

Validation of Low-Cost IMUs for Telerehabilitation Exercises

 ,
, 
Abstract
1. Introduction
- Development of an effective rehabilitation protocol, based on scientific literature and kinesiological expertise, which can be performed remotely through wearable sensors and provide biofeedback;
- Selection of a set of parameters capable of describing different motor capacities;
- Assessment of the validity of prototypical sensors;
- Evaluation of the effectiveness of the IoT-based system in individuals with chronic conditions, identifying potential limitations;
- Assessment of the system’s usability in a home environment.
2. Materials and Methods
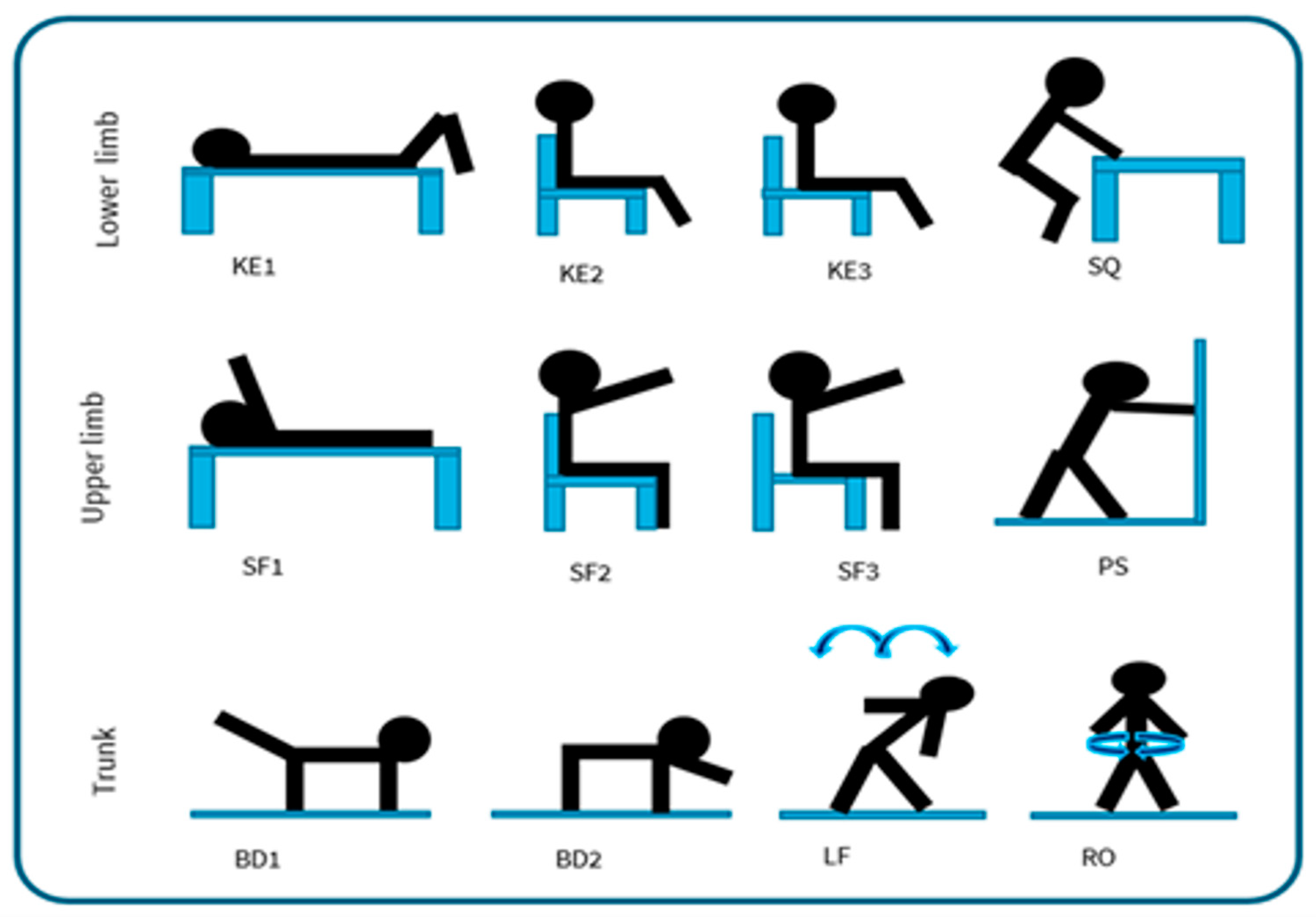
2.1. REHACT Motor Rehabilitation Protocol
- For the lower limbs: knee extension lying down (KE1), knee extension sitting with a back support (KE2), knee extension without back support (KE3), half squat supported on a table (SQ);
- For the upper limbs: shoulder flexion lying down (SF1), shoulder flexion sitting with a back support (SF2), shoulder flexion without back support (SF3), wall push-up (PS);
- For the trunk: bird dog exercise [24] using only the legs (BD1), bird dog using only the arms (BD2), lateral flexion of the column (LF), rotation of the column (RO).
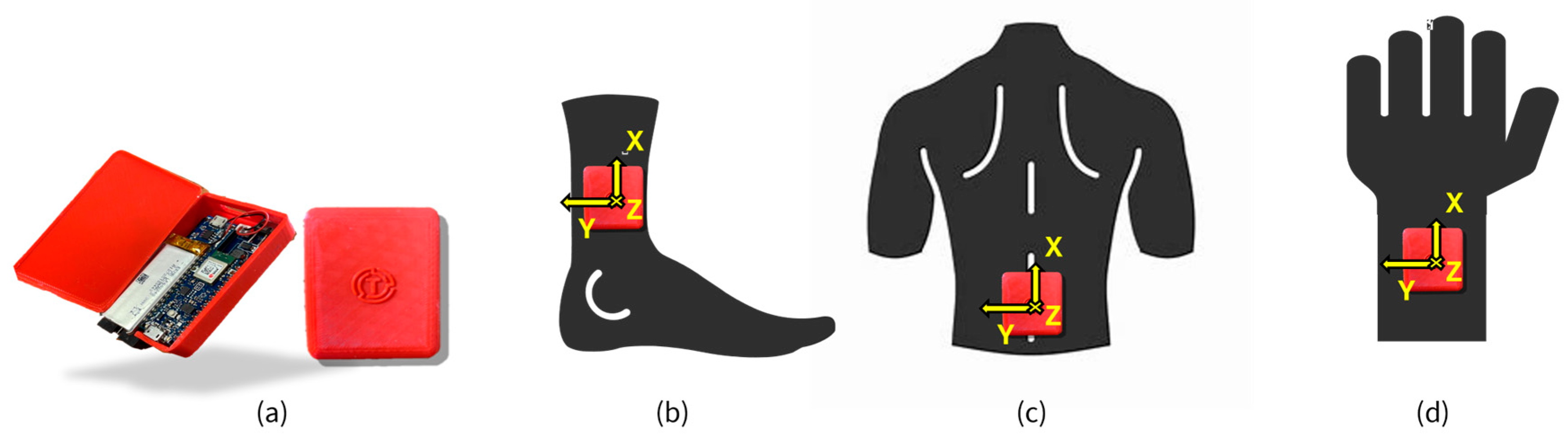
2.2. REHACT Sensors and Infrastructure
2.3. Movement Characterization
- REP—number of repetitions made by the participant for each set;
- TIME—duration, for each repetition;
- Acceleration Peak (, , )—the acceleration peaks on the different axes (X, Y, Z) were determined by extracting the maximum values within each identified repetition of the filtered data sets;
- Angular velocity Peak (, , )—angular velocity peaks about the different axes (X, Y, Z) were calculated as maximum value within each identified repetition of the filtered data sets;
- Movement Intensity (MI)—the mean value of the Euclidean norm of the linear triaxial filtered acceleration () of the wearable sensor, as measured in g, was calculated over the exercise sets in healthy participant [11,12]. This metric was used in previous studies to quantify exercise intensity in clinical applications [12,26,27].
- Movement intensity variation (MIV)—difference in the MI values calculated for the two sets.
