
Ultrasound Echogenicity as an Indicator of Muscle Fatigue during Functional Electrical Stimulation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
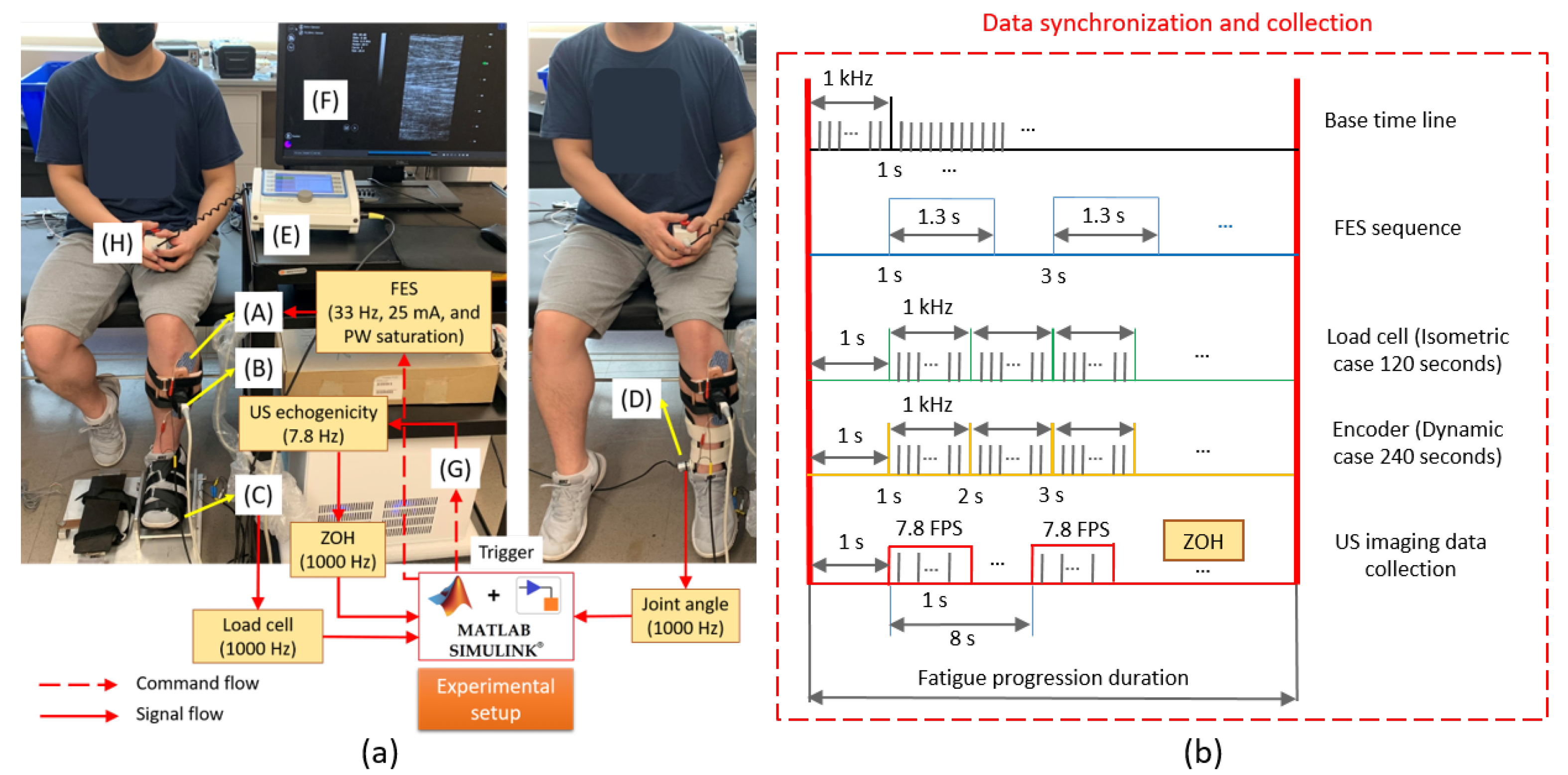
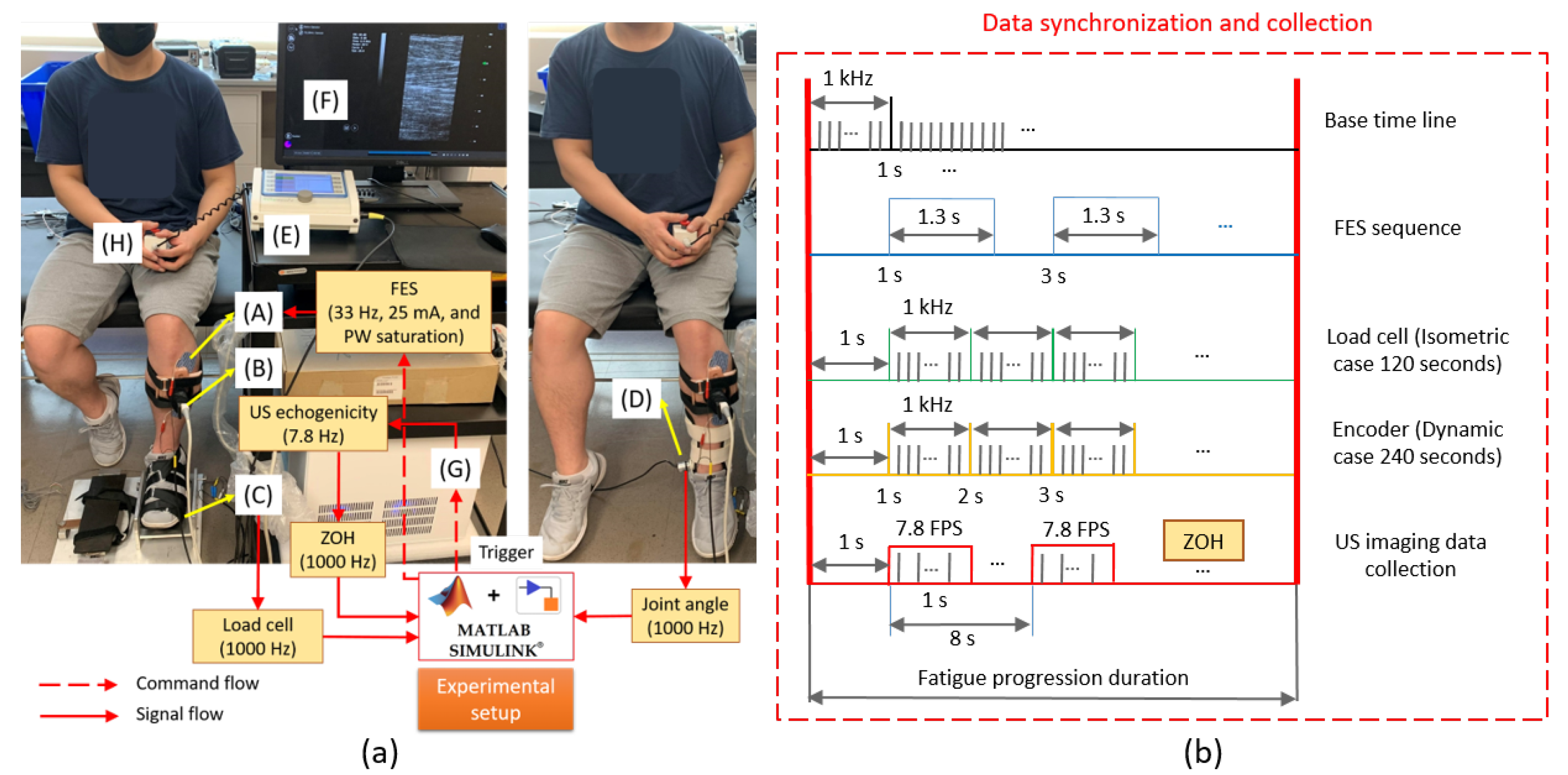
2.2. Experimental Protocol and Data Collection
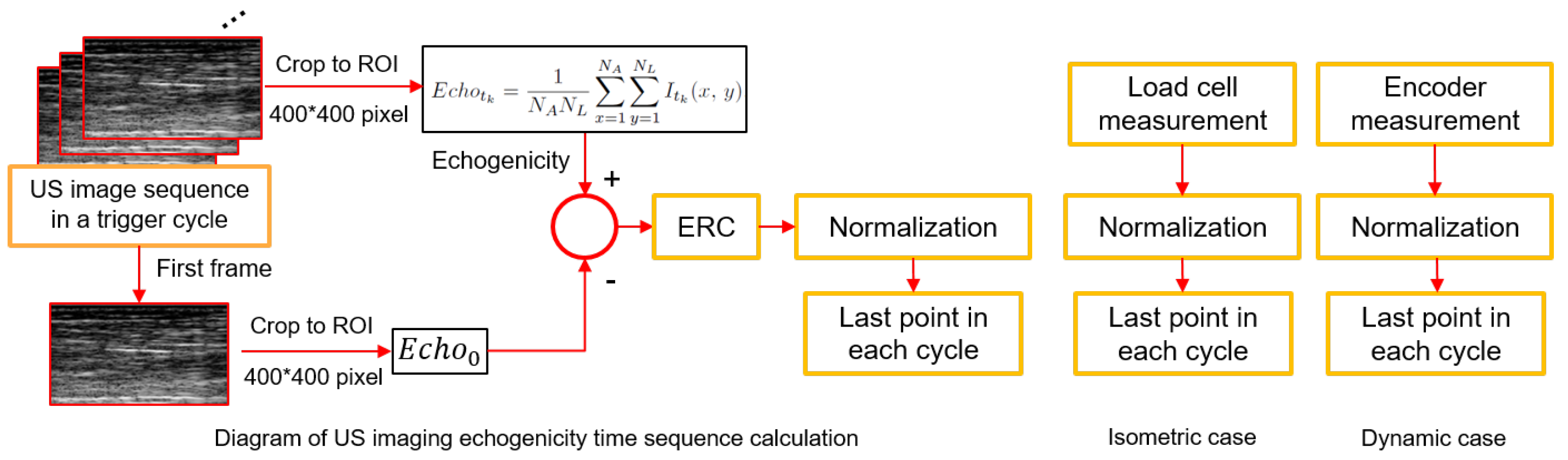
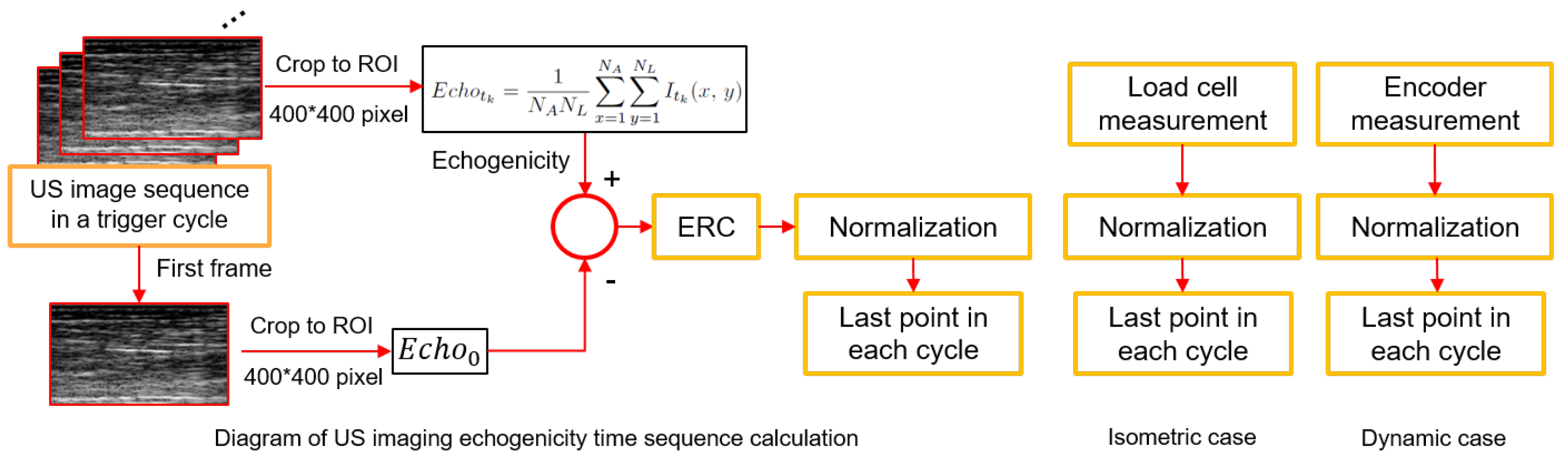
2.3. Data Processing and Analysis
2.4. Statistical Analysis
3. Results
3.1. Individual FES Pulse Width Threshold and Saturation Determination
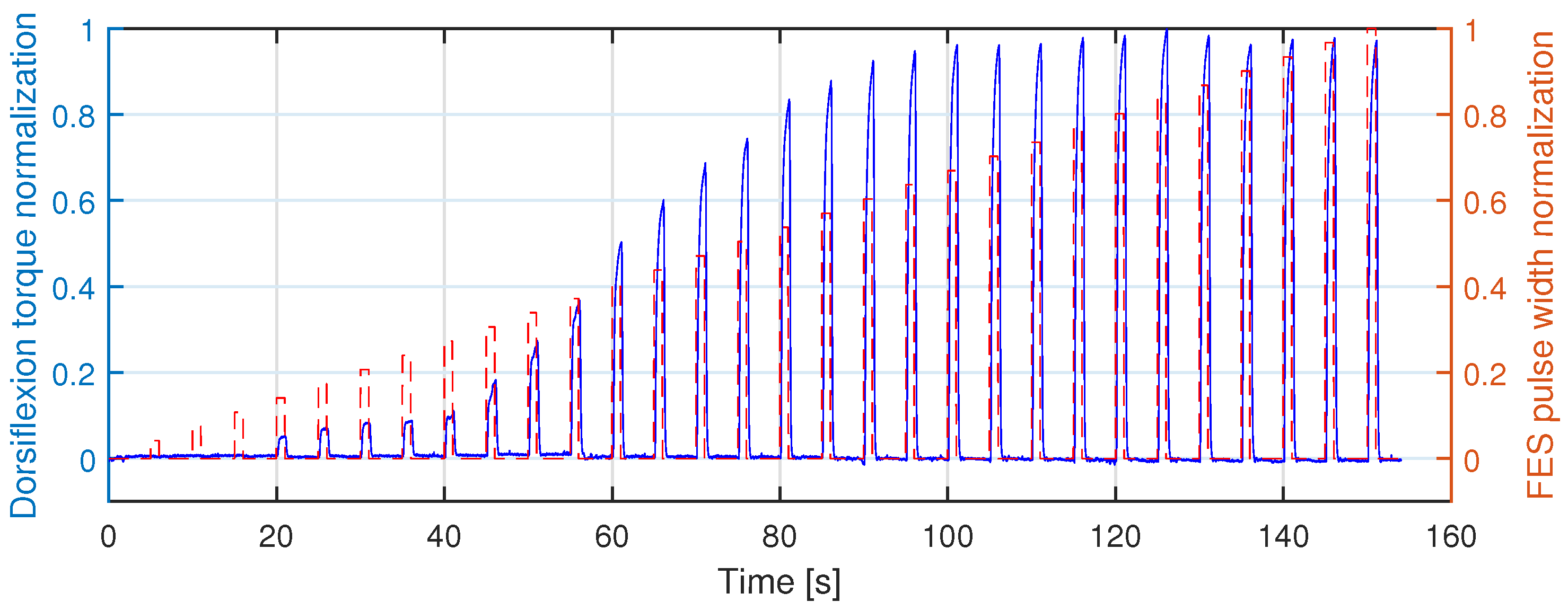
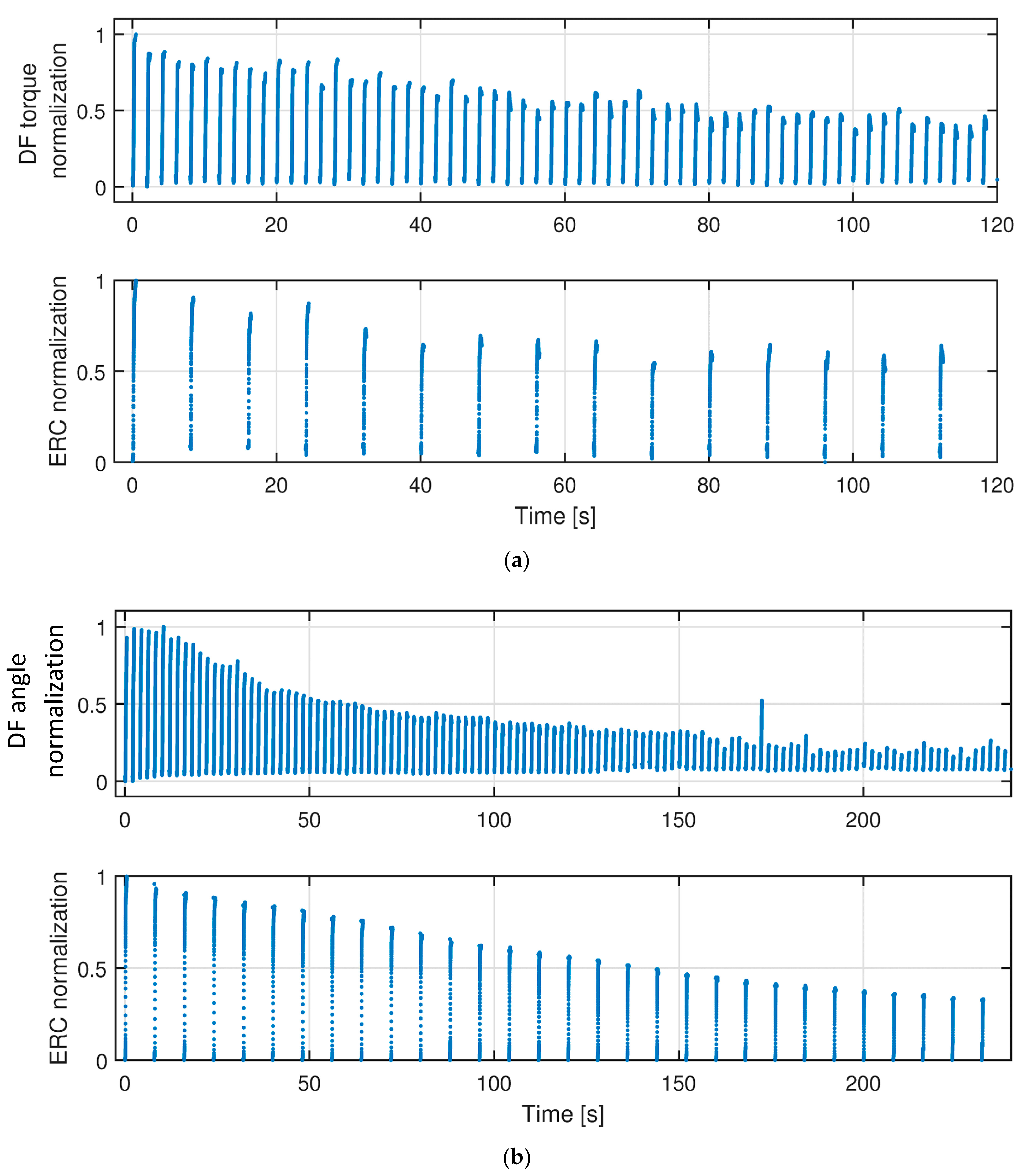
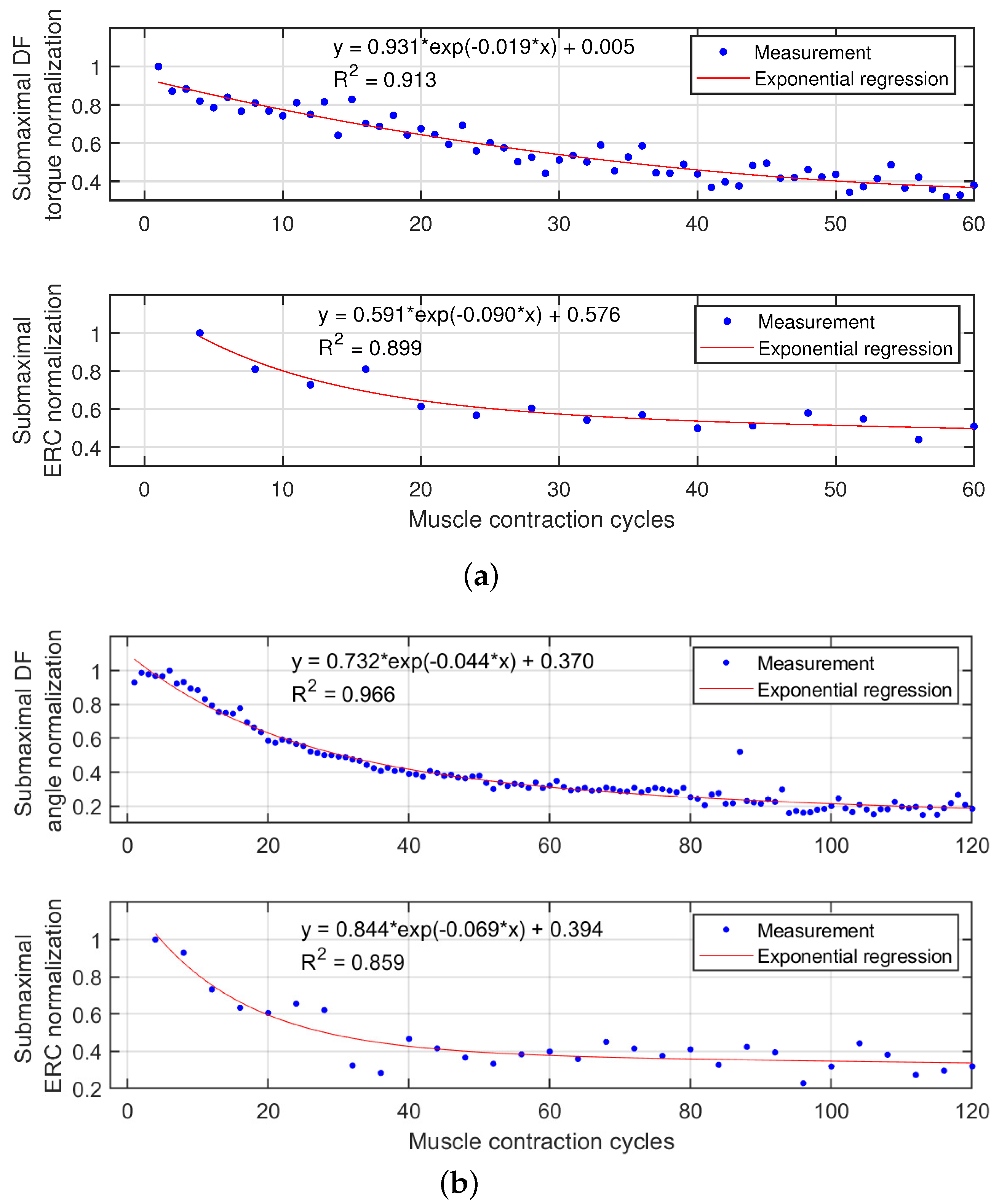
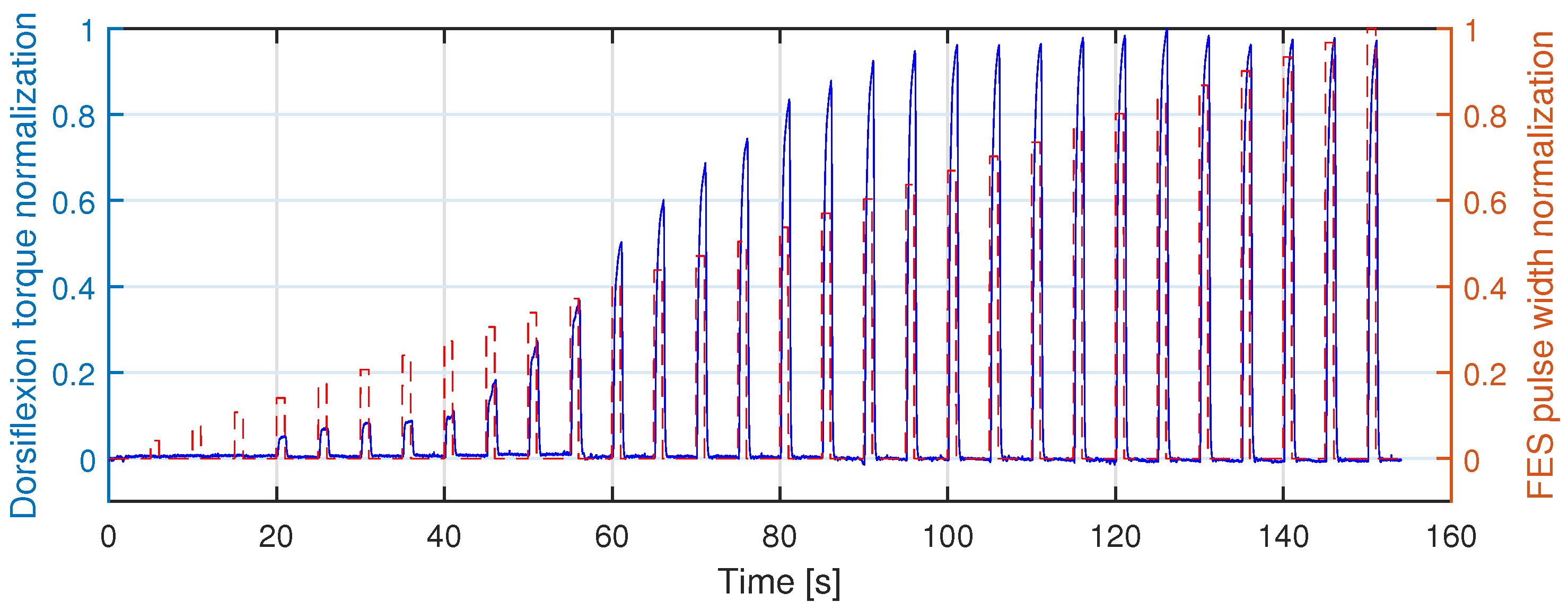
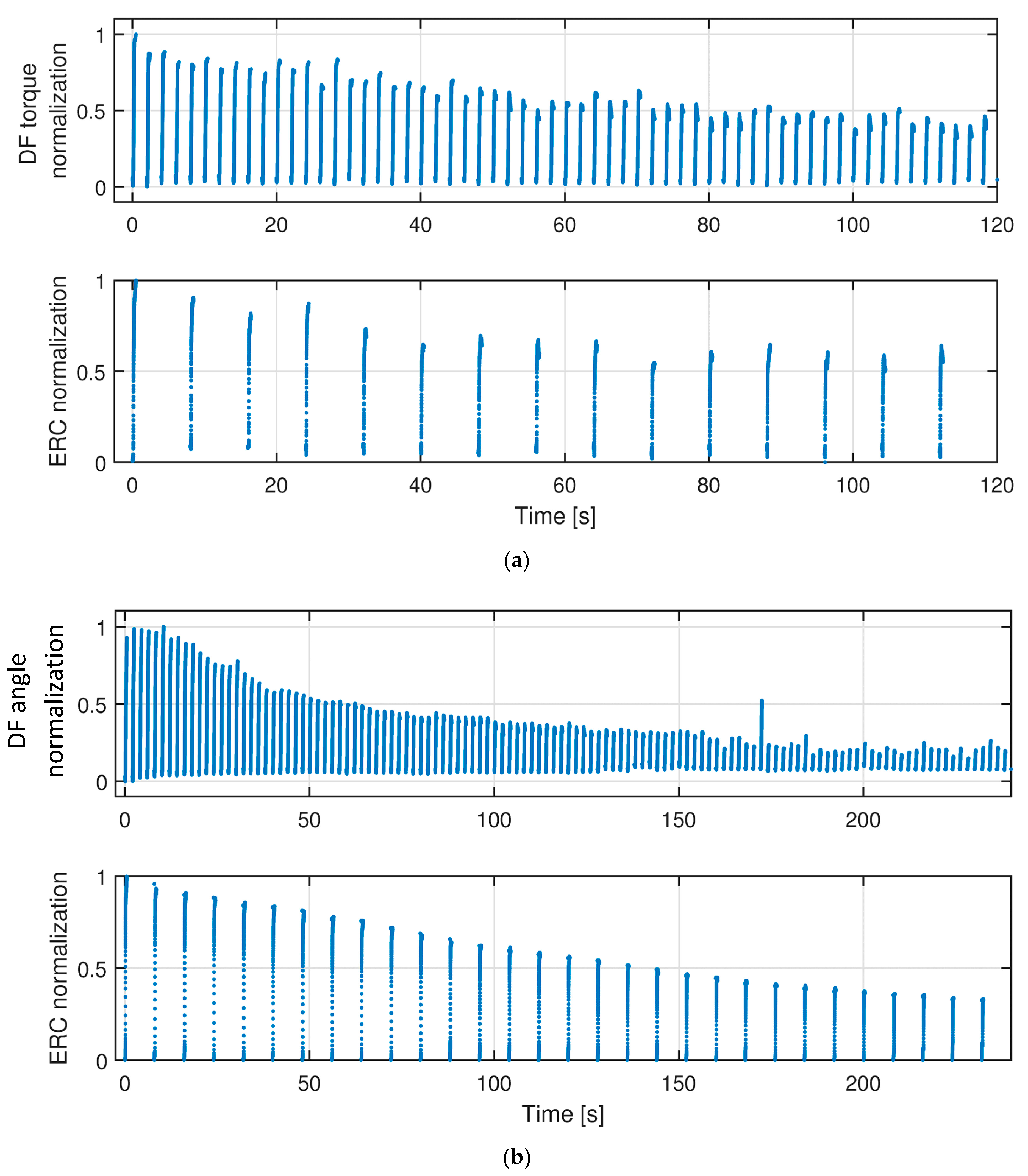
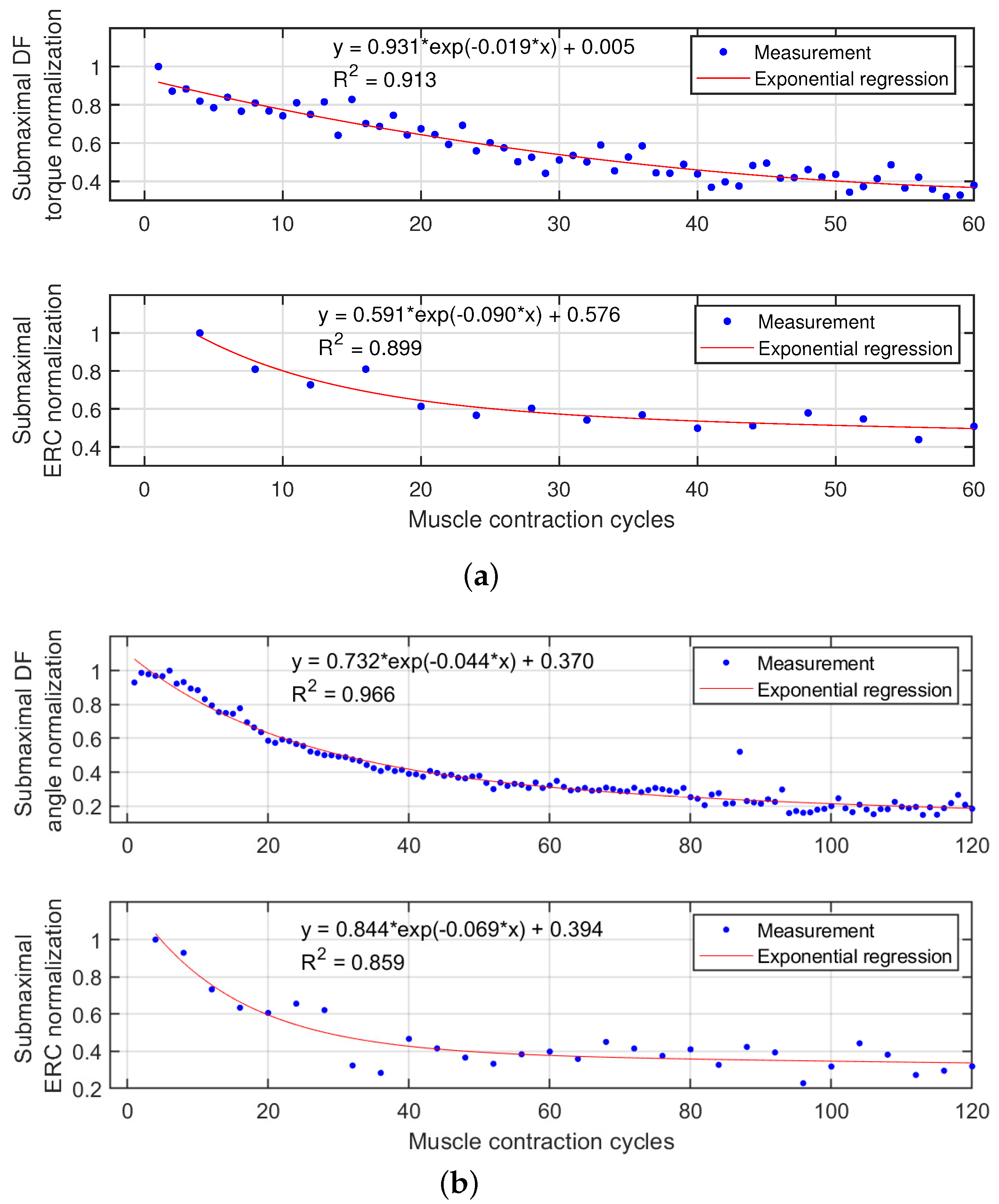
3.2. TA Muscle Fatigue Effects on Isometric and Dynamic Ankle Dorsiflexion
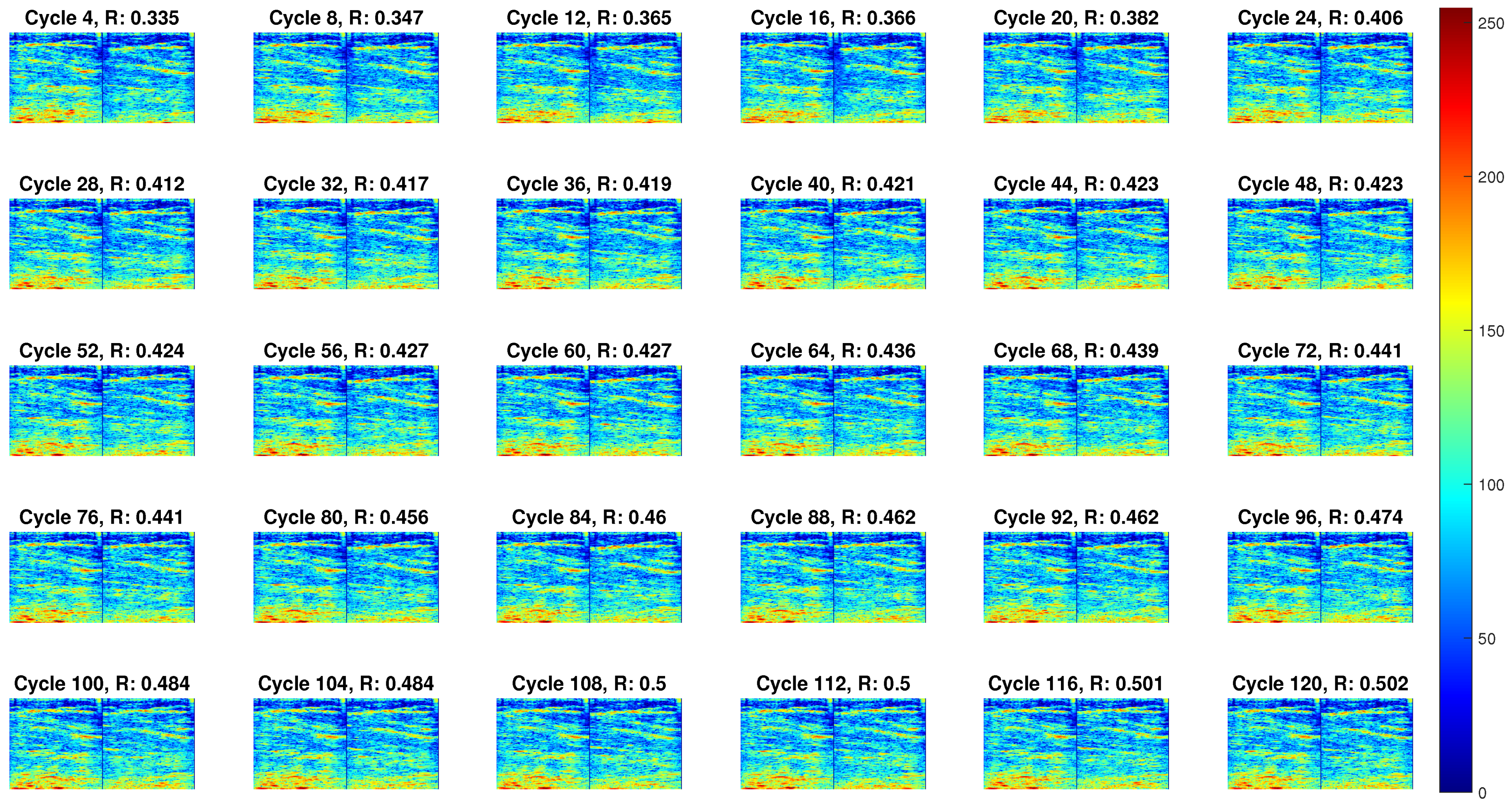
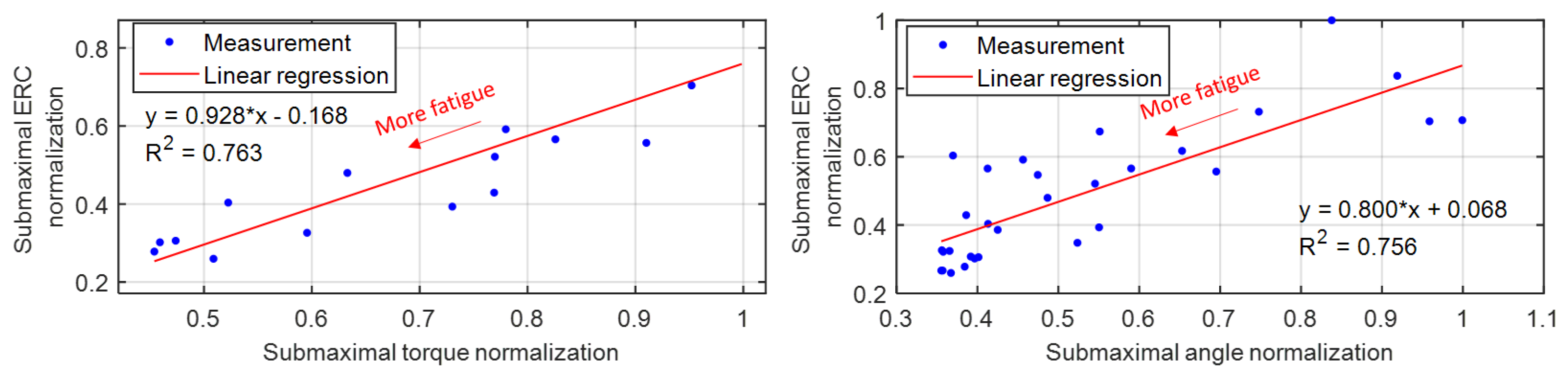
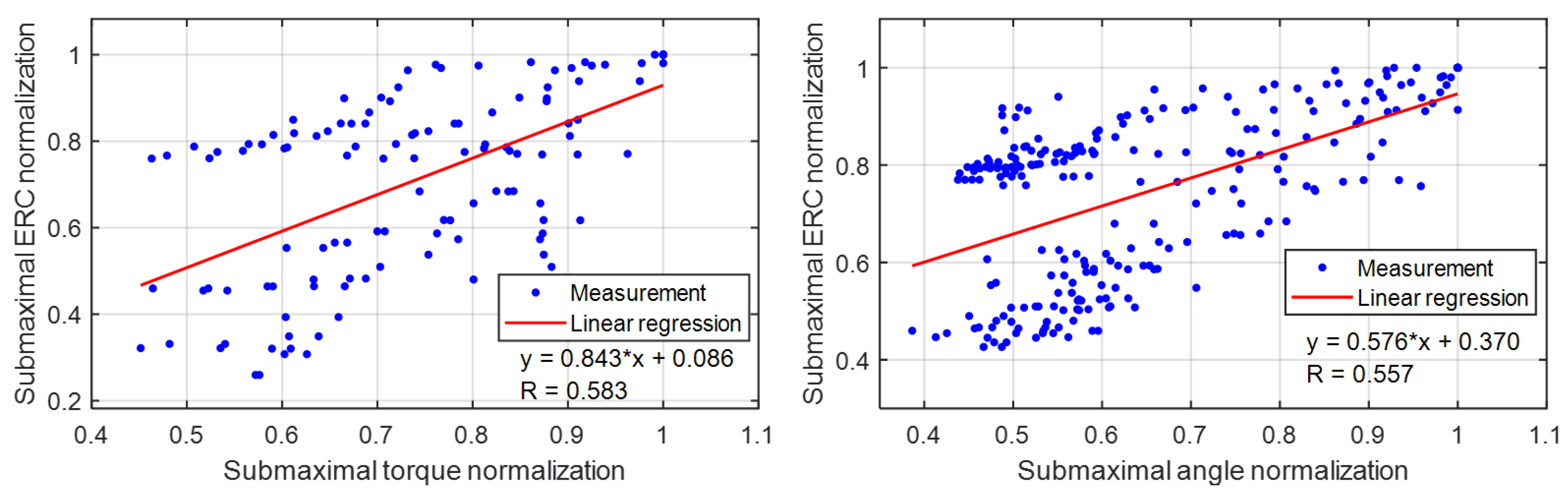
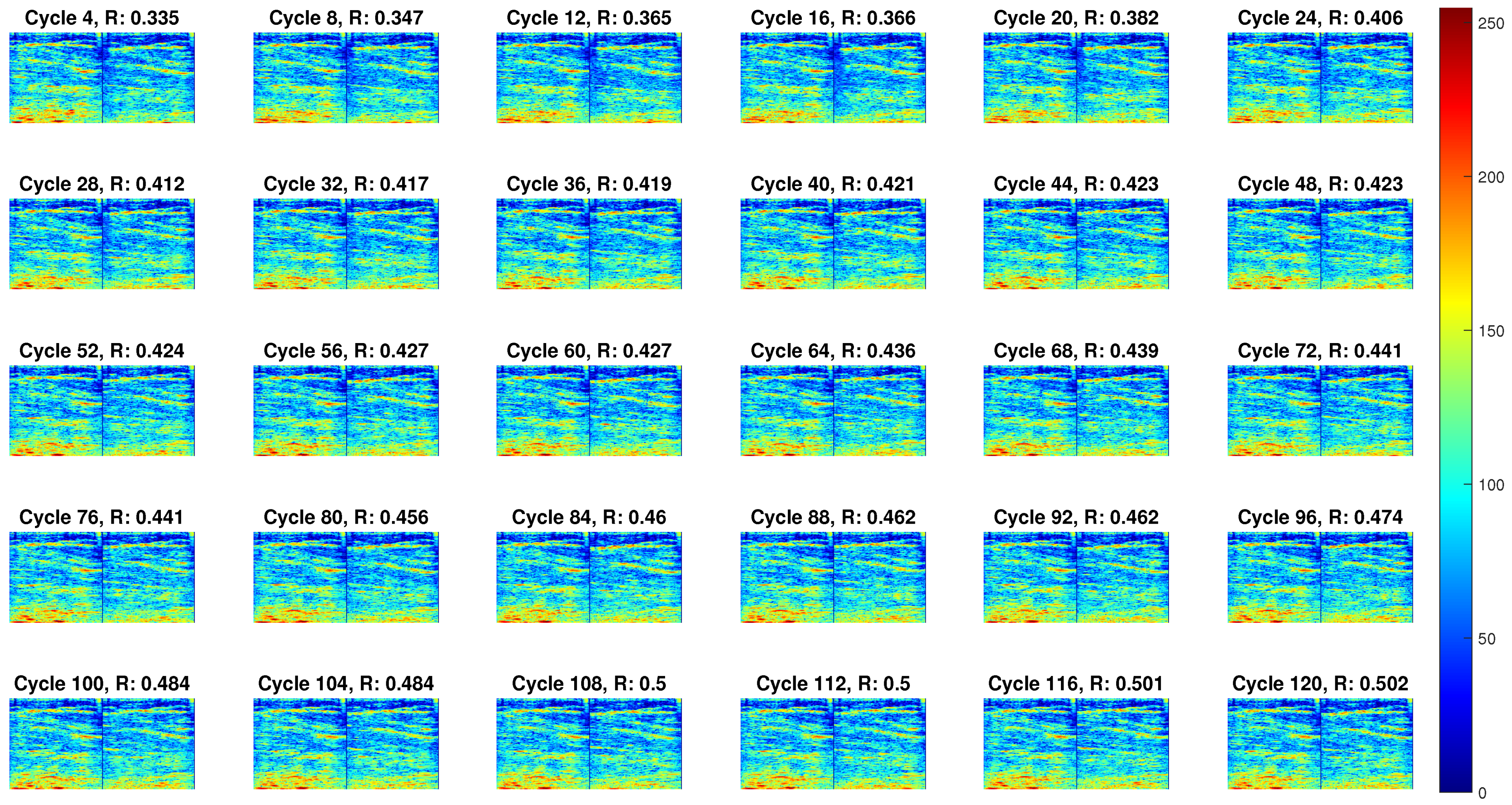
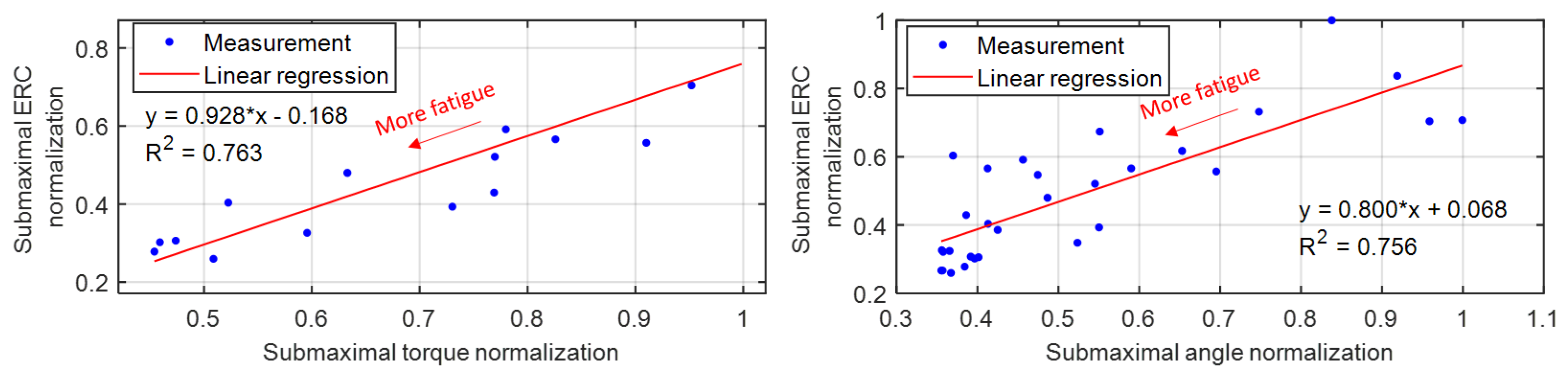
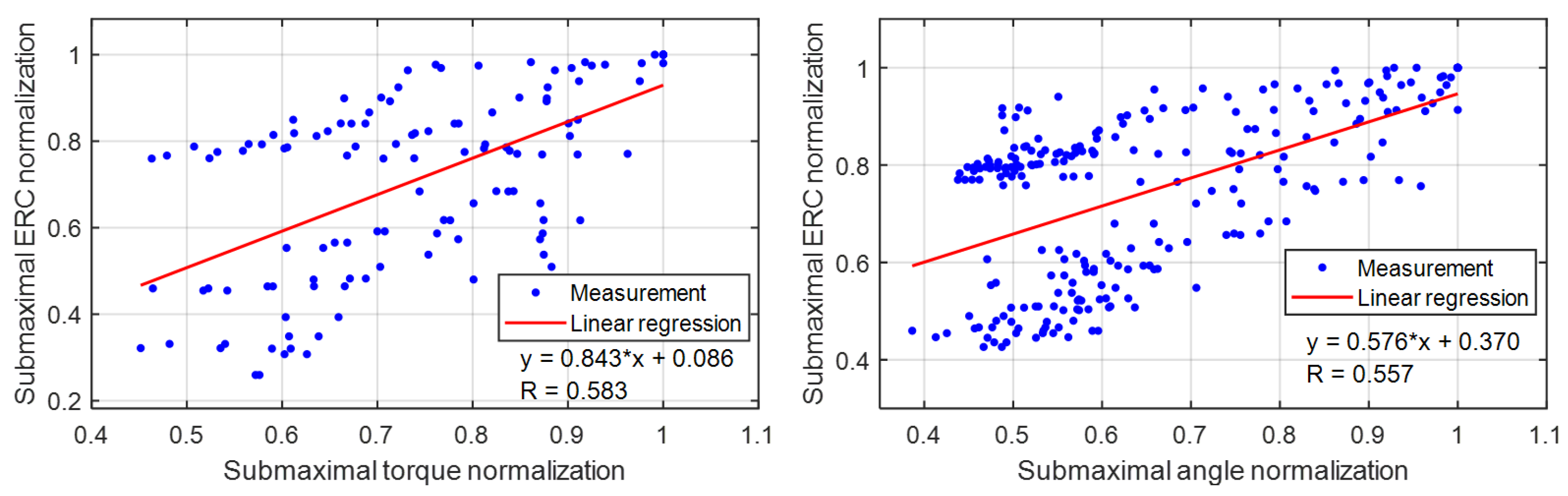
3.3. Implication of US Echogenicity as a Fatigue Indicator
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SCI | spinal cord injury |
| CNS | central nervous system |
| FES | functional electrical stimulation |
| EMG | electromyography |
| sEMG | surface electromyography |
| eEMG | evoked electromyography |
| US | ultrasound |
| TA | tibialis anteior |
| ERC | echogenicity relative change |
| IRB | institutional Review Board |
| coefficient of determination | |
| 1D | one-dimensional |
| 2D | two-dimensional |
| 3D | three-dimensional |
| ROI | region of interest |
| RF | radio frequency |
References
- Zhang, Q.; Iyer, A.; Lambeth, K.; Kim, K.; Sharma, N. Ultrasound Echogenicity-based Assessment of Muscle Fatigue During Functional Electrical Stimulation. In Proceedings of the 2021 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Mexico City, Mexico, 1–5 November 2021; pp. 5948–5952. [Google Scholar] [CrossRef]
