
The Relationship between Sleeping Position and Sleep Quality: A Flexible Sensor-Based Study


Abstract
:1. Introduction
2. Study of a Flexible Wearable Sleeping-Position Monitoring Device
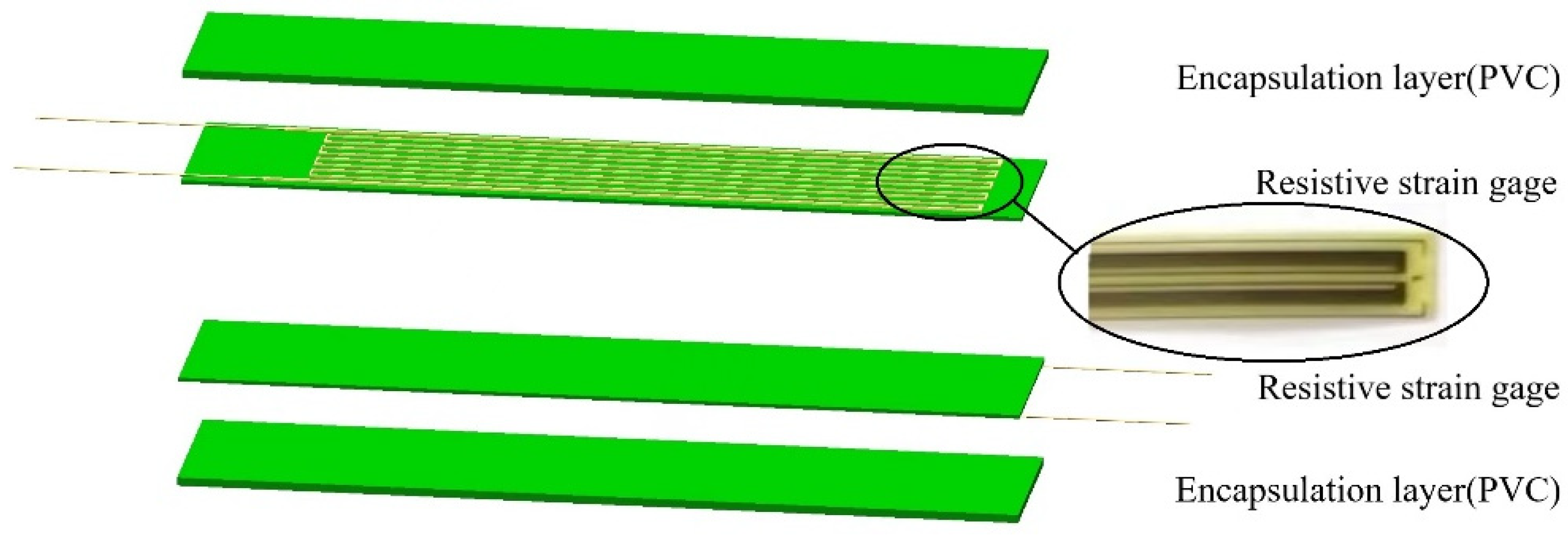
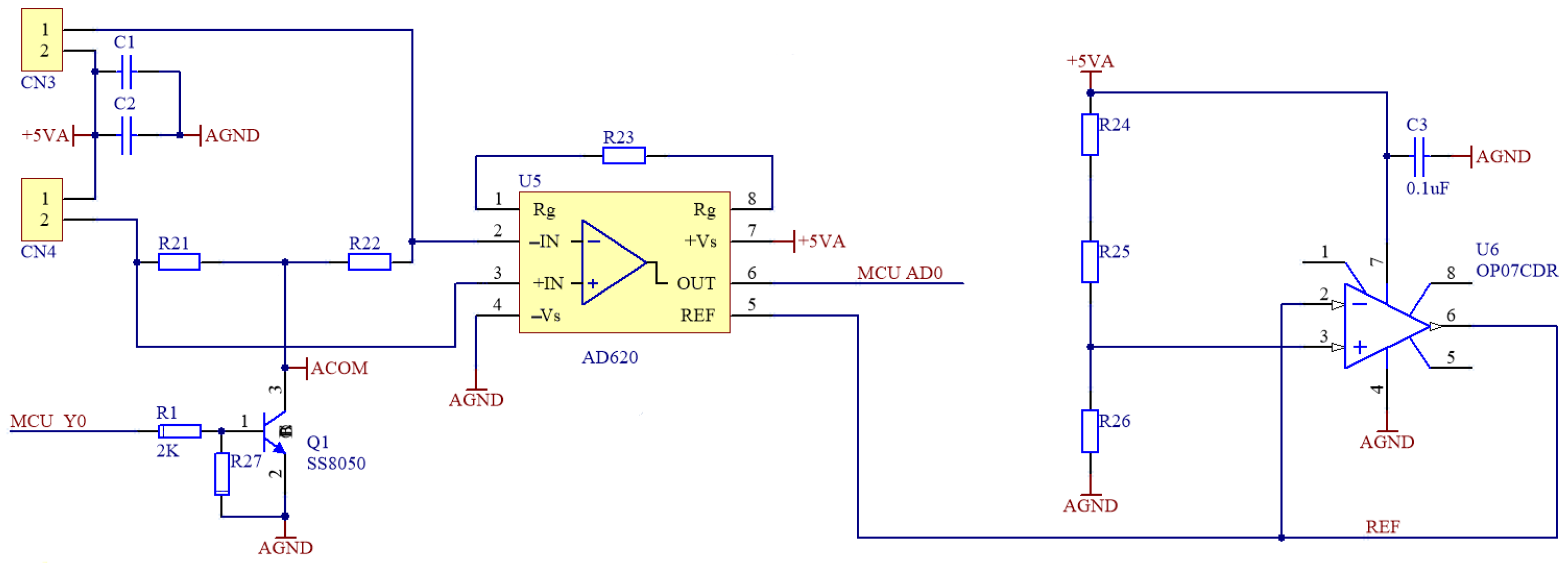
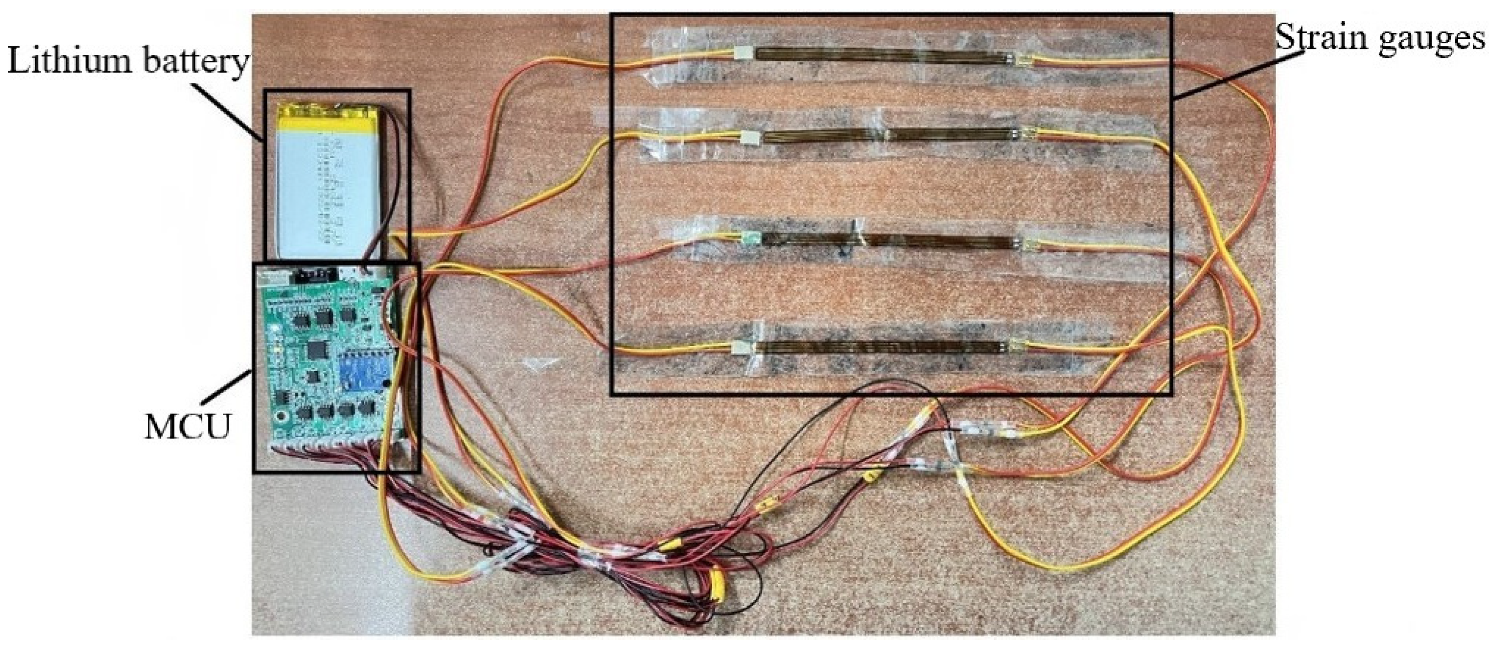
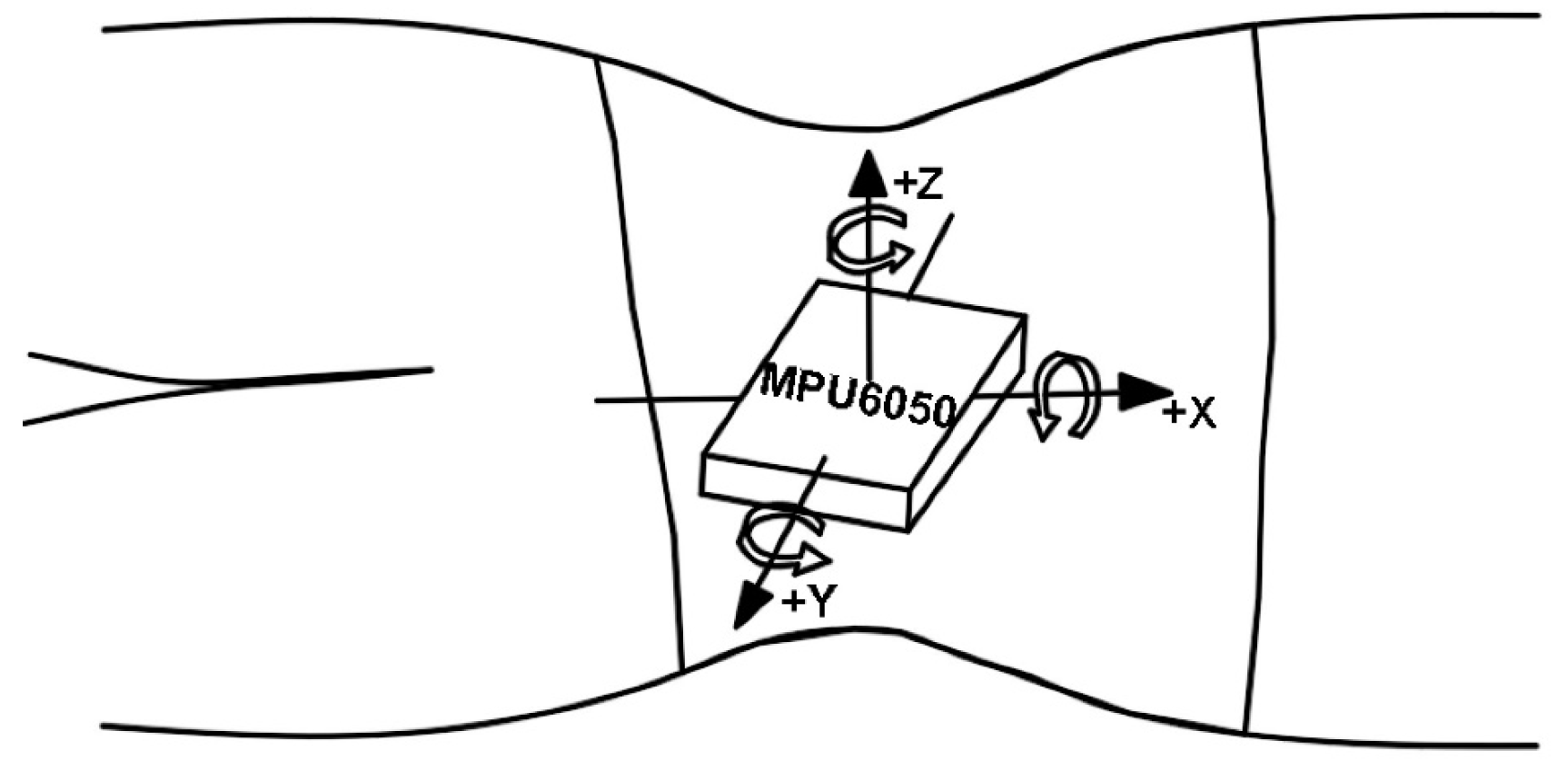
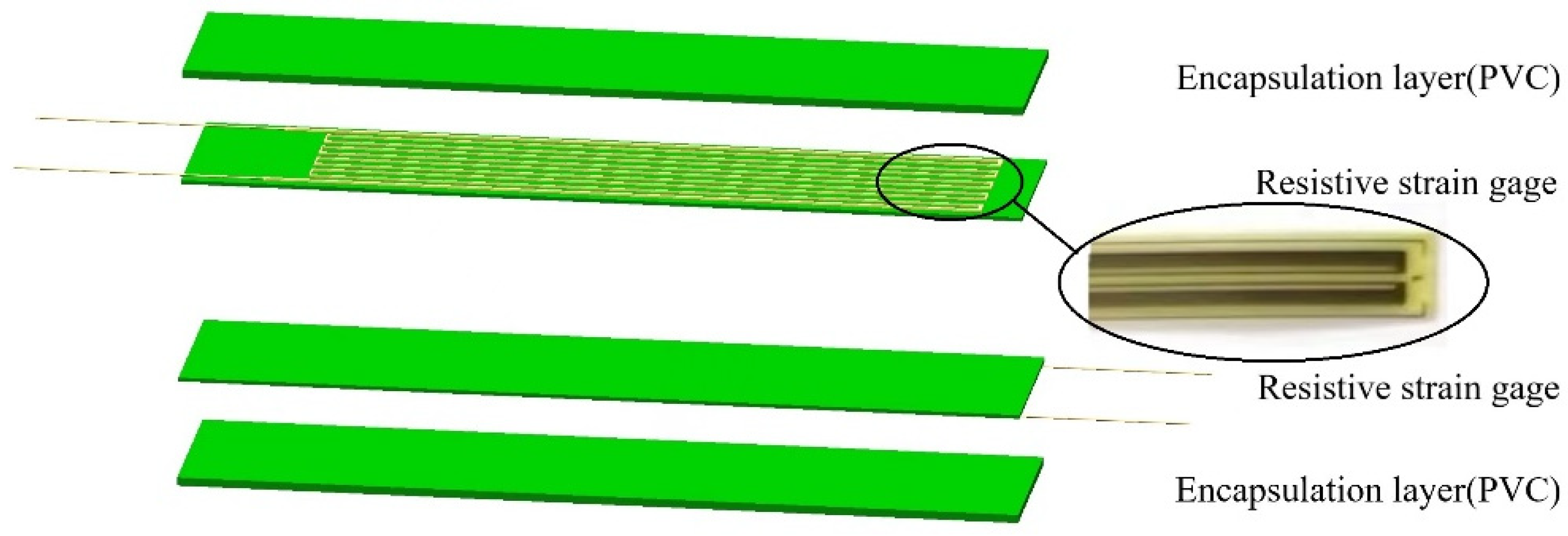
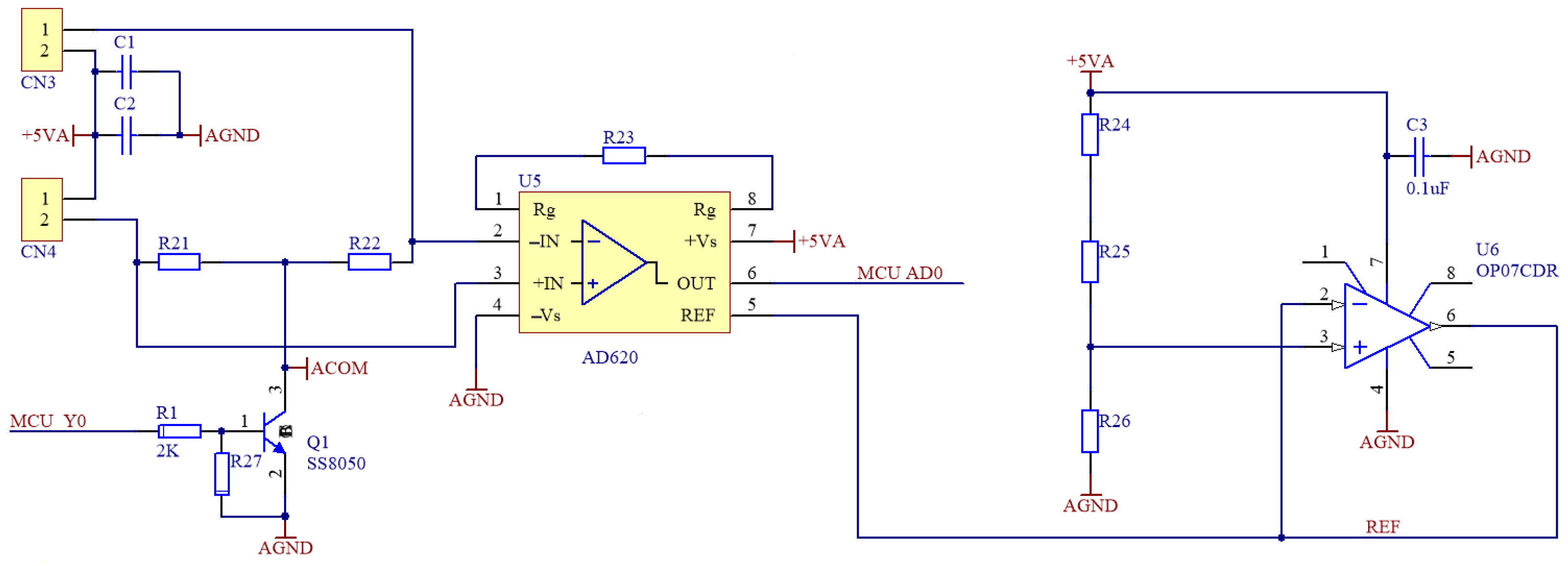
