
CAFS: An Attention-Based Co-Segmentation Semi-Supervised Method for Nasopharyngeal Carcinoma Segmentation


Abstract
:1. Introduction
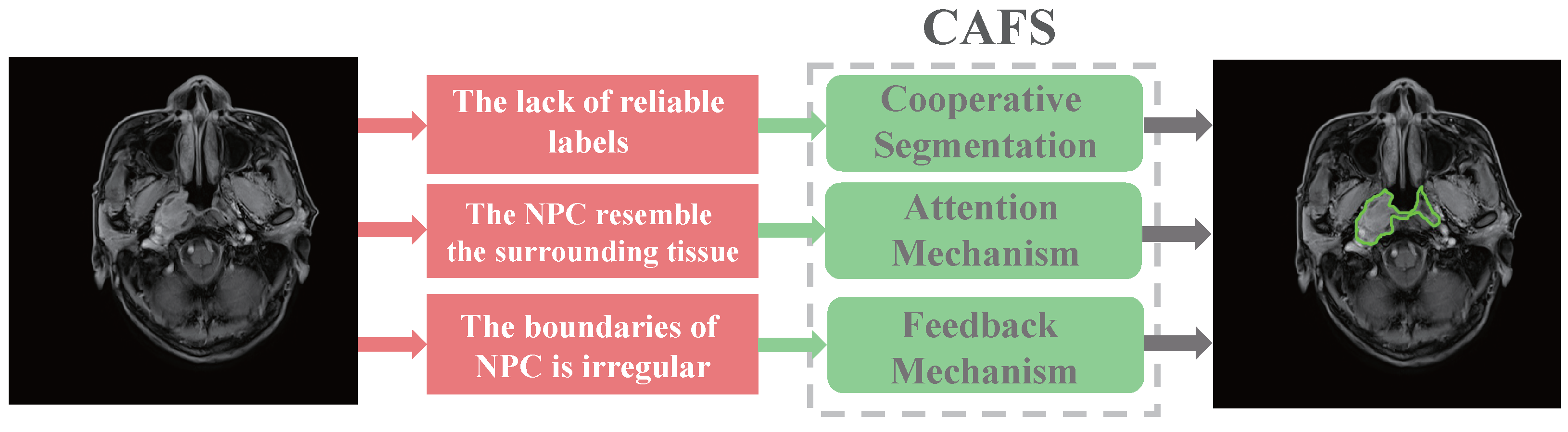
- The teacher–student cooperative segmentation mechanism allows CAFS to segment nasopharyngeal carcinoma using only a small amount of labeled data;
- The attention mechanism could prevent confusing nasopharyngeal carcinoma with surrounding tissues;
- The feedback mechanism allows CAFS to segment nasopharyngeal carcinoma more accurately.
2. Related Work
2.1. Fully-Supervised
2.2. Semi-Supervised
3. Methodology
3.1. Cooperative Segmentation
3.2. Attention Mechanism
3.3. Feedback Mechanism
4. Experiments
4.1. Data
4.2. Implementation Details
4.3. Evaluation Metrics
5. Results
5.1. Performance of CAFS
5.2. Ablation Analysis
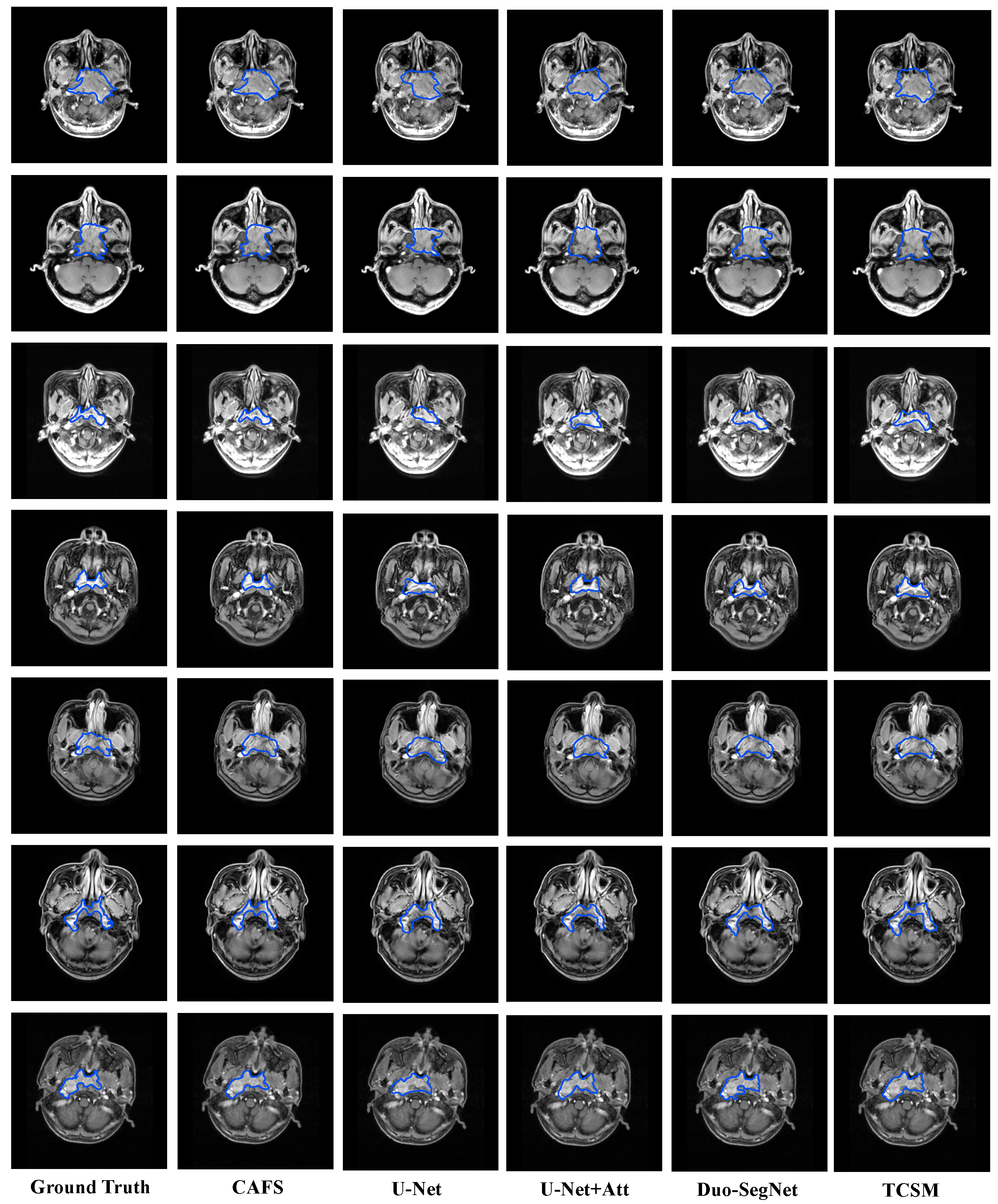
5.3. Comparison with State-of-the-Art Models
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mohammed, M.A.; Abd Ghani, M.K.; Hamed, R.I.; Ibrahim, D.A. Review on Nasopharyngeal Carcinoma: Concepts, methods of analysis, segmentation, classification, prediction and impact: A review of the research literature. J. Comput. Sci. 2017, 21, 283–298. [Google Scholar] [CrossRef]
- Chua, M.L.; Wee, J.T.; Hui, E.P.; Chan, A.T. Nasopharyngeal carcinoma. Lancet 2016, 387, 1012–1024. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.P.; Chan, A.T.; Le, Q.T.; Blanchard, P.; Sun, Y.; Ma, J. Nasopharyngeal carcinoma. Lancet 2019, 394, 64–80. [Google Scholar] [CrossRef]
- Wei, W.I.; Sham, J.S. Nasopharyngeal carcinoma. Lancet 2005, 365, 2041–2054. [Google Scholar] [CrossRef]
- Yao, J.J.; Qi, Z.Y.; Liu, Z.G.; Jiang, G.M.; Xu, X.W.; Chen, S.Y.; Zhu, F.T.; Zhang, W.J.; Lawrence, W.R.; Ma, J.; et al. Clinical features and survival outcomes between ascending and descending types of nasopharyngeal carcinoma in the intensity-modulated radiotherapy era: A big-data intelligence platform-based analysis. Radiother. Oncol. 2019, 137, 137–144. [Google Scholar] [CrossRef]
- Lee, A.; Ma, B.; Ng, W.T.; Chan, A. Management of nasopharyngeal carcinoma: Current practice and future perspective. J. Clin. Oncol. 2015, 33, 3356–3364. [Google Scholar] [CrossRef]
- Pham, D.L.; Xu, C.; Prince, J.L. Current methods in medical image segmentation. Annu. Rev. Biomed. Eng. 2000, 2, 315–337. [Google Scholar] [CrossRef] [PubMed]
- Jaffe, N.; Bruland, O.S.; Bielack, S. Pediatric and Adolescent Osteosarcoma; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2010; Volume 152. [Google Scholar]