- The National SCI Statistical Center. Spinal Cord Injury (SCI) Facts and Figures at a Glance; National Spinal Cord Injury Statistical Center: Birmingham, Alabama, 2017. [Google Scholar]
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart disease and stroke statistics—2020 update: A report from the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef]
- Iezzoni, L.I.; McCarthy, E.P.; Davis, R.B.; Siebens, H. Mobility difficulties are not only a problem of old age. J. Gen. Intern. Med. 2001, 16, 235–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantrowitz, A. Electronic physiologic aids. In Report of the Maimonides Hospital; Maimonides Hospital: Brooklyn, NY, USA, 1960; pp. 4–5. [Google Scholar]
- Liberson, W.; Holmquest, H.; Scot, D.; Dow, M. Functional electrotherapy: Stimulation of the peroneal nerve synchronized with the swing phase of the gait of hemiplegic patients. Arch. Phys. Med 1961, 42, 101–105. [Google Scholar]
- Granat, M.H.; Maxwell, D.J.; Ferguson, A.C.; Lees, K.R.; Barbenet, J.C. Peroneal stimulator: Evaluation for the correction of spastic drop foot in hemiplegia. Arch. Phys. Med. Rehabil. 1996, 77, 19–24. [Google Scholar] [CrossRef]
- Lyons, G.; Sinkjaer, T.; Burridge, J.; Wilcox, D. A review of portable FES-based neural orthoses for the correction of drop foot. IEEE Trans. Neur. Syst. Rehab. Eng. 2002, 10, 260–279. [Google Scholar] [CrossRef] [PubMed]
- Kottink, A.I.; Oostendorp, L.J.; Buurke, J.H.; Nene, A.V.; Hermens, H.J.; IJzerman, M.J. The Orthotic Effect of Functional Electrical Stimulation on the Improvement of Walking in Stroke Patients with a Dropped Foot: A Systematic Review. Artif. Organs 2004, 28, 577–586. [Google Scholar] [CrossRef]
- Everaert, D.G.; Thompson, A.K.; Chong, S.L.; Stein, R.B. Does Functional Electrical Stimulation for Foot Drop Strengthen Corticospinal Connections? Neurorehabil. Neural Repair 2010, 24, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Kluding, P.M.; Dunning, K.; O’Dell, M.W.; Wu, S.S.; Ginosian, J.; Feld, J.; McBride, K. Foot Drop Stimulation Versus Ankle Foot Orthosis After Stroke. Stroke 2013, 44, 1660–1669. [Google Scholar] [CrossRef] [Green Version]