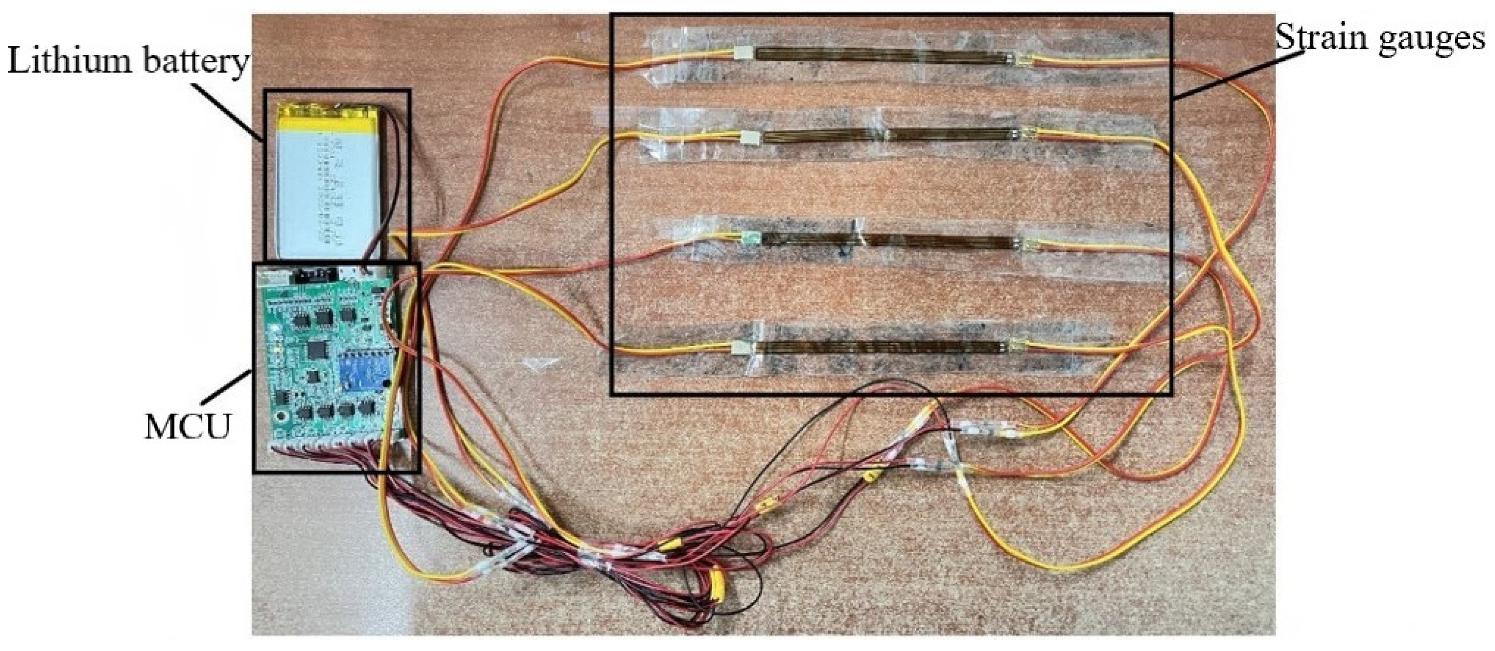
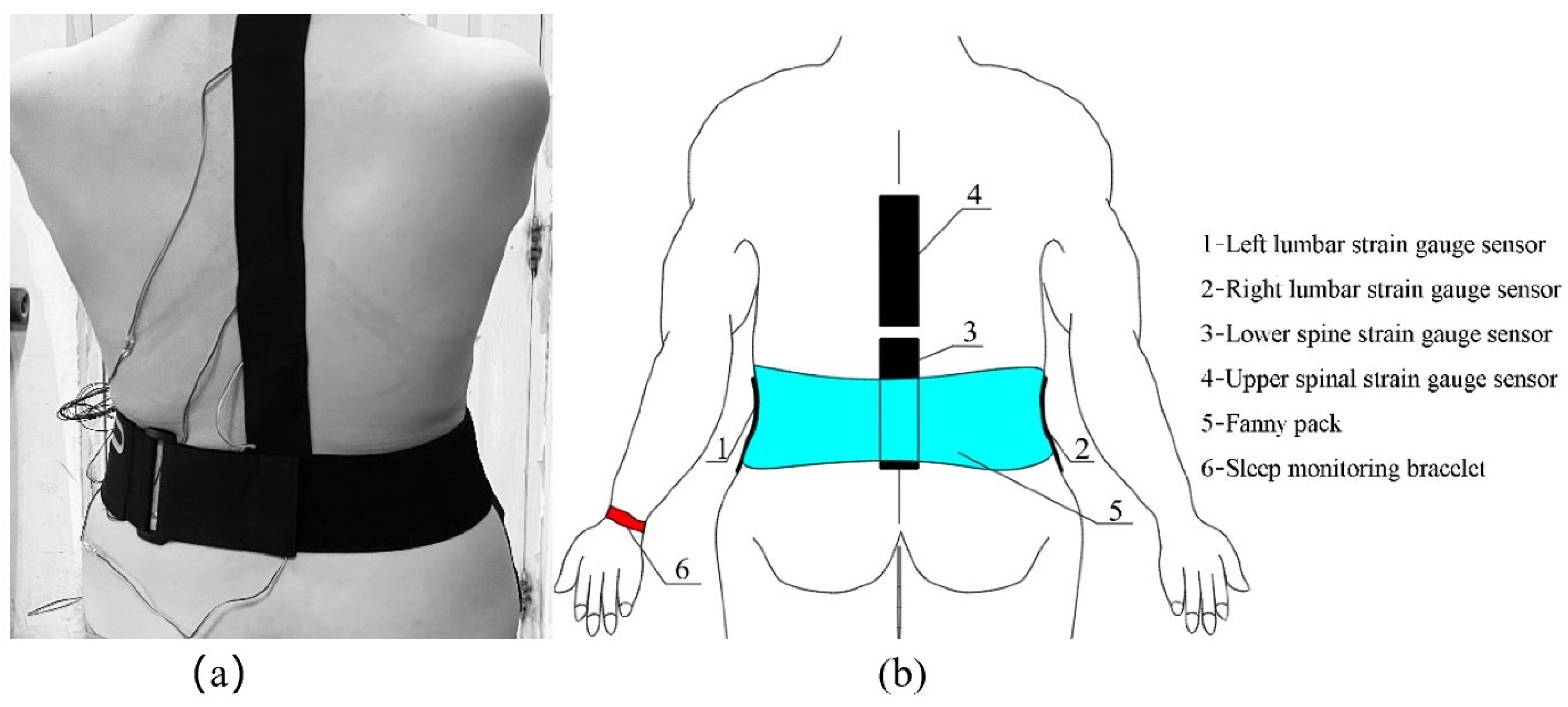
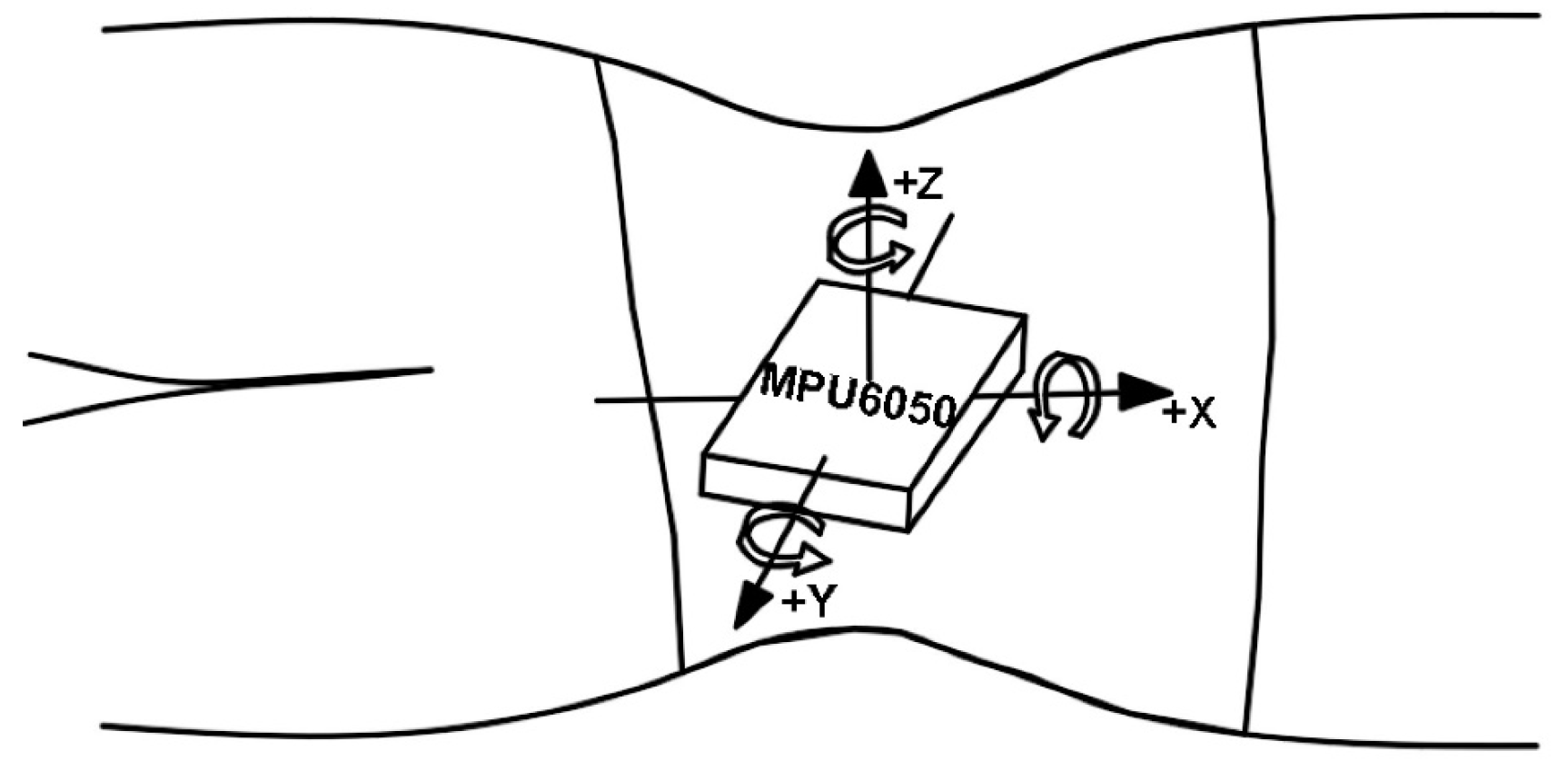
2.1. Structure of the Flexible Wearable Sleeping-Position Monitoring Device
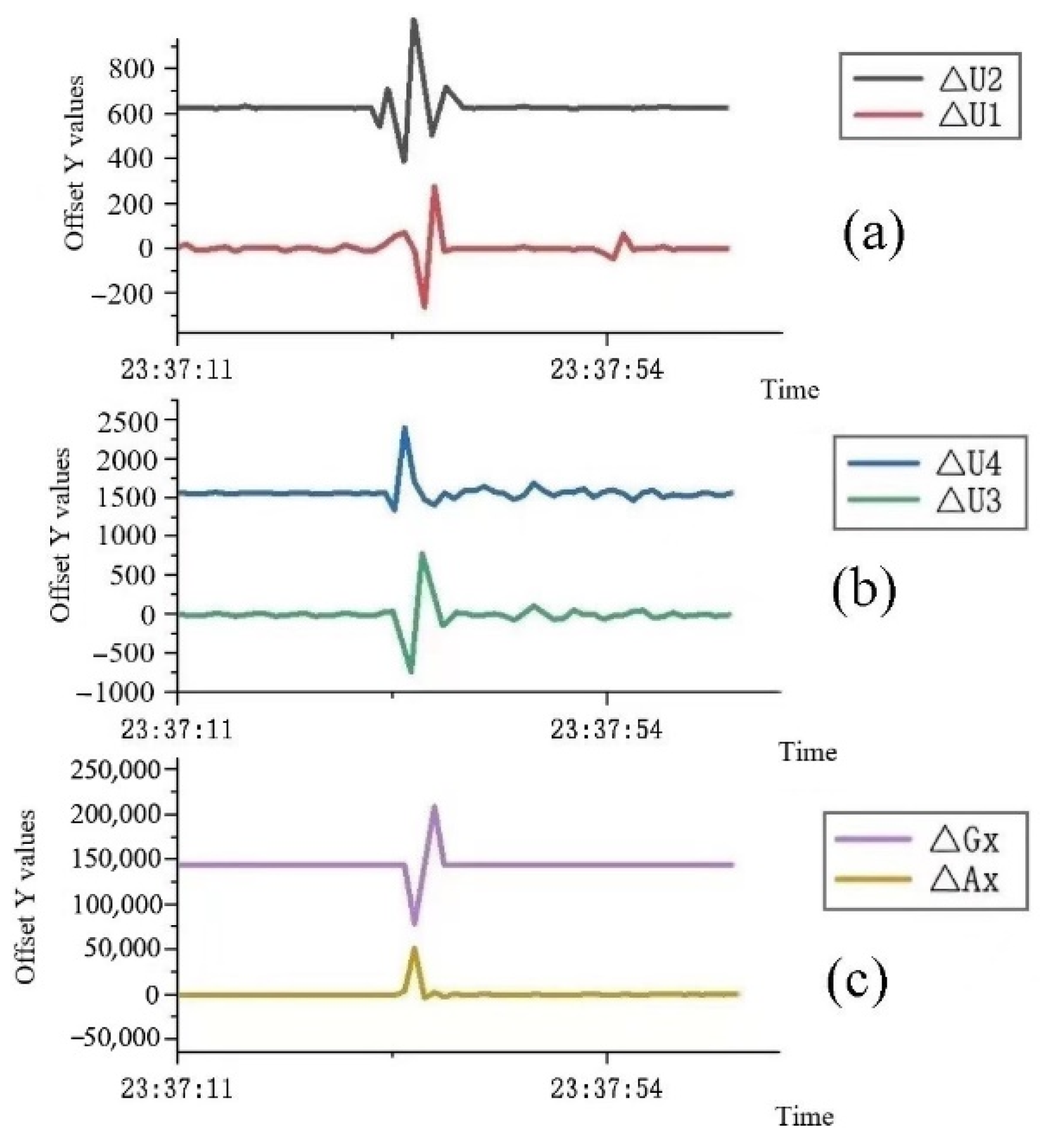
2.2. Experimental Procedure for the Reliability of the Flexible Wearable Sleeping-Position Monitoring Device
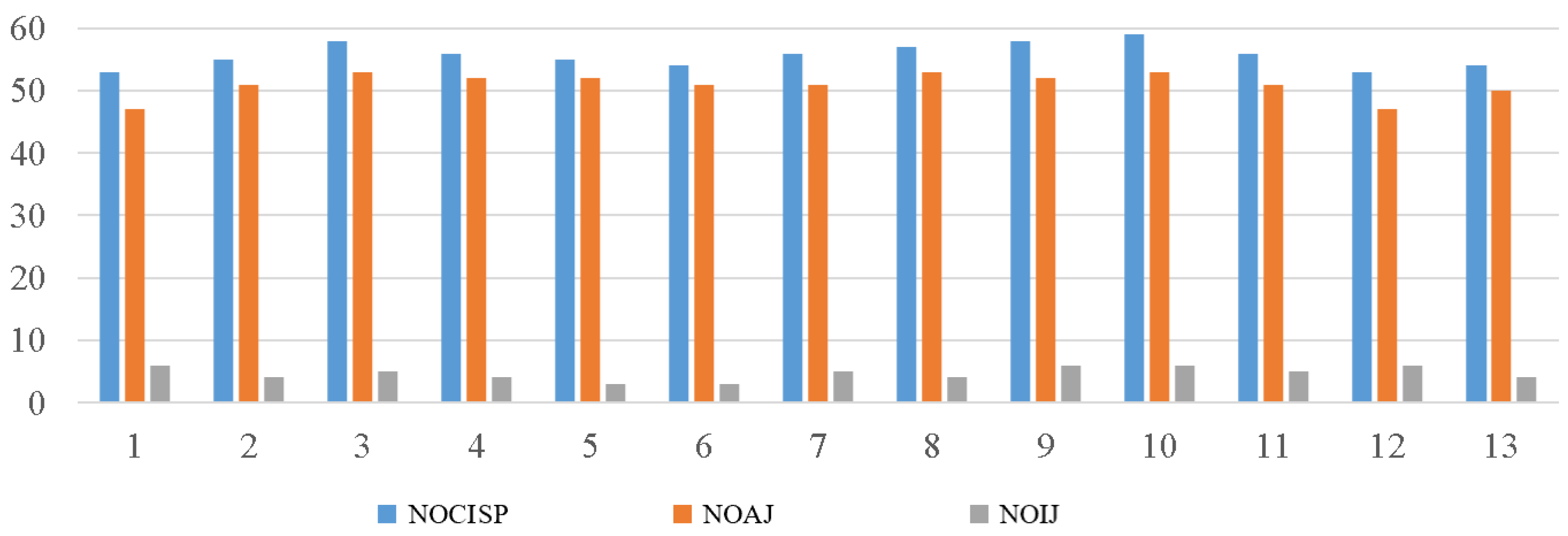