- Log dimensionless jerk (LDLJ)—measures gesture smoothness based on filtered acceleration data in each repetition [29,30], where smaller negative values correspond to smoother movements [12];where , , are the derivatives of the sensor’s triaxial acceleration with respect to time; is equal to the magnitude of the peak total acceleration minus the mean total acceleration of the movement, and t1 and t2 represent the time at beginning and end of the repetition;
- Dynamic Time Warping (DTW)—assesses movement stability [11,27]. DTW was used to compare filtered acceleration signals from successive repetitions of the same set, with the DTW distance for each consecutive pair serving as an indicator of stability. This analysis was performed using the default “dtw” function provided in MATLAB. A lower DTW distance value can be interpreted as a better ability to maintain control of the joint movement while performing the exercise [12];
- Peak range of Motion (PKROM)—This index was used to assess the maximum range of motion [28]. First, the orientation of each sensor was computed for every repetition using the Madgwick orientation algorithm [31], whose beta coefficients were defined for each set of sensors as those minimizing orientation differences between devices, based on magnetometer calibration data (β prototype = 0.6, β reference = 0.1). Then, the joint angle (in degrees) was calculated along the specific axis of movement for each exercise (ROM), and finally, the peak values were computed within each identified repetition (PKROM).
2.4. Validation Study
2.5. Statistical Analysis
3. Results
4. Discussion
- design a rehabilitation protocol, based on scientific evidence and kinesiological expertise, which could be performed remotely using wearable sensors;
- select a set of parameters for motor capacity assessment;
- validate prototype sensors against reference systems.
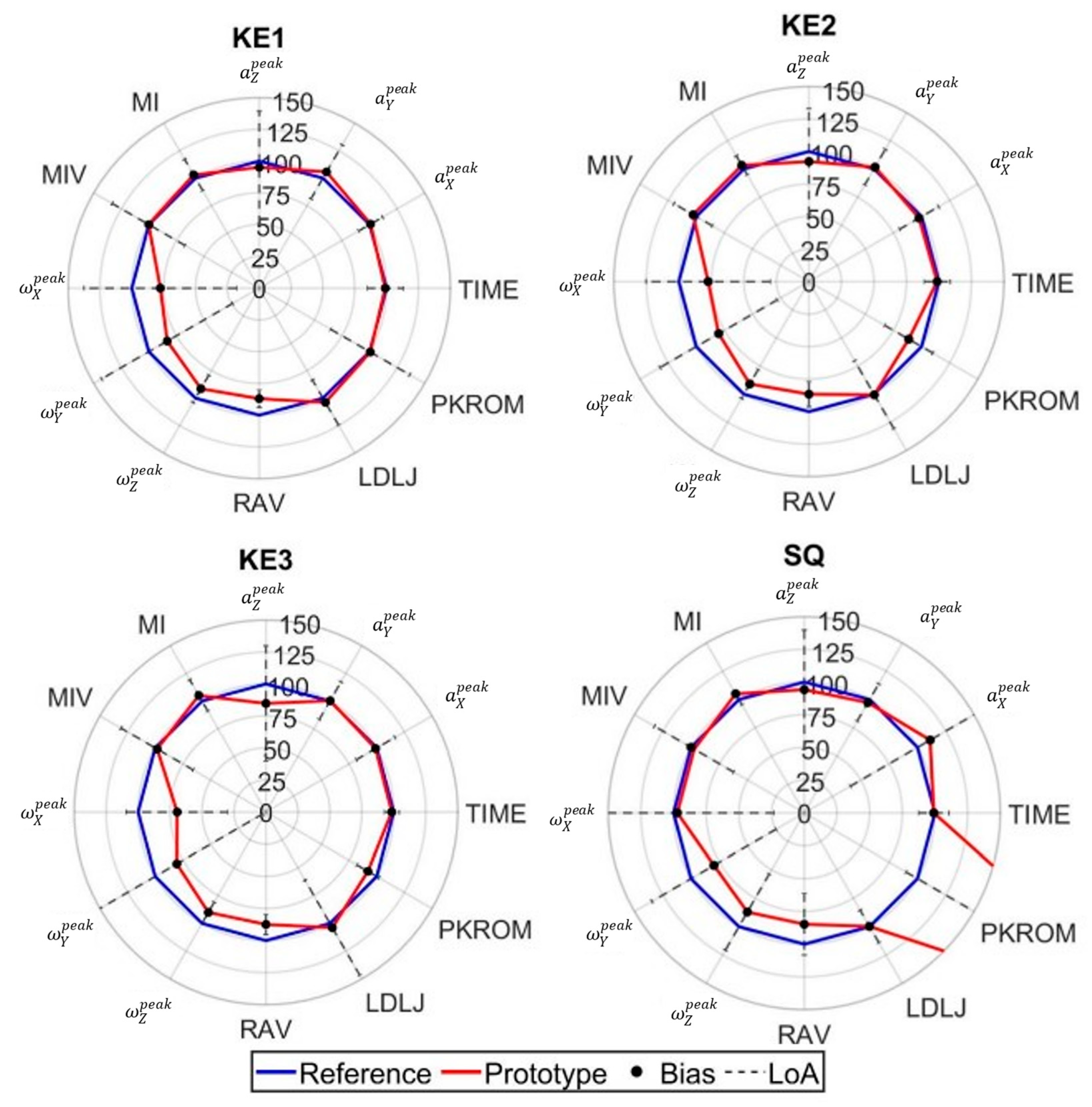
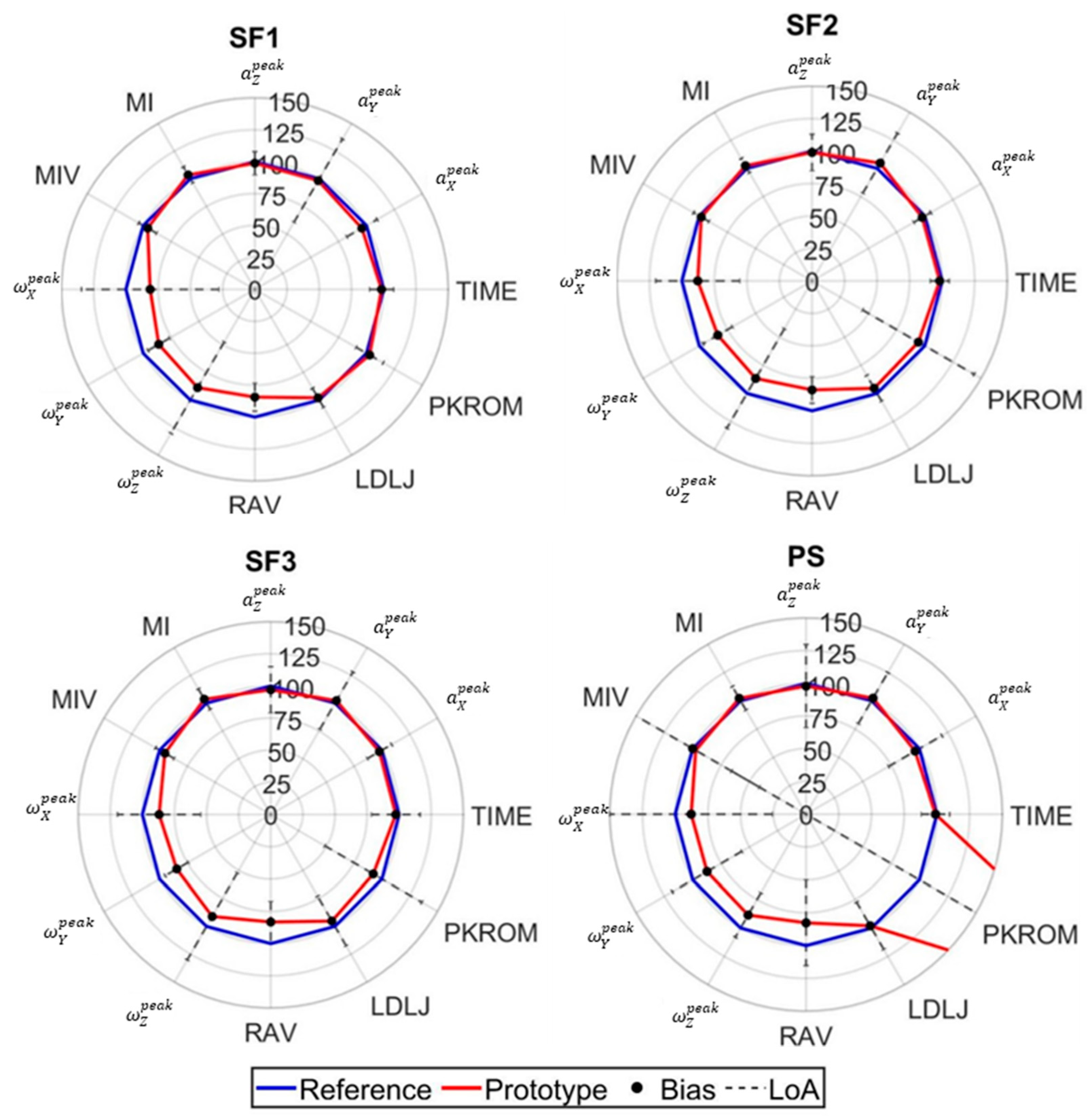
- Quantity parameters exhibited robust validity for conventional rehabilitation parameters (repetition count and execution time) (Figure 5, Figure 6 and Figure 7), demonstrating homoscedastic behavior across all evaluated exercises (τ < 0.1) (Table A1). The system validity is further substantiated by the use of the same algorithm for repetition identification in both reference and prototype sensors. This consistency is a basic prerequisite for reliable monitoring physical therapy exercises.
