acta Anesthesiol. Scand. 2017, 61, 758–766. [Google Scholar] [CrossRef]
- Apfel, C.C.; Korttila, K.; Abdalla, M.; Kerger, H.; Turan, A.; Vedder, I.; Zernak, C.; Danner, K.; Jokela, R.; Pocock, S.J.; et al. A factorial trial of six interventions for the prevention of postop-erative nausea and vomiting. N. Engl. J. Med. 2004, 350, 2441–2451. [Google Scholar] [CrossRef] [Green Version]
- Weibel, S.; Rücker, G.; Eberhart, L.H.; Pace, N.L.; Hartl, H.M.; Jordan, O.L.; Mayer, D.; Riemer, M.; Schaefer, M.S.; Raj, D.; et al. Drugs for preventing postoperative nausea and vomiting in adults after general anesthesia: A network meta-analysis. Cochrane Database Syst. Rev. 2020, 10, CD012859. [Google Scholar] [CrossRef]
- Nitahara, K.; Sugi, Y.; Shono, S.; Hamada, T.; Higa, K. Risk factors for nausea and vomiting following vitrectomy in adults. Eur. J. Anesthesiol. 2007, 24, 166–170. [Google Scholar]
- Iwamoto, K.; Schwartz, H. Antiemetic Effect of Droperidol After Ophthalmic Surgery. Arch. Ophthalmol. 1978, 96, 1378–1379. [Google Scholar] [CrossRef]
- Quinn, A.C.; Brown, J.H.; Wallace, P.G.; Asbury, A.J. Studies in postoperative sequelae. Nausea and vomiting-still a problem. Anesthesia 1994, 49, 62–65. [Google Scholar] [CrossRef]
- Koivuranta, M.; Läärä, E.; Snåre, L.; Alahuhta, S. A survey of postoperative nausea and vomiting. Anesthesia 1997, 52, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Apfel, C.C.; Greim, C.A.; Haubitz, I.; Goepfert, C.; Usadel, J.; Sefrin, P.; Roewer, N. A risk score to predict the probability of postoperative vomiting in adults. Acta Anesthesiol. Scand. 1998, 42, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Apfel, C.C.; Kranke, P.; Katz, M.H.; Goepfert, C.; Papenfuss, T.; Rauch, S.; Heineck, R.; Greim, C.-A.; Roewer, N. Volatile anesthetics may be the main cause of early but not delayed postoperative vomiting: A randomized controlled trial of factorial design. Br. J. Anesth. 2002, 88, 659–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borgeat, A.; Stirnemann, H.R. Antiemetische Wirkung von Propofol [Antiemetic effect of propofol]. Anesthesist 1998, 47, 918–924. [Google Scholar] [CrossRef]
- Ewalenko, P.; Janny, S.; Dejonckheere, M.; Andry, G.; Wyns, C. Antiemetic effect of subhypnotic doses of propofol after thyroidectomy. Br. J. Anesth. 1996, 77, 463–467. [Google Scholar] [CrossRef] [PubMed]
- Niu, K.; Liu, H.; Chen, R.W.; Fang, Q.W.; Wen, H.; Guo, S.M.; Williams, J.P.; An, J.X. Use of propofol for prevention of post-delivery nausea during cesarean section: A double-blind, randomized, placebo-controlled trial. J. Anesth. 2018, 32, 748–755. [Google Scholar] [CrossRef] [Green Version]
- Khalid, A.; Siddiqui, S.Z.; Aftab, S.; Sabbar, S.; Haider, S. Recovery profile—A comparison of isoflurane and propofol anesthesia for laparoscopic cholecystectomy. J. Coll. Physicians Surg. Pak. 2008, 18, 329–333. [Google Scholar]
- Xie, D.; Zhao, J.; Guo, R.; Jiao, L.; Zhang, Y.; Lau, W.B.; Lopez, B.; Christopher, T.; Gao, E.; Cao, J.; et al. Sevoflurane Pre-conditioning Ameliorates Diabetic Myocardial Ischemia/Reperfusion Injury Via Differential Regulation of p38 and ERK. Sci. Rep. 2020, 10, 23. [Google Scholar] [CrossRef]