2.3. Statistical Analysis of the Reliability of the Flexible Wearable Sleeping-Position Monitoring Device
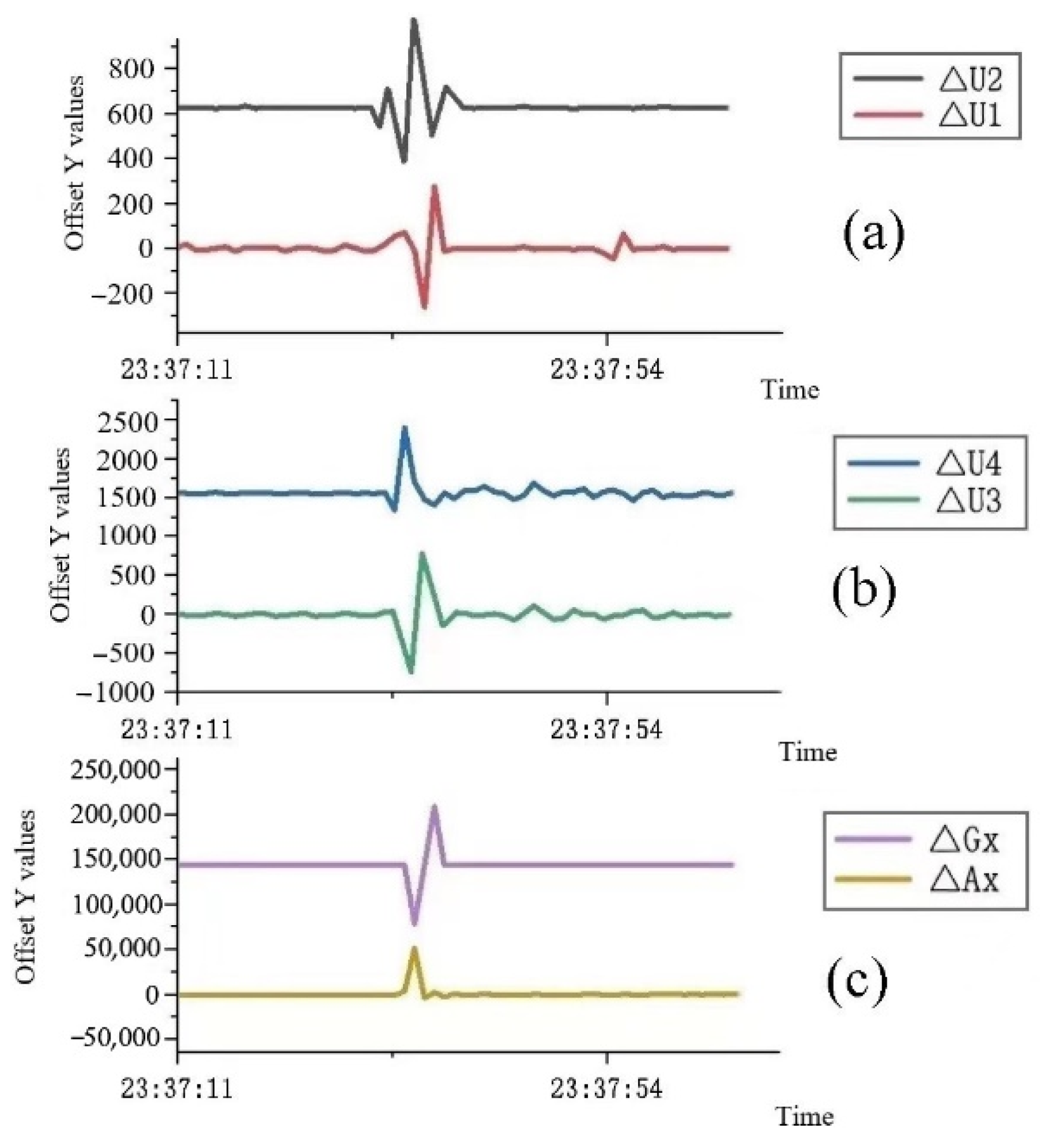
2.4. Validation of the Reliability Results of the Flexible Wearable Sleeping-Position Monitoring Device
3. Experimental Study on the Effect of Sleeping-Position Change on Sleep
3.1. Sleep Effects of Changes in Sleeping Position
3.2. Experimental Design for Sleep Effects of Changes in Sleeping Position