- Melo, P.; Silva, M.; Martins, J.; Newman, D. Technical developments of functional electrical stimulation to correct drop foot: Sensing, actuation and control strategies. Clin. Biomech. 2015, 30, 101–113. [Google Scholar] [CrossRef] [Green Version]
- Sharma, N.; Kirsch, N.A.; Alibeji, N.A.; Dixon, W.E. A Non-Linear Control Method to Compensate for Muscle Fatigue during Neuromuscular Electrical Stimulation. Front. Robot. AI 2017, 4, 68. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, R.; Masani, K.; Micera, S.; Morari, M.; Popovic, M.R. Spatially distributed sequential stimulation reduces fatigue in paralyzed triceps surae muscles: A case study. Artif. Organs 2011, 35, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Sayenko, D.G.; Nguyen, R.; Hirabayashi, T.; Popovic, M.R.; Masani, K. Method to reduce muscle fatigue during transcutaneous neuromuscular electrical stimulation in major knee and ankle muscle groups. Neurorehabil. Neural Repair 2015, 29, 722–733. [Google Scholar] [CrossRef] [PubMed]
- Sayenko, D.G.; Nguyen, R.; Popovic, M.R.; Masani, K. Reducing muscle fatigue during transcutaneous neuromuscular electrical stimulation by spatially and sequentially distributing electrical stimulation sources. Eur. J. Appl. Physiol. 2014, 114, 793–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downey, R.J.; Bellman, M.J.; Kawai, H.; Gregory, C.M.; Dixon, W.E. Comparing the induced muscle fatigue between asynchronous and synchronous electrical stimulation in able-bodied and spinal cord injured populations. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 23, 964–972. [Google Scholar] [CrossRef] [PubMed]
- Downey, R.J.; Cheng, T.H.; Bellman, M.J.; Dixon, W.E. Closed-loop asynchronous neuromuscular electrical stimulation prolongs functional movements in the lower body. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 1117–1127. [Google Scholar] [CrossRef] [PubMed]
