
Can Formal Security Verification Really Be Optional? Scrutinizing the Security of IMD Authentication Protocols


Abstract
:1. Introduction
- We examined various security and privacy requirements along with numerous threats that surround IMDs.
- We performed formal security validation of the contemporary authentication schemes based on BAN logic and AVISPA against several security goals.
- We compared these schemes concerning security strength, computational overhead, latency, and additional features, such as emergency authentication, adaptiveness, and key update mechanisms.
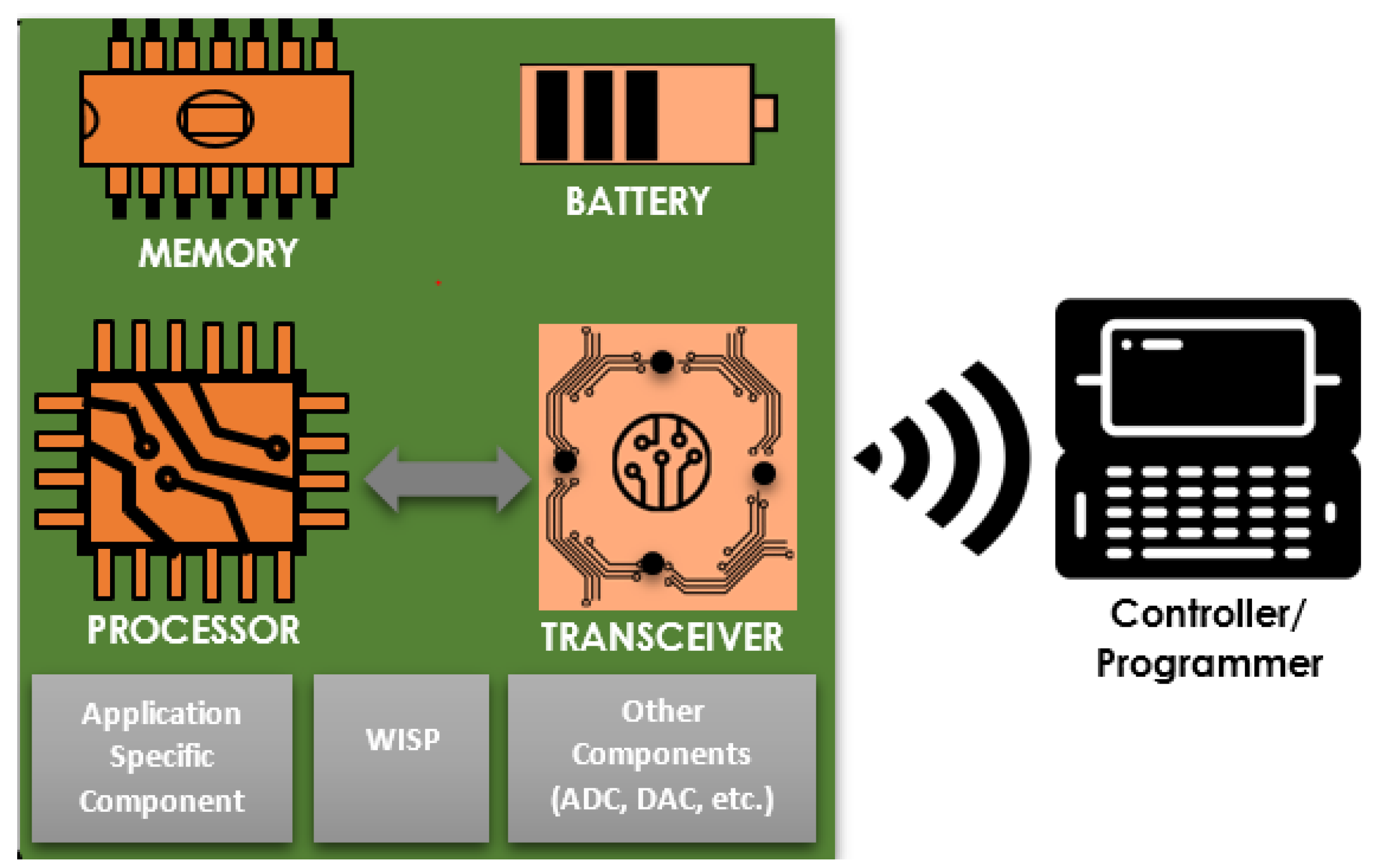
2. Typical IMD System Architecture
- Sensor devices. These are small, in-body implanted, battery-powered, and wireless communication enabled sensors to sense, collect, and send patient information to a controller. In general, there are three categories (based on the data measured/collected) of such sensors: those that measure vital physiological information (such as glucose level, EEG, ECG, etc.), those that gather main environmental parameters, such as humidity, temperature, and pressure, and those that measure signals related to the human body movements [31].
- Battery. Implanted sensors need the power to sense information on the body and produce an output. The source of energy for active implants comes from batteries. These batteries can be chargeable or non-chargeable, depending on the sensor type [32], and external or through independent power sources [33]. While the former approach uses optical charging, ultrasonic transducer, and inductive coupling, the latter uses the body environment energy to generate electrical energy for IMDs. Either way, efficient power management is a must since it is difficult (or not desirable) to change batteries now and then. Hence, batteries fixed with these implants should serve for a prolonged period.
- Memory. Memory is vital for the proper functioning of IMDs. It enables implants to store sensed data, configurations, and other important information (such as security keys). The device memory is generally non-volatile (read-only memory (ROM)), retaining its contents regardless of the power supply. In addition, the electrically erasable programmable ROM (EEPROM) and flash memories can be good candidates [32].
- Processing unit. The processing unit is the brain of the entire IMD system, which processes instructions and control signals. The processing unit actively directs the communication between IMDs and external devices, efficient power and transceiver management, and is responsible for other essential tasks, such as sensing and processing data [32].