3.3. Experimental Procedure for the Effect of Changes in Sleeping Position on Sleep
3.4. Objective and Subjective Sleep-Quality Measures
3.5. Statistical Analysis of Experimental Data on the Effect of Changes in Sleeping Position on Sleep
3.6. Experimental Results on the Effect of Changes in Sleeping Position on Sleep
4. Discussion
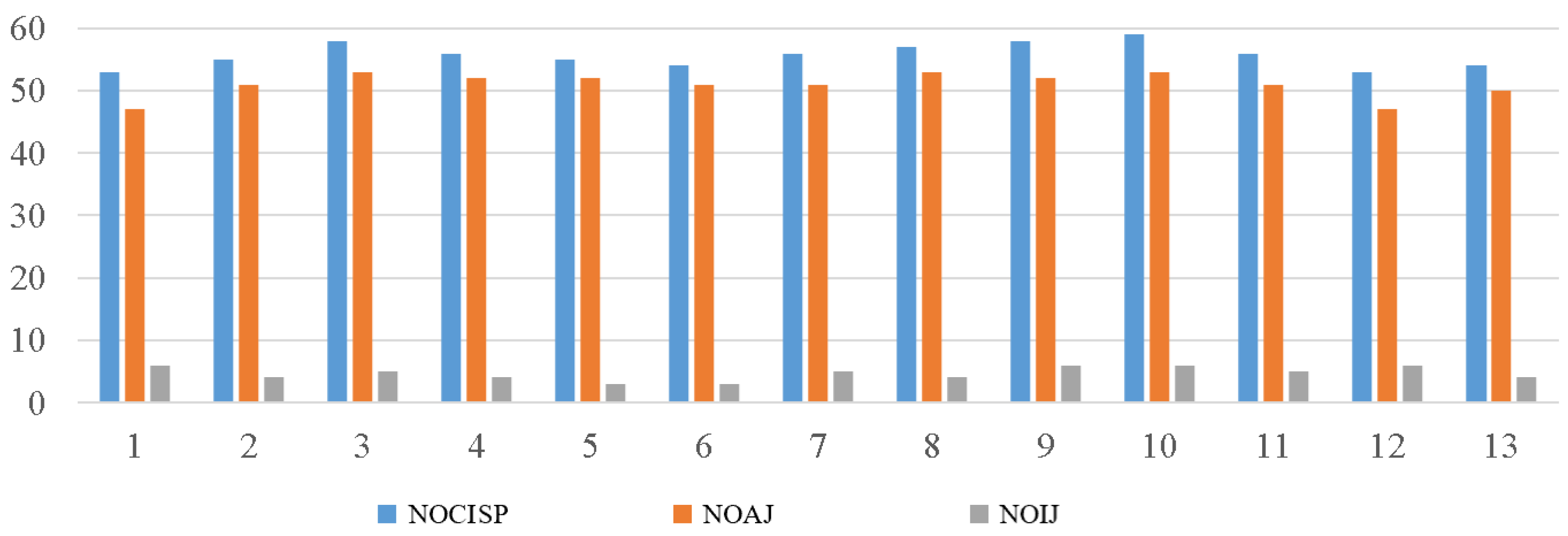
- The average number of posture changes of the 13 subjects in the reliability experiment of the flexible wearable sleeping-position monitoring device was 55.69 ± 1.93, the number of correct judgments was 51.00 ± 2.00, and the number of incorrect judgments was 4.69 ± 1.11; thus, the accuracy rate was 91.58% ± 1.98%. During the sleep experiment, the experiment validated the accuracy and reliability of the data measured by the flexible wearable sleeping-position monitoring device.