- Vøllestad, N.K. Measurement of human muscle fatigue. J. Neurosci. Methods 1997, 74, 219–227. [Google Scholar] [CrossRef]
- Sadoyama, T.; Miyano, H. Frequency analysis of surface EMG to evaluation of muscle fatigue. Eur. J. Appl. Physiol. Occup. Physiol. 1981, 47, 239–246. [Google Scholar] [CrossRef]
- Cifrek, M.; Medved, V.; Tonković, S.; Ostojić, S. Surface EMG based muscle fatigue evaluation in biomechanics. Clin. Biomech. 2009, 24, 327–340. [Google Scholar] [CrossRef]
- Rogers, D.R.; MacIsaac, D.T. EMG-based muscle fatigue assessment during dynamic contractions using principal component analysis. J. Electromyogr. Kinesiol. 2011, 21, 811–818. [Google Scholar] [CrossRef]
- Ibitoye, M.O.; Hamzaid, N.A.; Zuniga, J.M.; Wahab, A.K.A. Mechanomyography and muscle function assessment: A review of current state and prospects. Clin. Biomech. 2014, 29, 691–704. [Google Scholar] [CrossRef]
- Yoshitake, Y.; Ue, H.; Miyazaki, M.; Moritani, T. Assessment of lower-back muscle fatigue using electromyography, mechanomyography, and near-infrared spectroscopy. Eur. J. Appl. Physiol. 2001, 84, 174–179. [Google Scholar] [CrossRef]
- Praagman, M.; Veeger, H.; Chadwick, E.; Colier, W.; Van Der Helm, F. Muscle oxygen consumption, determined by NIRS, in relation to external force and EMG. J. Biomech. 2003, 36, 905–912. [Google Scholar] [CrossRef]
- Scano, A.; Pirovano, I.; Manunza, M.; Spinelli, L.; Contini, D.; Torricelli, A.; Re, R. Sustained fatigue assessment during isometric exercises with time-domain near infrared spectroscopy and surface electromyography signals. Biomed. Opt. Express 2020, 11, 7357–7375. [Google Scholar] [CrossRef]
- Dawson, M.J.; Gadian, D.; Wilkie, D. Muscular fatigue investigated by phosphorus nuclear magnetic resonance. Nature 1978, 274, 861–866. [Google Scholar] [CrossRef]