- Watcha, M.F.; White, P.F. Postoperative nausea and vomiting: Its etiology, treatment, and prevention. Anesthesiology 1992, 77, 162–184. [Google Scholar] [CrossRef]
- Kranke, P.; Apfel, C.C.; Papenfuss, T.; Rauch, S.; Löbmann, U.; Rübsam, B.; Greim, C.-A.; Roewer, N. An increased body mass index is no risk factor for postoperative nausea and vomiting. A systematic review and results of original data. Acta Anesth. Scand. 2001, 45, 160–166. [Google Scholar] [CrossRef]
- Kim, J.H.; Hong, M.; Kim, Y.J.; Lee, H.S.; Kwon, Y.S.; Lee, J.J. Effect of Body Mass Index on Postoperative Nausea and Vomiting: Propensity Analysis. J. Clin. Med. 2020, 9, 1612. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.M.; Duncan, P.G.; DeBoer, D.P.; Tweed, W.A. The postoperative interview: Assessing risk factors for nausea and vomiting. Anesth. Analg. 1994, 78, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Stadler, M.; Bardiau, F.; Seidel, L.; Albert, A.; Boogaerts, J.G. Difference in Risk Factors for Postoperative Nausea and Vomiting. Anesthesiology 2003, 98, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Allison, C.E.; De Lange, J.J.; Koole, F.D.; Zuurmond, W.W.; Ros, H.H.; van Schagen, N.T. A comparison of the incidence of the oculocardiac and oculorespiratory reflexes during sevoflurane or halothane anesthesia for strabismus surgery in children. Anesth. Analg. 2000, 90, 306–310. [Google Scholar] [PubMed]
- Carlisle, J.B.; Stevenson, C.A. Drugs for preventing postoperative nausea and vomiting. Cochrane Database Syst. Rev. 2006, 3, CD004125. [Google Scholar]
- Mandelcorn, M.; Taback, N.; Mandelcorn, E.; Ananthanarayan, C. Risk factors for pain and nausea following retinal and vitreous surgery under conscious sedation. Can. J. Ophthalmol. 1999, 34, 281–285. [Google Scholar]
- Mallick-Searle, T.; Fillman, M. The pathophysiology, incidence, impact, and treatment of opioid-induced nausea and vomiting. J. Am. Assoc. Nurse Pract. 2017, 29, 704–710. [Google Scholar] [CrossRef]
- Chang, D.J.; Desjardins, P.J.; Bird, S.R.; Black, P.; Chen, E.; Petruschke, R.A.; Geba, G.P. Comparison of rofecoxib and a multidose oxycodone/acetaminophen regimen for the treatment of acute pain following oral surgery: A randomized con-trolled trial. Curr. Med. Res. Opin. 2004, 20, 939–949. [Google Scholar] [CrossRef]
- Daniels, S.; Casson, E.; Stegmann, J.-U.; Oh, C.; Okamoto, A.; Rauschkolb, C.; Upmalis, D. A randomized, double-blind, placebo-controlled phase 3 study of the relative efficacy and tolerability of tapentadol IR and oxycodone IR for acute pain. Curr. Med. Res. Opin. 2009, 25, 1551–1561. [Google Scholar] [CrossRef]
- Gan, T.J.; Diemunsch, P.; Habib, A.S.; Kovac, A.; Kranke, P.; Meyer, T.A.; Watcha, M.; Chung, F.; Angus, S.; Apfel, C.C.; et al. Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesth. Analg. 2014, 118, 85–113. [Google Scholar] [CrossRef] [Green Version]