- Movement Intensity parameters showed varying degrees of consistency and of agreement (Figure 5, Figure 6 and Figure 7). Open chain exercises (KE1, KE2, KE3, SF1, SF2, SF3) had a better performance in terms of both BIAS and LoA with respect to closed chain ones (SQ, PS, BD1, BD2, LF, RO). While peak acceleration measurements (, , ) and derived parameters (MI, MIV) demonstrated good consistency and agreement, angular velocity measurements (, , )showed substantial variability and disagreement. For example, in the lower limb exercises (Table A2), biases range from −0.48 to −16.9, while the limits of agreement (LoA) vary between 4.7 and 26.0 across the different exercises. Similar patterns can be observed for both upper limb (Table A3) and trunk exercises (Table A4). Although these differences appear to be reduced in the RAV parameter, they highlight the need for hardware improvement.
- Quality parameters had different behaviors: LDLJ showed acceptable consistency; conversely, DTW had a heteroscedastic behavior, which led to its exclusion and calls for a refinement in the stability assessment; PKROM had high LoA in most of the exercises, presenting a limited applicability for rehabilitation environment. For example, in the SQ exercise, the prototype estimated a PKROM of 29 degrees, while in the PS exercise, it measured 65 degrees, which is significantly higher compared to the reference sensor values (Table 3). Acceptable levels of consistency and variability can be observed in the KE2, KE3, and SF1 exercises, together with reasonably narrow limits of agreement and the favorable cost-benefit ratio of the prototype, suggesting the use of PKROM as suitable for monitoring in practical applications. The error in orientation estimation certainly suffers from the abovementioned differences amongst angular velocities, not excluding other sources of error and calling for implementing ad hoc sensor fusion algorithms.
Limits and Future Development
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ECG | Electrocardiogram |
| SpO2 | Oxygen saturation levels |
| IMU | Inertial measurement unit |
| IoT | Internet of Things |
| TRL | Technology Readiness Level |
| KE1 | Knee extension lying down |
| KE2 | Knee extension sitting with back support |
| KE3 | Knee extension sitting without back support |
| SQ | Half squat in support |
| SF1 | Shoulder flexion lying down |
| SF2 | Shoulder flexion sitting with back support |
| SF3 | Shoulder flexion sitting without back support |
| PS | Wall push up |
| BD1 | Bird dog using legs |
| BD2 | Bird dog using arms |
| LF | Trunk lateral flexion |
| RO | Trunk Rotation |
| QT | “Quantity” movement parameter |
| REP | Number of repetitions |
| TIME | Time to perform repetition |
| I | “Intensity” movement parameter |
| Peak of acceleration x-axis | |
| Peak of acceleration y-axis | |
| Peak of acceleration z-axis | |
| Peak of angular velocity x-axis | |
| Peak of angular velocity y-axis | |
| Peak of angular velocity z-axis | |
| MI | Movement intensity |
| MIV | Movement intensity variability |
| RAV | Range of angular velocity |
| QL | “Quality” movement parameter |
| LDLJ | Log dimensionless jerk |
| DTW | Dynamic time warping |
| ROM | Range of motion |
| PKROM | Maximum value of range of motion |
| RPE | Rate of perception exertion |
| VAS | Visual analog scale |
| BIAS | Difference between the mean reference and the |
| LoA | Limit of agreement |
| BA | Bland and Altman analysis |
| CI | Confidence intervals |
| seBIAS | Standard error for the BIAS |
Appendix A
Bland and Altman Parameters

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exercises | Parameter | Bias | LoA | CI% Bias | CI% LoA | Kendal’s τ | Outliers | t-Value | se Bias |
|---|---|---|---|---|---|---|---|---|---|
| KE1 | REP | 0 | 0 | 0% | 0% | \ | 0 | 0 | 0 |
| TIME [s] | 0.02 | 0.32 | 1% | 3% | 0.01 | 6 | 1.96 | 0 | |
| KE2 | REP | 0 | 0 | 0% | 0% | \ | 0 | 0 | 0 |
| TIME [s] | 0.02 | 0.17 | 0% | 1% | 0.01 | 0 | 1.96 | 0 | |
| KE3 | REP | 0 | 0 | 0% | 0% | \ | 0 | 0 | 0 |
| TIME [s] | 0.02 | 0.10 | 0% | 1% | 0.01 | 0 | 1.96 | 0 | |
| SQ | REP | 0 | 0 | 0% | 0% | \ | 0 | 0 | 0 |
| TIME [s] | 0.02 | 0.25 | 10% | 2% | 0.06 | 4 | 1.96 | 0 | |
| SF1 | REP | 0 | 0 | 0% | 0% | \ | 0 | 0 | 0 |
| TIME [s] | −0.05 | 0.26 | 1% | 2% | 0.01 | 8 | 1.96 | 0 | |
| SF2 | REP | 0 | 0 | 0% | 0% | \ | 0 | 0 | 0 |
| TIME [s] | −0.04 | 0.17 | 0% | 1% | 0.05 | 5 | 1.96 | 0 | |
| SF3 | REP | 0 | 0 | 0% | 0% | \ | 0 | 0 | 0 |
| TIME [s] | −0.05 | 0.41 | 2% | 3% | 0.01 | 2 | 1.96 | 0.01 | |
| PS | REP | 0 | 0 | 0% | 0% | \ | 0 | 0 | 0 |
| TIME [s] | −0.02 | 0.27 | 1% | 2% | 0.01 | 8 | 1.96 | 0 | |
| BD1 | REP | 0 | 0 | 0% | 0% | \ | 0 | 0 | 0 |
| TIME [s] | −0.01 | 0.63 | 4% | 7% | 0.09 | 0 | 1.96 | 0.02 | |
| BD2 | REP | 0 | 0 | 0% | 0% | \ | 0 | 0 | 0 |
| TIME [s] | −0.01 | 0.35 | 2% | 4% | 0.07 | 5 | 1.97 | 0.01 | |
| LF | REP | 0 | 0 | 0% | 0% | \ | 0 | 0 | 0 |
| TIME [s] | −0.03 | 0.61 | 11% | 20% | 0.07 | 10 | 1.97 | 0.05 | |