- Pirner, S.; Tingelhoff, K.; Wagner, I.; Westphal, R.; Rilk, M.; Wahl, F.; Bootz, F.; Eichhorn, K.W. CT-based manual segmentation and evaluation of paranasal sinuses. Eur. Arch. Oto-Rhino-Laryngol. 2009, 266, 507–518. [Google Scholar] [CrossRef]
- Chiu, S.J.; Li, X.T.; Nicholas, P.; Toth, C.A.; Izatt, J.A.; Farsiu, S. Automatic segmentation of seven retinal layers in SDOCT images congruent with expert manual segmentation. Opt. Express 2010, 18, 19413–19428. [Google Scholar] [CrossRef] [Green Version]
- Ching, T.; Himmelstein, D.S.; Beaulieu-Jones, B.K.; Kalinin, A.A.; Do, B.T.; Way, G.P.; Ferrero, E.; Agapow, P.M.; Zietz, M.; Hoffman, M.M.; et al. Opportunities and obstacles for deep learning in biology and medicine. J. R. Soc. Interface 2018, 15, 20170387. [Google Scholar] [CrossRef] [Green Version]
- Gao, Z.; Chung, J.; Abdelrazek, M.; Leung, S.; Hau, W.K.; Xian, Z.; Zhang, H.; Li, S. Privileged modality distillation for vessel border detection in intracoronary imaging. IEEE Trans. Med. Imaging 2019, 39, 1524–1534. [Google Scholar] [CrossRef]
- Wu, C.; Zhang, H.; Chen, J.; Gao, Z.; Zhang, P.; Muhammad, K.; Del Ser, J. Vessel-GAN: Angiographic reconstructions from myocardial CT perfusion with explainable generative adversarial networks. Future Gener. Comput. Syst. 2022, 130, 128–139. [Google Scholar] [CrossRef]
- Gao, Z.; Wu, S.; Liu, Z.; Luo, J.; Zhang, H.; Gong, M.; Li, S. Learning the implicit strain reconstruction in ultrasound elastography using privileged information. Med. Image Anal. 2019, 58, 101534. [Google Scholar] [CrossRef]
- Zhang, M.; Zhou, Y.; Zhao, J.; Man, Y.; Liu, B.; Yao, R. A survey of semi-and weakly supervised semantic segmentation of images. Artif. Intell. Rev. 2020, 53, 4259–4288. [Google Scholar] [CrossRef]
- Guo, S.; Xu, L.; Feng, C.; Xiong, H.; Gao, Z.; Zhang, H. Multi-level semantic adaptation for few-shot segmentation on cardiac image sequences. Med. Image Anal. 2021, 73, 102170. [Google Scholar] [CrossRef]
- Chong, V.; Fan, Y.F. Detection of recurrent nasopharyngeal carcinoma: MR imaging versus CT. Radiology 1997, 202, 463–470. [Google Scholar] [CrossRef]
- Dumrongpisutikul, N.; Luangcharuthorn, K. Imaging characteristics of nasopharyngeal carcinoma for predicting distant metastasis. Clin. Radiol. 2019, 74, 818.e9–818.e15. [Google Scholar] [CrossRef]
- Huang, K.W.; Zhao, Z.Y.; Gong, Q.; Zha, J.; Chen, L.; Yang, R. Nasopharyngeal carcinoma segmentation via HMRF-EM with maximum entropy. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 2968–2972. [Google Scholar]