- Transceiver. To communicate different sensed data to the external devices (such as a programmer) and receive other information from the external devices, IMDs need to establish a wireless medium. An electronic device, known as a transceiver (transmitter and receiver), assists this exchange of information. A specifically designed transceiver called the Medical Implant Communication System (MICS) is available for medical implants with low-power, short-range, and high data rate features [34].
- Application-Specific Components. These components are optional, meaning they may not appear in all implanted devices. One good illustration is the Smart Implant Security Core (SISC) [35]. Communication between IMD and a programmer via wireless medium passes through this device. It runs an energy-efficient security protocol by using energy harvesting when it performs authentication with the programmer. Apart from that, SISC helps defend against denial-of-service attacks, particularly resource exhaustion attacks.
- Wireless Identification and Sensing Platform (WISP). One of the significant constraints of implanted devices is related to power. These devices reside in the human body, making them challenging to recharge or frequently change. Hence, a device called WISP is proposed [32]. Using WISP, therefore, it is possible to conserve the battery of an IMD, especially during an authentication process, as it harvests energy from the reader via radiofrequency.
- Programmer/Controller. Sensing or measuring vital physiological states is only half of the primary goal of using implants. The sensors should also convey the sensed information to an external device (a specially designed controller or a smartphone) near the IMDs. Apart from collecting sensed information from the implants, programmers/controllers assist in configuration setup and regulation of therapy, among others.
3. Security and Privacy Requirements, Threats, and Proposed Solutions
3.1. Security and Privacy Requirements
- Confidentiality: the physiological information collected by IMDs is often sent out to a reader via a wireless medium, which both authorized and malicious users can observe. Accordingly, it is essential to encrypt this information to protect the data transmitted from exploitation by the adversaries sitting between the IMD and the reader.
- Integrity: protecting the integrity of the information transmitted via the wireless link in IMD reader communication defends against unauthorized modification. In addition, when illegitimate users tamper with the data, it should be known by the authorized users that the data is modified.