| RO | REP | 0 | 0 | 0% | 0% | \ | 0 | 0 | 0 |
| TIME [s] | −0.03 | 1.40 | 11% | 2% | 0.07 | 10 | 1.97 | 0.05 |
| Exercises | Parameter | Bias | LoA | CI% Bias | CI% LoA | Kendal’s τ | Outliers | t-Value | se Bias |
|---|---|---|---|---|---|---|---|---|---|
| KE1 | [g] | 0.01 | 0.16 | 0% | 1% | 0.01 | 3 | 1.96 | 0 |
| [g] | 0.02 | 0.12 | 0% | 1% | 0.05 | 4 | 1.96 | 0 | |
| [g] | 0.01 | 0.11 | 0% | 1% | 0.01 | 7 | 1.96 | 0 | |
| [deg/s] | −5.4 | 14.7 | 0.8 | 13% | 0.06 | 7 | 1.96 | 0.4 | |
| [deg/s] | −5.9 | 21.0 | 1.19 | 20% | 0.03 | 19 | 1.96 | 0.6 | |
| [deg/s] | −16.9 | 24.7 | 1.32 | 22% | 0.04 | 0 | 1.96 | 0.6 | |
| MI [g] | 0 | 0.04 | 0% | 1% | 0.05 | 0 | 2.01 | 0 | |
| MIV [g] | 0 | 0.06 | 1% | 1% | 0.06 | 0 | 2.01 | 0 | |
| RAV [rad/s] | 0.06 | 0.03 | 0% | 0% | 0.05 | 1 | 1.96 | 0 | |
| KE2 | [g] | 0.02 | 0.15 | 0% | 1% | 0.08 | 0 | 1.96 | 0 |
| [g] | 0.01 | 0.12 | 0% | 1% | 0.01 | 2 | 1.96 | 0 | |
| [g] | 0.01 | 0.09 | 0% | 0% | 0.02 | 9 | 1.96 | 0 | |
| [deg/s] | −6.9 | 14.6 | 79% | 13% | 0.08 | 5 | 1.96 | 0.4 | |
| [deg/s] | −7.7 | 20.1 | 11% | 19% | 0.07 | 15 | 1.96 | 0.5 | |
| [deg/s] | −18.6 | 26.3 | 14% | 23% | 0.01 | 0 | 1.96 | 0.7 | |
| MI [g] | 0 | 0.02 | 0% | 0% | 0.03 | 0 | 2.01 | 0 | |
| MIV [g] | 0 | 0.01 | 0% | 0% | 0.03 | 0 | 2.01 | 0 | |
| RAV [rad/s] | 0.07 | 0.05 | 0% | 0% | 0.05 | 0 | 1.96 | 0 | |
| KE3 | [g] | 0.04 | 0.11 | 0% | 0% | 0.02 | 0 | 1.96 | 0 |
| [g] | 0.01 | 0.12 | 0% | 0% | 0.02 | 0 | 1.96 | 0 | |
| [g] | 0.01 | 0.10 | 0% | 0% | 0.02 | 0 | 1.96 | 0 | |
| [deg/s] | −7.0 | 13.6 | 59% | 11% | 0.08 | 5 | 1.96 | 0.5 | |
| [deg/s] | −7.1 | 18.1 | 10% | 16% | 0.05 | 4 | 1.96 | 0.3 | |
| [deg/s] | −13.6 | 24.5 | 14% | 23% | 0.01 | 0 | 1.96 | 0.2 | |
| MI [g] | 0 | 0.02 | 0% | 0% | 0.03 | 0 | 2.01 | 0 | |
| MIV [g] | 0 | 0.01 | 0% | 0% | 0.03 | 0 | 2.01 | 0 | |
| RAV [rad/s] | 0.06 | 0.04 | 0% | 0% | 0.01 | 0 | 1.96 | 0 | |
| SQ | [g] | 0.01 | 0.06 | 0% | 0% | 0.03 | 19 | 1.96 | 0 |
| [g] | 0.01 | 0.07 | 0% | 0% | 0.02 | 15 | 1.96 | 0 | |
| [g] | 0 | 0.05 | 0% | 0% | 0.08 | 20 | 1.96 | 0 | |
| [deg/s] | 0.18 | 4.7 | 26% | 46% | 0.02 | 15 | 1.96 | 0.13 | |
| [deg/s] | −2.2 | 6.0 | 34% | 59% | 0.02 | 22 | 1.96 | 0.17 | |
| [deg/s] | −5.8 | 15.2 | 9% | 14% | 0.02 | 15 | 1.96 | 0.43 | |
| MI [g] | 0 | 0.01 | 0% | 0% | 0.01 | 2 | 2.02 | 0 | |
| MIV [g] | 0 | 0 | 0% | 0% | 0.01 | 3 | 2.02 | 0 | |
| RAV [rad/s] | 0.02 | 0.03 | 0% | 0% | 0.01 | 14 | 1.96 | 0 |
| Exercises | Parameter | Bias | LoA | CI% Bias | CI% LoA | Kendal’s τ | Outliers | t-Value | se Bias |
|---|---|---|---|---|---|---|---|---|---|
| SF1 | [g] | −0.02 | 0.09 | 0% | 0% | 0.01 | 7 | 1.96 | 0 |
| [g] | −0.01 | 0.28 | 1% | 2% | 0.01 | 2 | 1.96 | 0 | |
| [g] | −0.02 | 0.18 | 1% | 1% | 0.04 | 3 | 1.96 | 0 | |
| [deg/s] | −9.0 | 25.5 | 14% | 24% | 0.02 | 10 | 1.96 | 0.7 | |
| [deg/s] | −25.2 | 17.5 | 9% | 16% | 0.02 | 1 | 1.96 | 0.47 | |
| [deg/s] | −6.2 | 23.0 | 13% | 22% | 0.02 | 13 | 1.96 | 0.67 | |
| MI [g] | 0.02 | 0.06 | 1% | 1% | 0.01 | 2 | 2.02 | 0 | |
| MIV [g] | −0.02 | 0.05 | 0% | 1% | 0.08 | 0 | 2.01 | 0 | |
| RAV [rad/s] | −0.07 | 0.05 | 0% | 0% | 0.01 | 0 | 1.96 | 0 | |
| SF2 | [g] | −0.03 | 0.10 | 0% | 1% | 0.01 | 6 | 1.96 | 0 |
| [g] | 0.03 | 0.17 | 0% | 1% | 0.01 | 3 | 1.96 | 0 | |
| [g] | −0.01 | 0.14 | 0% | 1% | 0.06 | 6 | 1.96 | 0 | |
| [deg/s] | −8.8 | 23.2 | 12% | 21% | 0.02 | 0 | 1.96 | 0.63 | |
| [deg/s] | −30.7 | 24.6 | 13% | 22% | 0.04 | 0 | 1.96 | 0.66 | |
| [deg/s] | −6.6 | 22.0 | 12% | 20% | 0.02 | 0 | 1.96 | 0.61 | |
| MI [g] | 0.01 | 0.04 | 0% | 1% | 0.05 | 1 | 2.01 | 0 | |
| MIV [g] | 0 | 0.02 | 0% | 0% | 0.02 | 2 | 2.02 | 0 | |
| RAV [rad/s] | −0.07 | 0.04 | 0% | 0% | 0.05 | 0 | 1.96 | 0 | |
| SF3 | [g] | −0.03 | 0.16 | 0% | 1% | 0.01 | 6 | 1.96 | 0 |
| [g] | 0.01 | 0.17 | 0% | 1% | 0.08 | 3 | 1.96 | 0 | |
| [g] | −0.02 | 0.15 | 0% | 1% | 0.01 | 6 | 1.96 | 0 | |
| [deg/s] | −10.2 | 25.2 | 13% | 24% | 0.02 | 0 | 1.96 | 0.63 | |
| [deg/s] | −30.4 | 20.4 | 10% | 18% | 0.04 | 0 | 1.96 | 0.66 | |
| [deg/s] | −5.26 | 23.1 | 12% | 22% | 0.02 | 8 | 1.96 | 0.61 | |
| MI [g] | 0.02 | 0.05 | 0% | 1% | 0.04 | 1 | 2.01 | 0 | |
| MIV [g] | −0.01 | 0.03 | 0% | 0% | 0.01 | 2 | 2.02 | 0 | |
| RAV [rad/s] | −0.09 | 0.08 | 0% | 0% | 0.6 * | 0 | 1.96 | 0 | |
| PS | [g] | −0.01 | 0.08 | 0% | 0% | 0.04 | 23 | 1.96 | 0 |
| [g] | 0 | 0.05 | 0% | 0% | 0.01 | 25 | 1.96 | 0 | |
| [g] | 0 | 0.04 | 0% | 0% | 0.03 | 30 | 1.96 | 0 | |
| [deg/s] | −1.3 | 6.6 | 39% | 68% | 0.01 | 36 | 1.96 | 0.2 | |
| [deg/s] | −4.4 | 10.7 | 62% | 107% | 0.04 | 48 | 1.96 | 0.3 | |
| [deg/s] | −5.1 | 8.7 | 50% | 87% | 0.01 | 24 | 1.96 | 0.25 | |
| MI [g] | 0 | 0.02 | 0% | 0% | 0.08 | 3 | 2.02 | 0 | |
| MIV [g] | 0 | 0.01 | 0% | 0% | 0.01 | 3 | 2.02 | 0 | |
| RAV [rad/s] | −0.02 | 0.04 | 0% | 0% | 0.01 | 25 | 1.96 | 0 |
| Exercises | Parameter | Bias | LoA | CI% Bias | CI% LoA | Kendal’s τ | Outliers | t-Value | se Bias |
|---|---|---|---|---|---|---|---|---|---|
| BD1 | [g] | 0 | 0.04 | 0% | 0% | 0.01 | 8 | 1.97 | 0 |
| [g] | 0 | 0.1 | 0% | 1% | 0.08 | 0 | 1.96 | 0 | |