- Tsao, S.W.; Yip, Y.L.; Tsang, C.M.; Pang, P.S.; Lau, V.M.Y.; Zhang, G.; Lo, K.W. Etiological factors of nasopharyngeal carcinoma. Oral Oncol. 2014, 50, 330–338. [Google Scholar] [CrossRef]
- Zhu, X.J. Semi-Supervised Learning Literature Survey; University of Wisconsin-Madison: Madison, WI, USA, 2005. [Google Scholar]
- Hinton, G.; Vinyals, O.; Dean, J. Distilling the knowledge in a neural network. arXiv 2015, arXiv:1503.02531. [Google Scholar]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Tao, G.; Li, H.; Huang, J.; Han, C.; Chen, J.; Ruan, G.; Huang, W.; Hu, Y.; Dan, T.; Zhang, B.; et al. SeqSeg: A sequential method to achieve nasopharyngeal carcinoma segmentation free from background dominance. Med. Image Anal. 2022, 78, 102381. [Google Scholar] [CrossRef]
- Li, X.; Tang, M.; Guo, F.; Li, Y.; Cao, K.; Song, Q.; Wu, X.; Sun, S.; Zhou, J. DDNet: 3D densely connected convolutional networks with feature pyramids for nasopharyngeal carcinoma segmentation. IET Image Process. 2022, 16, 39–48. [Google Scholar] [CrossRef]
- Li, Y.; Dan, T.; Li, H.; Chen, J.; Peng, H.; Liu, L.; Cai, H. NPCNet: Jointly Segment Primary Nasopharyngeal Carcinoma Tumors and Metastatic Lymph Nodes in MR Images. IEEE Trans. Med. Imaging 2022, 41, 1639–1650. [Google Scholar] [CrossRef]
- Meng, M.; Gu, B.; Bi, L.; Song, S.; Feng, D.D.; Kim, J. DeepMTS: Deep multi-task learning for survival prediction in patients with advanced nasopharyngeal carcinoma using pretreatment PET/CT. IEEE J. Biomed. Health Inform. 2022, 1–10. [Google Scholar] [CrossRef]
- Shen, D.; Wu, G.; Suk, H.I. Deep learning in medical image analysis. Annu. Rev. Biomed. Eng. 2017, 19, 221–248. [Google Scholar] [CrossRef] [Green Version]
- Razzak, M.I.; Naz, S.; Zaib, A. Deep learning for medical image processing: Overview, challenges and the future. Classif. BioApps 2018, 26, 323–350. [Google Scholar]
- Gao, Z.; Wang, X.; Sun, S.; Wu, D.; Bai, J.; Yin, Y.; Liu, X.; Zhang, H.; de Albuquerque, V.H.C. Learning physical properties in complex visual scenes: An intelligent machine for perceiving blood flow dynamics from static CT angiography imaging. Neural Networks 2020, 123, 82–93. [Google Scholar] [CrossRef]
- LeCun, Y.; Boser, B.; Denker, J.; Henderson, D.; Howard, R.; Hubbard, W.; Jackel, L. Handwritten digit recognition with a back-propagation network. Adv. Neural Inf. Process. Syst. 1989, 2, 396–404. [Google Scholar]