- Availability: this is one of the three security triads (confidentiality, integrity, and availability) that has the objective of making the IMD-enabled system accessible to authorized users despite the presence of adversaries.
- Mutual authentication: unless authorized access is in place, an adversary can impersonate the IMD or the reader to fool the other. Hence, communicating parties need to make sure whom they are talking to before disclosing important information.
- Authorization: once the confidentiality, integrity, and availability of IMDs are guaranteed, and the users (a human user or a device such as a reader) are authenticated, proper authorization to identify the privileges of these users’ proceeds. For instance, a doctor who may issue commands to the IMD should be distinct from a nurse who may only read information to monitor the patient.
- Non-repudiation: there are cases in which one party’s actions (knowingly or not) bring unwanted consequences. For instance, in an IMD-enabled health care system, there can be many participants in the process of diagnosing, monitoring, and treating patients. These professionals should not be able to repudiate the actions they took during the process so that, if anything terrible happened next, it is possible to know who did what.
- Session key agreement: communicating entities need to agree on a session key and use that key to encrypt the exchanged information. Session keys are symmetric keys that are primarily derived from another key (called a master key) to restrict ciphertexts and minimize the exposure of an attack. Furthermore, using session keys improves communication performance since these keys do not need to be stored and searched. Moreover, symmetric key encryption is faster.
- Perfect forward secrecy: satisfying this security requirement means the past sessions will not be compromised even if a master key is compromised. In the context of IMDs, if the long-term key is stolen, and if this is known, the key can be updated, and only minimal information would be disclosed while all past communications can be kept safe from future compromises.
- Emergency authentication: if we deal with patients with implanted devices, there can always be emergencies requiring human intervention. Emergency authentication is one of the paradox requirements since unauthorized users need to access the implants to override the authorization and authentication properties, which calls for a clear definition of an emergency.