| [g] | 0 | 0.04 | 0% | 0% | 0.01 | 6 | 1.97 | 0 | |
| [deg/s] | −3.9 | 12.4 | 78% | 135% | 0.03 | 0 | 1.96 | 0.39 | |
| [deg/s] | 0 | 3.4 | 21% | 37% | 0.02 | 7 | 1.97 | 0.11 | |
| [deg/s] | −1 | 6.3 | 40% | 69% | 0.01 | 2 | 1.96 | 0.2 | |
| MI [g] | 0 | 0.03 | 0% | 1% | 0.01 | 0 | 2.1 | 0 | |
| MIV [g] | 0 | 0 | 0% | 0% | 0.02 | 1 | 2.1 | 0 | |
| RAV [rad/s] | −0.01 | 0.02 | 0% | 0% | 0.02 | 4 | 1.96 | 0 | |
| BD2 | [g] | 0 | 0.03 | 0% | 0% | 0.01 | 6 | 240 | 0 |
| [g] | 0 | 0.03 | 0% | 0% | 0.01 | 1 | 179 | 0 | |
| [g] | 0 | 0.05 | 0% | 0% | 0.02 | 2 | 208 | 0.01 | |
| [deg/s] | −0.3 | 3.7 | 24% | 43% | 0.02 | 2 | 224 | 0.39 | |
| [deg/s] | −1.9 | 3.4 | 22% | 38% | 0.04 | 2 | 231 | 0.37 | |
| [deg/s] | −0.9 | 2.8 | 19% | 33% | 0.03 | 3 | 209 | 0.06 | |
| MI [g] | 0 | 0.01 | 0% | 0% | 0.03 | 0 | 18 | 0.15 | |
| MIV [g] | 0 | 0 | 0% | 0% | 0.03 | 0 | 16 | 0.07 | |
| RAV [rad/s] | 0 | 0 | 0% | 0% | 0.04 | 0 | 221 | 0.3 | |
| LF | [g] | 0 | 0.01 | 0% | 0% | 0.03 | 12 | 1.97 | 0 |
| [g] | 0 | 0.03 | 0% | 0% | 0.09 | 12 | 1.97 | 0 | |
| [g] | 0 | 0.03 | 0% | 0% | 0.02 | 13 | 1.97 | 0 | |
| [deg/s] | −13.5 | 19.4 | 15% | 27% | 0.06 | 11 | 1.97 | 0.8 | |
| [deg/s] | −0.0 | 5.2 | 43% | 75% | 0.01 | 16 | 1.97 | 0.22 | |
| [deg/s] | −8.6 | 14.6 | 11% | 20% | 0.5 * | 12 | 1.97 | 0.6 | |
| MI [g] | 0 | 0 | 0% | 0% | 0.03 | 1 | 2.1 | 0 | |
| MIV [g] | 0 | 0 | 0% | 0% | 0.01 | 0 | 2.1 | 0 | |
| RAV [rad/s] | −0.09 | 0.08 | 0% | 0% | 0.6 * | 0 | 1.96 | 0 | |
| RO | [g] | −0.03 | 1.40 | 0% | 0% | 0.03 | 12 | 1.97 | 0 |
| [g] | 0 | 0.01 | 0% | 0% | 0.09 | 12 | 1.97 | 0 | |
| [g] | 0 | 0.03 | 0% | 0% | 0.02 | 13 | 1.97 | 0 | |
| [deg/s] | 0 | 0.0 | 115% | 274% | 0.06 | 11 | 1.97 | 0.8 | |
| [deg/s] | −13.5 | 19.4 | 43% | 75% | 0.01 | 16 | 1.97 | 0.22 | |
| [deg/s] | −0.0 | 5.2 | 119% | 206% | 0.5 * | 12 | 1.97 | 0.6 | |
| MI [g] | −8.61 | 14.56 | 0% | 0% | 0.03 | 1 | 2.1 | 0 | |
| MIV [g] | 0 | 0 | 0% | 0% | 0.01 | 0 | 2.1 | 0 | |
| RAV [rad/s] | −0.03 | 0.03 | 0% | 0% | 0.02 | 12 | 1.97 | 0 |
| Exercises | Parameter | Bias | LoA | CI% Bias | CI% LoA | Kendal’s τ | Outliers | t-Value | se Bias |
|---|---|---|---|---|---|---|---|---|---|
| KE1 | LDLJ [a.u.] | 0.06 | 0.32 | 1% | 3% | 0.01 | 0 | 1.96 | 0 |
| PKROM [deg] | 0.7 | 41.9 | 23% | 40% | 0.05 | 40 | 1.96 | 0.09 | |
| DTW [m/s2] | −1.9 | 3.1 | 2% | 3% | 0.06 | 4 | 1.96 | 1.15 | |
| KE2 | LDLJ [a.u.] | 0.00 | 0.48 | 2% | 4% | 0.03 | 7 | 1.96 | 0.01 |
| PKROM [deg] | −8.9 | 15.9 | 9% | 15% | 0.01 | 4 | 1.96 | 0.43 | |
| DTW [m/s2] | −2.5 | 5.0 | 30% | 53% | 0.06 | 41 | 1.96 | 0.15 | |
| KE3 | LDLJ [a.u.] | 0.00 | 0.42 | 1% | 2% | 0.01 | 2 | 1.96 | 0.01 |
| PKROM [deg] | −8.9 | 11.9 | 6% | 13% | 0.01 | 4 | 1.96 | 0.43 | |
| DTW [m/s2] | −2.0 | 4.8 | 30% | 50% | 0.03 | 40 | 1.96 | 0.15 | |
| SQ | LDLJ [a.u.] | 0 | 0.27 | 1% | 2% | 0.01 | 30 | 1.96 | 0 |
| PKROM [deg] | 20.9 | 21.8 | 12% | 21% | 0.7 * | 14 | 1.96 | 0.62 | |
| DTW [m/s2] | −1.7 | 2.6 | 20% | 30% | 0.6 * | 44 | 1.96 | 0.08 | |
| SF1 | LDLJ [a.u.] | 0.03 | 0.15 | 0% | 1% | 0.08 | 1 | 1.96 | 0 |
| PKROM [deg] | 4.7 | 20.4 | 13% | 23% | 0.0 | 54 | 1.96 | 0.67 | |
| DTW [m/s2] | −4.3 | 6.5 | 40% | 70% | 0.7 * | 34 | 1.96 | 0.19 | |
| SF2 | LDLJ [a.u.] | 0.08 | 0.21 | 1% | 1% | 0.01 | 4 | 1.96 | 0 |
| PKROM [deg] | −4.0 | 34.9 | 19% | 33% | 0.0 | 4 | 1.96 | 0.96 | |
| DTW [m/s2] | −3.5 | 4.8 | 30% | 50% | 0.7 * | 33 | 1.96 | 0.14 | |
| SF3 | LDLJ [a.u.] | 0.08 | 0.41 | 2% | 3% | 0.08 | 1 | 1.96 | 0.01 |
| PKROM [deg] | −5.4 | 30.1 | 160% | 290% | 0.0 | 7 | 1.96 | 0.83 | |
| DTW [m/s2] | −3.1 | 5.6 | 30% | 60% | 0.6 * | 47 | 1.96 | 0.17 | |
| PS | LDLJ [a.u.] | 0.03 | 0.31 | 1% | 3% | 0.07 | 272 | 1.96 | 0 |
| PKROM [deg] | 43.6 | 79.6 | 470% | 82% | 0.6 * | 39 | 1.96 | 2.4 | |
| DTW [m/s2] | −2.6 | 3.8 | 20% | 40% | 0.8 * | 55 | 1.97 | 0.15 | |
| BD1 | LDLJ [a.u.] | 0.12 | 1.29 | 8% | 14% | 0.01 | 61 | 1.97 | 0.04 |
| PKROM [deg] | −5.8 | 33.4 | 216% | 374% | 0.03 | 54 | 1.96 | 1.09 | |
| DTW [m/s2] | −2.3 | 4.2 | 29% | 50% | 0.7 * | 73 | 1.97 | 0.14 | |
| BD2 | LDLJ [a.u.] | 0.11 | 0.92 | 6% | 10% | 0.03 | 58 | 1.97 | 0.03 |
| PKROM [deg] | 2.3 | 25.0 | 166% | 288% | 0.03 | 61 | 1.97 | 0.84 | |
| DTW [m/s2] | −1.0 | 1.5 | 11% | 19% | 0.7 * | 78 | 1.97 | 0.05 | |
| LF | LDLJ [a.u.] | 0.08 | 0.5 | 4% | 7% | 0.06 | 13 | 1.97 | 0.02 |
| PKROM [deg] | −9.8 | 60.7 | 506% | 877% | 0.02 | 18 | 1.97 | 2.56 | |
| DTW [m/s2] | −2.3 | 4.2 | 41% | 72% | 0.8 * | 36 | 1.98 | 0.21 | |
| RO | LDLJ [a.u.] | 0.29 | 1.15 | 9% | 16% | 0.07 | 16 | 1.97 | 0.04 |
| PKROM [deg] | 0.1 | 70.0 | 58% | 1014% | 0.02 | 17 | 1.97 | 2.96 | |
| DTW [m/s2] | −2.3 | 3.13 | 28% | 49% | 0.7 * | 27 | 1.97 | 0.14 |
References
- Haleem, A.; Javaid, M.; Singh, R.P.; Suman, R. Telemedicine for healthcare: Capabilities, features, barriers, and applications. Sens. Int. 2021, 2, 100117. [Google Scholar] [CrossRef] [PubMed]