- Apfel, C.C.; Turan, A.; Souza, K.; Pergolizzi, J.; Hornuss, C. Intravenous acetaminophen reduces postoperative nausea and vomiting: A systematic review and meta-analysis. Proc. Natl. Acad. Sci. USA 2013, 154, 677–689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefánsson, E. Diabetic macular edema. Saudi J. Ophthalmol. 2009, 23, 143–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ribeiro, J.A.S.; Ribeiro, D.S.; Scott, I.U.; Abrão, J.; Jorge, R. Pain during pars plana vitrectomy following sub-Tenon versus peribulbar anesthesia: A randomized trial. PLoS ONE 2020, 15, e0236624. [Google Scholar] [CrossRef] [PubMed]
- Ostri, C.; la Cour, M.; Lund-Andersen, H. Diabetic vitrectomy in a large type 1 diabetes patient population: Long-term incidence and risk factors. Acta Ophthalmol. 2013, 92, 439–443. [Google Scholar] [CrossRef]
- Wilkes, S.R. Current therapy of diabetic retinopathy: Laser and vitreoretinal surgery. J. Natl. Med. Assoc. 1993, 85, 841–847. [Google Scholar]
- Cherian, D.; Parkman, H.P. Nausea and vomiting in diabetic and idiopathic gastroparesis. Neurogastroenterol. Motil. 2012, 24, 217-e103. [Google Scholar] [CrossRef]
- Parkman, H.P.; Hallinan, E.K.; Hasler, W.L.; Farrugia, G.; Koch, K.L.; Calles, J.; Snape, W.J.; Abell, T.L.; Sarosiek, I.; McCallum, R.W.; et al. Nausea and vomiting in gastroparesis: Similarities and differences in idiopathic and diabetic gastroparesis. Neurogastroenterol. Motil. 2016, 28, 1902–1914. [Google Scholar] [CrossRef]
- Fleischer, J. Diabetic Autonomic Imbalance and Glycemic Variability. J. Diabetes Sci. Technol. 2012, 6, 1207–1215. [Google Scholar] [CrossRef] [Green Version]
- McCaul, C.; Moran, C.; O’Cronin, D.; Naughton, F.; Geary, M.; Carton, E.; Gardiner, J. Intravenous fluid loading with or without supplementary dextrose does not prevent nausea, vomiting and pain after laparoscopy. Can. J. Anesth. 2003, 50, 440–444. [Google Scholar] [CrossRef]
- Haentjens, L.L.; Ghoundiwal, D.; Touhiri, K.; Renard, M.; Engelman, E.; Anaf, V.; Simon, P.; Barvais, L.; Ickx, B.E. Does infusion of colloid influence the occur-rence of postoperative nausea and vomiting after elective surgery in women? Anesth. Analg. 2009, 108, 1788–1793. [Google Scholar] [CrossRef]
- Dagher, C.F.; Abboud, B.; Richa, F.; Abouzeid, H.; El-Khoury, C.; Doumit, C.; Yaghi, C.; Yazbeck, P. Effect of intravenous crystalloid infusion on postoperative nausea and vomiting after thyroidectomy: A prospective, randomized, controlled study. Eur. J. Anesthesiol. 2009, 26, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Kovac, A.L. Postoperative Nausea and Vomiting in Pediatric Patients. Pediatr. Drugs 2021, 23, 11–37. [Google Scholar] [CrossRef] [PubMed]
- Apfel, C.C.; Läärä, E.; Koivuranta, M.; Greim, C.A.; Roewer, N. A simplified risk score for predicting postoperative nausea and vomiting: Conclusions from cross-validations between two centers. Anesthesiology 1999, 91, 693–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apfel, C.C.; Meyer, A.; Orhan-Sungur, M.; Jalota, L.; Whelan, R.P.; Jukar-Rao, S. Supplemental intravenous crystalloids for the prevention of postoperative nausea and vomiting: Quantitative review. Br. J. Anesth. 2012, 108, 893–902. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.Z.; Taguchi, A.; Holtmann, B.; Kurz, A. Effect of supplemental pre-operative fluid on postoperative nausea and vomiting. Anesthesia 2003, 58, 780–784. [Google Scholar] [CrossRef] [PubMed]