- Zhang, Q.; Hayashibe, M.; Fraisse, P.; Guiraud, D. FES-induced torque prediction with evoked EMG sensing for muscle fatigue tracking. IEEE/ASME Trans. Mechatron. 2011, 16, 816–826. [Google Scholar] [CrossRef] [Green Version]
- Ambrosini, E.; Ferrante, S.; Schauer, T.; Klauer, C.; Gaffuri, M.; Ferrigno, G.; Pedrocchi, A. A myocontrolled neuroprosthesis integrated with a passive exoskeleton to support upper limb activities. J. Electromyogr. Kinesiol. 2014, 24, 307–317. [Google Scholar] [CrossRef]
- Pilkar, R.; Yarossi, M.; Ramanujam, A.; Rajagopalan, V.; Bayram, M.B.; Mitchell, M.; Canton, S.; Forrest, G. Application of empirical mode decomposition combined with notch filtering for interpretation of surface electromyograms during functional electrical stimulation. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 25, 1268–1277. [Google Scholar] [CrossRef] [PubMed]
- Mandrile, F.; Farina, D.; Pozzo, M.; Merletti, R. Stimulation artifact in surface EMG signal: Effect of the stimulation waveform, detection system, and current amplitude using hybrid stimulation technique. IEEE Trans. Neural Syst. Rehabil. Eng. 2003, 11, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Guiraud, D.; Andreu, D.; Benoussaad, M.; Fattal, C.; Hayashibe, M. Real-time estimation of FES-induced joint torque with evoked EMG. J. Neuroeng. Rehabil. 2016, 13, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crouch, D.L.; Pan, L.; Filer, W.; Stallings, J.W.; Huang, H. Comparing Surface and Intramuscular Electromyography for Simultaneous and Proportional Control Based on a Musculoskeletal Model: A Pilot Study. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 1735–1744. [Google Scholar] [CrossRef]
- Shi, J.; Zheng, Y.P.; Chen, X.; Huang, Q.H. Assessment of muscle fatigue using sonomyography: Muscle thickness change detected from ultrasound images. Med. Eng. Phys. 2007, 29, 472–479. [Google Scholar] [CrossRef] [Green Version]
- Witte, R.S.; Kim, K.; Martin, B.J.; O’Donnell, M. Effect of fatigue on muscle elasticity in the human forearm using ultrasound strain imaging. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 4490–4493. [Google Scholar]