- Device-existence privacy: this privacy requirement challenges the protocol designers to conceal the device’s information of an IMD-enabled system and prohibit an adversary from learning its existence.
- Device-type privacy: in the cases where the presence of a device cannot be wholly concealed or its privacy cannot be maintained, the type of the device should stay anonymous. By doing so, it is possible to protect the patient from device-type specific attacks.
- Specific-device ID privacy: the unique ID (or serial number) of an IMD should not be disclosed to unauthorized users. Doing so protects the patients by prohibiting attackers from tracking down their locations.
- Measurement and log privacy: the information measured, collected, and analyzed in either IMD or the reader should be kept private. Keeping the privacy of logs enables the investigation and trace actions taken during the communication.
- Bearer privacy: these are often related to information such as patients’ names, record history, tests, IMD characteristics, etc., which should be kept private.
3.2. Security Issues and Proposed Solutions
4. Formal Security Verification
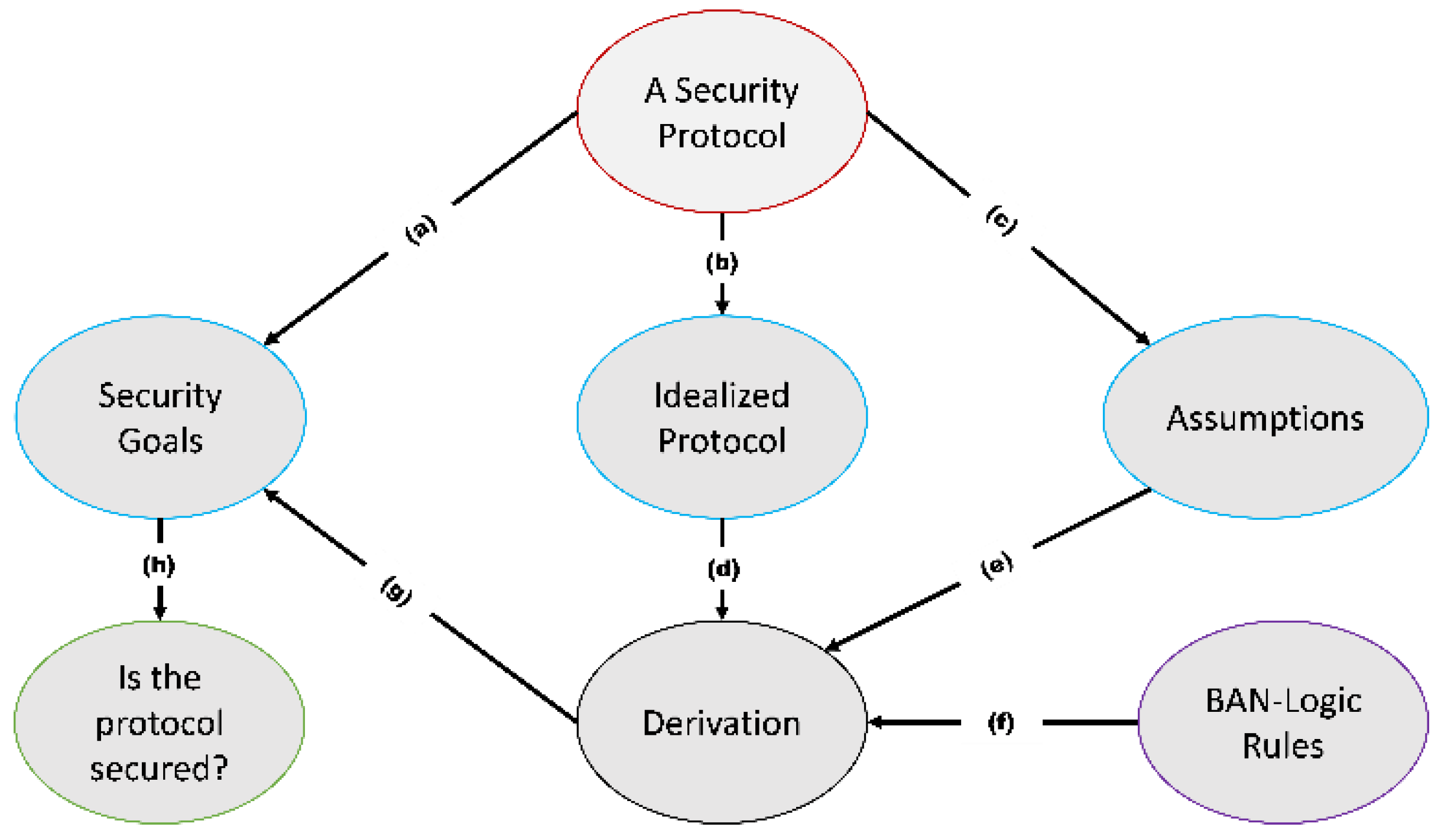
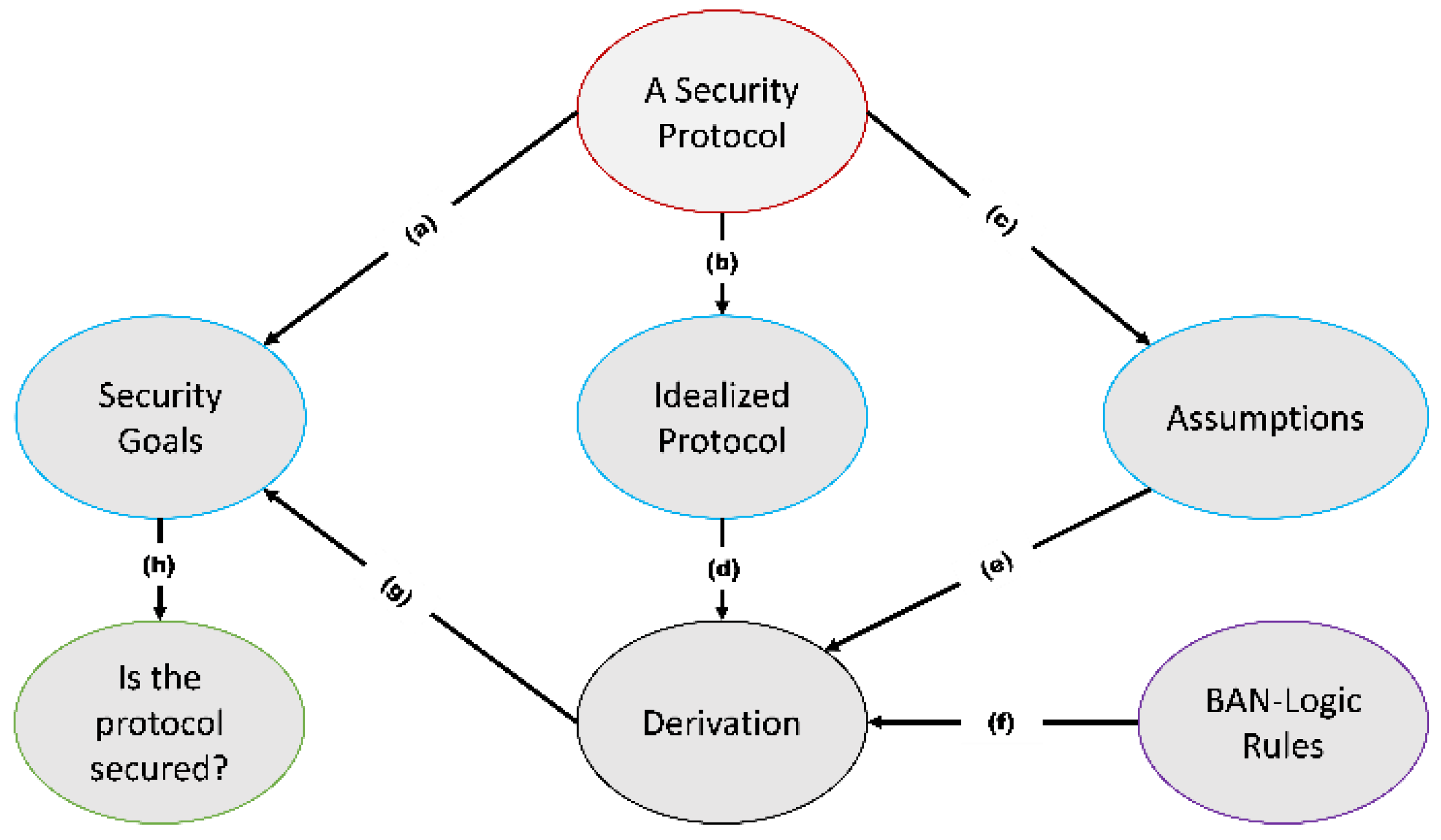
4.1. BAN Logic Based Formal Security Verification
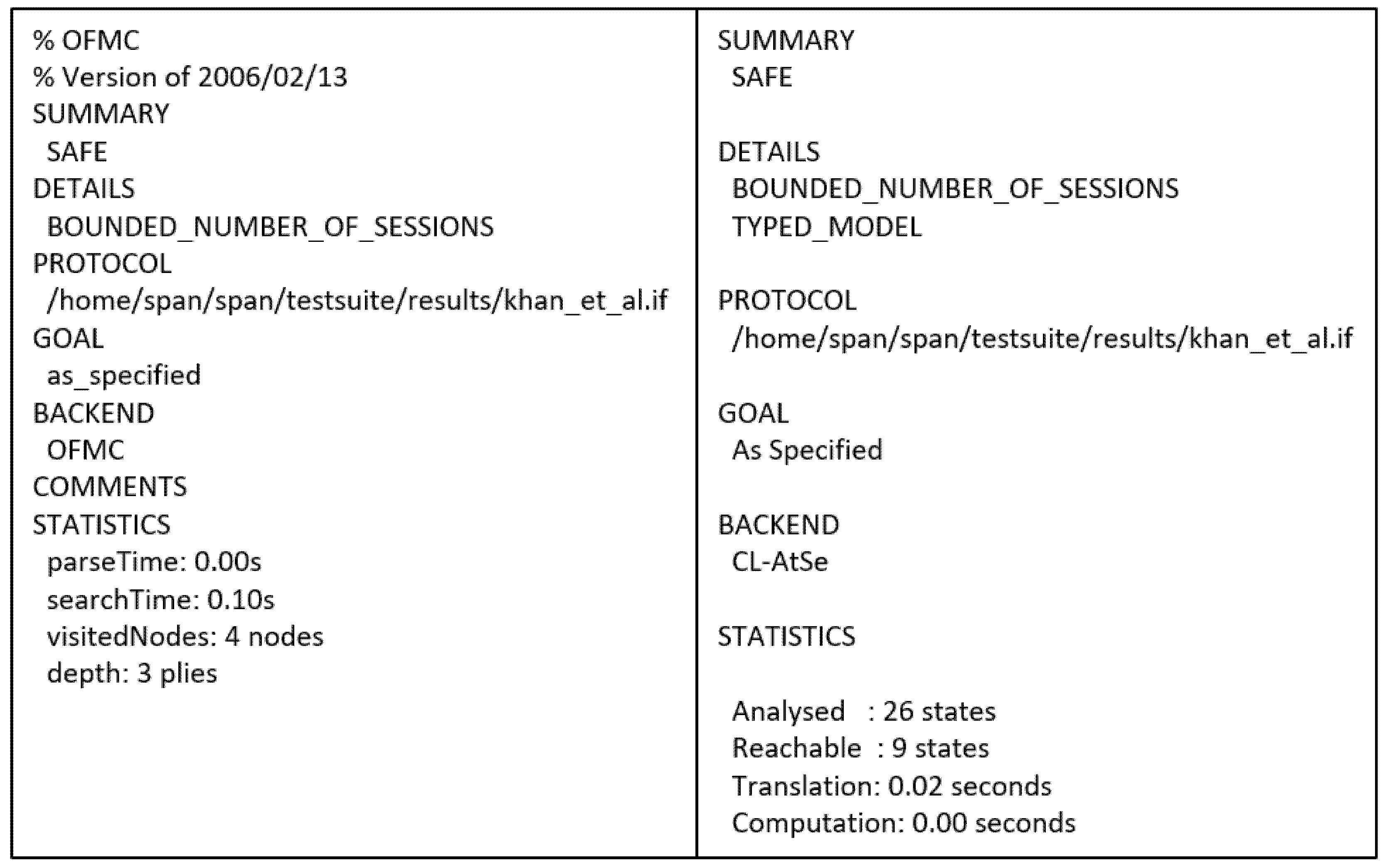
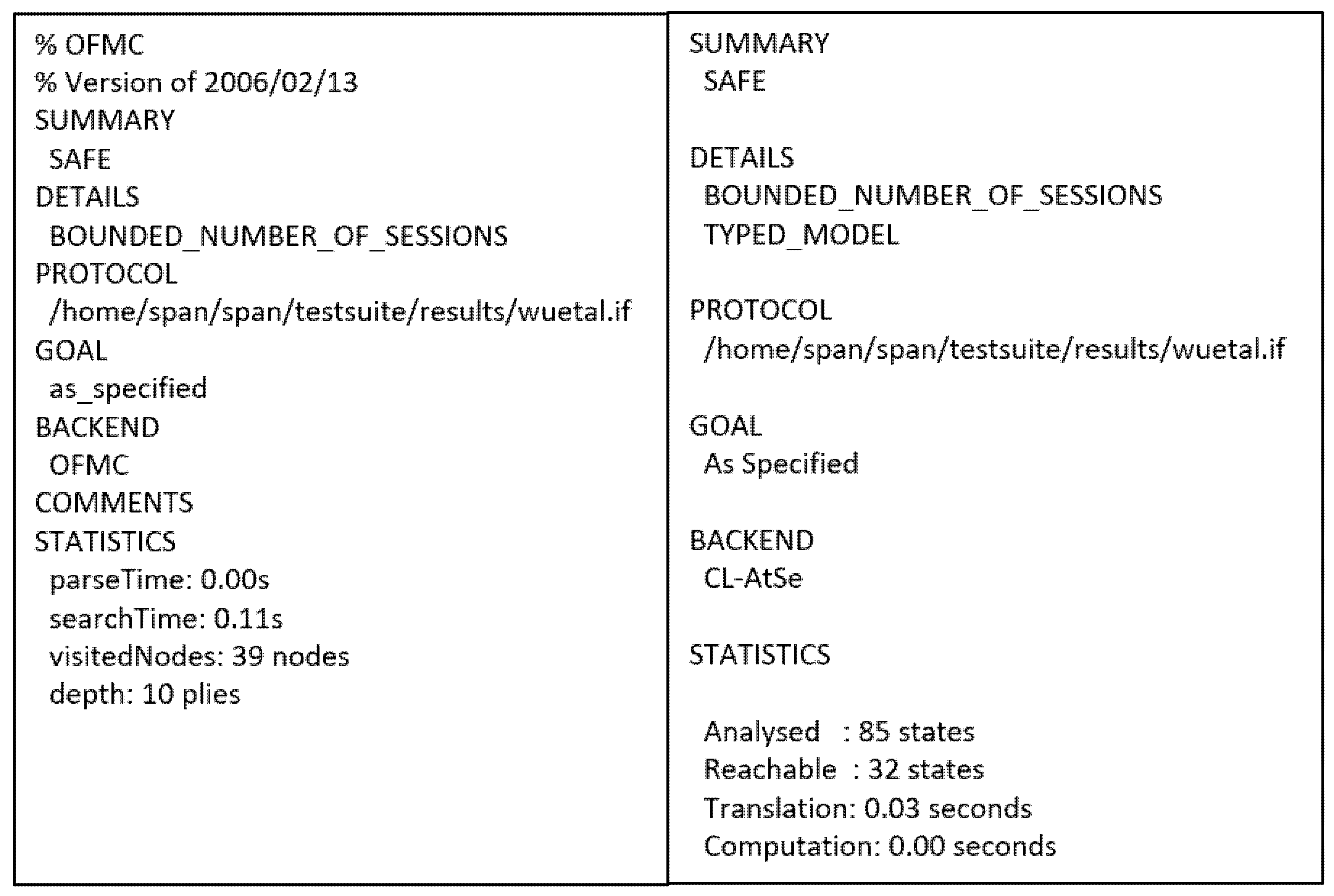
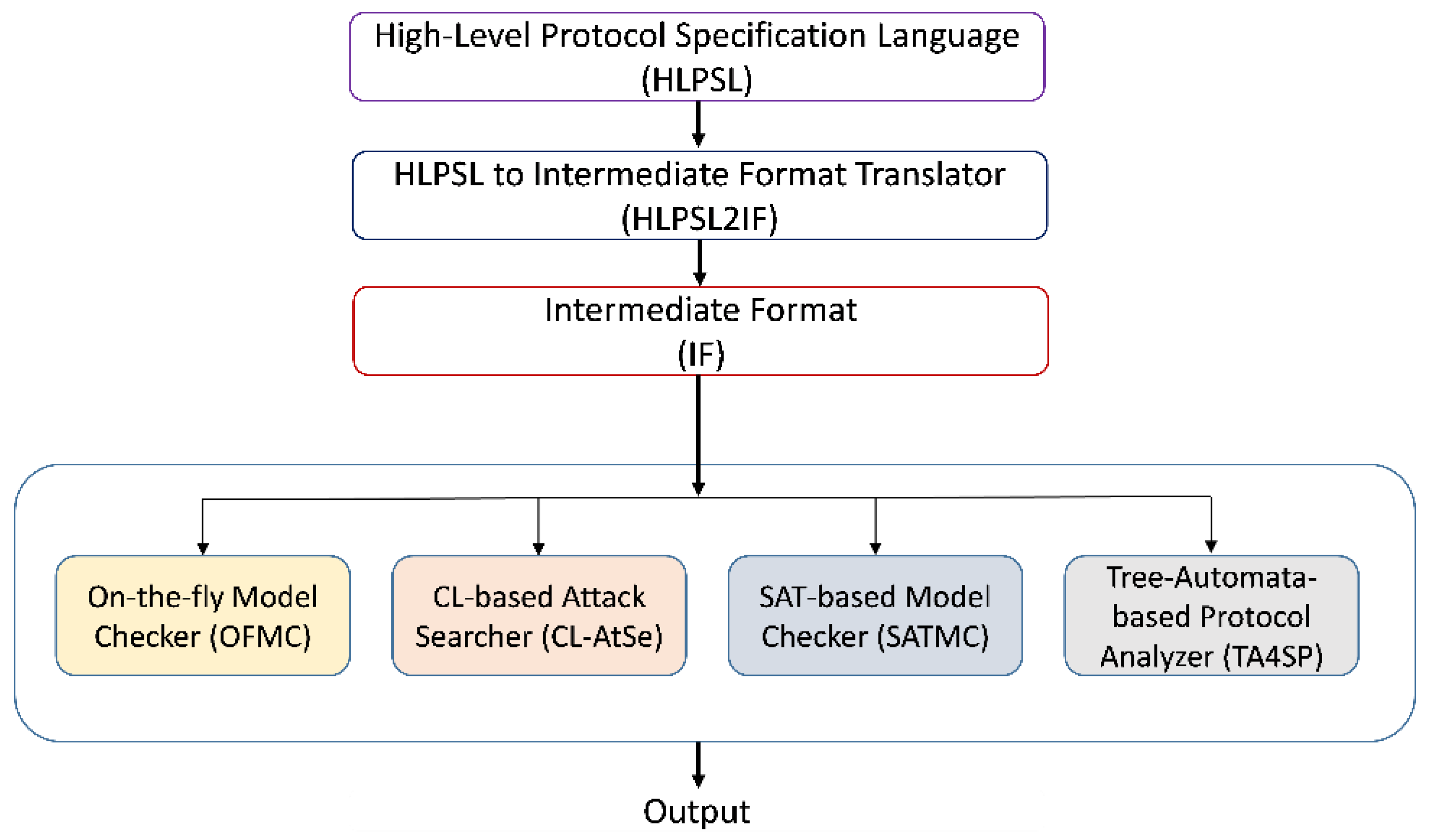
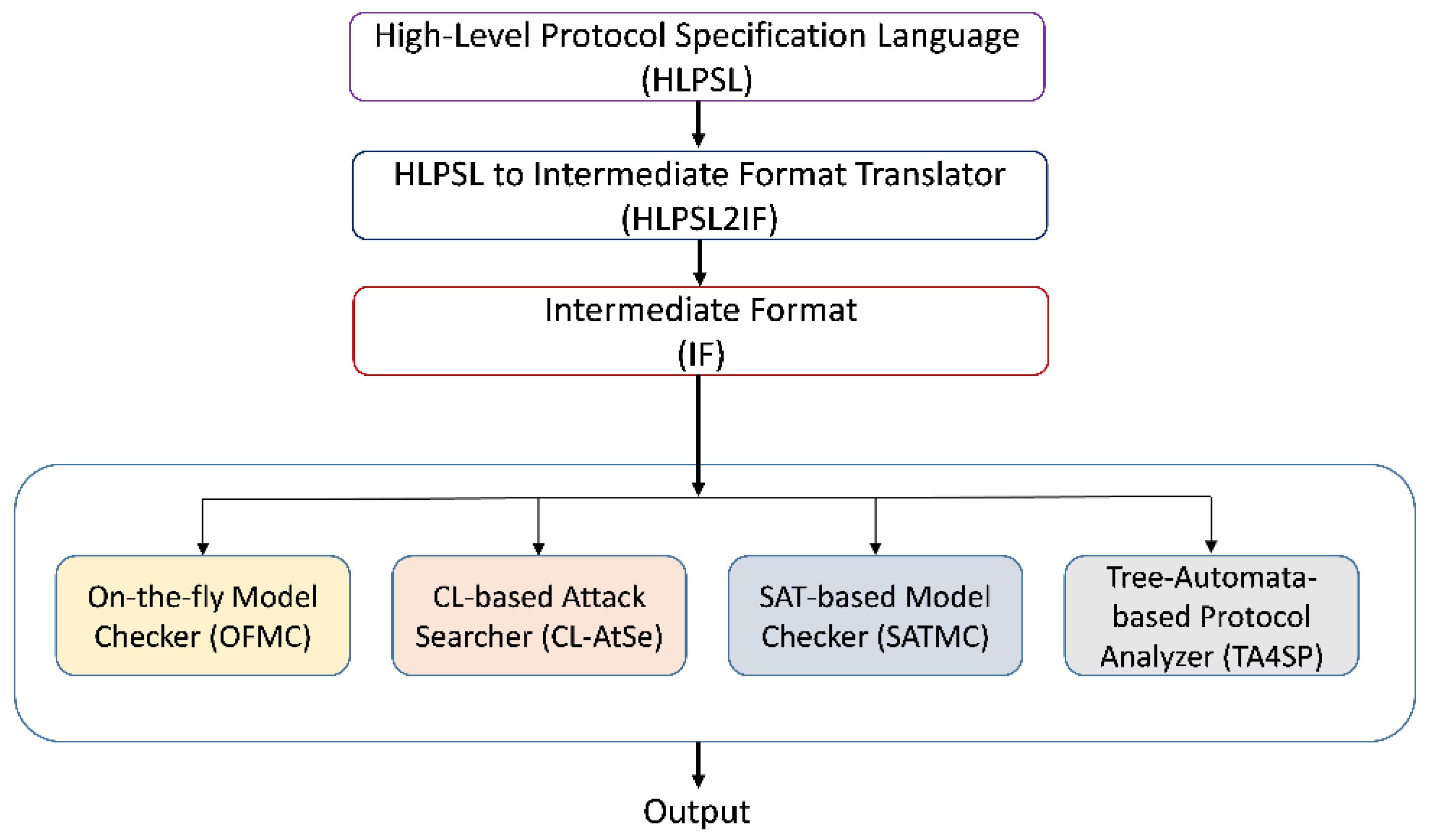
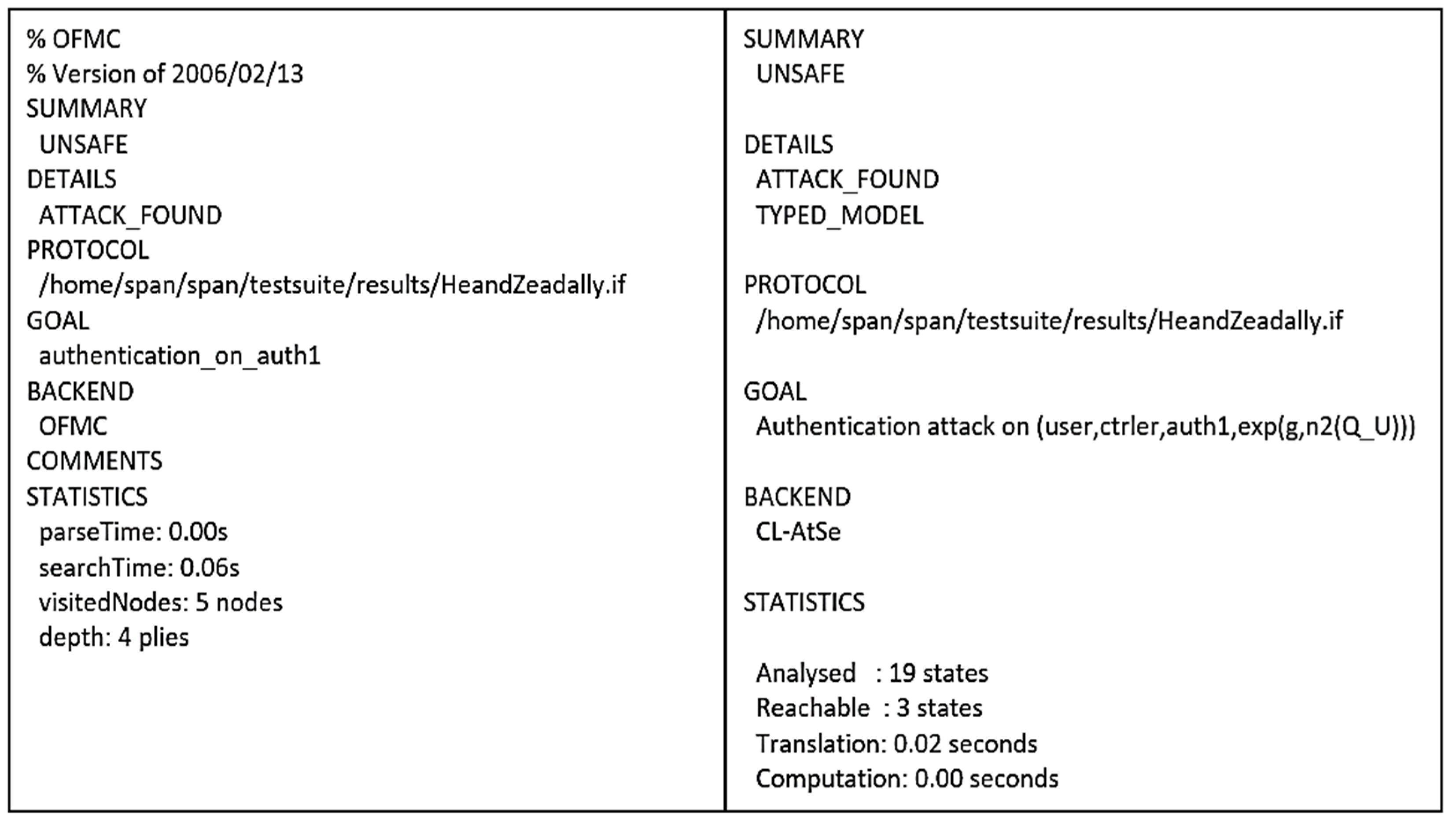
4.2. AVISPA Based Formal Security Analysis
4.3. Formal Security Analysis of IMD Authentication Protocols
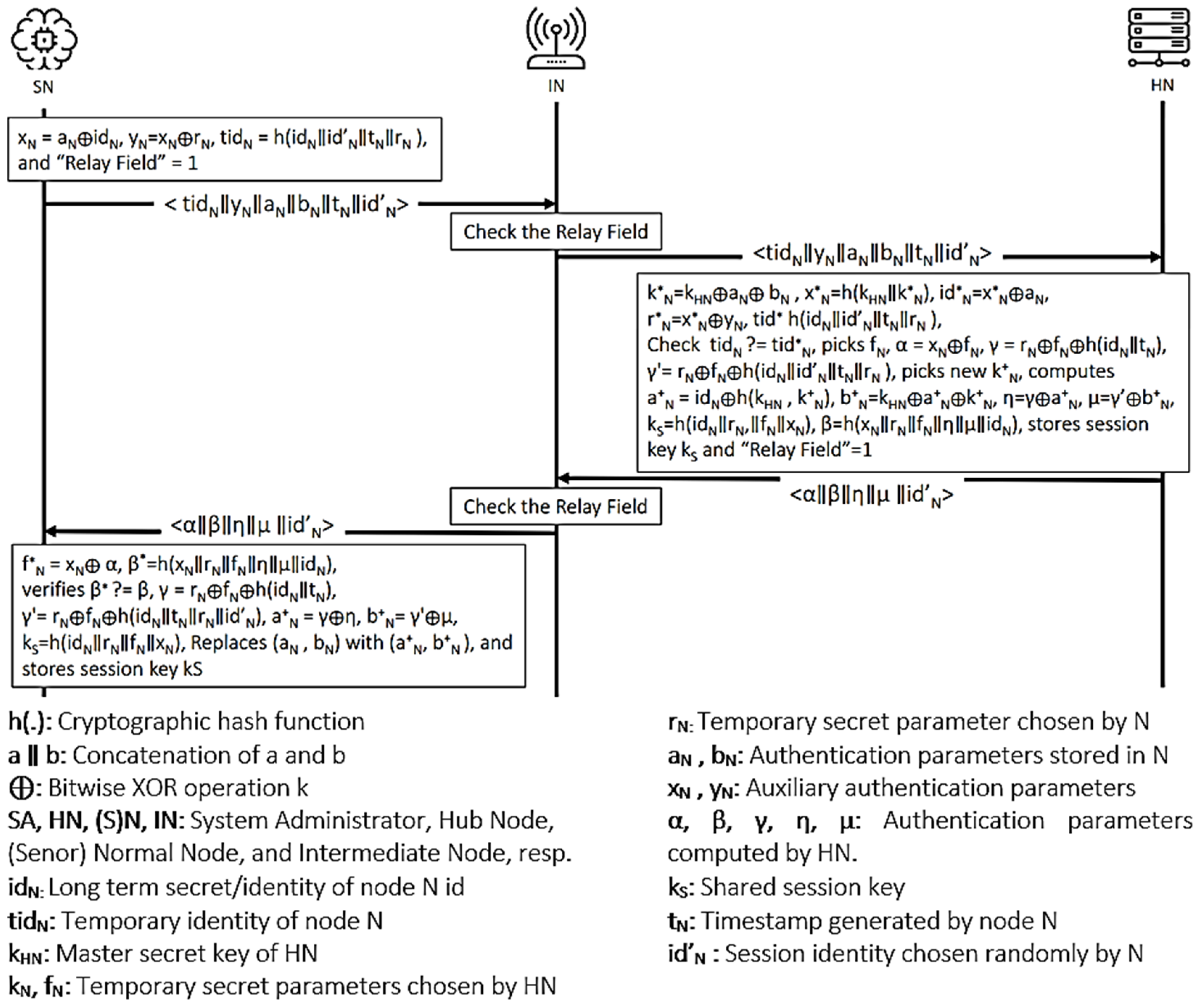
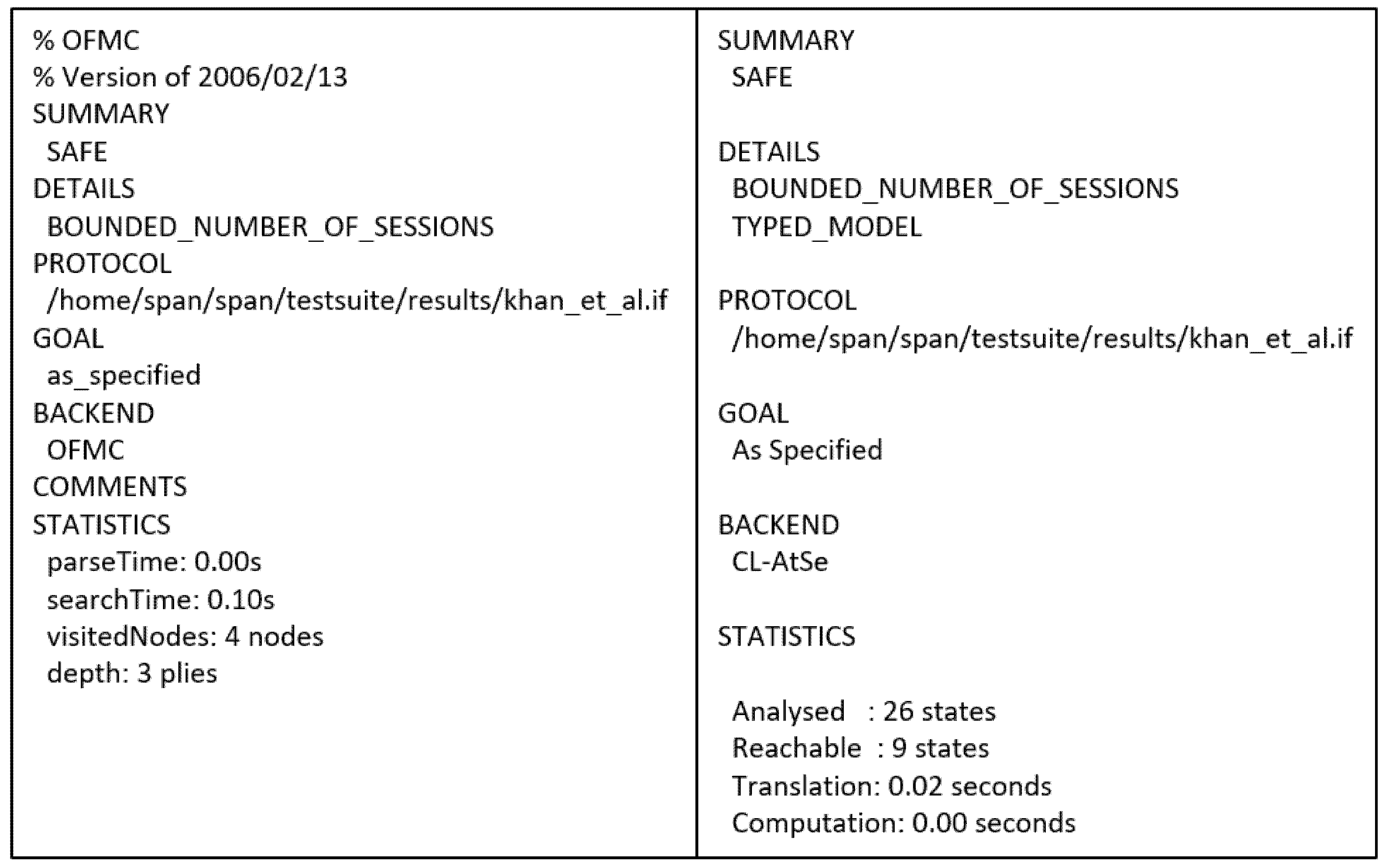
4.3.1. Khan et al.’s Protocol
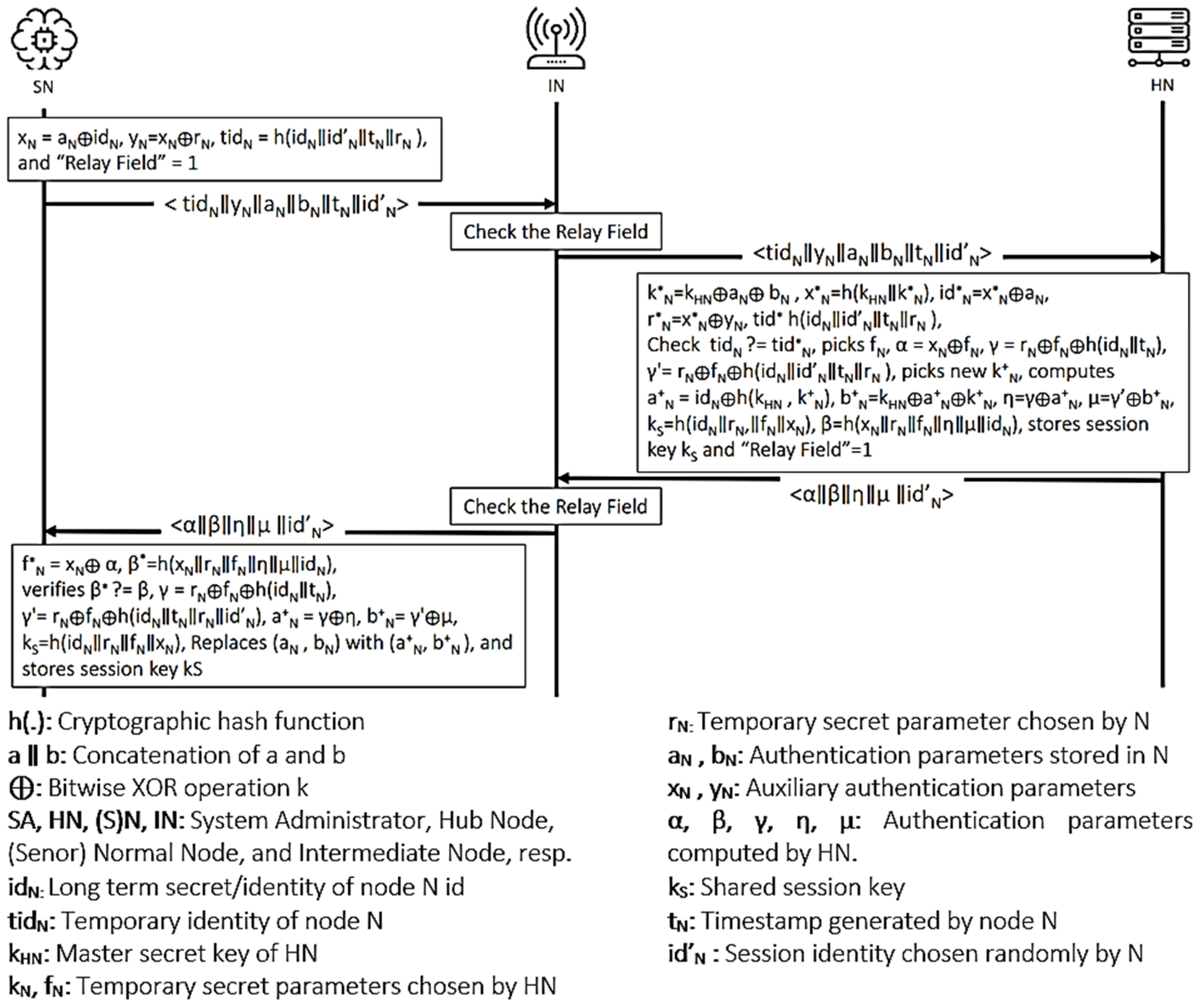
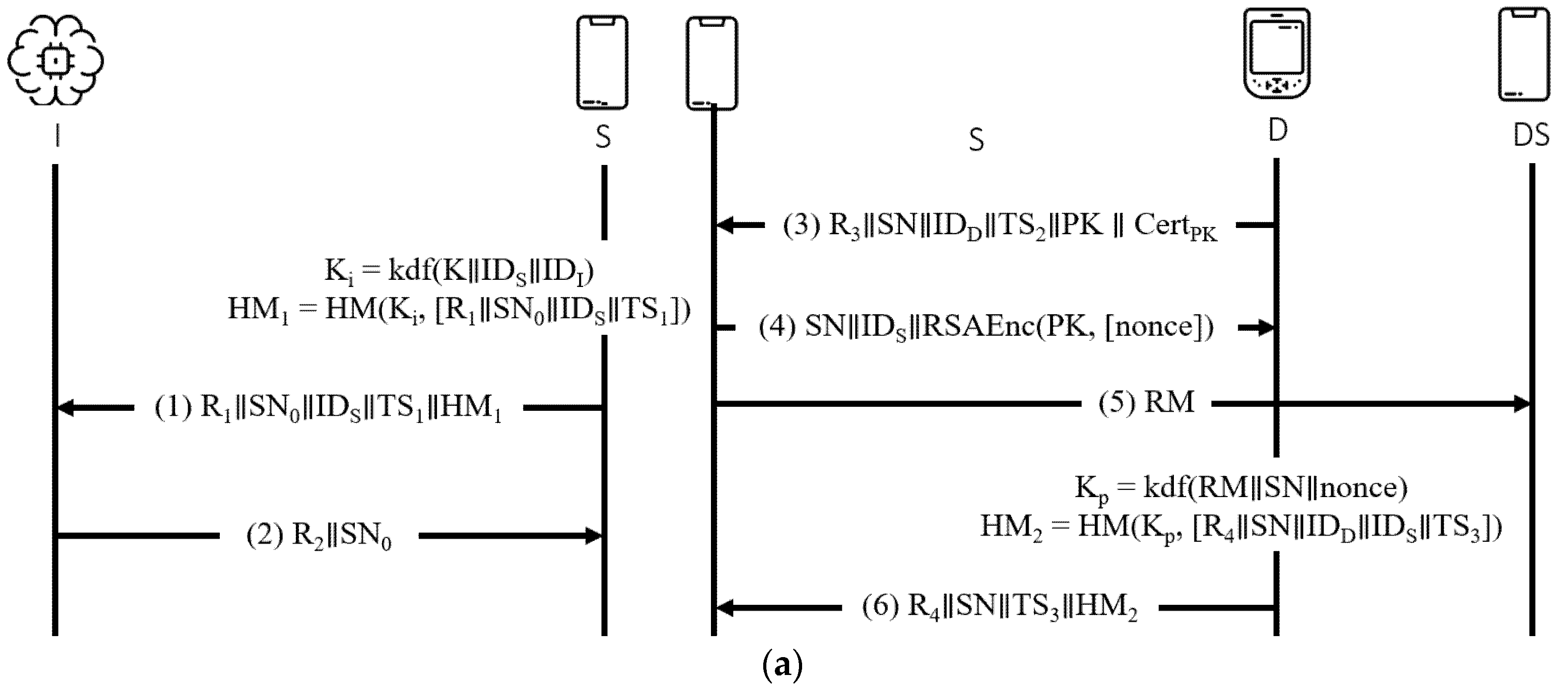
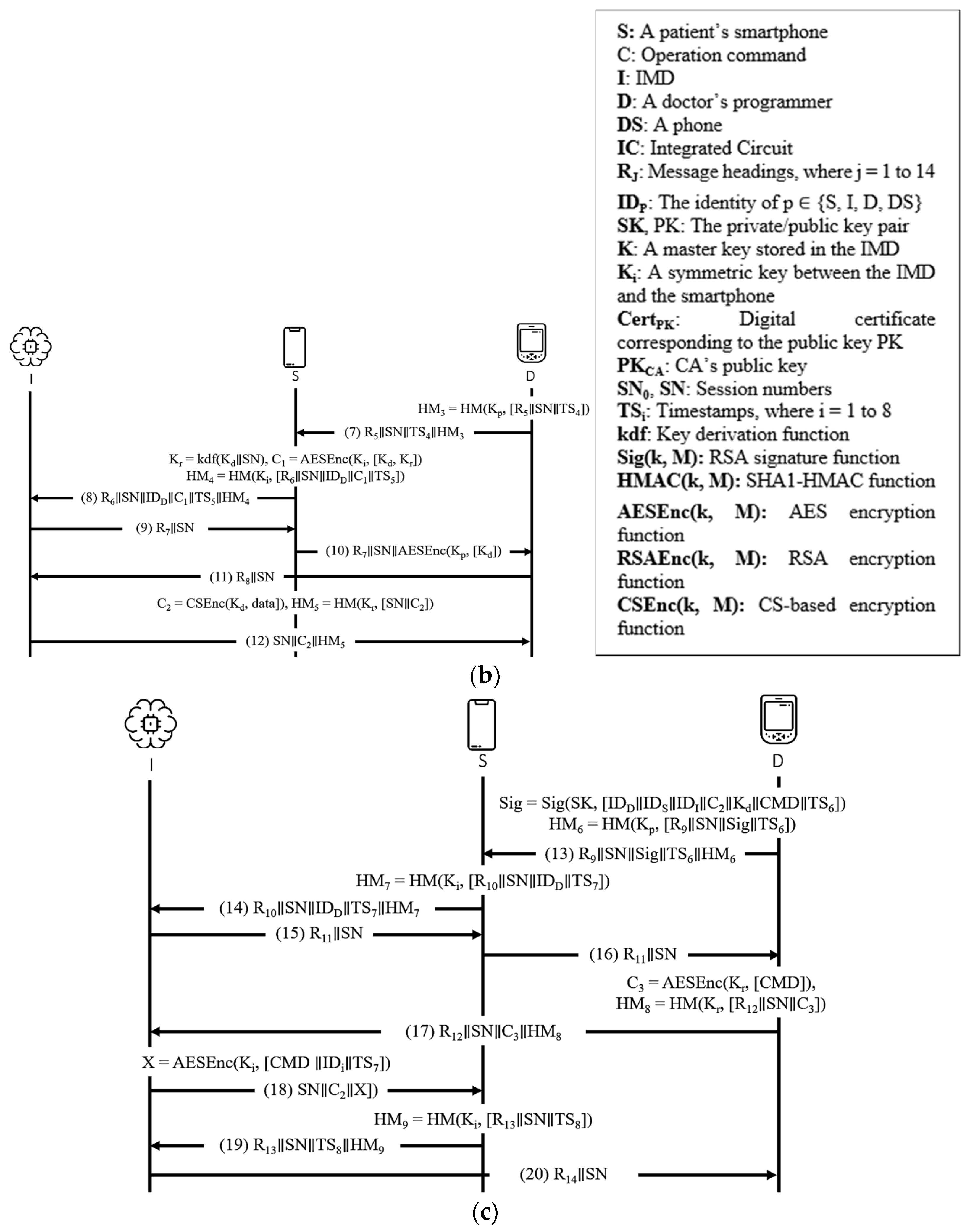
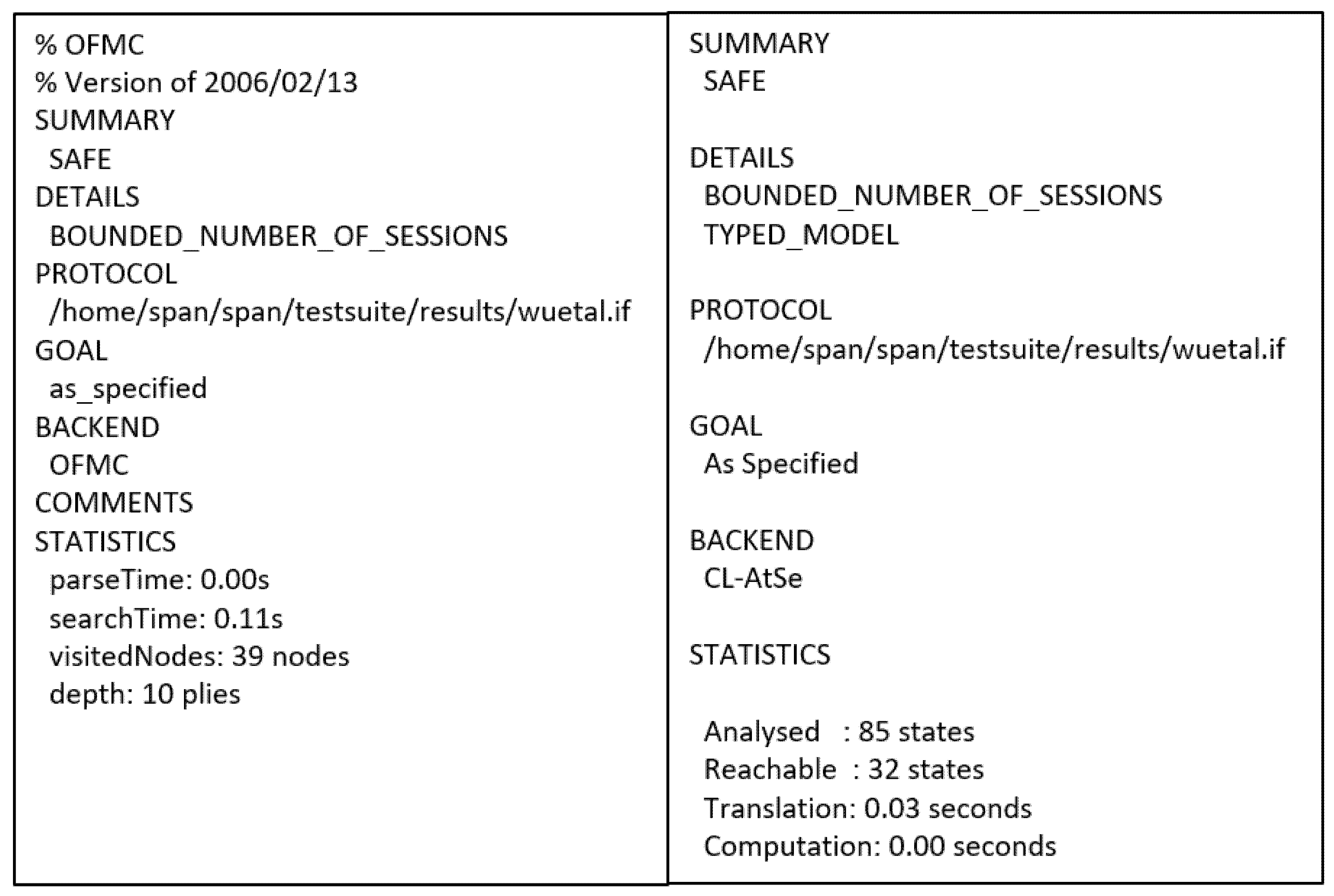
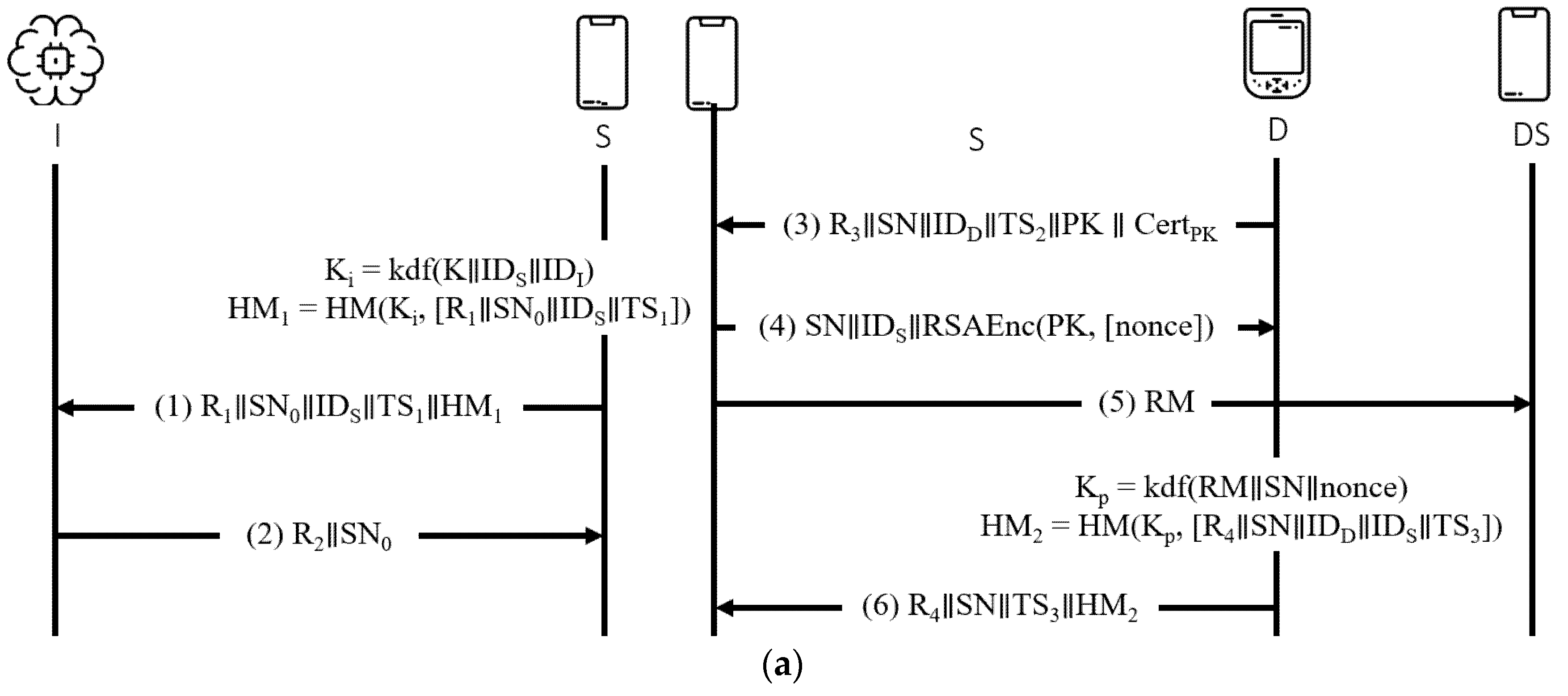
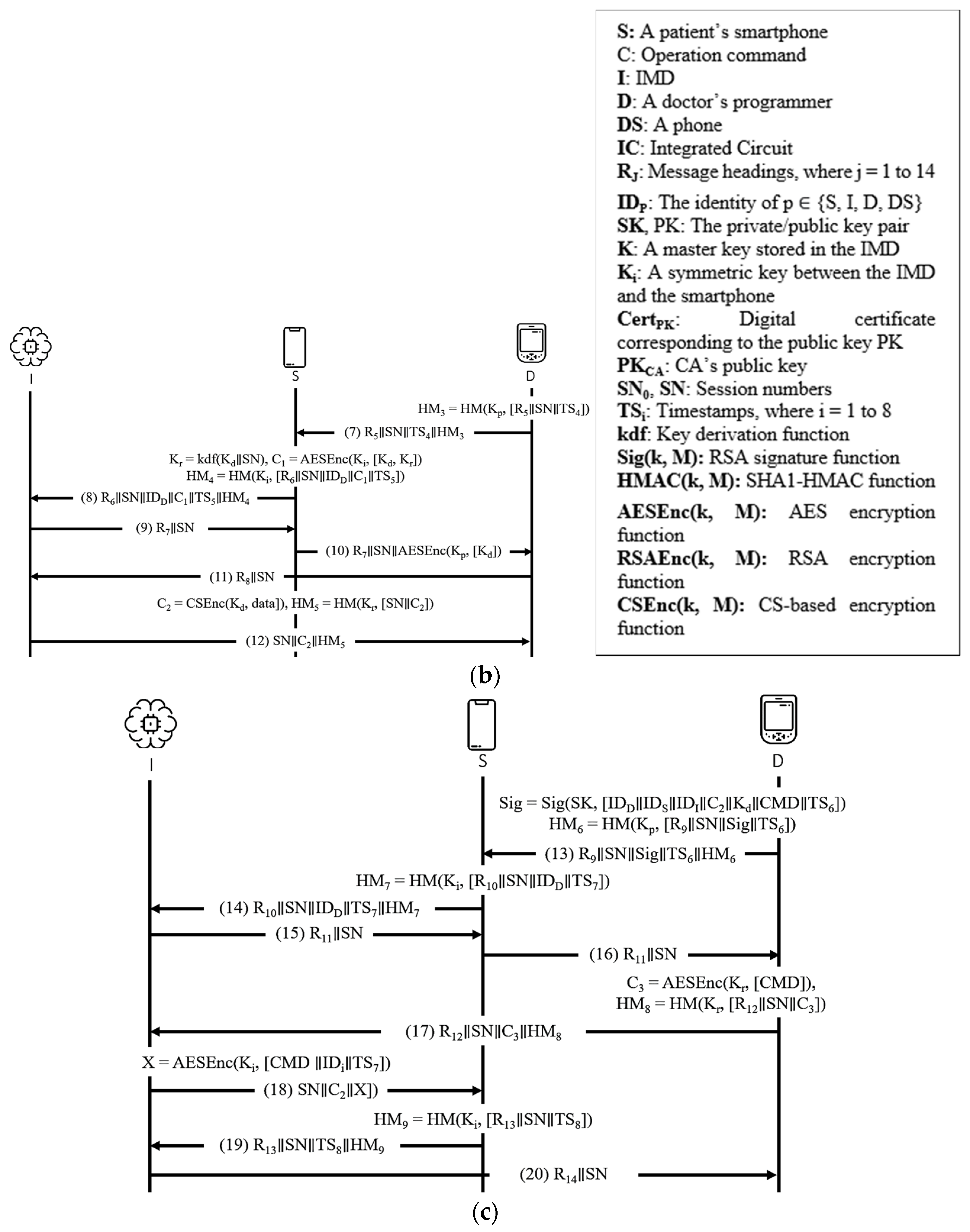
4.3.2. Wu et al.’s Protocol
- BAN logic-based formal security analysis.Figure 6. Wu et al.’s protocol.
![Sensors 21 08383 g006]()
● Idealization (I1) (I2) (I3) , (I4) , (I5) , ● Assumption (A1) (A2) (A3) (A4) (A5) (A6) (A7) (A8) (A9) (A10) (A11) (A12) (A13) (A14) (A15) ● Goals (G1) (G2) (G3) (G4) (G5) (G6) (G7) (G8) (G9) (G10) ● Derivations (D1) (D2) (D3) (D4) (D5) (D6) (D7) (D8) (D9) (D10) (I3) (D11) (D12) (D13) (D14) (D15) (D16) (D17) (D18) (D19) (D20) (D21) (D22) (D23) (D24) (D25) (D26) (D27) (D28) (D29) By (D28),(I15), JR
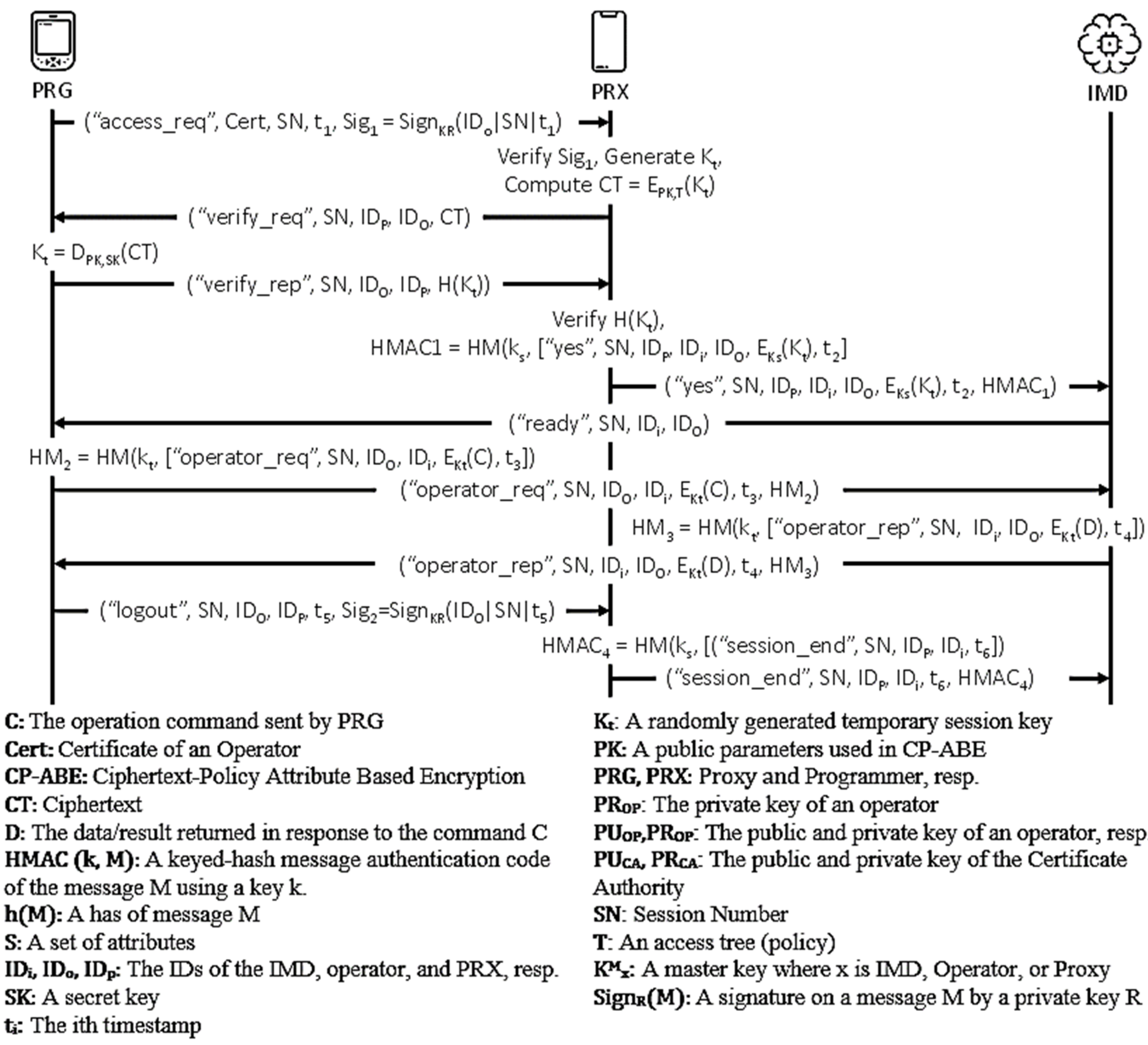
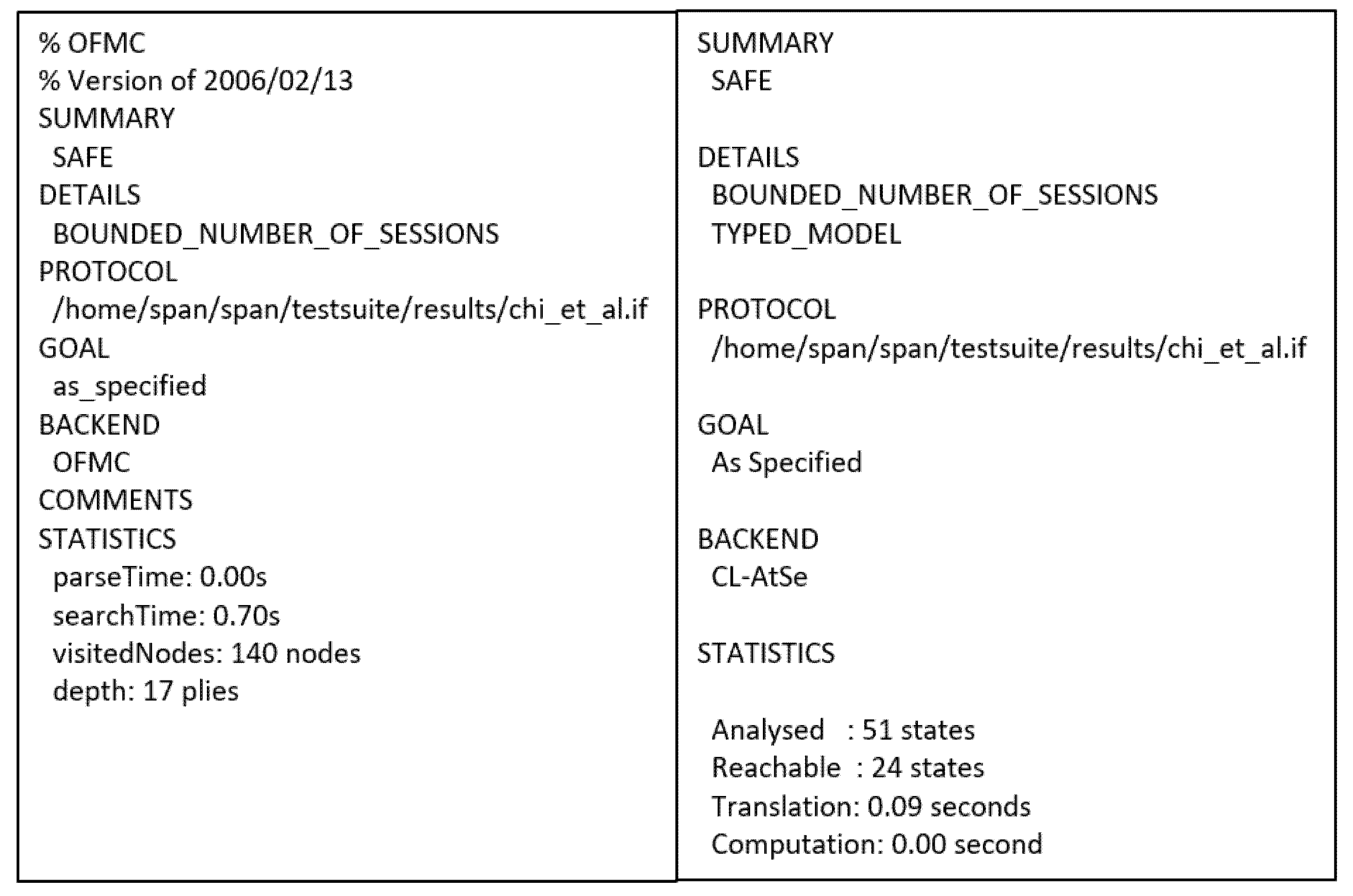
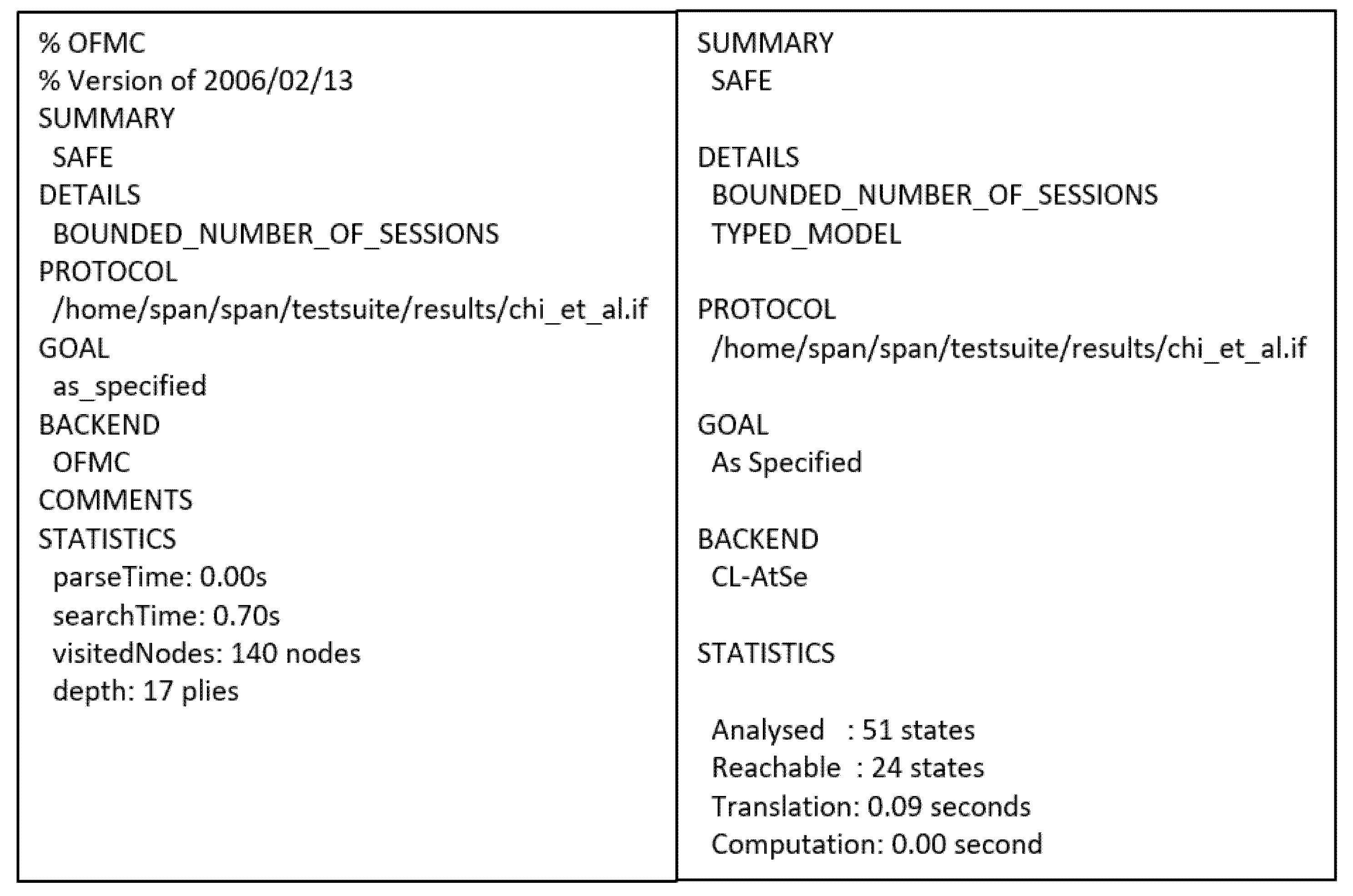
4.3.3. Chi et al.’s Protocol
- BAN logic-based formal security analysis.