- Gu, J.; Wang, Z.; Kuen, J.; Ma, L.; Shahroudy, A.; Shuai, B.; Liu, T.; Wang, X.; Wang, G.; Cai, J.; et al. Recent advances in convolutional neural networks. Pattern Recognit. 2018, 77, 354–377. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Han, G.; Liu, X. DCNet: Densely Connected Deep Convolutional Encoder–Decoder Network for Nasopharyngeal Carcinoma Segmentation. Sensors 2021, 21, 7877. [Google Scholar] [CrossRef]
- Pan, X.; Dai, D.; Wang, H.; Liu, X.; Bai, W. Nasopharyngeal Organ Segmentation Algorithm Based on Dilated Convolution Feature Pyramid. In Proceedings of the International Conference on Image, Vision and Intelligent Systems (ICIVIS 2021), Changsha, China, 15–17 June 2021; Springer: Berlin/Heidelberg, Germany, 2022; pp. 45–58. [Google Scholar]
- Yang, G.; Dai, Z.; Zhang, Y.; Zhu, L.; Tan, J.; Chen, Z.; Zhang, B.; Cai, C.; He, Q.; Li, F.; et al. Multiscale Local Enhancement Deep Convolutional Networks for the Automated 3D Segmentation of Gross Tumor Volumes in Nasopharyngeal Carcinoma: A Multi-Institutional Dataset Study. Front. Oncol. 2022, 12, 827991. [Google Scholar] [CrossRef]
- Guo, F.; Shi, C.; Li, X.; Wu, X.; Zhou, J.; Lv, J. Image segmentation of nasopharyngeal carcinoma using 3D CNN with long-range skip connection and multi-scale feature pyramid. Soft Comput. 2020, 24, 12671–12680. [Google Scholar] [CrossRef]
- Cheng, W.; Wan, S.; Zhaodong, F.; Zhou, Q.; Lin, Q. Automatic Gross Tumor Volume Delineation of Nasopharyngeal Carcinoma in 3D CT Images. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, e381–e382. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Lima, Peru, 4–8 October 2020; Springer: Berlin/Heidelberg, Germany, 2015; pp. 234–241. [Google Scholar]
- Zhang, J.; Gu, L.; Han, G.; Liu, X. AttR2U-Net: A Fully Automated Model for MRI Nasopharyngeal Carcinoma Segmentation Based on Spatial Attention and Residual Recurrent Convolution. Front. Oncol. 2021, 11, 816672. [Google Scholar] [CrossRef]
- Li, F.H.; Zhao, X.M. MD-Unet: A deformable network for nasal cavity and paranasal sinus tumor segmentation. Signal Image Video Process. 2022, 16, 1225–1233. [Google Scholar] [CrossRef]
- Tang, P.; Yang, P.; Nie, D.; Wu, X.; Zhou, J.; Wang, Y. Unified medical image segmentation by learning from uncertainty in an end-to-end manner. Knowl.-Based Syst. 2022, 241, 108215. [Google Scholar] [CrossRef]
- Chen, H.; Qi, Y.; Yin, Y.; Li, T.; Liu, X.; Li, X.; Gong, G.; Wang, L. MMFNet: A multi-modality MRI fusion network for segmentation of nasopharyngeal carcinoma. Neurocomputing 2020, 394, 27–40. [Google Scholar] [CrossRef] [Green Version]
- Lin, M.; Cai, Q.; Zhou, J. 3D Md-Unet: A novel model of multi-dataset collaboration for medical image segmentation. Neurocomputing 2022, 492, 530–544. [Google Scholar] [CrossRef]