- Jirasakulsuk, N.; Saengpromma, P.; Khruakhorn, S. Real-time telerehabilitation in older adults with musculoskeletal conditions: Systematic review and meta-analysis. JMIR Rehabil. Assist. Technol. 2022, 9, e36028. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.G.d.S.; Pinto, A.C.P.N.; Garcia, B.M.S.P.; Eid, R.A.C.; Mól, C.G.; Nawa, R.K. Telerehabilitation improves physical function and reduces dyspnoea in people with COVID-19 and post-COVID-19 conditions: A systematic review. J. Physiother. 2022, 68, 90–98. [Google Scholar] [CrossRef]
- Lundell, S.; Holmner, A.; Rehn, B.; Nyberg, A.; Wadell, K. Telehealthcare in COPD: A systematic review and meta-analysis on physical outcomes and dyspnea. Respir. Med. 2015, 109, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Ibeggazene, S.; Turner, R.; Rosario, D.; Bourke, L. Remote interventions to improve exercise behaviour in sedentary people living with and beyond cancer: A systematic review and meta-analysis. BMC Cancer 2021, 21, 308. [Google Scholar] [CrossRef]
- Berton, A.; Candela, U.G.; Fioravanti, V.; Giannone, L.; Arcangeli, S.; Denaro, V. Virtual reality, augmented reality, gamification, and telerehabilitation: Psychological impact on orthopedic patients’ rehabilitation. J. Clin. Med. 2020, 9, 2567. [Google Scholar] [CrossRef]
- Kingston, G.; Gray, M.A.; Williams, G. A critical review of the evidence on the use of videotapes or DVD to promote patient compliance with home programmes. Disabil. Rehabil. Assist. Technol. 2010, 5, 153–163. [Google Scholar] [CrossRef]
- Stavropoulos, T.G.; Papastergiou, A.; Mpaltadoros, L.; Nikolopoulos, S.; Kompatsiaris, I. IoT Wearable sensors and devices in elderly care: A literature review. Sensors 2020, 20, 2826. [Google Scholar] [CrossRef]
- Lu, L.; Zhang, J.; Xie, Y.; Gao, F.; Xu, S.; Wu, X.; Ye, Z. Wearable health devices in health care: Narrative systematic review. JMIR mHealth uHealth 2020, 8, e18907. [Google Scholar] [CrossRef]
- Giggins, O.M.; Persson, U.M.; Caulfield, B. Biofeedback in rehabilitation. J. Neuroeng. Rehabil. 2013, 10, 60. [Google Scholar] [CrossRef]
- Tedesco, S.; Urru, A.; Peckitt, J.; O’Flynn, B. Inertial sensors-based lower-limb rehabilitation assessment: A comprehensive evaluation of gait, kinematic and statistical metrics. Int. J. Adv. Life Sci. 2017, 9, 33–49. Available online: http://www.iariajournals.org/life_sciences/ (accessed on 1 June 2017).
- Komaris, D.S.; Tarfali, G.; O’Flynn, B.; Tedesco, S. Unsupervised IMU-based evaluation of at-home exercise programmes: A feasibility study. BMC Sports Sci. Med. Rehabil. 2022, 14, 28. [Google Scholar] [CrossRef]
- Picerno, P.; Iosa, M.; D’Souza, C.; Benedetti, M.G.; Paolucci, S.; Morone, G. Wearable inertial sensors for human movement analysis: A five-year update. Expert Rev. Med. Devices 2021, 18 (Suppl. 1), 79–94. [Google Scholar] [CrossRef] [PubMed]
- Porciuncula, F.; Roto, A.V.; Kumar, D.; Davis, I.; Walsh, C.J.; Awad, L.N. Wearable Movement Sensors for Rehabilitation: A Focused Review of Technological and Clinical Advances. PM&R 2018, 10 (Suppl. 2), S220–S232. [Google Scholar] [CrossRef]
- Routhier, F.; Duclos, N.C.; Lacroix, É.; Lettre, J.; Turcotte, E.; Hamel, N.; Michaud, F.; Duclos, C.; Archambault, P.S.; Bouyer, L.J. Clinicians’ perspectives on inertial measurement units in clinical practice. PLoS ONE 2020, 15, e0241922. [Google Scholar] [CrossRef]
- Saaei, F.; Klappa, S.G. Rethinking telerehabilitation: Attitudes of physical therapists and patients. J. Patient Exp. 2021, 28, 8. [Google Scholar] [CrossRef] [PubMed]
- Silva-Batista, C.; Wilhelm, J.L.; Scanlan, K.T.; Stojak, M.; Carlson-Kuhta, P.; Chen, S.; Liu, W.; de la Huerta, T.N.G.; Horak, F.B.; Mancini, M.; et al. Balance telerehabilitation and wearable technology for people with Parkinson’s disease (TelePD trial). BMC Neurol. 2023, 23, 368. [Google Scholar] [CrossRef]
- Capecci, M.; Cima, R.; Barbini, F.A.; Mantoan, A.; Sernissi, F.; Lai, S.; Fava, R.; Tagliapietra, L.; Ascari, L.; Izzo, R.N.; et al. Telerehabilitation with ARC intellicare to cope with motor and respiratory disabilities: Results about the process, usability, and clinical effect of the “Ricominciare” Pilot Study. Sensors 2023, 23, 7238. [Google Scholar] [CrossRef]
- Caramia, F.; D’Angelantonio, E.; De Angelis, F.; Lucangeli, L.; Campanini, I.; Pallotti, A.; Camomilla, V. Design of a care pathway in telerehabilitation on respiratory exercise and physical reactivation of patients suffering from respiratory diseases or COVID-19. In Proceedings of the 17th International Symposium of 3-D Analysis of Human Movement (3D-AHM 2022), Tokyo, Japan, 16–19 July 2022. [Google Scholar]
- Atzori, L.; Iera, A.; Morabito, G. The Internet of Things: A survey. Comput. Netw. 2010, 54, 2787–2805. [Google Scholar] [CrossRef]
- Bruno, I.; Lobo, G.; Covino, B.V.; Donarelli, A.; Marchetti, V.; Panni, A.S.; Molinari, F. Technology readiness revisited: A proposal for extending the scope of impact assessment of European public services. In Proceedings of the 13th International Conference on Theory and Practice of Electronic Governance, Athens, Greece, 23–25 September 2020; pp. 369–380. [Google Scholar]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef]