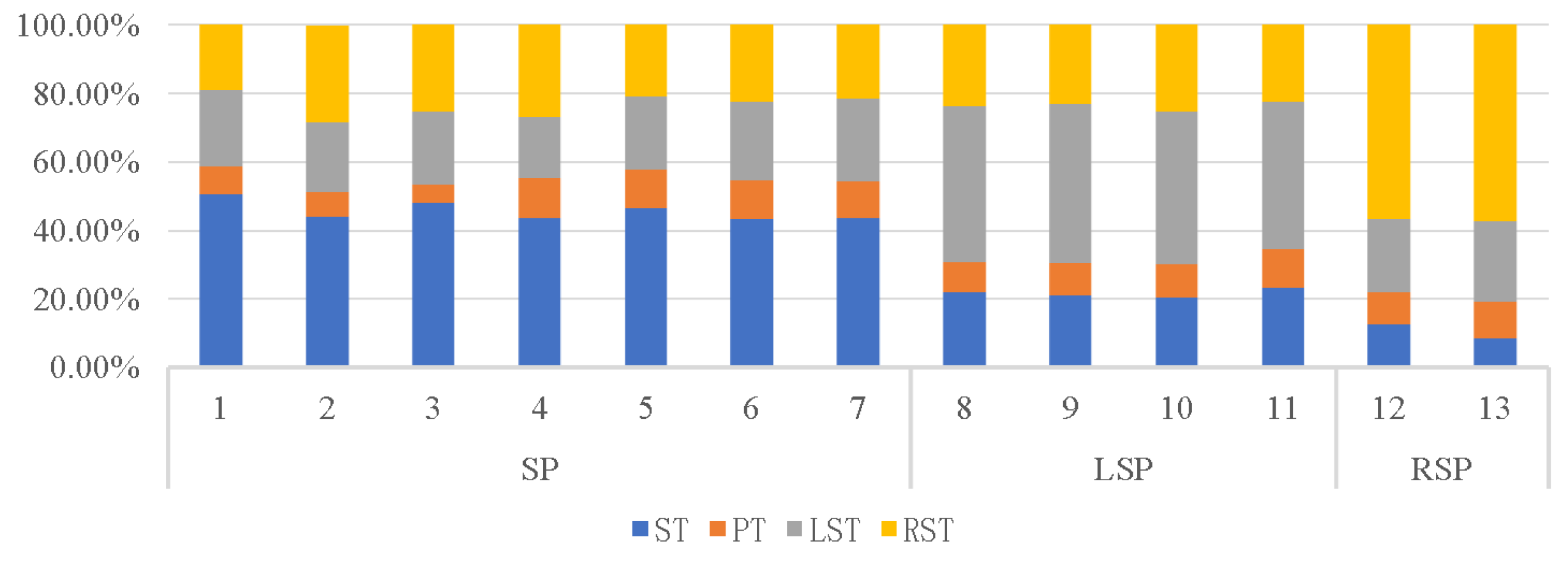
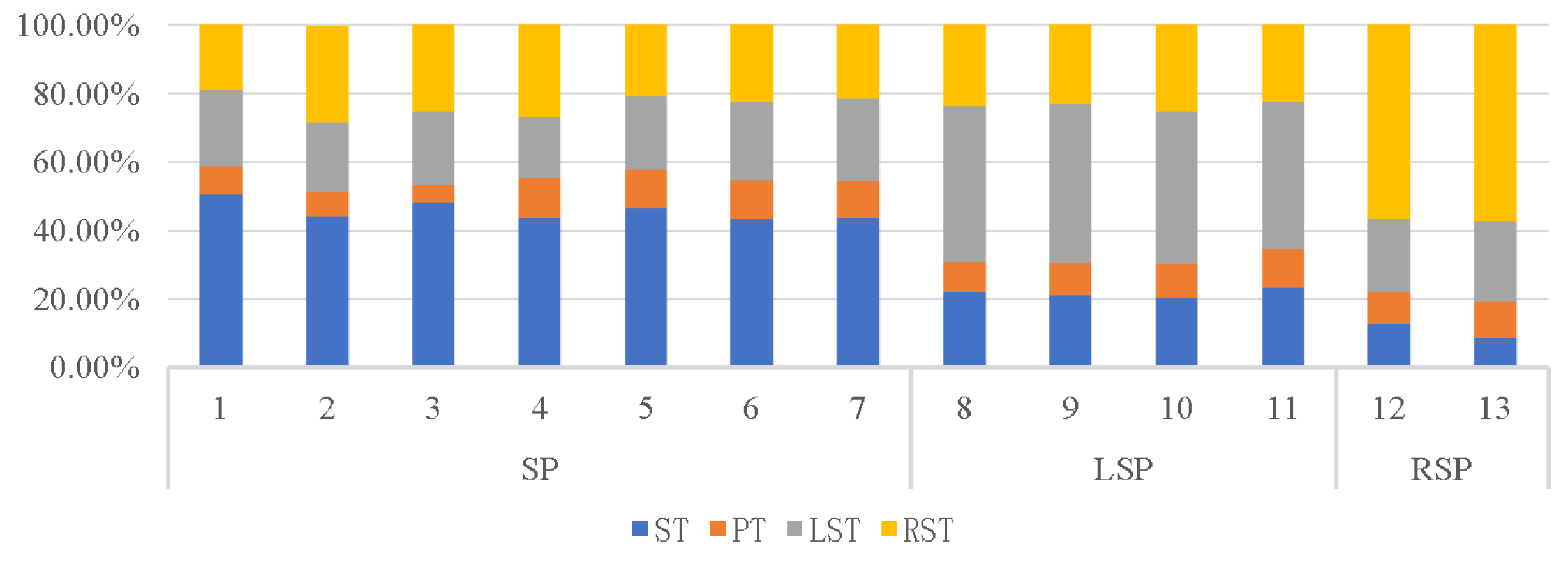
- Analysis of data on sleeping-position preferences showed that the supine position was preferred by more than half of the subjects, followed by the left lateral position and finally the right lateral position, with a lack of subjects in the prone position due to the small number of subjects. According to the proportion of time spent in each of the four positions, the biggest difference between subjects who prefer the three different decumbent positions was that they spent about half of their night in their preferred position and about 10% of their time in the prone position.