- Liao, W.; He, J.; Luo, X.; Wu, M.; Shen, Y.; Li, C.; Xiao, J.; Wang, G.; Chen, N. Automatic delineation of gross tumor volume based on magnetic resonance imaging by performing a novel semi-supervised learning framework in nasopharyngeal carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2022, 113, 893–902. [Google Scholar] [CrossRef]
- Senkyire, I.B.; Liu, Z. Supervised and semi-supervised methods for abdominal organ segmentation: A review. Int. J. Autom. Comput. 2021, 18, 887–914. [Google Scholar] [CrossRef]
- Cheplygina, V.; de Bruijne, M.; Pluim, J.P. Not-so-supervised: A survey of semi-supervised, multi-instance, and transfer learning in medical image analysis. Med. Image Anal. 2019, 54, 280–296. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Chen, J.; Xie, X.; Ma, K.; Zheng, Y. Self-loop uncertainty: A novel pseudo-label for semi-supervised medical image segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Lima, Peru, 4–8 October 2020; Springer: Berlin/Heidelberg, Germany, 2020; pp. 614–623. [Google Scholar]
- Qiao, S.; Shen, W.; Zhang, Z.; Wang, B.; Yuille, A. Deep co-training for semi-supervised image recognition. In Proceedings of the European Conference on Computer Vision (ECCV), Munich, Germany, 8–14 September 2018; pp. 135–152. [Google Scholar]
- Ning, X.; Wang, X.; Xu, S.; Cai, W.; Zhang, L.; Yu, L.; Li, W. A review of research on co-training. Concurr. Comput. Pract. Exp. 2021, e6276. [Google Scholar] [CrossRef]
- Hu, L.; Li, J.; Peng, X.; Xiao, J.; Zhan, B.; Zu, C.; Wu, X.; Zhou, J.; Wang, Y. Semi-supervised NPC segmentation with uncertainty and attention guided consistency. Knowl.-Based Syst. 2022, 239, 108021. [Google Scholar] [CrossRef]
- Luo, X.; Liao, W.; Chen, J.; Song, T.; Chen, Y.; Zhang, S.; Chen, N.; Wang, G.; Zhang, S. Efficient semi-supervised gross target volume of nasopharyngeal carcinoma segmentation via uncertainty rectified pyramid consistency. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Strasbourg, France, 27 September–1 October 2021; Springer: Berlin/Heidelberg, Germany, 2021; pp. 318–329. [Google Scholar]
- Zhang, Y.; Liao, Q.; Jiao, R.; Zhang, J. Uncertainty-Guided Mutual Consistency Learning for Semi-Supervised Medical Image Segmentation. arXiv 2021, arXiv:2112.02508. [Google Scholar] [CrossRef]
- Sun, L.; Wu, J.; Ding, X.; Huang, Y.; Wang, G.; Yu, Y. A teacher–student framework for semi-supervised medical image segmentation from mixed supervision. arXiv 2020, arXiv:2010.12219. [Google Scholar]