- Sheng, Z.; Sharma, N.; Kim, K. Quantitative Assessment of Changes in Muscle Contractility Due to Fatigue During NMES: An Ultrasound Imaging Approach. IEEE Trans. Biomed. Eng. 2019, 67, 832–841. [Google Scholar] [CrossRef]
- Sheng, Z.; Sharma, N.; Kim, K. Ultra-High-Frame-Rate Ultrasound Monitoring of Muscle Contractility Changes Due to Neuromuscular Electrical Stimulation. Ann. Biomed. Eng. 2021, 49, 262–275. [Google Scholar] [CrossRef]
- Sikdar, S.; Rangwala, H.; Eastlake, E.B.; Hunt, I.A.; Nelson, A.J.; Devanathan, J.; Shin, A.; Pancrazio, J.J. Novel method for predicting dexterous individual finger movements by imaging muscle activity using a wearable ultrasonic system. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 22, 69–76. [Google Scholar] [CrossRef]
- Zhang, Q.; Iyer, A.; Kim, K.; Sharma, N. Evaluation of Non-invasive Ankle Joint Effort Prediction Methods for Use in Neurorehabilitation Using Electromyography and Ultrasound Imaging. IEEE Trans. Biomed. Eng. 2021, 68, 1044–1055. [Google Scholar] [CrossRef]
- Zhang, Q.; Kim, K.; Sharma, N. Prediction of Ankle Dorsiflexion Moment by Combined Ultrasound Sonography and Electromyography. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 318–327. [Google Scholar] [CrossRef]
- Kirsch, N.; Alibeji, N.; Sharma, N. Nonlinear model predictive control of functional electrical stimulation. Control Eng. Pract. 2017, 58, 319–331. [Google Scholar] [CrossRef] [Green Version]
- Seynnes, O.R.; Cronin, N.J. Simple Muscle Architecture Analysis (SMA): An ImageJ macro tool to automate measurements in B-mode ultrasound scans. PLoS ONE 2020, 15, e0229034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gavin, H.P. The Levenberg–Marquardt Algorithm for Nonlinear Least Squares Curve-Fitting Problems; Department of Civil and Environmental Engineering, Duke University: Durham, NC, USA, 2019; pp. 1–19. [Google Scholar]