● Idealization (I1) (I2) (I3) (I4) (I5) (I6) (I7) (I8) ● Assumption (A1) (A2) (A3) (A4) (A5) (A6) (A7) (A8) (A9) (A10) (A11) (A12) (A13) (A14) (A15) (A16) (A17) (A18) (A19) (A20) (A21) (A22) (A23) ● Goals (G1) (G2) (G3) (G4) (G5) (G6) (G7) (G8) (G9) (G10) (G11) (G12) (G13) (G14) (G15) (G16) (G17) ● Derivations By (I2) By (I3) (I4) By (I5) (I6) (I7)
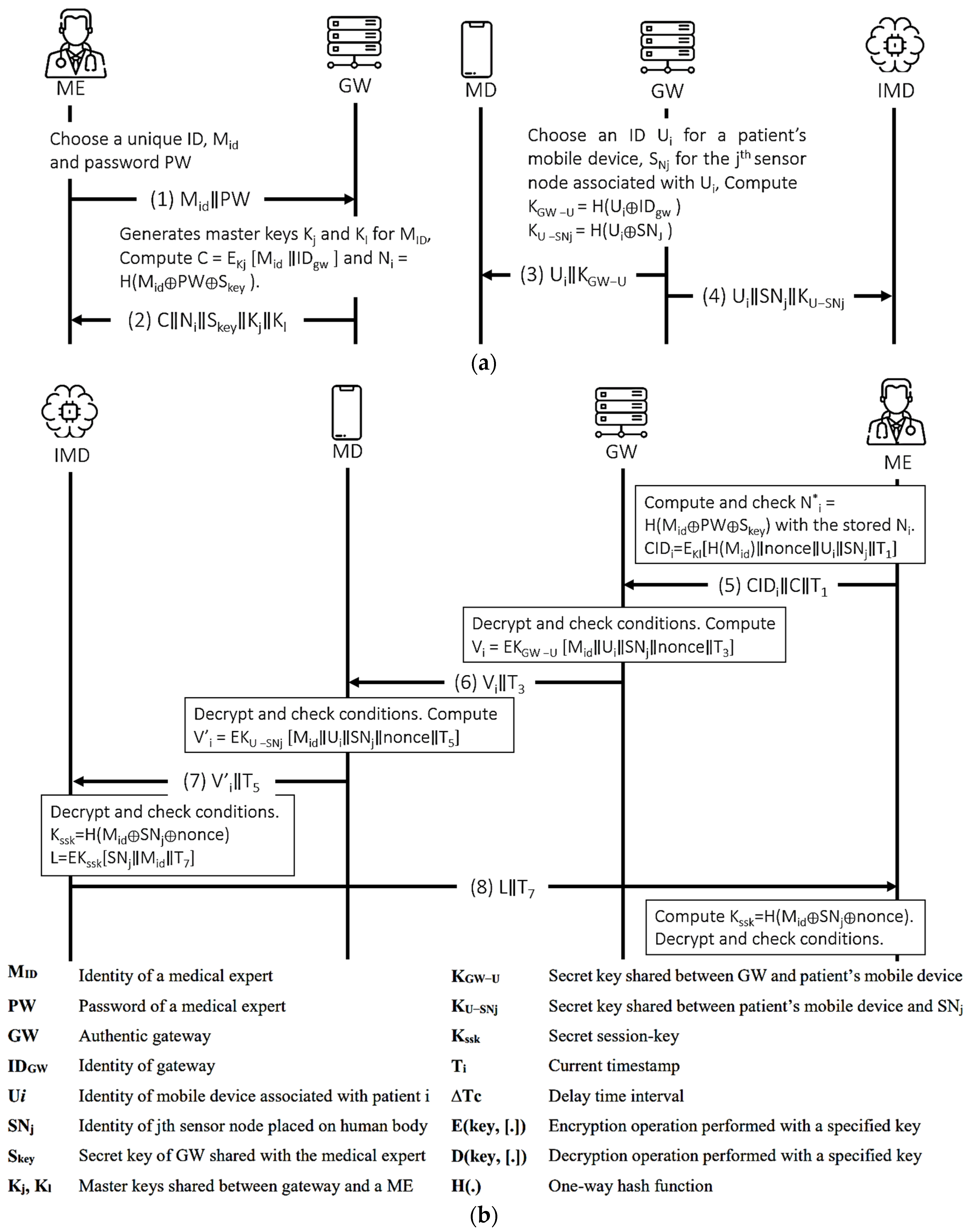
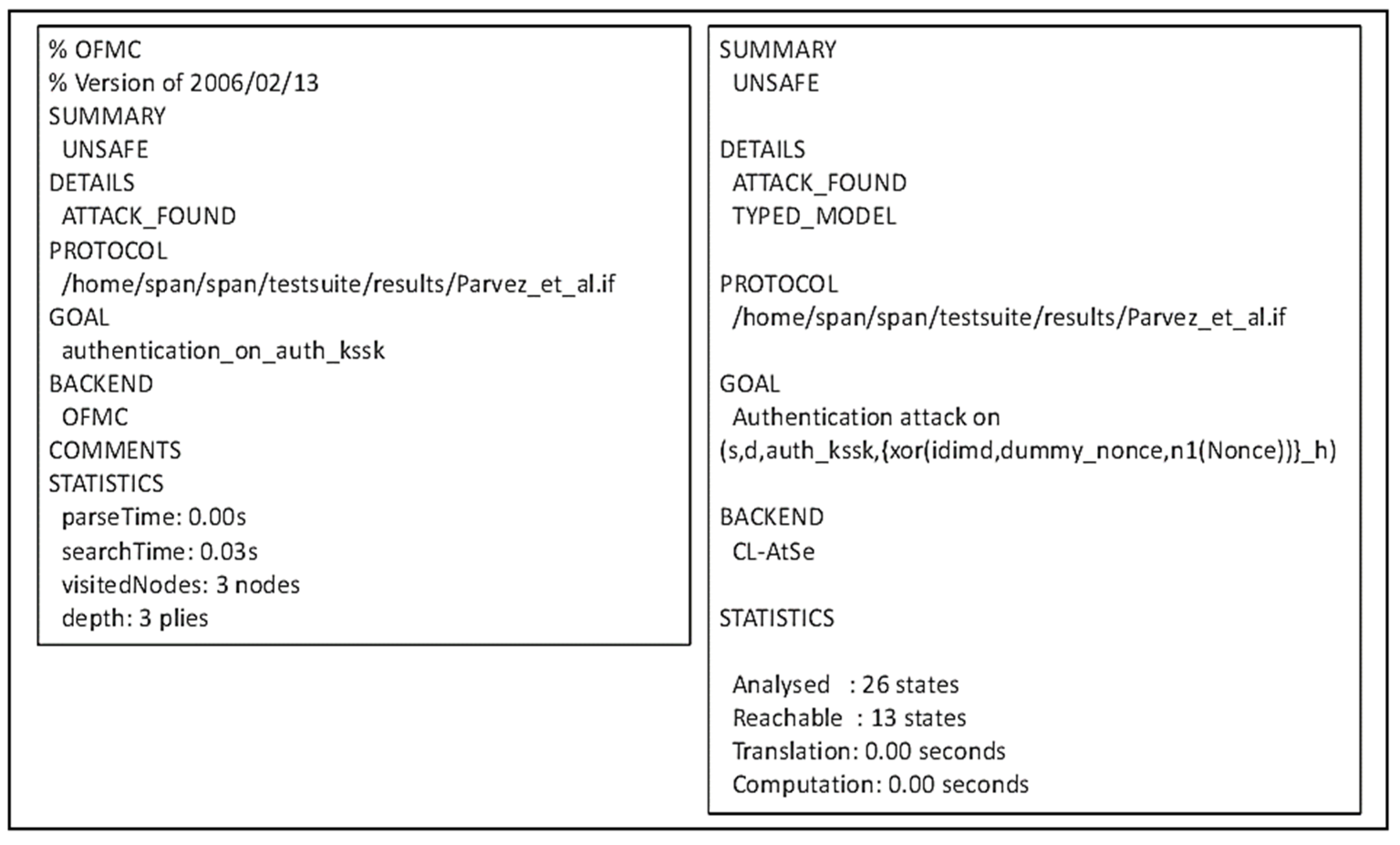
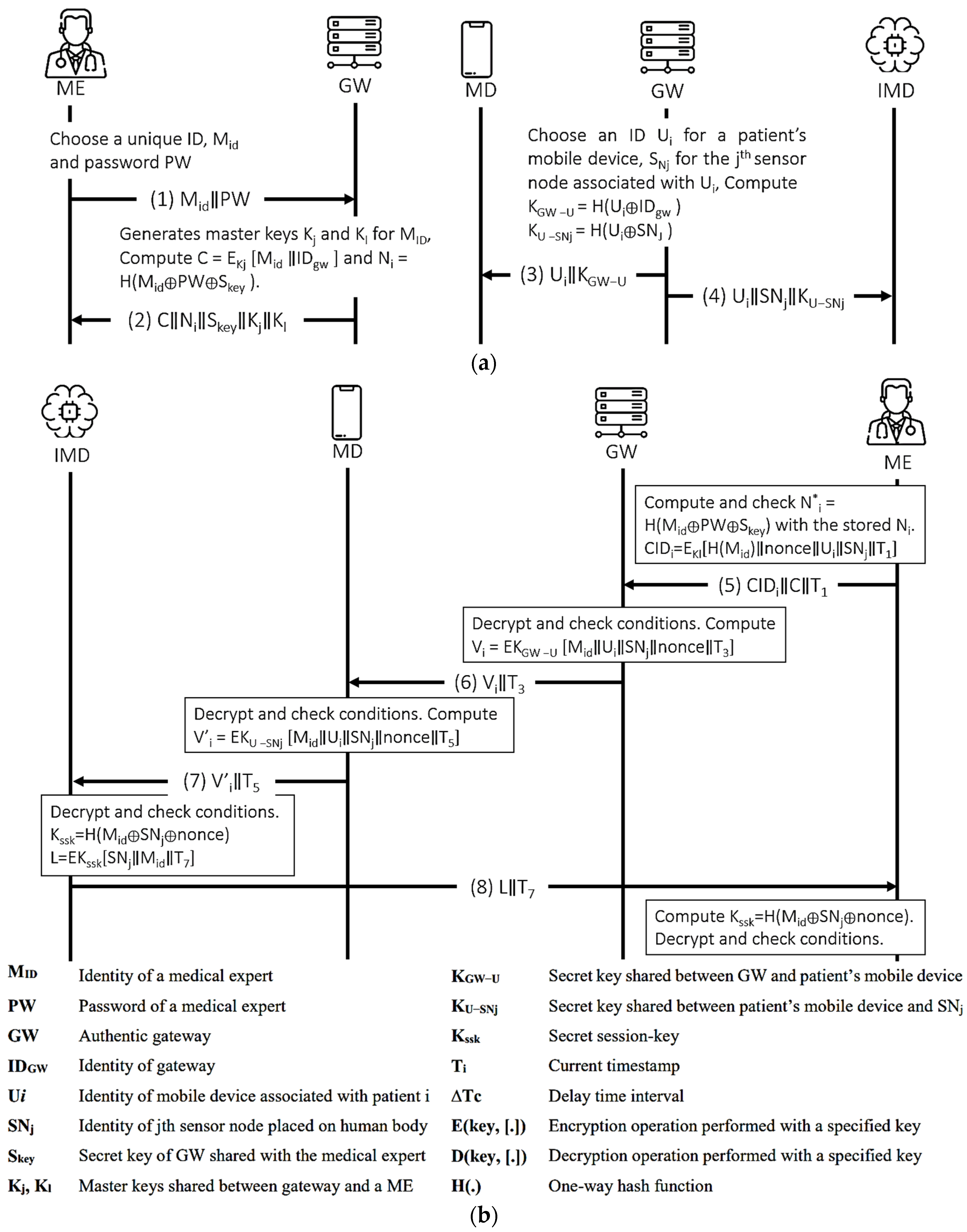
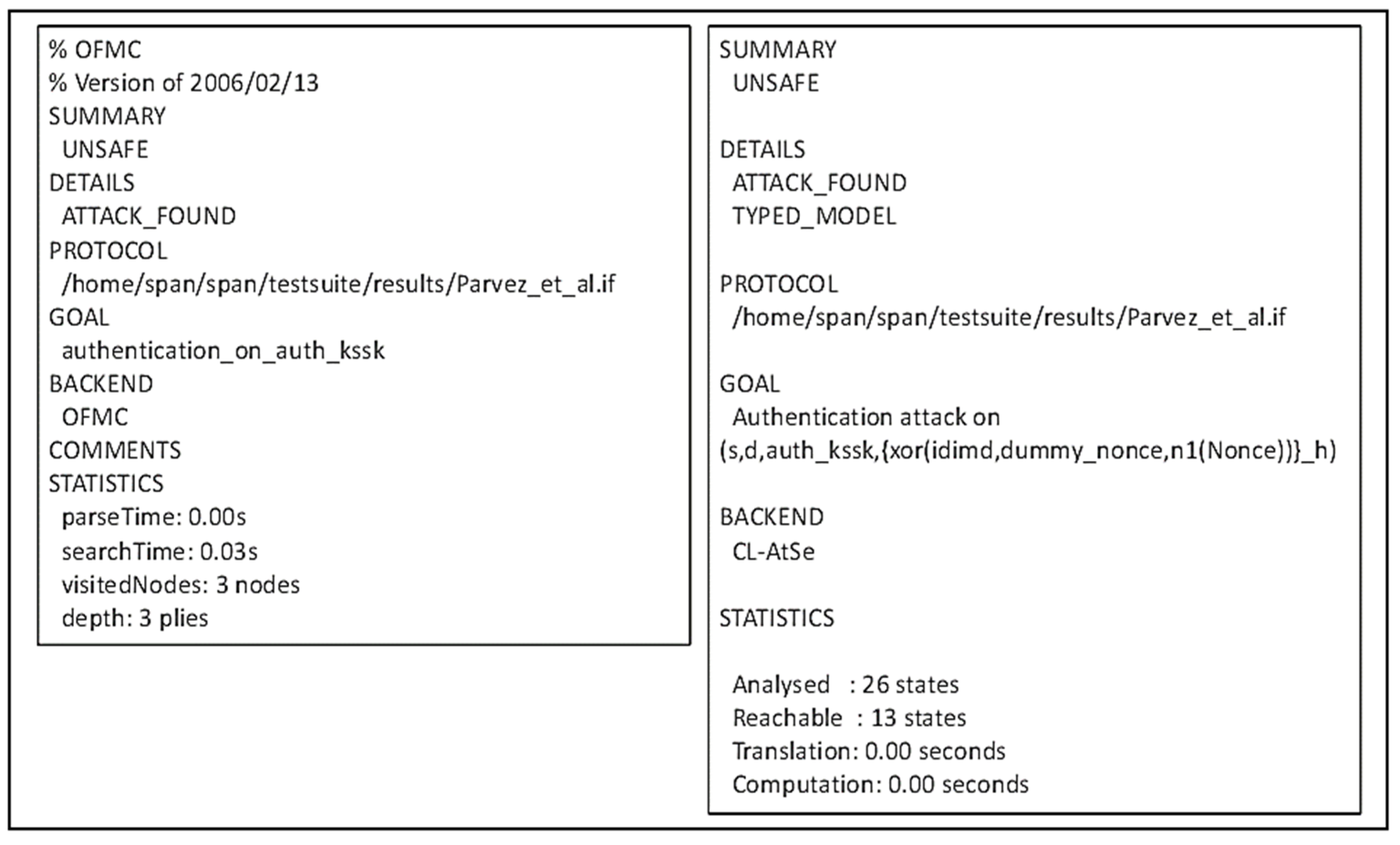
4.3.4. Parvez et al.’s Protocol
- BAN logic-based formal security analysis.