- Mnih, V.; Heess, N.; Graves, A. Recurrent models of visual attention. In Proceedings of the 28th Annual Conference on Neural Information, Montreal, QC, Canada, 8–13 December 2014. [Google Scholar]
- Guo, M.H.; Liu, Z.N.; Mu, T.J.; Hu, S.M. Beyond self-attention: External attention using two linear layers for visual tasks. arXiv 2021, arXiv:2105.02358. [Google Scholar]
- Vaswani, A.; Shazeer, N.; Parmar, N.; Uszkoreit, J.; Jones, L.; Gomez, A.N.; Kaiser, Ł.; Polosukhin, I. Attention is all you need. In Proceedings of the 31st Conference on Neural Information Processing Systems (NIPS 2017), Long Beach, CA, USA, 4–9 December 2017. [Google Scholar]
- Park, J.; Woo, S.; Lee, J.Y.; Kweon, I.S. Bam: Bottleneck attention module. arXiv 2018, arXiv:1807.06514. [Google Scholar]
- Itti, L.; Koch, C. Computational modelling of visual attention. Nat. Rev. Neurosci. 2001, 2, 194–203. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Wang, W.; Hu, X.; Yang, J. Selective kernel networks. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Long Beach, CA, USA, 15–20 June 2019; pp. 510–519. [Google Scholar]
- Zeng, X.; Huang, R.; Zhong, Y.; Sun, D.; Han, C.; Lin, D.; Ni, D.; Wang, Y. Reciprocal Learning for Semi-supervised Segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Strasbourg, France, 27 September–1 October 2021; Springer: Berlin/Heidelberg, Germany, 2021; pp. 352–361. [Google Scholar]
- Woo, S.; Park, J.; Lee, J.Y.; Kweon, I.S. Cbam: Convolutional block attention module. In Proceedings of the European Conference on Computer Vision (ECCV), Munich, Germany, 8–14 September 2018; pp. 3–19. [Google Scholar]
- Hu, J.; Shen, L.; Sun, G. Squeeze-and-excitation networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 7132–7141. [Google Scholar]
- Wang, Q.; Wu, B.; Zhu, P.; Li, P.; Zuo, W.; Hu, Q. Supplementary material for ‘ECA-Net: Efficient channel attention for deep convolutional neural networks. In Proceedings of the 2020 IEEE/CVF Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 13–19 June 2020; pp. 13–19. [Google Scholar]
- Li, Y.; Yao, T.; Pan, Y.; Mei, T. Contextual transformer networks for visual recognition. IEEE Trans. Pattern Anal. Mach. Intell. 2022, 1. [Google Scholar] [CrossRef]
- Peiris, H.; Chen, Z.; Egan, G.; Harandi, M. Duo-SegNet: Adversarial Dual-Views for Semi-Supervised Medical Image Segmentation. In Proceedings of the International Conference on Medical Image Computing and Computer-Assisted Intervention, Strasbourg, France, 27 September–1 October 2021; Springer: Berlin/Heidelberg, Germany; pp. 428–438. [Google Scholar]