- Ibitoye, M.O.; Estigoni, E.H.; Hamzaid, N.A.; Wahab, A.K.A.; Davis, G.M. The effectiveness of FES-evoked EMG potentials to assess muscle force and fatigue in individuals with spinal cord injury. Sensors 2014, 14, 12598–12622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Q.; Iyer, A.; Sun, Z.; Kim, K.; Sharma, N. A Dual-modal Approach Using Electromyography and Sonomyography Improves Prediction of Dynamic Ankle Dorsiflexion Motion. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1944–1954. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Sub01 | Sub02 | Sub03 | Sub04 | Sub05 | Sub06 | Sub07 | Sub08 |
|---|---|---|---|---|---|---|---|---|
| Threshold | 100 | 40 | 20 | 20 | 60 | 80 | 60 | 40 |
| Saturation | 420 | 580 | 520 | 500 | 520 | 500 | 400 | 560 |
| Participants | Coefficients and of Exponential Regression Models | |||||||
|---|---|---|---|---|---|---|---|---|
| Isometric Condition | Dynamic Condition | |||||||
| Sub01 | 0.955 | −0.022 | 0.015 | 0.929 | 0.952 | −0.016 | 0.115 | 0.923 |
| Sub02 | 0.948 | −0.018 | 0.098 | 0.919 | 0.600 | −0.020 | 0.405 | 0.904 |
| Sub03 | 0.931 | −0.019 | 0.005 | 0.876 | 0.894 | −0.034 | 0.186 | 0.965 |
| Sub04 | 0.515 | −0.020 | 0.502 | 0.942 | 0.732 | −0.048 | 0.453 | 0.940 |
| Sub05 | 0.616 | −0.019 | 0.760 | 0.957 | 0.733 | −0.037 | 0.377 | 0.926 |
| Sub06 | 0.981 | −0.011 | 0.428 | 0.803 | 0.478 | −0.037 | 0.526 | 0.888 |
| Sub07 | 0.824 | −0.018 | 0.301 | 0.904 | 0.518 | −0.049 | 0.567 | 0.911 |
| Sub08 | 0.835 | −0.031 | 0.165 | 0.925 | 0.457 | −0.053 | 0.631 | 0.907 |
| Sub01 | 0.581 | −0.082 | 0.598 | 0.967 | 0.634 | −0.025 | 0.436 | 0.919 |
| Sub02 | 0.390 | −0.036 | 0.193 | 0.772 | 0.751 | −0.013 | 0.119 | 0.763 |
| Sub03 | 0.643 | −0.073 | 0.497 | 0.899 | 0.867 | −0.062 | 0.350 | 0.857 |
| Sub04 | 0.695 | −0.060 | 0.452 | 0.966 | 0.622 | −0.026 | 0.449 | 0.919 |
| Sub05 | 0.730 | −0.036 | 0.193 | 0.771 | 0.751 | −0.013 | 0.119 | 0.763 |
| Sub06 | 0.665 | −0.055 | 0.455 | 0.966 | 0.642 | −0.046 | 0.408 | 0.919 |