● Idealization (I1) (I2) (I3) (I4) Figure 10. Parvez et al.’s protocol. (a) Registration procedure. (b) Authentication Procedure.![Sensors 21 08383 g010]()
● Assumption (A1) (A2) (A3) (A4) (A5) (A6) (A7) (A8) (A9) (A10) (A11) (A12) (A13) (A14) ● Goals (G1) (G2) (G3) (G4) (G5) (G6) ● Derivations (D1) (D2) (D3) (D4) (D5) (D6) (I2) (D7) (D8) (D9) (D10) (D11) (D12) (D13) . (D14) (D15) (D16) (D17) (D18) (D19) (D20) (D21) (D22)
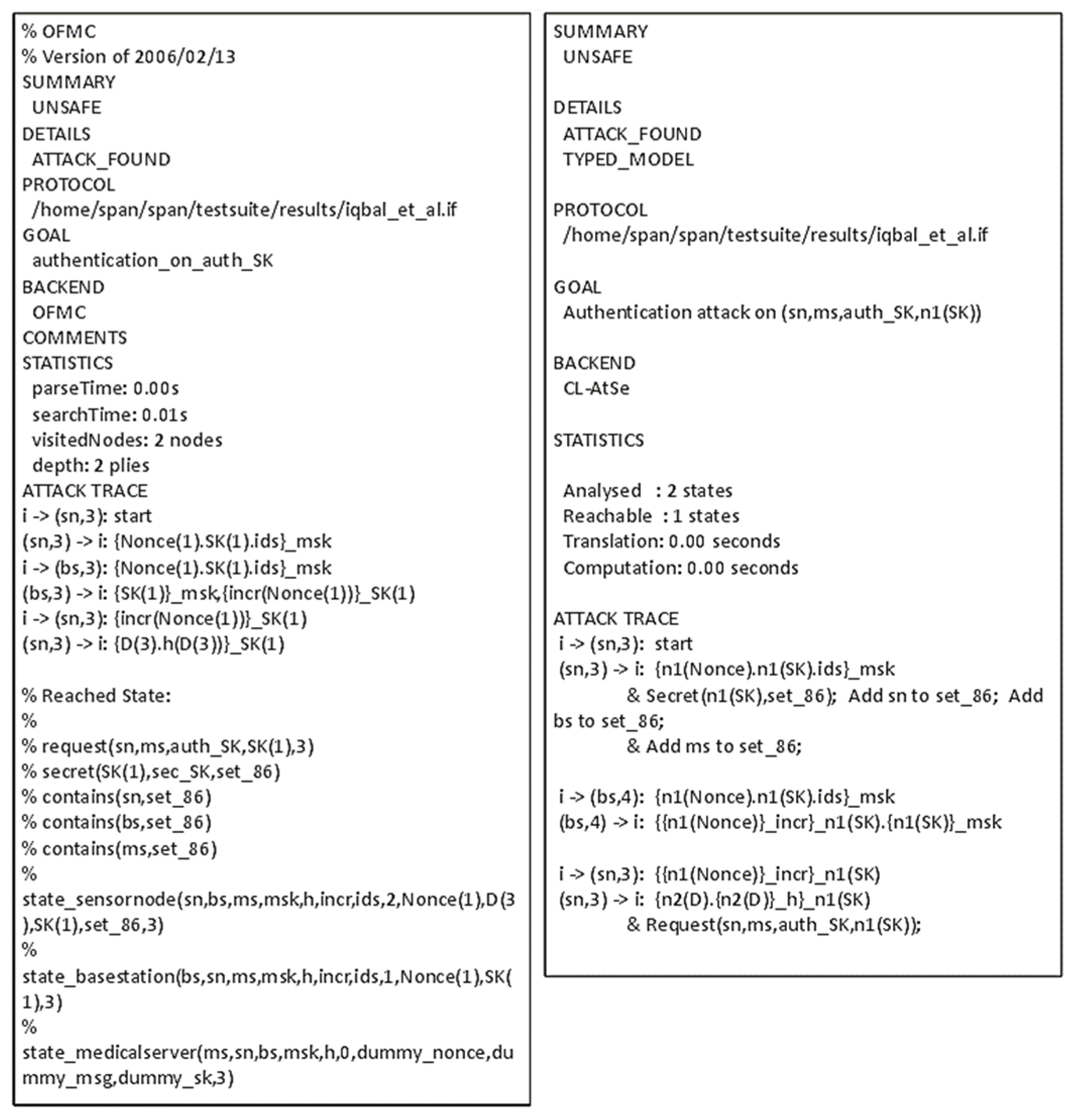
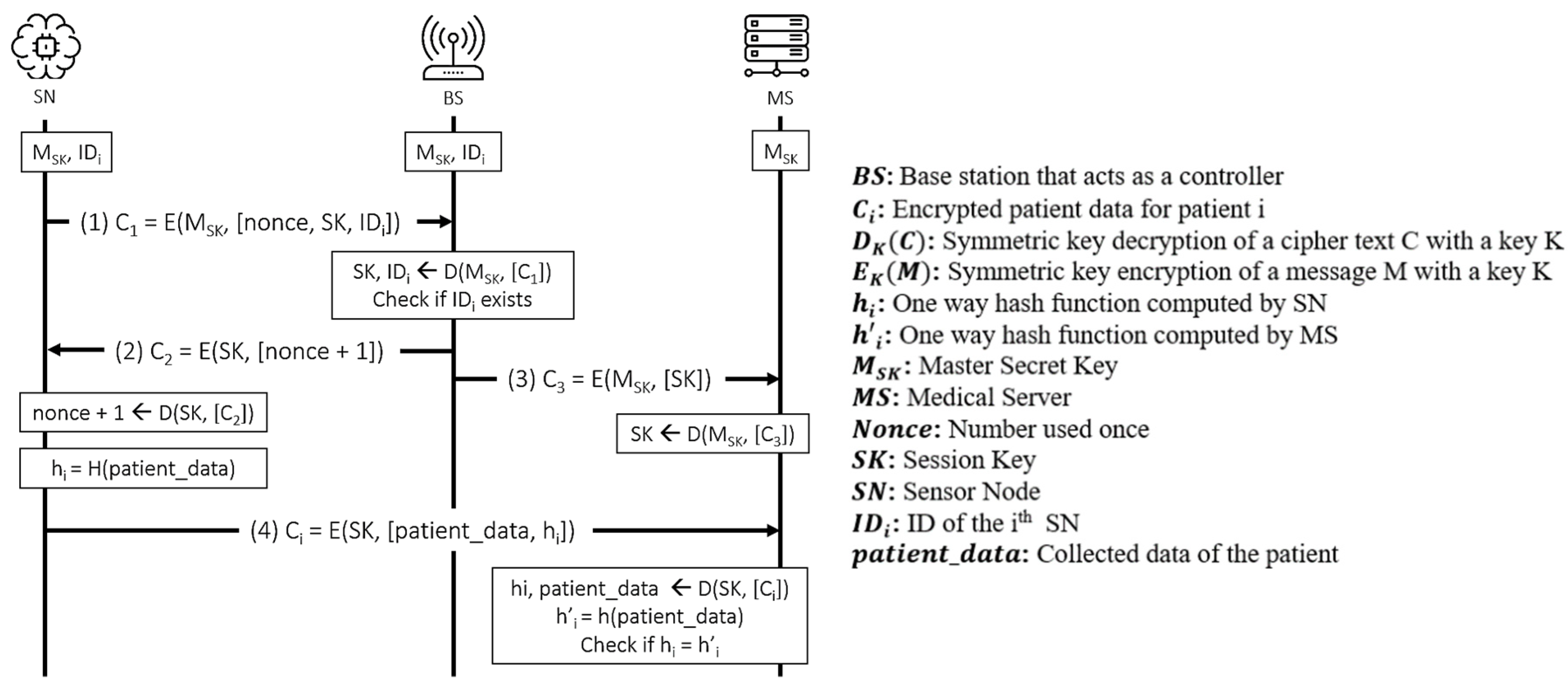
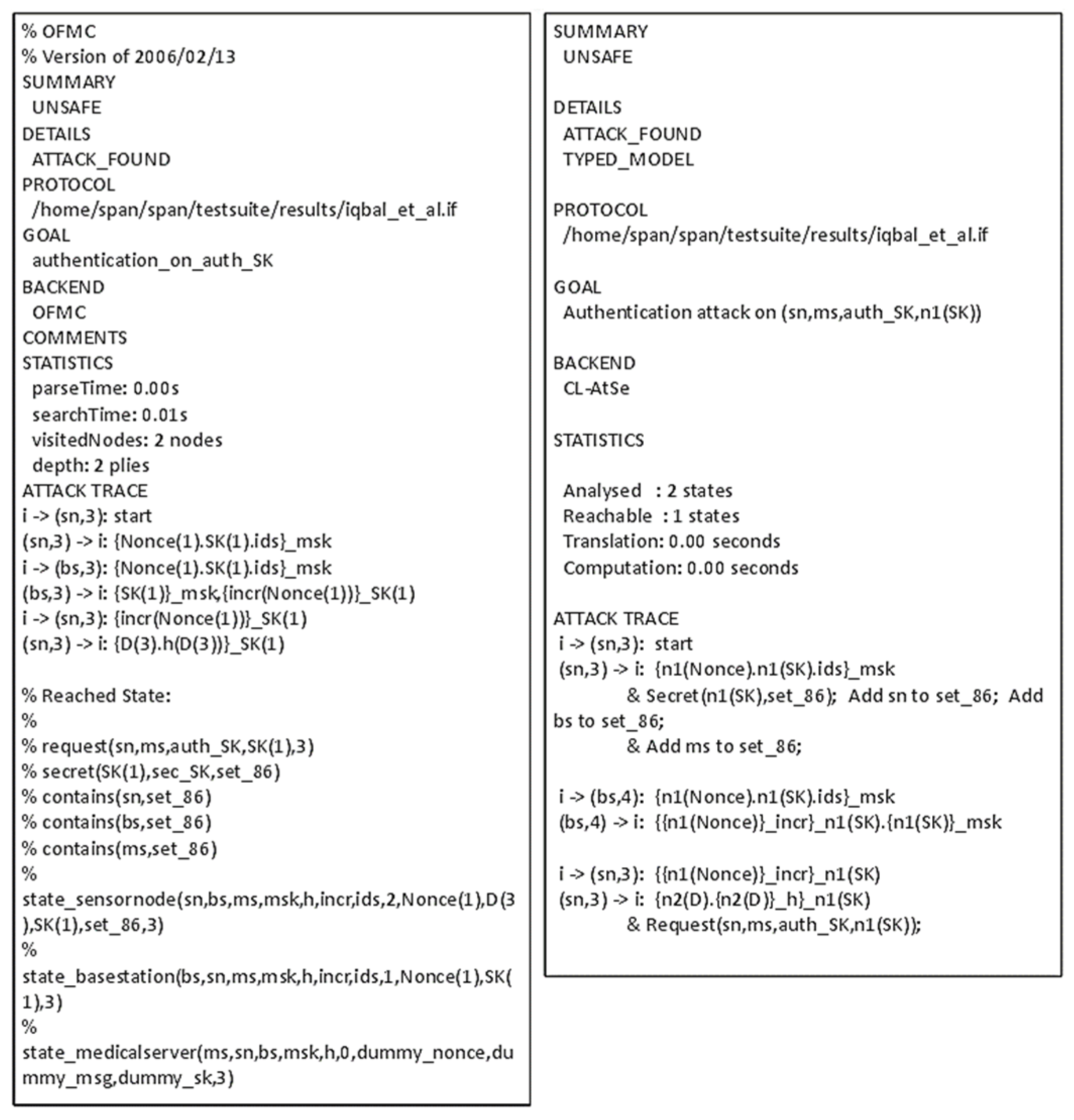
4.3.5. Iqbal et al.’s Protocol
- BAN logic-based formal security analysis
● Idealization (I1) (I2) (I3) (I4) ● Assumption (A1) (A2) (A3) (A4) (A5) (A6) ● Hypotheses (H1) (H2) ● Goals (G1) (G2) (G3) (G4) (G5) ● Derivations (D1) (D2) (D3) (D4) (D5) (D6) (I2) (D7) (D8) , FR, BC (D9) (D10) (D11) , FR (D12) By (D10), (H2), JR
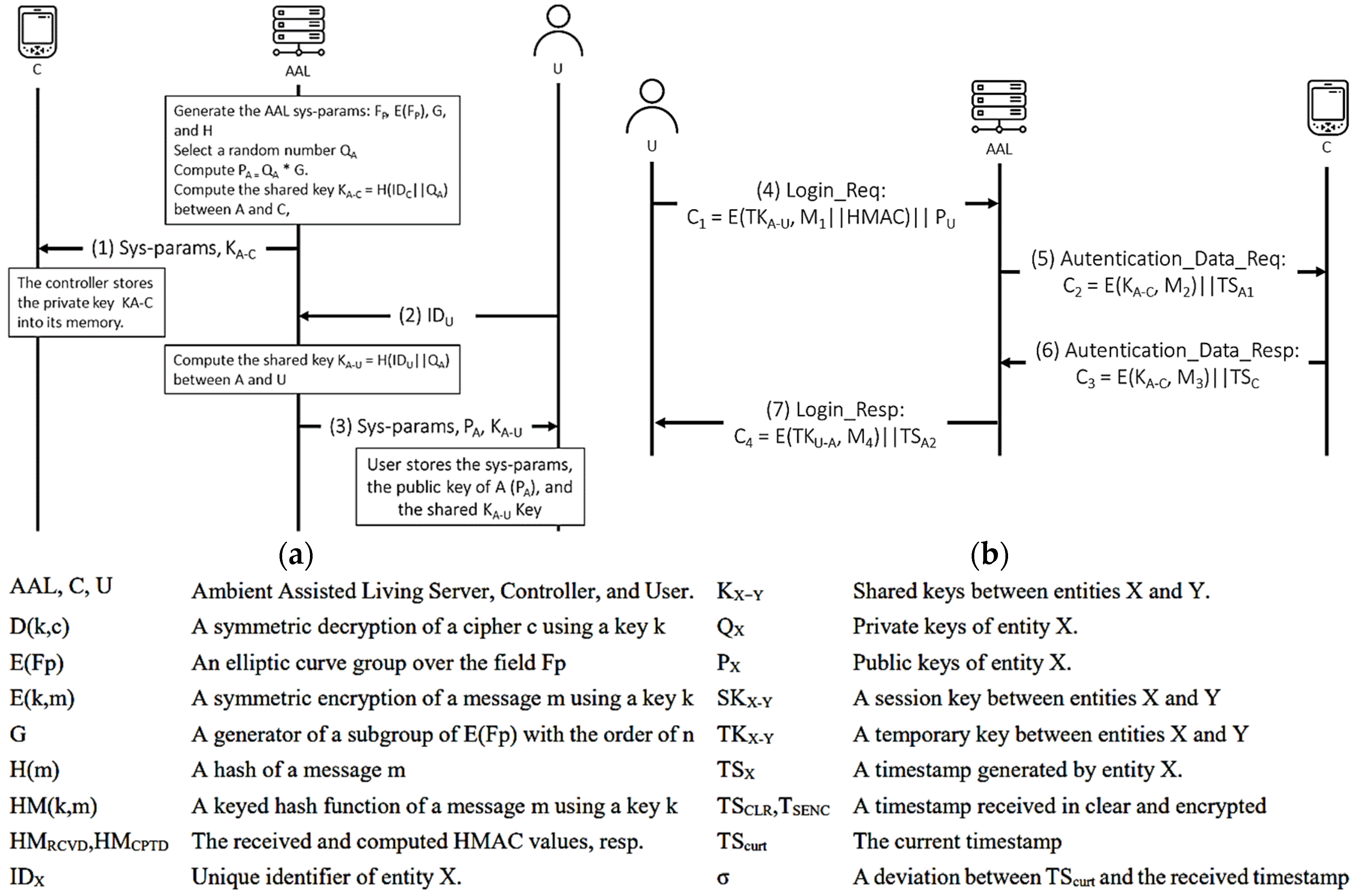
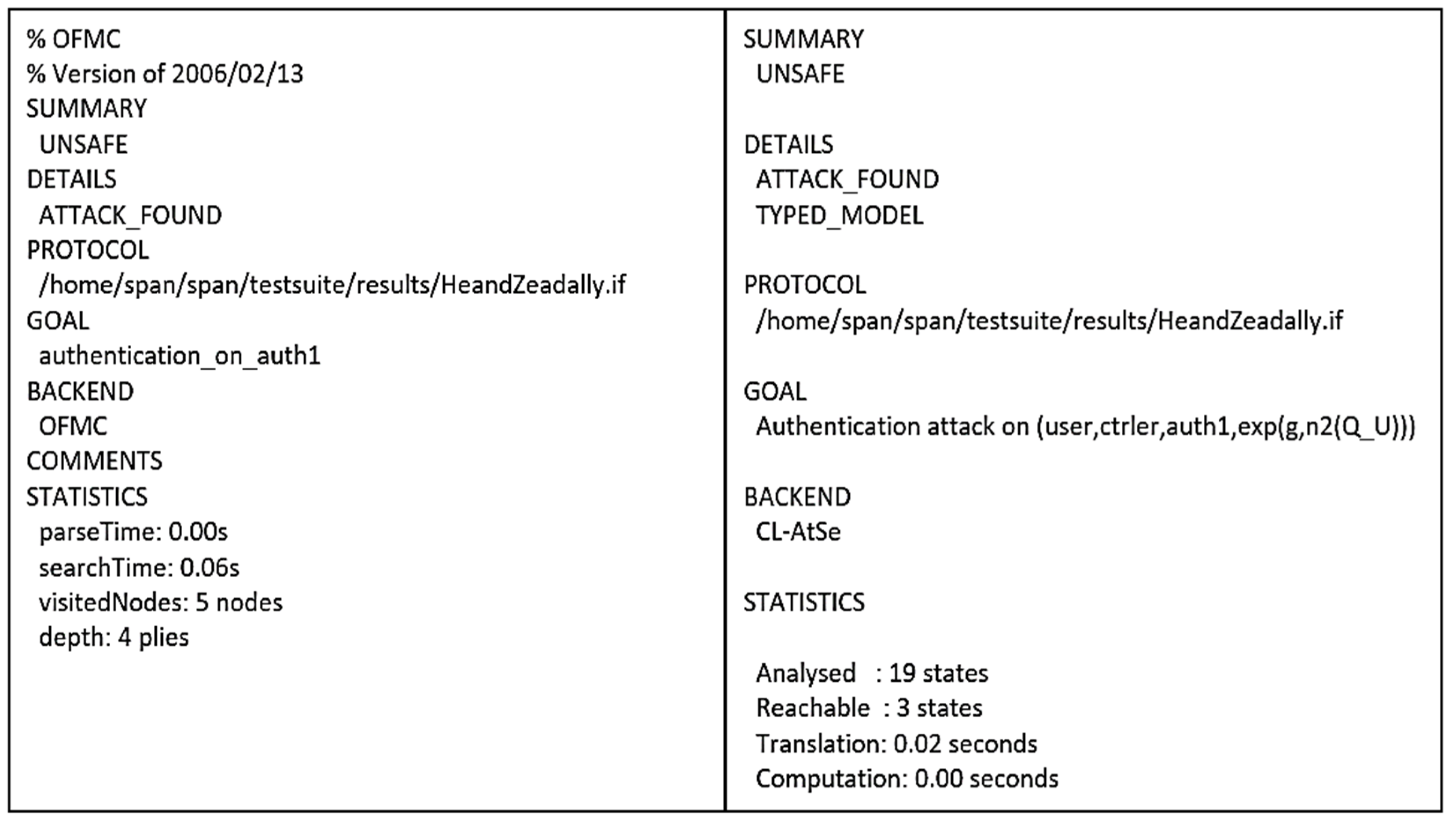
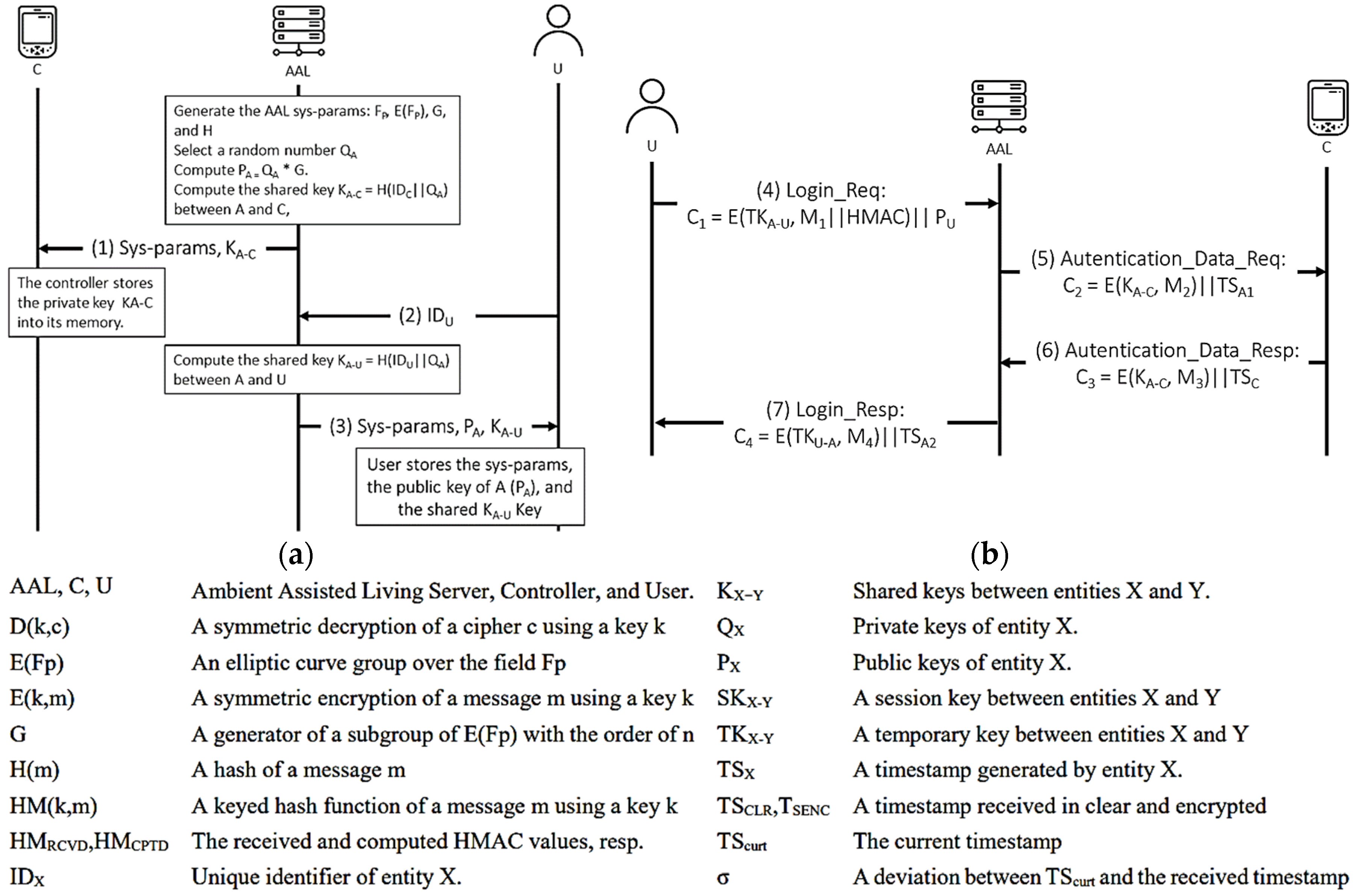
4.3.6. He and Zeadally’s Protocol
- BAN logic-based formal security analysis.