- Li, X.; Yu, L.; Chen, H.; Fu, C.W.; Xing, L.; Heng, P.A. Transformation-consistent self-ensembling model for semisupervised medical image segmentation. IEEE Trans. Neural Networks Learn. Syst. 2020, 32, 523–534. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Optimizer | Weight Decay | Learning Rate | Training Iterations | Batch Size |
|---|---|---|---|---|
| SGD | 0.0001 | 0.001 | 1500 | 8 |
| Number of Labeled Data | DSC | Jaccard | Precision | Recall |
|---|---|---|---|---|
| 500 | 0.8345 | 0.7234 | 0.8378 | 0.8469 |
| 1000 | 0.8723 | 0.7964 | 0.8849 | 0.8796 |
| 1500 | 0.8387 | 0.7207 | 0.8342 | 0.8479 |
| 2000 | 0.8420 | 0.7297 | 0.8413 | 0.8485 |
| Attention Mechanism | DSC | Jaccard | Precision | Recall |
|---|---|---|---|---|
| Ours | 0.8723 | 0.7964 | 0.8849 | 0.8796 |
| CBAM [62] | 0.8078 | 0.6303 | 0.6970 | 0.8682 |
| SEAttention [63] | 0.7986 | 0.6647 | 0.7258 | 0.8876 |
| ECAAttention [64] | 0.7924 | 0.6562 | 0.7187 | 0.8830 |
| CoTAttention [65] | 0.8200 | 0.6949 | 0.8639 | 0.7366 |
| Model | DSC | Jaccard | Precision | Recall |
|---|---|---|---|---|
| C-S + Fb + Att | 0.8723 | 0.7964 | 0.8849 | 0.8796 |
| C-S + Fb | 0.8394 | 0.7632 | 0.8425 | 0.8487 |
| C-S + Att | 0.8579 | 0.7758 | 0.8562 | 0.8478 |
| C-S | 0.8385 | 0.7467 | 0.8312 | 0.8335 |
| Without Pre-training | 0.5935 | 0.4376 | 0.4230 | 0.5226 |
| Model | DSC | Jaccard | Precision | Recall |
|---|---|---|---|---|
| CAFS | 0.8723 | 0.7964 | 0.8849 | 0.8796 |
| U-Net [39] | 0.7456 | 0.6868 | 0.6569 | 0.8822 |
| U-Net + Att | 0.8198 | 0.7011 | 0.8202 | 0.8309 |
| Duo-SegNet [66] | 0.8130 | 0.6849 | 0.7966 | 0.8307 |
| TCSM [67] | 0.7970 | 0.6987 | 0.8014 | 0.8978 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Han, G.; Lin, T.; Liu, X. CAFS: An Attention-Based Co-Segmentation Semi-Supervised Method for Nasopharyngeal Carcinoma Segmentation. Sensors 2022, 22, 5053. https://doi.org/10.3390/s22135053
Chen Y, Han G, Lin T, Liu X. CAFS: An Attention-Based Co-Segmentation Semi-Supervised Method for Nasopharyngeal Carcinoma Segmentation. Sensors. 2022; 22(13):5053. https://doi.org/10.3390/s22135053
Chicago/Turabian StyleChen, Yitong, Guanghui Han, Tianyu Lin, and Xiujian Liu. 2022. "CAFS: An Attention-Based Co-Segmentation Semi-Supervised Method for Nasopharyngeal Carcinoma Segmentation" Sensors 22, no. 13: 5053. https://doi.org/10.3390/s22135053
APA StyleChen, Y., Han, G., Lin, T., & Liu, X. (2022). CAFS: An Attention-Based Co-Segmentation Semi-Supervised Method for Nasopharyngeal Carcinoma Segmentation. Sensors, 22(13), 5053. https://doi.org/10.3390/s22135053