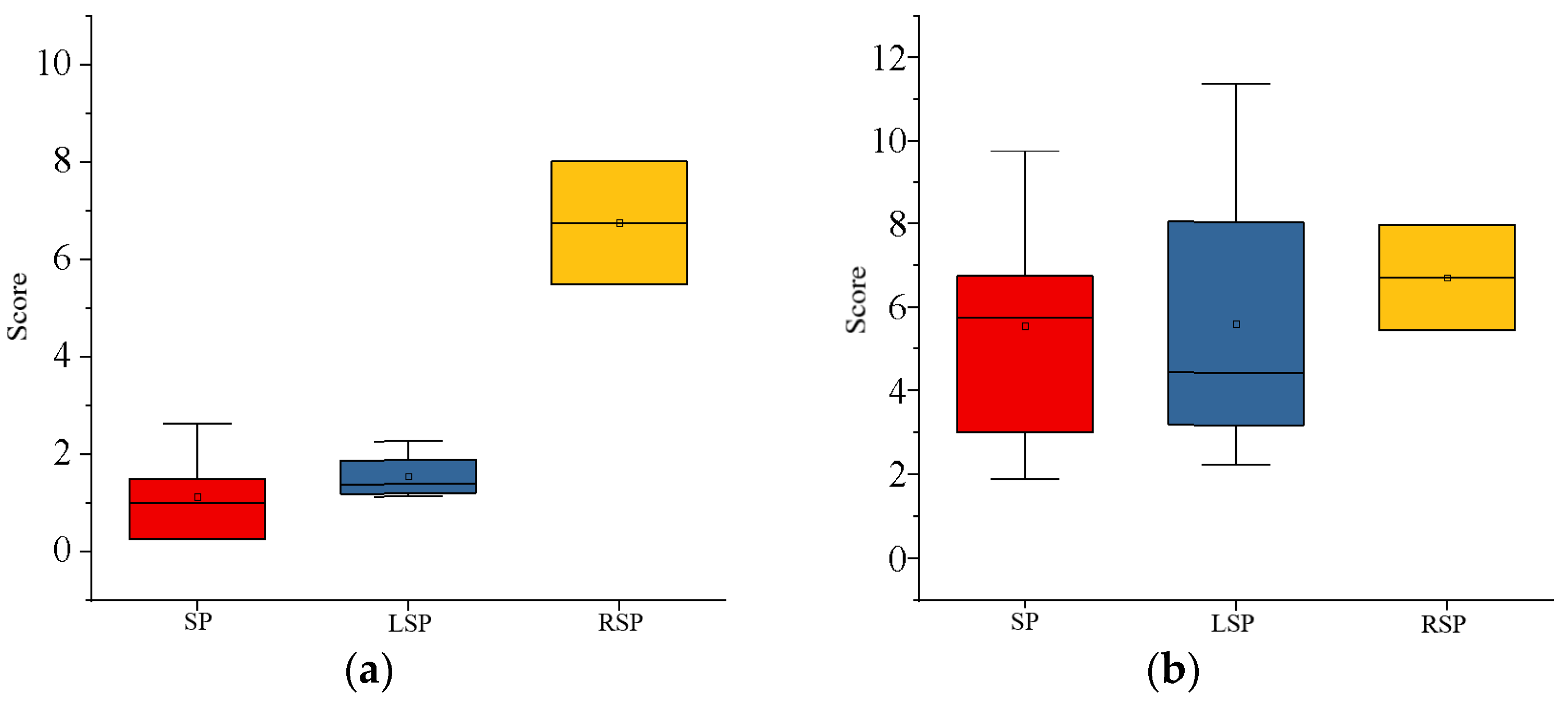
- Analysis of the subjective sleep-quality data revealed that sleep-position preference influenced sleep quality, with subjects in the right lateral position having the best sleep quality and those in the left lateral position having slightly higher sleep quality than those in the supine position. Subjective sleep quality was reflected in the results of the Karolinska Sleepiness Scale and the Mood Scale. Each day of the experiment, these scales were completed the night before and the morning after. Subjects who preferred to sleep on their right side scored significantly lower in the early morning of the second day than they did the night before, implying that subjects who spent most of their time sleeping on their right side recovered better after a night of rest and adjustment.
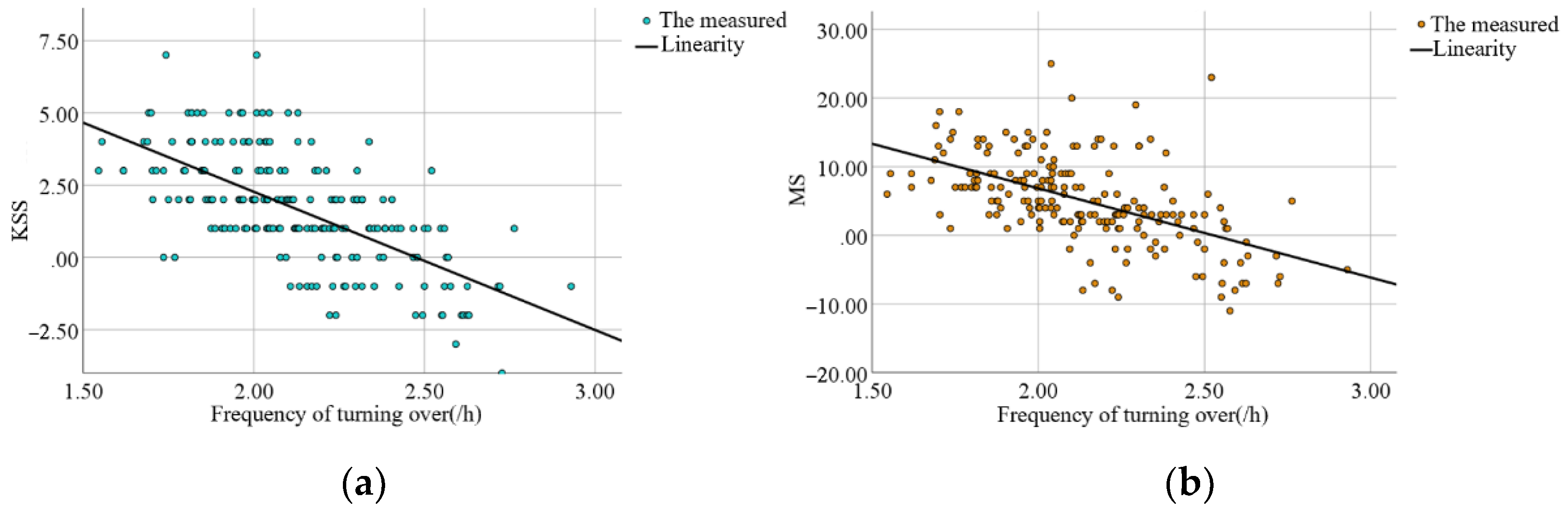
- The effect of turning frequency on subjective sleep quality showed that subjects would turn over more frequently when their sleep quality was poor. When subjects were deeply asleep, they would turn less frequently, and when they first went to bed, they would turn over frequently to find a suitable position to fall asleep, but the preferred position was not always the one in which they fell asleep. Individual variation in turning frequency precludes fitting a mathematical equation. The frequency of turning in subjects ranged from 1.86/h to 2.40/h, and subjects could turn over dozens of times in a single night’s sleep, indicating that each individual does not stay in the same position for long periods during sleep.
- Analysis of the objective sleep data revealed that sleeping-position preference and frequency of turning interacted with sleep parameters such as multiple awakenings and the rapid eye movement period. For starters, subjects with a right-sided preference had fewer awakenings and shorter awakening times than those with other sleeping-position preferences. On the other hand, subjects with a supine preference had a slightly higher number of awakenings than subjects with a left lateral preference, with the lower awakening time being a higher number of awakenings but a shorter duration of the awakenings. In subjects who preferred to sleep supine, the increased number of awakenings may have resulted in a lower subjective sleep-quality rating. Second, subjects who preferred the right lateral position had the longest duration of slow-wave sleep and a significantly shorter duration of rapid eye movement, indicating a lower proclivity to wake up during the night.
5. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bo, C.; Deyu, W.; Xuwei, Z.; Chunping, L.; Guangwu, W. Lantu, Turn-over bed design for medical use. Mach. Des. Res. 2007, 34, 20–22. [Google Scholar]
- Dawson, D.; Reid, K.J. Fatigue, alcohol and performance impairment. Nature 1997, 388, 235. [Google Scholar] [CrossRef] [PubMed]
- Verhaert, V.; Haex, B.; De Wilde, T.D.; Berckmans, D.; Verbraecken, J.; Valck, E.D.; Sloten, J.V. Ergonomics in bed design: The effect of spinal alignment on sleep parameters. Ergonomics 2011, 54, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Lahm, R.; Iaizzo, P.A. Physiologic responses during rest on a sleep system at varied degrees of firmness in a normal population. Ergonomics 2002, 45, 798–815. [Google Scholar] [CrossRef]
- Chang, S.; Huijun, W.; Bing, Z. Sleep status of adult residents aged 18–64 in 15 provinces (autonomous regions and municipalities directly under the central government) in China in 2015. Health Res. 2020, 49, 4. [Google Scholar]
- Buysse, D.J.; Grunstein, R.; Horne, J.; Lavie, P. Can an improvement in sleep positively impact on health? Sleep Med. Rev. 2010, 14, 405–410. [Google Scholar] [CrossRef]
- Bertisch, S.M.; Pollock, B.D.; Mittleman, M.A.; Buysse, D.J.; Bazzano, L.A.; Gottlieb, D.J.; Redline, S. Insomnia with Objective Short Sleep Duration and Risk of Incident Cardiovascular Disease and All-Cause Mortality: Sleep Heart Health Study. Sleep 2018, 41, zsy047. [Google Scholar] [CrossRef]
- Jacobson, B.H.; Boolani, A.; Dunklee, G.; Shepardson, A.; Acharya, H. Effect of prescribed sleep surfaces on back pain and sleep quality in patients diagnosed with low back and shoulder pain. Appl. Ergon. 2010, 42, 91–97. [Google Scholar] [CrossRef]
- DeVocht, J.W.; Wilder, D.G.; Bandstra, E.R.; Spratt, K.F. Biomechanical evaluation of four different mattresses. Appl. Ergon. 2006, 37, 297–304. [Google Scholar] [CrossRef]
- Jacobson, B.H.; Wallace, T.; Gemmell, H. Subjective rating of perceived back pain, stiffness and sleep quality following introduction of medium-firm bedding systems. J. Chiropr. Med. 2006, 5, 128–134. [Google Scholar] [CrossRef]
- Kovacs, F.M.; Abraira, V.; Peña, A.; Martín-Rodríguez, J.G.; Sánchez-Vera, M.; Ferrer, E.; Ruano, D.; Guillén, P.; Gestoso, M.; Muriel, A.; et al. Effect of firmness of mattress on chronic non-specific low-back pain: Randomised, double-blind, controlled, multicentre trial. Lancet 2003, 362, 1599–1604. [Google Scholar] [CrossRef]
- Verhaert, V.; van Deun, D.; Verbraecken, J.; Vandekerckhove, M.; Exadaktylos, V.; Haex, B.; Sloten, J.V. Smart control of spinal alignment through active adjustment of mechanical bed properties during sleep. J. Ambient Intell. Smart Environ. 2013, 5, 369–380. [Google Scholar] [CrossRef]
- Nachemson, A. Intravital dynamic pressure measurements in lumbar discs: A study of common movements, maneuvers and exercises. Scand. J. Rehabil. Med. 1970, 1, 1–40. [Google Scholar]
- Li, J.-Q.; Kwong, W.-H.; Chan, Y.-L.; Kawabata, M. Comparison of In Vivo Intradiscal Pressure between Sitting and Standing in Human Lumbar Spine: A Systematic Review and Meta-Analysis. Life 2022, 12, 457. [Google Scholar] [CrossRef]
- Dolan, P.; Adams, M.; Hutton, W. Commonly adopted postures and their effect on the lumbar spine. Spine 1988, 13, 197–201. [Google Scholar] [CrossRef]
- Coenen, A.M.L. De slaap en het bed: Een psychobiologische beschouwing. Med. Antropol. 2006, 18, 133–148. [Google Scholar]
- Joseph, D.K.; Dominique, L.; Pierre, G. Sleep positions and position shifts in five age groups: An ontogenetic picture. Sleep 1992, 15, 143–149. [Google Scholar]
- Deun, D.V.; Verhaert, V.; Willemen, T.; Wuyts, J.; Verbraecken, J.; Exadaktylos, V.; Haex, B.; Sloten, J.V. Biomechanics-based active control of bedding support properties and its influence on sleep. Work 2012, 41, 1274–1280. [Google Scholar] [CrossRef]
- Huo, Y.; Zhou, B.; He, H.Y.; Zhao, L.; Zhang, X.L.; Li, J.; Zuo, Y.H.; Zheng, Y.; Ren, Z.H.; Han, F.; et al. Comparison and correlation analysis of sleep parameters between watch-type sleep monitor (Actiwatch) and polysomnography. Beijing Da Xue Xue Bao Yi Xue Ban 2021, 53, 942–945. [Google Scholar]
- Tal, A.; Shinar, Z.; Shaki, D.; Codish, S.; Goldbart, A. Validation of Contact-Free Sleep Monitoring Device with Comparison to Polysomnography. J. Clin. Sleep Med. 2017, 13, 517–522. [Google Scholar] [CrossRef]
- Alaferdov, A.V.; Savu, R.; Rackauskas, T.; Rackauskas, S.; Canesqui, M.; de Lara, D.; Setti, G.; Joanni, E.; de Trindade, G.; Lima, U.; et al. A wearable, highly stable, strain and bending sensor based on high aspect ratio graphite nanobelts. Nanotechnology 2016, 27, 375501. [Google Scholar] [CrossRef]
- Liu, H.; Zhao, H.; Li, S.; Hu, J.; Zheng, X.; Li, R.; Chen, Y.; Su, Y. Adhesion-Free Thin-Film-Like Curvature Sensors Integrated on Flexible and Wearable Electronics for Monitoring Bending of Joints and Various Body Gestures. Adv. Mater. Technol. 2019, 4, 1800327. [Google Scholar] [CrossRef]
- Buysse, D.J.; Iii, C.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Driller, M.W.; Dunican, I. No familiarization or ‘first-night effect’ evident when monitoring sleep using wrist actigraphy. J. Sleep Res. 2021, 30, e13246. [Google Scholar] [CrossRef] [PubMed]
- Roomkham, S.; Hittle, M.; Cheung, J.; Lovell, D.; Mignot, E.; Perrin, D. Sleep monitoring with the Apple Watch: Comparison to a clinically validated actigraph. F1000Research 2019, 8, 754. [Google Scholar] [CrossRef]
- Mollayeva, T.; Thurairajah, P.; Burton, K.; Mollayeva, S.; Shapiro, C.M.; Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: A systematic review and meta-analysis. Sleep Med. Rev. 2016, 25, 52–73. [Google Scholar] [CrossRef] [PubMed]
- Shahid, A.; Wilkinson, K.; Marcu, S.; Shapiro, C.M. Karolinska Sleepiness Scale (KSS), Stop, That and One Hundred Other Sleep Scales; Springer: Berlin/Heidelberg, Germany, 2011; pp. 209–210. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SPP | ST (%) | PT (%) | LST (%) | RST (%) |
|---|---|---|---|---|
| SP | 45.68 ± 1.04 | 9.35 ± 0.93 | 21.43 ± 0.76 | 23.54 ± 1.32 |
| LSP | 21.62 ± 0.63 | 9.86 ± 0.52 | 44.86 ± 0.71 | 23.67 ± 0.56 |
| RSP | 10.53 ± 2.00 | 10.03 ± 0.59 | 22.35 ± 1.06 | 57.08 ± 0.35 |
| SPP | SP | LSP | RSP |
|---|---|---|---|
| TIB (min) | 471.50 ± 4.94 | 472.15 ± 2.96 | 471.77 ± 7.02 |
| SOL (min) | 20.81 ± 5.05 | 19.47 ± 4.63 | 26.00 ± 0.94 |
| TST (min) | 445.20 ± 6.63 | 442.30 ± 6.68 | 441.23 ± 7.68 |
| TWT (min) | 3.69 ± 0.50 | 7.03 ± 3.43 | 4.20 ± 0.38 |
| Awakings (n) | 0.80 ± 0.46 | 0.75 ± 0.70 | 0.23 ± 0.05 |
| Awake (min) | 1.81 ± 2.11 | 3.35 ± 2.37 | 0.33 ± 0.09 |
| SWS (min) | 245.87 ± 27.93 | 231.40 ± 47.07 | 274.07 ± 5.37 |
| REM (min) | 82.59 ± 17.07 | 89.55 ± 3.61 | 70.37 ± 16.36 |
| Awake (%TIB) | 0.41 ± 0.48 | 0.75 ± 0.53 | 0.08 ± 0.02 |
| SWS (%TIB) | 55.25 ± 6.70 | 52.27 ± 10.24 | 62.15 ± 2.39 |
| REM (%TIB) | 18.52 ± 3.66 | 20.26 ± 1.10 | 15.92 ± 3.43 |
| SEI (%) | 94.43 ± 1.07 | 93.68% ± 1.34 | 93.53% ± 0.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Xiao, A.; Zheng, T.; Xiao, H.; Huang, R. The Relationship between Sleeping Position and Sleep Quality: A Flexible Sensor-Based Study. Sensors 2022, 22, 6220. https://doi.org/10.3390/s22166220
Zhang Y, Xiao A, Zheng T, Xiao H, Huang R. The Relationship between Sleeping Position and Sleep Quality: A Flexible Sensor-Based Study. Sensors. 2022; 22(16):6220. https://doi.org/10.3390/s22166220
Chicago/Turabian StyleZhang, Yuan, Aiping Xiao, Tianhao Zheng, Huafei Xiao, and Ruiyan Huang. 2022. "The Relationship between Sleeping Position and Sleep Quality: A Flexible Sensor-Based Study" Sensors 22, no. 16: 6220. https://doi.org/10.3390/s22166220
APA StyleZhang, Y., Xiao, A., Zheng, T., Xiao, H., & Huang, R. (2022). The Relationship between Sleeping Position and Sleep Quality: A Flexible Sensor-Based Study. Sensors, 22(16), 6220. https://doi.org/10.3390/s22166220