- Ruta, U.; Möllhoff, T.; Markodimitrakis, H.; Brodner, G. Attenuation of the oculocardiac reflex after topically applied lignocaine during surgery for strabismus in children. Eur. J. Anesthesiol. 1996, 13, 11–15. [Google Scholar] [CrossRef]
- Sajedi, P.; Nejad, M.S.; Montazeri, K.; Baloochestani, E. Comparing the preventive effect of 2 percent topical lidocaine and intra-venous atropine on oculocardiac reflex in ophthalmological surgeries under general anesthesia. Int. J. Prev. Med. 2013, 4, 1258–1265. [Google Scholar]
- Grant, M.C.; Kim, J.; Page, A.J.; Hobson, D.; Wick, E.; Wu, C.L. The Effect of Intravenous Midazolam on Postoperative Nausea and Vomiting: A Meta-Analysis. Anesth. Analg. 2016, 122, 656–663. [Google Scholar] [CrossRef]
- Ledowski, T.; Burke, J.; Hruby, J. Surgical pleth index: Prediction of postoperative pain and influence of arousal. Br. J. Anesth. 2016, 117, 371–374. [Google Scholar] [CrossRef] [Green Version]
- Stasiowski, M.; Missir, A.; Pluta, A.; Szumera, I.; Stasiak, M.; Szopa, W.; Błaszczyk, B.; Możdżyński, B.; Majchrzak, K.; Tymowski, M.; et al. Influence of infiltration anesthesia on perioperative outcomes following lumbar discectomy under surgical pleth index-guided general anesthesia: A preliminary report from a randomised controlled prospective trial. Adv. Med. Sci. 2020, 65, 149–155. [Google Scholar] [CrossRef]
- Stasiowski, M.; Starzewska, M.; Niewiadomska, E.; Król, S.; Marczak, K.; Żak, J.; Pluta, A.; Eszyk, J.; Grabarek, B.; Szumera, I.; et al. Adequacy of Anesthesia Guidance for Colonoscopy Procedures. Pharmaceuticals 2021, 14, 464. [Google Scholar] [CrossRef] [PubMed]
- Stasiowski, M.J.; Szumera, I.; Wardas, P.; Król, S.; Żak, J.; Missir, A.; Pluta, A.; Niewiadomska, E.; Krawczyk, L.; Jałowiecki, P.; et al. Adequacy of Anesthesia and Pupillometry for Endoscopic Sinus Surgery. J. Clin. Med. 2021, 10, 4683. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, R.C. Techniques of orbital regional anesthesia. Br. J. Anesth. 1995, 75, 88–92. [Google Scholar] [CrossRef]
- Gruenewald, M.; Ilies, C. Monitoring the nociception–anti-nociception balance. Best Pract. Res. Clin. Anesthesiol. 2013, 27, 235–247. [Google Scholar] [CrossRef] [PubMed]
- Kusza, K.; Kübler, A.; Maciejewski, D.; Mikstacki, A.; Owczuk, R.; Wujtewicz, M.; Piechota, M. Guidelines of the Polish Soci-ety of Anesthesiology and Intensive Therapy determining principles, conditions and organisational aspects of anesthesiol-ogy and intensive therapy services. Anesthesiol. Intensive Ther. 2013, 44, 201–212. [Google Scholar]
- Abouammoh, M.A.; Abdelhalim, A.A.; Mohamed, E.A.; Elzoughari, I.; Mustafa, M.; Al-Zahrani, T.A. Subtenon block com-bined with general anesthesia for vitreoretinal surgery improves postoperative analgesia in adult: A randomized controlled trial. J. Clin. Anesth. 2016, 30, 78–86. [Google Scholar] [CrossRef]
- Misiołek, H.; Cettler, M.; Woroń, J.; Wordliczek, J.; Dobrogowski, J.; Mayzner-Zawadzka, E. The 2014 guidelines for post-operative pain management. Anesthesiol. Intensive Ther. 2014, 46, 221–244. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).