| Sub07 | 0.618 | −0.057 | 0.398 | 0.891 | 0.691 | −0.038 | 0.309 | 0.863 |
| Sub08 | 0.724 | −0.046 | 0.344 | 0.895 | 0.685 | −0.039 | 0.308 | 0.865 |
| Participants | Coefficients and of Linear Regression Models | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Isometric Condition | Dynamic Condition | |||||||||
| a | p-Value | b | p-Value | a | p-Value | b | p-Value | |||
| Sub01 | 0.895 | 0.245 | 0.889 | 1.009 | −0.014 | 0.879 | ||||
| Sub02 | 0.894 | −0.118 | 0.852 | 1.036 | −0.155 | 0.682 | ||||
| Sub03 | 0.879 | 0.124 | 0.879 | 0.752 | 0.161 | 0.827 | ||||
| Sub04 | 1.475 | −0.555 | 0.911 | 0.900 | 0.126 | 0.847 | ||||
| Sub05 | 0.928 | −0.168 | 0.117 | 0.763 | 0.800 | 0.068 | 0.274 | 0.756 | ||
| Sub06 | 0.754 | 0.206 | 0.843 | 1.245 | −0.144 | 0.839 | ||||
| Sub07 | 1.319 | −0.248 | 0.811 | 1.019 | 0.005 | 0.763 | ||||
| Sub08 | 1.169 | −0.234 | 0.771 | 0.955 | 0.133 | 0.755 | ||||
| Mean | 1.039 | - | −0.094 | - | 0.840 | 0.965 | - | 0.023 | - | 0.794 |
| Standard deviation | 0.253 | - | 0.271 | - | 0.054 | 0.154 | - | 0.123 | - | 0.065 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Q.; Iyer, A.; Lambeth, K.; Kim, K.; Sharma, N. Ultrasound Echogenicity as an Indicator of Muscle Fatigue during Functional Electrical Stimulation. Sensors 2022, 22, 335. https://doi.org/10.3390/s22010335
Zhang Q, Iyer A, Lambeth K, Kim K, Sharma N. Ultrasound Echogenicity as an Indicator of Muscle Fatigue during Functional Electrical Stimulation. Sensors. 2022; 22(1):335. https://doi.org/10.3390/s22010335
Chicago/Turabian StyleZhang, Qiang, Ashwin Iyer, Krysten Lambeth, Kang Kim, and Nitin Sharma. 2022. "Ultrasound Echogenicity as an Indicator of Muscle Fatigue during Functional Electrical Stimulation" Sensors 22, no. 1: 335. https://doi.org/10.3390/s22010335
APA StyleZhang, Q., Iyer, A., Lambeth, K., Kim, K., & Sharma, N. (2022). Ultrasound Echogenicity as an Indicator of Muscle Fatigue during Functional Electrical Stimulation. Sensors, 22(1), 335. https://doi.org/10.3390/s22010335