● Idealization (I1) (I2) (I3) (I4) ● Assumption (A1) (A2) (A3) (A4) (A5) (A6) (A7) (A8) (A9) (A10) (A11) Figure 14. He and Zeadally’s protocol. (a) Registration phase. (b) Authentication phase.![Sensors 21 08383 g014]()
● Hypotheses (H1) ● Goals (G1) (G2) (G3) (G4) (G5) (G6) (G7) (G8) (G9) (G10) (G11) (G12) ● Derivations (D1) , (D2) (D3) (D4) (D5) (D6) (D7) (D8) (D9) (D10) (D11) (D12) (D13) (D14) (D15) (D16) By (D13), BC, (A6), DH (D17) (D18) (D19) (D20) (D21) (D22) (D23) (D24) (D25) (D26) (D27) (D28)
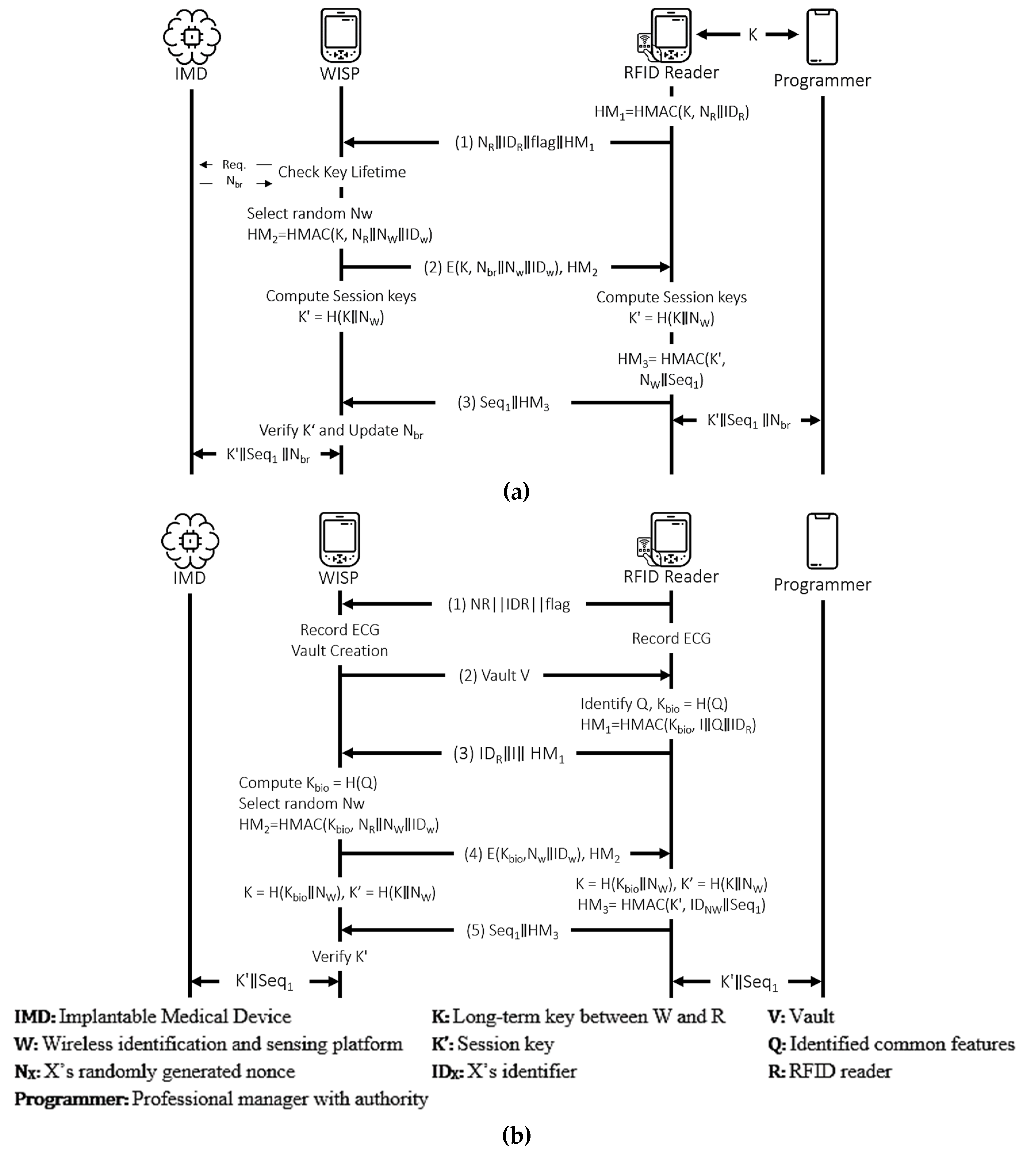
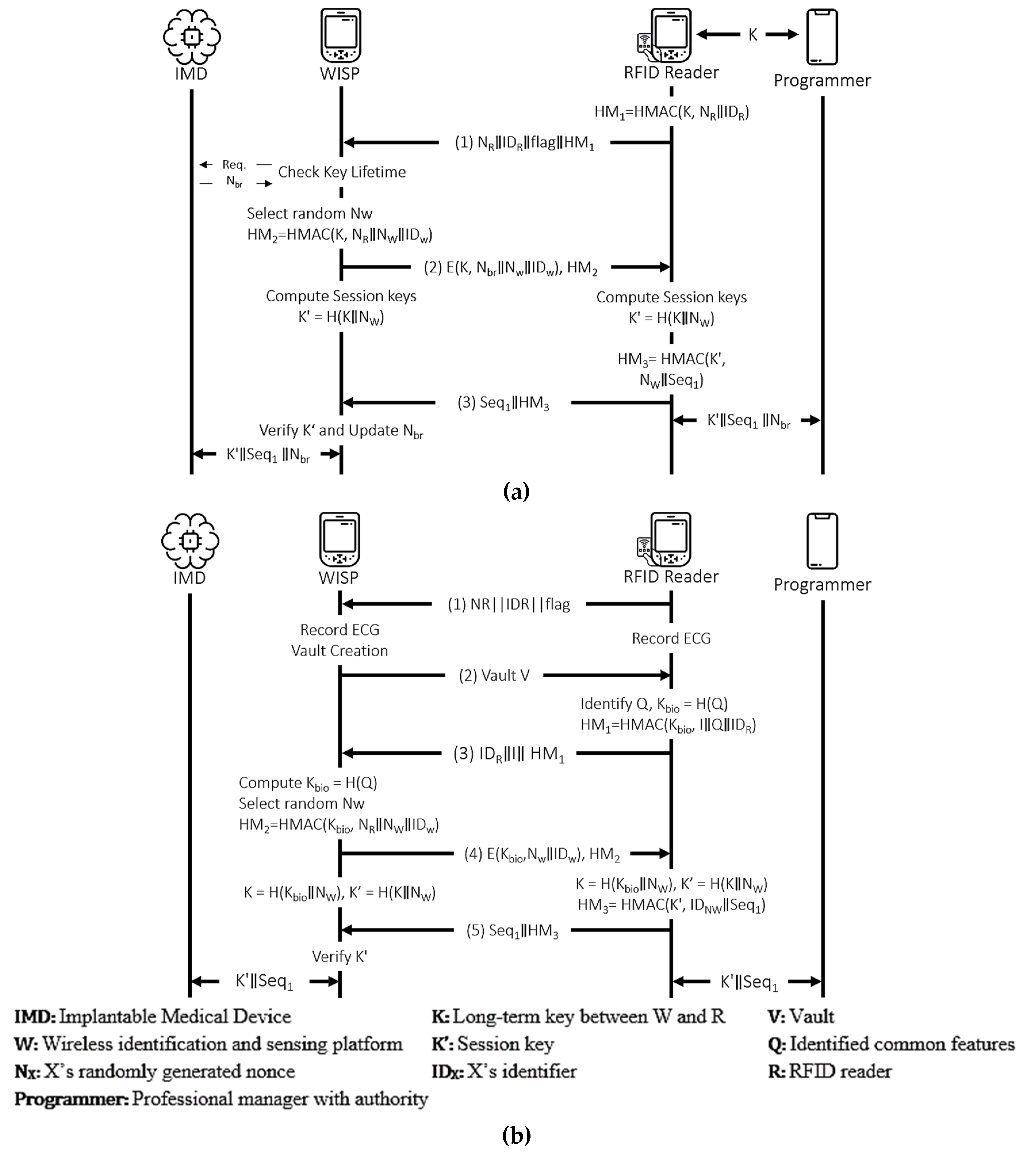
4.3.7. Ellouze et al.’s Protocol
- BAN logic-based formal security analysis.
- Regular mode.
● Idealization (I1) (I2) (I3) ● Assumption (A1) (A2) (A3) (A4) ● Hypotheses (H1) (H2) ● Goals (G1) (G2) (G3) (G4) (G5) (G6) (G7) ● Derivations (D1) (D2) (D3) (D4) (D5) (D6) (I2) (D7) (D8) (D9) (D10) (D11) (D12) (D13) By (D12), (A2), FR, NV - Emergency Mode
● Idealization (I1) (I2) (I3) Figure 16. Ellouze et al.’s protocol. (a) Regular Mode. (b) Emergency Mode.![Sensors 21 08383 g016]()
● Assumption (A1) (A2) (A3) (A4) ● Hypotheses (H1) (H2) ● Goals (G1) (G2) (G3) (G4) (G5) (G6) (G7) ● Derivations (D1) (D2) . (D3) . (D4) (D5) (D6) (I2) (D7) (D8) (D9) (D10) (D11) (I3) (D12) (D13)
5. Discussion
6. Comparative Analysis
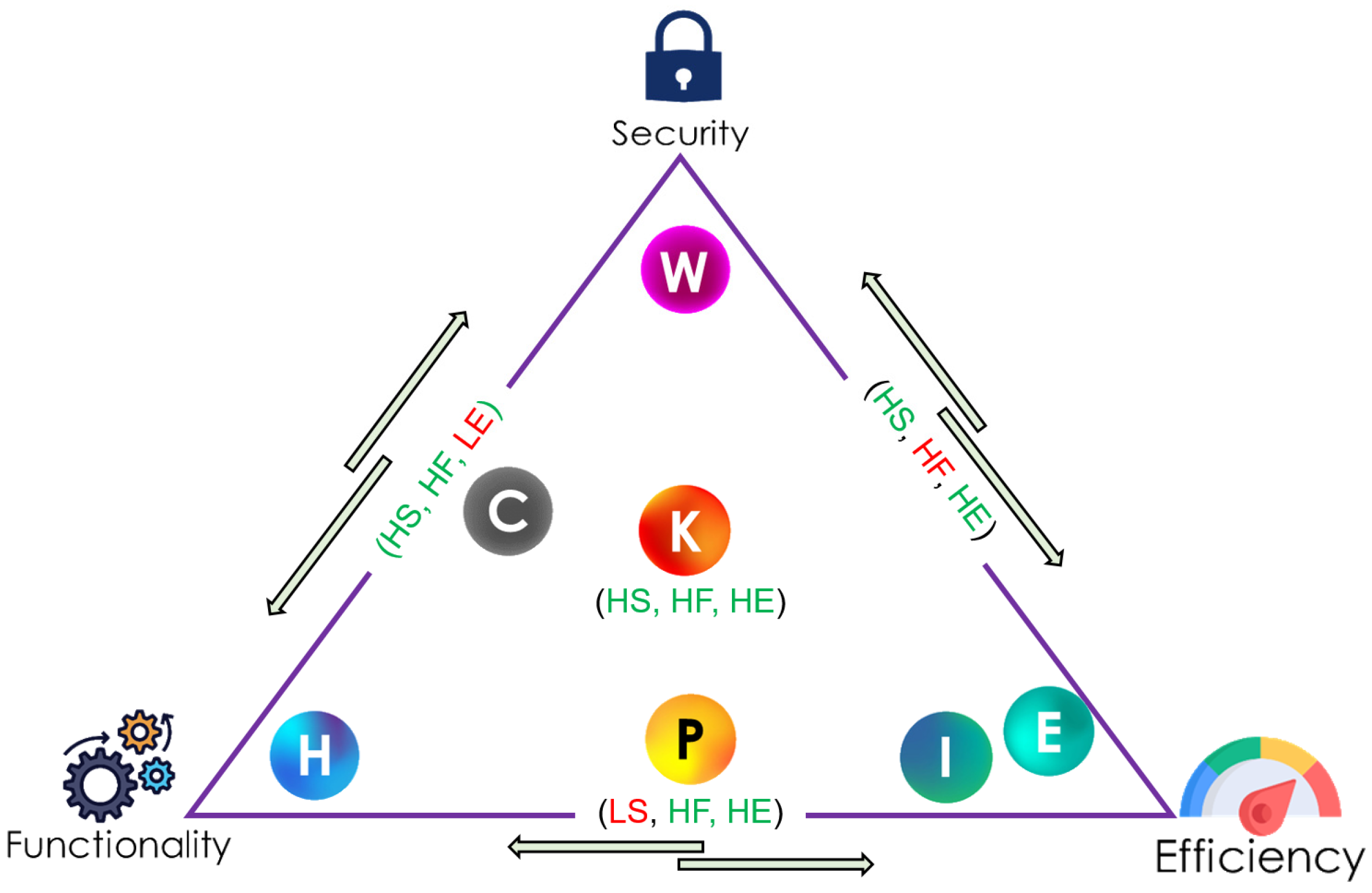
6.1. Comparison by Security Strength
6.2. Comparison by Functionality
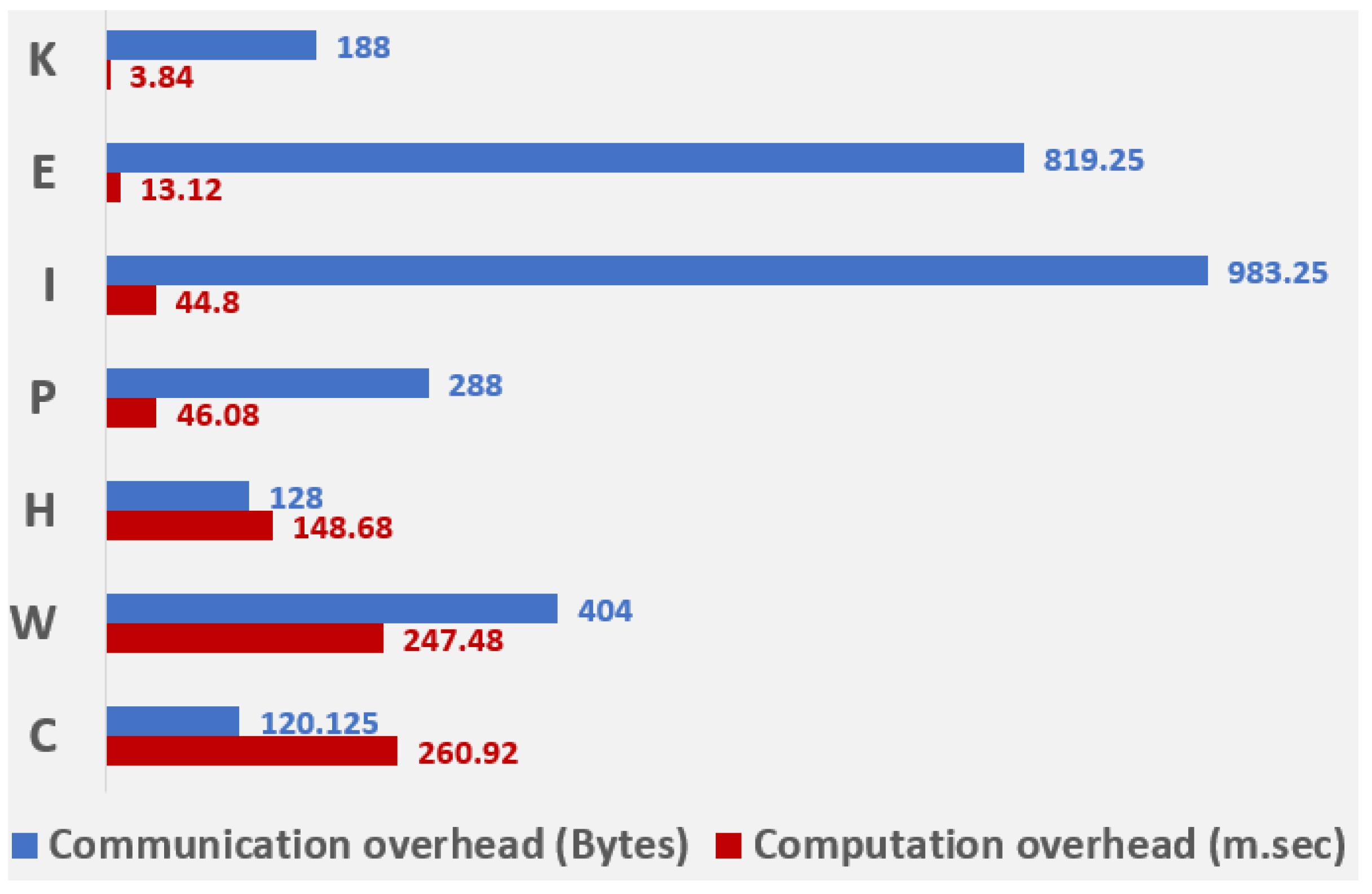
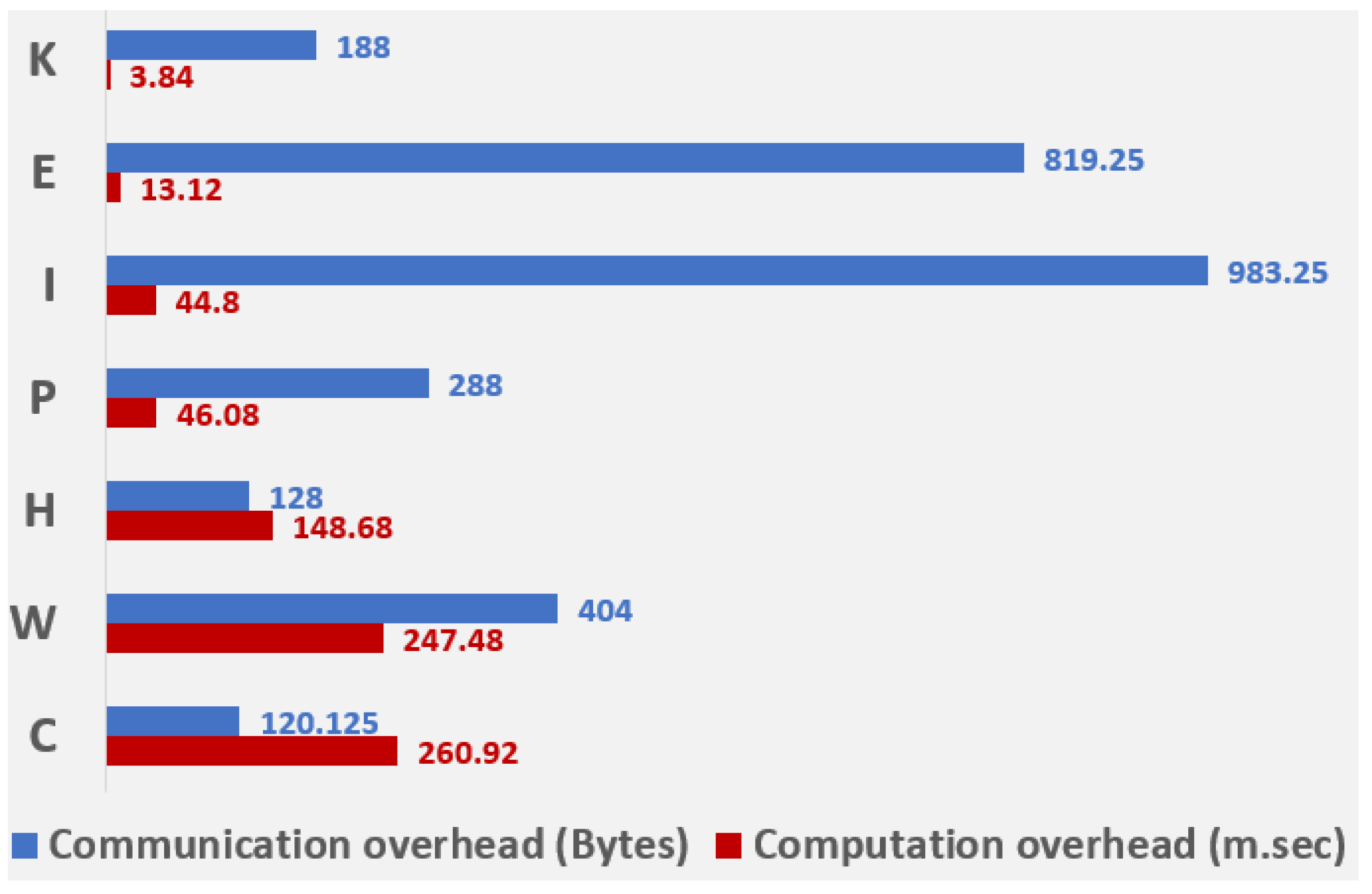
6.3. Comparison by Computational and Communicational Overhead
6.4. Overall Comparison of the Authentication Protocols
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coherent Market Insights. U.S. Implantable Medical Devices Market Analysis. 2020. Available online: https://www.coherentmarketinsights.com/market-insight/us-implantable-medical-devices-market-3853 (accessed on 20 November 2021).