- Nikitas, C.; Kikidis, D.; Bibas, A.; Pavlou, M.; Zachou, Z.; Bamiou, D.E. Recommendations for physical activity in the elderly population: A scoping review of guidelines. J. Frailty Sarcopenia Falls 2022, 7, 18–28. [Google Scholar] [CrossRef] [PubMed]
- Graham, J. Exercise: Bird Dog. Strength Cond. J. 2009, 31, 93–94. [Google Scholar] [CrossRef]
- Winter, D.A. Signal Processing. In Biomechanics and Motor Control of Human Movement; John Wiley & Sons: Hoboken, NJ, USA, 2009; pp. 14–44. [Google Scholar] [CrossRef]
- Strohrmann, C.; Labruyère, R.; Gerber, C.N.; van Hedel, H.J.; Arnrich, B.; Tröster, G. Monitoring motor capacity changes of children during rehabilitation using body-worn sensors. J. Neuroeng. Rehabil. 2013, 10, 83. [Google Scholar] [CrossRef]
- Jiang, S.; Zhang, B.; Wei, D. The elderly fall risk assessment and prediction based on gait analysis. In Proceedings of the 2011 IEEE 11th International Conference on Computer and Information Technology, Paphos, Cyprus, 31 August–2 September 2011; pp. 176–180. [Google Scholar] [CrossRef]
- Venek, V.; Kranzinger, S.; Schwameder, H.; Stöggl, T. Human movement quality assessment using sensor technologies in recreational and professional sports: A scoping review. Sensors 2022, 22, 4786. [Google Scholar] [CrossRef] [PubMed]
- Hogan, N.; Sternad, D. Sensitivity of smoothness measures to movement duration, amplitude, and arrests. J. Mot. Behav. 2009, 41, 529–534. [Google Scholar] [CrossRef]
- Melendez-Calderon, A.; Shirota, C.; Balasubramanian, S. Estimating movement smoothness from inertial measurement units. Front. Bioeng. Biotechnol. 2021, 8, 558771. [Google Scholar] [CrossRef]
- Madgwick, S.O.H.; Harrison, A.J.L.; Vaidyanathan, R. Estimation of IMU and MARG orientation using a gradient descent algorithm. In Proceedings of the IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; pp. 1–7. [Google Scholar] [CrossRef]
- Adamowicz, L.; Gurchiek, R.D.; Ferri, J.; Ursiny, A.T.; Fiorentino, N.; McGinnis, R.S. Validation of novel relative orientation and inertial sensor-to-segment alignment algorithms for estimating 3D hip joint angles. Sensors 2019, 19, 5143. [Google Scholar] [CrossRef] [PubMed]
- Saisana, M. Barthel Index. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014. [Google Scholar] [CrossRef]
- Heath, E.M. Borg’s Perceived Exertion and Pain Scales. Med. Sci. Sports Exerc. 1998, 30, 1461. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistics Notes: Measurement error proportional to the mean. BMJ 1996, 313, 106. [Google Scholar] [CrossRef]
- Kendall, M.G. A new measure of rank correlation. Biometrika 1938, 30, 81–93. [Google Scholar] [CrossRef]
- Brehm, M.-A.; Scholtes, V.A.; Dallmeijer, A.J.; Twisk, J.W.; Harlaar, J. The importance of addressing heteroscedasticity in the reliability analysis of ratio-scaled variables: An example based on walking energy-cost measurements. Dev. Med. Child Neurol. 2012, 54, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed]



| Characteristics | Prototypical IMU | Reference IMU |
|---|---|---|
| Unit cost | ≈30 euros (production cost) | Up to 2000 euros * (commercial cost) |
| Dimension | 7 × 4.5 × 1.5 cm | 5 × 4 × 1.4 cm |
| Mass | 35 g | 26 g |
| Battery | 10 h | Up to 12 h |
| Connection | Bluetooth | Wireless |
| Sample frequency | 32 Hz | 128 Hz |
| Accelerometer range | ±4 g | ±6 g |
| Gyroscope range | ±2000 deg/s | ±2000 deg/s |
| Magnetometer range | ±6 Gauss | ±6 Gauss |
| Category | Exercises | RPE [a.u.] | VAS [0–10] |
|---|---|---|---|
| Lower limb | KE1 | 1.4 ± 1.5 | 9.1 ± 1.2 |
| KE2 | 1.3 ± 1.1 | 9.1 ± 1.2 | |
| KE3 | 0.8 ± 1.0 | 9.1 ± 1.2 | |
| SQ | 0.9 ± 1.0 | 9.1 ± 1.2 | |
| Upper limb | SF1 | 1.2 ± 1.6 | 8.7 ± 1.5 |
| SF2 | 1.5 ± 1.6 | 8.7 ± 1.5 | |
| SF3 | 1.8 ± 1.8 | 8.7 ± 1.5 | |
| PS | 1.4 ± 1.1 | 8.7 ± 1.5 | |
| Trunk | BD1 | 1.4 ± 1.5 | 9.1 ± 1.2 |
| BD2 | 2.1 ± 1.8 | 7.9 ± 3.1 | |
| LF | 1.1 ± 1.2 | 8.8 ± 1.4 | |
| RO | 1.8 ± 1.8 | 8.7 ± 1.6 |
| Reference IMUs | ||||||||||||||||
| Category | Exercises | Quantity | Intensity | Quality | ||||||||||||
| REP | TIME [s] | [g] | [g] | [g] | [deg/s] | [deg/s] | [deg/s] | MI [g] | MIV [g] | RAV [rad/s] | LDLJ [a.u.] | PKROM [deg] | DTW [m/s2] | |||
| Lower limb | KE1 | Mean | 8 | 2.3 | 1.6 | 0.5 | 0.3 | 26.0 | 43.4 | 197.7 | 0.3 | 0.2 | 0.5 | −1.6 | 117.4 | 4.6 |
| Std | 0 | 0.5 | 0.2 | 0.1 | 0.2 | 13.1 | 27.6 | 27.9 | 0 | 0 | 0.1 | 0.2 | 14.4 | 2.2 | ||
| KE2 | Mean | 8 | 1.8 | 0.9 | 0.8 | 0.2 | 32.2 | 48.9 | 205.2 | 0.3 | 0.1 | 0.6 | −1.5 | 75.2 | 7.5 | |
| Std | 0 | 0.5 | 0.2 | 0.1 | 0.1 | 18.4 | 37.8 | 41.5 | 0 | 0 | 0.1 | 0.6 | 13.5 | 3.4 | ||
| KE3 | Mean | 8 | 1.6 | 0.8 | 0.7 | 0.2 | 32.5 | 42.1 | 197.3 | 0.2 | 0.1 | 0.4 | −1.5 | 73.2 | 6.6 | |
| Std | 0 | 0.4 | 0.2 | 0.1 | 0 | 10.2 | 30.1 | 44.8 | 0 | 0 | 0.1 | 0.7 | 10.3 | 3.6 | ||
| SQ | Mean | 8 | 2.3 | 0.1 | 0.4 | 0.1 | 6.6 | 11.9 | 45.3 | 0.2 | 0 | 0.1 | −1.9 | 9.2 | 3.2 | |