- IMARC Implantable Medical Devices Market: Global Industry Trends, Share, Size, Growth, Opportunity and Forecast 2020–2025. 2020. Available online: https://www.imarcgroup.com/implantable-medical-devices-market (accessed on 20 November 2021).
- Maddock, N.A.; James, N.L.; McKenzie, D.R.; Patrick, J.F. Technological advances for polymers in active implantable medical devices. In The Design and Manufacture of Medical Devices; Elsevier: Amsterdam, The Netherlands, 2012; pp. 239–272. [Google Scholar]
- Kitana, A.; Traore, I.; Woungang, I. Towards an Epidemic SMS-based Cellular Botnet. J. Internet Serv. Inf. Secur. 2020, 10, 38–58. [Google Scholar]
- Shichkina, Y.A.; Kataeva, G.V.; Irishina, Y.A.; Stanevich, E.S. The use of mobile phones to monitor the status of patients with Parkinson’s disease. J. Wirel. Mob. Netw. Ubiquitous Comput. Dependable Appl. 2020, 11, 55–73. [Google Scholar]
- Camara, C.; Peris-Lopez, P.; Tapiador, J.E. Security and privacy issues in implantable medical devices: A comprehensive survey. J. Biomed. Inform. 2015, 55, 272–289. [Google Scholar] [CrossRef] [Green Version]
- Liu, N.; Yu, M.; Zang, W.; Sandhu, R.S. Cost and Effectiveness of TrustZone Defense and Side-Channel Attack on ARM Platform. J. Wirel. Mob. Netw. Ubiquitous Comput. Dependable Appl. 2020, 11, 1–15. [Google Scholar]
- Kasturi, G.S.; Jain, A.; Singh, J. Detection and Classification of Radio Frequency Jamming Attacks using Machine learning. J. Wirel. Mob. Netw. Ubiquitous Comput. Dependable Appl. 2020, 11, 49–62. [Google Scholar]
- Wong, S.K.; Yiu, S.-M. Location spoofing attack detection with pre-installed sensors in mobile devices. J. Wirel. Mob. Netw. Ubiquitous Comput. Dependable Appl. 2020, 11, 16–30. [Google Scholar]
- Alizadeh, M.; Andersson, K.; Schelen, O. A Survey of Secure Internet of Things in Relation to Blockchain. J. Internet Serv. Inf. Secur. 2020, 10, 47–75. [Google Scholar]
- Wong, S.K.; Yiu, S.-M. Identification of device motion status via Bluetooth discovery. J. Internet Serv. Inf. Secur. 2020, 10, 59–69. [Google Scholar]
- Rushanan, M.; Rubin, A.D.; Kune, D.F.; Swanson, C.M. Sok: Security and privacy in implantable medical devices and body area networks. In Proceedings of the 2014 IEEE Symposium on Security and Privacy, Berkeley, CA, USA, 18–21 May 2014; pp. 524–539. [Google Scholar]
- Siddiqi, M.A.; Doerr, C.; Strydis, C. Imdfence: Architecting a secure protocol for implantable medical devices. IEEE Access 2020, 8, 147948–147964. [Google Scholar] [CrossRef]
- Belkhouja, T.; Sorour, S.; Hefeida, M.S. Role-Based Hierarchical Medical Data Encryption for Implantable Medical Devices. In Proceeding of the 2019 IEEE Global Communications Conference (GLOBECOM), Waikoloa, HI, USA, 9–13 December 2019; pp. 1–6. [Google Scholar]
- Tutari, V.H.; Das, B.; Chowdhury, D.R. A Continuous Role-Based Authentication Scheme and Data Transmission Protocol for Implantable Medical Devices. In Proceedings of the 2019 Second International Conference on Advanced Computational and Communication Paradigms (ICACCP), Gangtok, India, 25–28 February 2019; pp. 1–6. [Google Scholar]
- Camara, C.; Peris-Lopez, P.; De Fuentes, J.M.; Marchal, S. Access control for implantable medical devices. IEEE Trans. Emerg. Top. Comput. 2020, 9, 1126–1138. [Google Scholar] [CrossRef]
- Zhang, Z.; Xu, X.; Han, S.; Liang, Y.; Liu, C. Wearable Proxy Device-Assisted Authentication Request Filtering for Implantable Medical Devices. In Proceedings of the 2020 IEEE Wireless Communications and Networking Conference (WCNC), Seoul, Korea, 25–28 May 2020; pp. 1–6. [Google Scholar]
- Astillo, P.V.; Choudhary, G.; Duguma, D.G.; Kim, J.; You, I. TrMAps: Trust Management in Specification-based Misbehavior Detection System for IMD-Enabled Artificial Pancreas System. IEEE J. Biomed. Health Inform. 2021, 25, 3763–3775. [Google Scholar] [CrossRef]
- Astillo, P.V.; Duguma, D.G.; Park, H.; Kim, J.; Kim, B.; You, I. Federated intelligence of anomaly detection agent in IoTMD-enabled Diabetes Management Control System. Futur. Gener. Comput. Syst. 2021, 128, 395–405. [Google Scholar] [CrossRef]
- Abhishta, A.; van Heeswijk, W.; Junger, M.; Nieuwenhuis, L.J.M.; Joosten, R. Why would we get attacked? An analysis of attacker’s aims behind DDoS attacks. J. Wirel. Mob. Netw. Ubiquitous Comput. Dependable Appl. 2020, 11, 3–22. [Google Scholar]
- Burrows, M.; Abadi, M.; Needham, R.M. A logic of authentication. Proc. R. Soc. Lond. A. Math. Phys. Sci. 1989, 426, 233–271. [Google Scholar]
- Armando, A.; Basin, D.; Boichut, Y.; Chevalier, Y.; Compagna, L.; Cuéllar, J.; Drielsma, P.H.; Héam, P.-C.; Kouchnarenko, O.; Mantovani, J.; et al. The AVISPA tool for the automated validation of internet security protocols and applications. In International Conference on Computer Aided Verification; Springer: Berlin/Heidelberg, Germany, 2005; pp. 281–285. [Google Scholar]
- Khan, H.; Dowling, B.; Martin, K.M. Highly efficient privacy-preserving key agreement for wireless body area Networks. In Proceedings of the 2018 17th IEEE International Conference On Trust, Security And Privacy in Computing and Communications/12th IEEE International Conference On Big Data Science And Engineering (TrustCom/BigDataSE), New York, NY, USA, 1–3 August 2018; pp. 1064–1069. [Google Scholar]
- Wu, L.; Chi, H.; Du, X. A Secure Proxy-based Access Control Scheme for Implantable Medical Devices. arXiv 2018, arXiv1803.07751. [Google Scholar]
- Chi, H.; Wu, L.; Du, X.; Zeng, Q.; Ratazzi, P. e-SAFE: Secure, efficient and forensics-enabled access to implantable medical devices. In Proceedings of the 2018 IEEE Conference on Communications and Network Security (CNS), Beijing, China, 30 May–1 June 2018; pp. 1–9. [Google Scholar]
- Parvez, K.; Zohra, F.T.; Jahan, M. A secure and lightweight user authentication mechanism for wireless body area network. In Proceedings of the 6th International Conference on Networking, Systems and Security, Dhaka, Bangladesh, 17–19 December 2019; pp. 139–143. [Google Scholar]
- Iqbal, J.; Umar, A.I.; ul Amin, N.; Din, N. Efficient Key Agreement and Nodes Authentication Scheme for Body Sensor Networks. Int. J. Adv. Comput. Sci. Appl. 2017, 8, 180–187. [Google Scholar] [CrossRef]
- He, D.; Zeadally, S. Authentication protocol for an ambient assisted living system. IEEE Commun. Mag. 2015, 53, 71–77. [Google Scholar]
- Ellouze, N.; Allouche, M.; Ben Ahmed, H.; Rekhis, S.; Boudriga, N. Securing implantable cardiac medical devices: Use of radio frequency energy harvesting. In Proceedings of the 3rd International Workshop on Trustworthy Embedded Devices, Berlin, Germany, 4 November 2013; pp. 35–42. [Google Scholar]
- Fu, C.; Du, X.; Wu, L.; Zeng, Q.; Mohamed, A.; Guizani, M. Poks based secure and energy-efficient access control for implantable medical devices. In International Conference on Security and Privacy in Communication Systems; Springer: Cham, Switzerland, 2019; pp. 105–125. [Google Scholar]
- Antonescu, B.; Basagni, S. Wireless body area networks: Challenges, trends and emerging technologies. In Proceedings of the 8th International Conference on Body Area Networks, Boston, MA, USA, 30 September–2 October 2013; pp. 1–7. [Google Scholar]
- Ellouze, N.; Allouche, M.; Ahmed, H.B.; Rekhis, S.; Boudriga, N. Security of implantable medical devices: Limits, requirements, and proposals. Secur. Commun. Netw. 2014, 7, 2475–2491. [Google Scholar] [CrossRef]
- Amar, A.B.; Kouki, A.B.; Cao, H. Power approaches for implantable medical devices. Sensors 2015, 15, 28889–28914. [Google Scholar] [CrossRef]
- Islam, M.N.; Yuce, M.R. Review of medical implant communication system (MICS) band and network. ICT Express 2016, 2, 188–194. [Google Scholar] [CrossRef] [Green Version]
- Strydis, C.; Seepers, R.M.; Peris-Lopez, P.; Siskos, D.; Sourdis, I. A system architecture, processor, and communication protocol for secure implants. ACM Trans. Archit. Code Optim. 2013, 10, 57. [Google Scholar] [CrossRef]
- He, D.; Zeadally, S.; Kumar, N.; Lee, J.-H. Anonymous authentication for wireless body area networks with provable security. IEEE Syst. J. 2016, 11, 2590–2601. [Google Scholar] [CrossRef]
- Halperin, D.; Heydt-Benjamin, T.S.; Ransford, B.; Clark, S.S.; Defend, B.; Morgan, W.; Fu, K.; Kohno, T.; Maisel, W.H. Pacemakers and Implantable Cardiac Defibrillators: Software Radio Attacks and Zero-Power Defenses. In Proceedings of the 2008 IEEE Symposium on Security and Privacy (SP 2008), Oakland, CA, USA, 18–22 May 2008; pp. 129–142. [Google Scholar]
- Burleson, W.; Clark, S.S.; Ransford, B.; Fu, K. Design challenges for secure implantable medical devices. In Proceedings of the DAC Design Automation Conference 2012, San Francisco, CA, USA, 3–7 June 2012; pp. 12–17. [Google Scholar]
- Zheng, G.; Shankaran, R.; Orgun, M.A.; Qiao, L.; Saleem, K. Ideas and challenges for securing wireless implantable medical devices: A review. IEEE Sens. J. 2016, 17, 562–576. [Google Scholar] [CrossRef]
- Gollakota, S.; Hassanieh, H.; Ransford, B.; Katabi, D.; Fu, K. They can hear your heartbeats: Non-invasive security for implantable medical devices. In Proceedings of the ACM SIGCOMM 2011 Conference, Toronto, ON, Canada, 15–19 August 2011; pp. 2–13. [Google Scholar]
- Duguma, D.G.; Kim, J.; Kim, B.; You, I. A Formal Security Verification on He and Zeadally’s Authentication Protocol for IMD-Enabled Ambient Assisted Living System. In Proceedings of the 2020 ACM International Conference on Intelligent Computing and its Emerging Applications, GangWon, Korea, 12–15 December 2020; pp. 1–6. [Google Scholar]
- Kim, J.; Lee, S.; Duguma, D.G.; Kim, B.; You, I. Comments on” Securing implantable cardiac medical devices” Use of radio frequency energy harvesting. In Proceedings of the 2020 ACM International Conference on Intelligent Computing and its Emerging Applications, GangWon, Korea, 12–15 December 2020; pp. 1–5. [Google Scholar]
- Boyd, C.; Mao, W. On a Limitation of BAN Logic. In Workshop on the Theory and Application of of Cryptographic Techniques; Springer: Berlin/Heidelberg, Germany, 1993; pp. 240–247. [Google Scholar]
- Von Oheimb, D. The high-level protocol specification language HLPSL developed in the EU project AVISPA. In Proceedings of the APPSEM 2005 Workshop, Frauenchiemsee, Germany, 12–15 September 2005; pp. 1–17. [Google Scholar]
- Al-Turjman, F.; Alturjman, S. Context-sensitive access in industrial internet of things (IIoT) healthcare applications. IEEE Trans. Ind. Inform. 2018, 14, 2736–2744. [Google Scholar] [CrossRef]
- Challa, S.; Wazid, M.; Das, A.K.; Khan, M.K. Authentication protocols for implantable medical devices: Taxonomy, analysis and future directions. IEEE Consum. Electron. Mag. 2017, 7, 57–65. [Google Scholar] [CrossRef]
- Saho, N.J.G.; Ezin, E.C. Comparative Study on the Performance of Elliptic Curve Cryptography Algorithms with Cryptography through RSA Algorithm. In Proceedings of the CARI 2020-Colloque Africain sur la Recherche en Informatique et en Mathématiques Apliquées, Thiès, Senegal, 22 September–2 October 2020. [Google Scholar]
- Fog, A. Instruction tables: Lists of Instruction latencies, Throughputs and Micro-Operation Breakdowns for Intel, AMD and VIA CPUs. Available online: https://www.agner.org/optimize/instruction_tables (accessed on 20 November 2021).
- FM4DD. X509 Certificate Examples for Testing and Verification. Available online: http://fm4dd.com/openssl/certexamples.htm (accessed on 20 November 2021).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Notation | Meaning |
|---|---|
| M believes that the message U is true | |
| M receives the message U at any point in time | |
| M previously sent the message U | |
| M has jurisdiction over U | |
| U is fresh | |
| S is a secret key shared between M and N | |
| S is the M’s public key | |
| S is a shared secret between M and N. | |
| U is encrypted with a key K | |
| U is combined with V |
| Rule Name | Rule |
|---|---|
| Message Meaning Rule (MM) | |
| Nonce Verification (NV) Rule | |
| Jurisdiction (JR) Rule | |
| Freshness (FR) Rule | |
| Decomposition (DR) Rule | |
| Belief Conjunction (BC) Rule | |
| Diffie–Hellman (DH) Rule |
| Notation | INT | CNF | AUT | SKA | PFS | RAP |
|---|---|---|---|---|---|---|
| Khan et. al | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Wu et. al. | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Chi et. al. | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Parvez et al. | ✗ | ∆ | ✓ | ✓ | ✓ | ✗ |
| Iqbal et. al. | ✗ | ✗ | ✓ | ✓ | ✗ | ✗ |
| He and Zeadally | ∆ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Ellouze et. al. | ∆ | ∆ | ✓ | ✓ | ∆ | ✓ |
| Notation | EMA | KUM | ADP | APP | ANO |
|---|---|---|---|---|---|
| Khan et. al | ✗ | ✗ | A | Generic | ✓ |
| Wu et. al. | ✗ | ✗ | A | Generic | ✗ |
| Chi et. al. | ✓ | ✗ | A | Generic | ✓ |
| Parvez et al. | ✗ | ✗ | A | Generic | ✓ |
| Iqbal et. al. | ✗ | ✗ | A+ | Generic | ✗ |
| He and Zeadally | ✗ | ✗ | A+ | Generic | ✓ |
| Ellouze et. al. | ✓ | ✗ | A- | Specific | ✗ |
| Notation | Meaning | Computational Time |
|---|---|---|
| TH | Cryptographic hash function | 0.32 |
| TSE | Symmetric encryption | 5.6 |
| TSD | Symmetric decryption | 5.6 |
| TEM | Elliptic curve point multiplication | 63 |
| TAE | Asymmetric encryption | 62 |
| TAD | Asymmetric decryption | 36 |
| TSIGN | RSA-1024 digital signature | 7 |
| TVER | RSA-1024 digital signature verification | ~0 |
| TXOR | Bitwise XOR operation | 0.32 |
| Message Type | Message Length |
|---|---|
| Public key size for an RSA encryption | 1024 |
| Length of an RSA Signature | 1024 |
| RSA-1024 digital Certificate | 602 |
| Elliptic curve point | 320 |
| Cryptographic hash function (SHA-1) | 160 |
| Key size for AES encryption | 128 |
| Identity | 32 |
| Timestamp | 32 |
| Sequence number | 32 |
| Symmetric decryption | 32 |
| Protocol | Overhead | Time (Milliseconds) |
|---|---|---|
| Khan et. al | 12TH + 23TXOR | 3.84 |
| Wu et. al. | 9TH + 3TSE +3TSD + 1TAE +1TAD + 2TSIGN + 2TVER | 247.48 |
| Chi et. al. | 16TH + 4TSE + 4TSD + 1TAE +1TAD + 2TSIGN + 2TV ER | 260.92 |
| Parvez et al. | 4TH + 4TSE + 4TSD | 46.08 |
| Iqbal et. al. | 4TSE + 4TSD | 44.80 |
| He and Zeadally. | 4TH + 4TSE + 4TSD + 6TEM | 148.68 |
| Ellouze et. al. | 6TH + 1TSE + 1TSD | 13.12 |
| Protocol | Roundtrips | Overheads (Bits) |
|---|---|---|
| Khan et. al | 2 | 1504 |
| Wu et. al. | 6 | 6554 |
| Chi et. al. | 9 | 7866 |
| Parvez et al. | 3.5 | 2304 |
| Iqbal et. al. | 2 | 1024 |
| He and Zeadally. | 3.5 | 3232 |
| Ellouze et. al. | 3 | 961 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duguma, D.G.; You, I.; Gebremariam, Y.E.; Kim, J. Can Formal Security Verification Really Be Optional? Scrutinizing the Security of IMD Authentication Protocols. Sensors 2021, 21, 8383. https://doi.org/10.3390/s21248383
Duguma DG, You I, Gebremariam YE, Kim J. Can Formal Security Verification Really Be Optional? Scrutinizing the Security of IMD Authentication Protocols. Sensors. 2021; 21(24):8383. https://doi.org/10.3390/s21248383
Chicago/Turabian StyleDuguma, Daniel Gerbi, Ilsun You, Yonas Engida Gebremariam, and Jiyoon Kim. 2021. "Can Formal Security Verification Really Be Optional? Scrutinizing the Security of IMD Authentication Protocols" Sensors 21, no. 24: 8383. https://doi.org/10.3390/s21248383
APA StyleDuguma, D. G., You, I., Gebremariam, Y. E., & Kim, J. (2021). Can Formal Security Verification Really Be Optional? Scrutinizing the Security of IMD Authentication Protocols. Sensors, 21(24), 8383. https://doi.org/10.3390/s21248383