| Std | 0 | 0.6 | 0.1 | 0.1 | 0.1 | 3.9 | 7.7 | 12.3 | 0 | 0 | 0 | 0.2 | 3.5 | 2.8 | ||
| Upper limb | SF1 | Mean | 8 | 3.2 | 0.7 | 0.8 | 2.0 | 52.6 | 181.0 | 69.4 | 0.8 | 0.6 | 0.5 | −1.8 | 153.9 | 8.2 |
| Std | 0 | 1.1 | 0.2 | 0.4 | 0.4 | 26.8 | 39.9 | 41.7 | 0.1 | 0.1 | 0.1 | 0.2 | 28.1 | 5.5 | ||
| SF2 | Mean | 8 | 2.5 | 1.4 | 0.7 | 1.1 | 72.3 | 188.0 | 54.9 | 0.7 | 0.4 | 0.5 | −1.9 | 69.1 | 6.8 | |
| Std | 0 | 0.6 | 0.3 | 0.2 | 0.4 | 27.3 | 36.6 | 28.3 | 0.1 | 0.1 | 0.1 | 0.3 | 11.1 | 4.8 | ||
| SF3 | Mean | 8 | 2.2 | 1.5 | 0.7 | 0.9 | 82.7 | 195.9 | 68.4 | 0.6 | 0.3 | 0.5 | −1.9 | 66.9 | 7.2 | |
| Std | 0 | 0.6 | 0.2 | 0.3 | 0.4 | 36.8 | 45.2 | 40.0 | 0.1 | 0 | 0.1 | 0.4 | 13.3 | 6.0 | ||
| PS | Mean | 8 | 2.6 | 0.4 | 0.2 | 0.2 | 12.4 | 35.7 | 44.4 | 0.2 | 0 | 0.1 | −1.4 | 22.3 | 4.8 | |
| Std | 0 | 0.5 | 0.2 | 0.1 | 0.1 | 9.3 | 18.5 | 10.6 | 0.1 | 0 | 0 | 0.6 | 12.3 | 4.6 | ||
| Trunk | BD1 | Mean | 8 | 2.0 | 0.1 | 0.2 | 0 | 21.8 | 5.7 | 8.7 | 0.1 | 0 | 0.1 | −1.3 | 29.4 | 4.9 |
| Std | 0 | 0.5 | 0.1 | 0.1 | 0 | 10.8 | 3.5 | 3.7 | 0.1 | 0 | 0 | 1.0 | 17.2 | 5.4 | ||
| BD2 | Mean | 8 | 1.9 | 0.1 | 0.1 | 0.1 | 6.4 | 10.9 | 6.5 | 0.1 | 0 | 0 | −0.9 | 65.7 | 2.1 | |
| Std | 0 | 0.5 | 0.1 | 0.1 | 0.1 | 4.5 | 6.6 | 4.1 | 0 | 0 | 0 | 0.9 | 17.5 | 2.2 | ||
| LF | Mean | 8 | 2.8 | 0 | 0.2 | 0.1 | 10.9 | 5.7 | 15.4 | 0.1 | 0 | 0 | −1.6 | 63.5 | 10.0 | |
| Std | 0 | 0.8 | 0 | 0.1 | 0 | 5.9 | 3.8 | 8.5 | 0 | 0 | 0 | 0.5 | 26.4 | 6.7 | ||
| RO | Mean | 8 | 2.6 | 0 | 0.1 | 0.1 | 80.5 | 7.0 | 20.7 | 0.1 | 0 | 0.2 | −2.0 | 52.9 | 3.5 | |
| Std | 0 | 0.7 | 0 | 0 | 0 | 19.3 | 3.3 | 11.3 | 0 | 0 | 0 | 0.7 | 22.1 | 2.3 | ||
| Prototype IMUs | ||||||||||||||||
| Category | Exercises | Quantity | Intensity | Quality | ||||||||||||
| REP | TIME [s] | [g] | [g] | [g] | [deg/s] | [deg/s] | [deg/s] | MI [g] | MIV [g] | RAV [rad/s] | LDLJ [a.u.] | PKROM [deg] | DTW [m/s2] | |||
| Lower limb | KE1 | Mean | 8 | 2.3 | 1.5 | 0.5 | 0.2 | 21.1 | 35.2 | 179.7 | 0.3 | 0.2 | 0.4 | −1.6 | 117.2 | 2.1 |
| Std | 0 | 0.5 | 0.1 | 0 | 0.1 | 13.1 | 22.2 | 27 | 0 | 0 | 0 | 0.2 | 19.9 | 1.4 | ||
| KE2 | Mean | 8 | 1.7 | 0.8 | 0.8 | 0.2 | 25.4 | 38.2 | 186.5 | 0.2 | 0.1 | 0.4 | −1.5 | 66.5 | 2.7 | |
| Std | 0 | 0.4 | 0.1 | 0.1 | 0.1 | 16.3 | 29.4 | 42.4 | 0 | 0 | 0.1 | 0.6 | 10.7 | 2.6 | ||
| KE3 | Mean | 8 | 1.6 | 0.8 | 0.7 | 0.2 | 22.5 | 32.1 | 177.3 | 0.2 | 0.1 | 0.4 | −1.5 | 63.2 | 2.6 | |
| Std | 0 | 0.4 | 0.2 | 0.1 | 0 | 10.2 | 20.1 | 34.8 | 0 | 0 | 0.1 | 0.7 | 9.3 | 1.6 | ||
| SQ | Mean | 8 | 2.3 | 0.1 | 0.1 | 0.5 | 6.5 | 35.5 | 3.5 | 0.2 | 0 | 0.1 | −1.9 | 21.0 | 1.3 | |
| Std | 0 | 0.5 | 0 | 0 | 0.1 | 3.2 | 165 | 1.8 | 0 | 0 | 0 | 0.2 | 8.4 | 1.1 | ||
| Upper limb | SF1 | Mean | 8 | 3.1 | 0.6 | 0.7 | 1.9 | 42.2 | 155.6 | 60.2 | 0.8 | 0.6 | 0.3 | −1.8 | 160.6 | 3.3 |
| Std | 0 | 1.5 | 0.2 | 0.3 | 0.4 | 20.2 | 35.6 | 33 | 0.1 | 0.1 | 0 | 0.2 | 24.1 | 1.7 | ||
| SF2 | Mean | 8 | 2.4 | 1.3 | 0.7 | 1.1 | 63.5 | 157.2 | 47.3 | 0.7 | 0.4 | 0.4 | −1.9 | 66.8 | 2.5 | |
| Std | 0 | 0.5 | 0.2 | 0.2 | 0.3 | 24.3 | 29.5 | 23.6 | 0 | 0.1 | 0 | 0.3 | 15.2 | 1.1 | ||
| SF3 | Mean | 8 | 2.1 | 1.4 | 0.7 | 0.8 | 71.8 | 165.4 | 61.7 | 0.6 | 0.3 | 0.4 | −1.9 | 63.2 | 3.3 | |
| Std | 0 | 0.5 | 0.2 | 0.2 | 0.3 | 32.1 | 38.9 | 34.3 | 0.1 | 0 | 0.1 | 0.4 | 15.3 | 3.9 | ||
| PS | Mean | 8 | 2.5 | 0.1 | 0.1 | 0.3 | 4.6 | 18.4 | 1.4 | 0.1 | 0 | 0.1 | −1.4 | 34.9 | 0.6 | |
| Std | 0 | 0.4 | 0 | 0 | 0.1 | 2.2 | 7.8 | 0.8 | 0 | 0 | 0 | 0.6 | 17.3 | 0.5 | ||
| Trunk | BD1 | Mean | 8 | 2.0 | 0.1 | 0.2 | 0.1 | 17.8 | 5.8 | 7.9 | 0.1 | 0 | 0 | −1.3 | 23.5 | 1.4 |
| Std | 0 | 0.5 | 0 | 0 | 0 | 8.4 | 3.5 | 4.6 | 0 | 0 | 0 | 1.0 | 13.3 | 1.5 | ||
| BD2 | Mean | 8 | 1.8 | 0.1 | 0.1 | 0.1 | 6 | 8.8 | 5.6 | 0.1 | 0 | 0 | −0.9 | 69.1 | 0.5 | |
| Std | 0 | 0.4 | 0 | 0 | 0 | 3.7 | 5.4 | 4 | 0 | 0 | 0 | 0.9 | 15.5 | 0.4 | ||
| LF | Mean | 8 | 2.6 | 0 | 0.2 | 0.1 | 8.2 | 4.5 | 13.8 | 0.1 | 0 | 0 | −1.6 | 53.6 | 1.3 | |
| Std | 0 | 0.8 | 0 | 0 | 0 | 4.4 | 2.5 | 7.5 | 0 | 0 | 0 | 0.5 | 26.2 | 2.0 | ||
| RO | Mean | 8 | 2.5 | 0 | 0.1 | 0.1 | 66.9 | 7.4 | 12 | 0.1 | 0 | 0.1 | −2.0 | 56.3 | 0.7 | |
| Std | 0 | 0.7 | 0 | 0 | 0 | 17.3 | 4 | 5.5 | 0 | 0 | 0 | 0.7 | 27.8 | 0.5 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caramia, F.; D’Angelantonio, E.; Lucangeli, L.; Camomilla, V. Validation of Low-Cost IMUs for Telerehabilitation Exercises. Sensors 2025, 25, 3129. https://doi.org/10.3390/s25103129
Caramia F, D’Angelantonio E, Lucangeli L, Camomilla V. Validation of Low-Cost IMUs for Telerehabilitation Exercises. Sensors. 2025; 25(10):3129. https://doi.org/10.3390/s25103129
Chicago/Turabian StyleCaramia, Federico, Emanuele D’Angelantonio, Leandro Lucangeli, and Valentina Camomilla. 2025. "Validation of Low-Cost IMUs for Telerehabilitation Exercises" Sensors 25, no. 10: 3129. https://doi.org/10.3390/s25103129
APA StyleCaramia, F., D’Angelantonio, E., Lucangeli, L., & Camomilla, V. (2025). Validation of Low-Cost IMUs for Telerehabilitation Exercises. Sensors, 25(10), 3129. https://doi.org/10.3390/s25103129