Estimating the Effects of Awareness on Neck-Muscle Loading in Frontal Impacts with EMG and MC Sensors

Abstract
1. Introduction
2. Materials and Methods
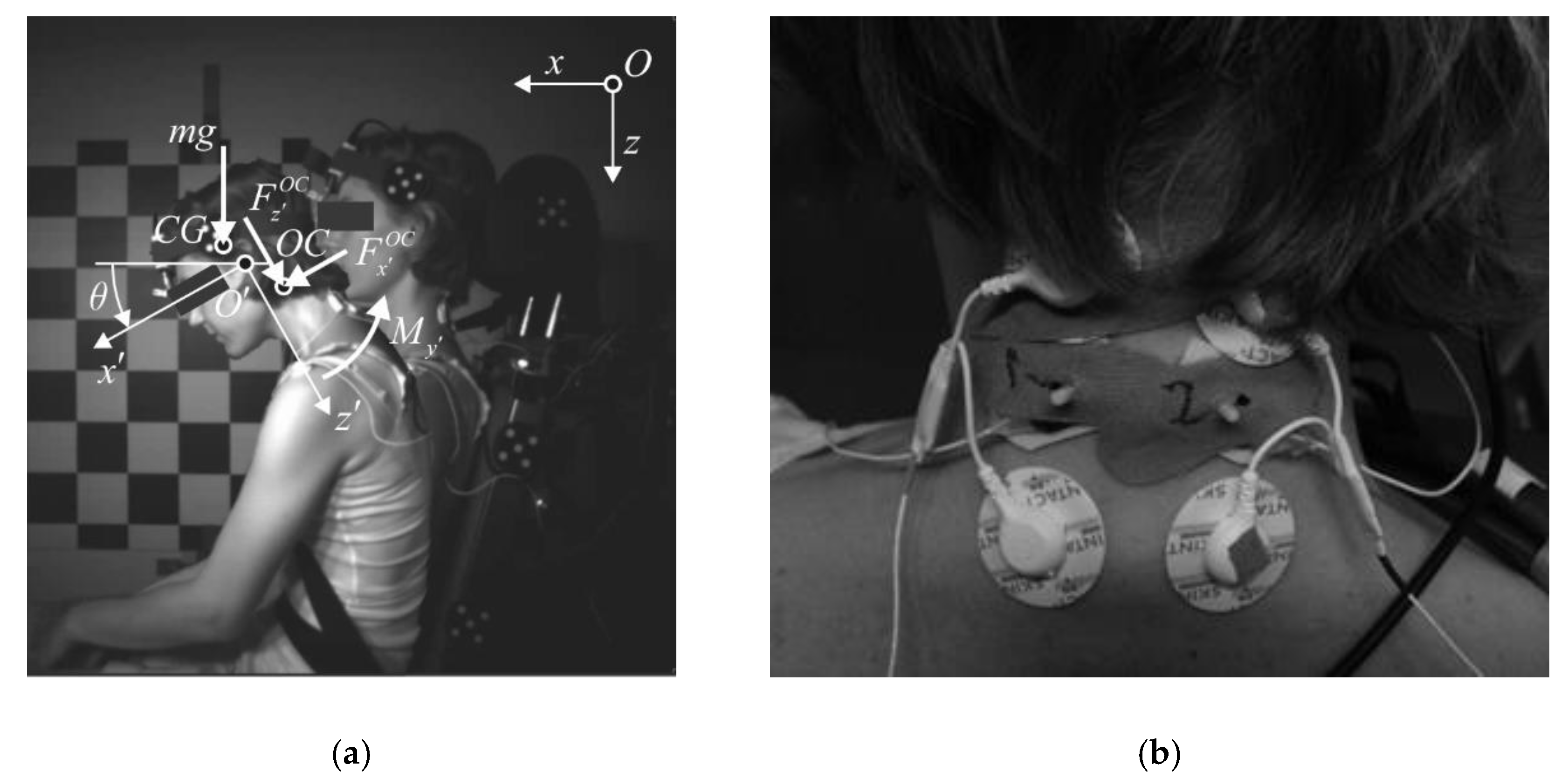
2.1. Experiment Setup
2.2. Analysis of the Dynamic Response
2.3. Statistical Analysis
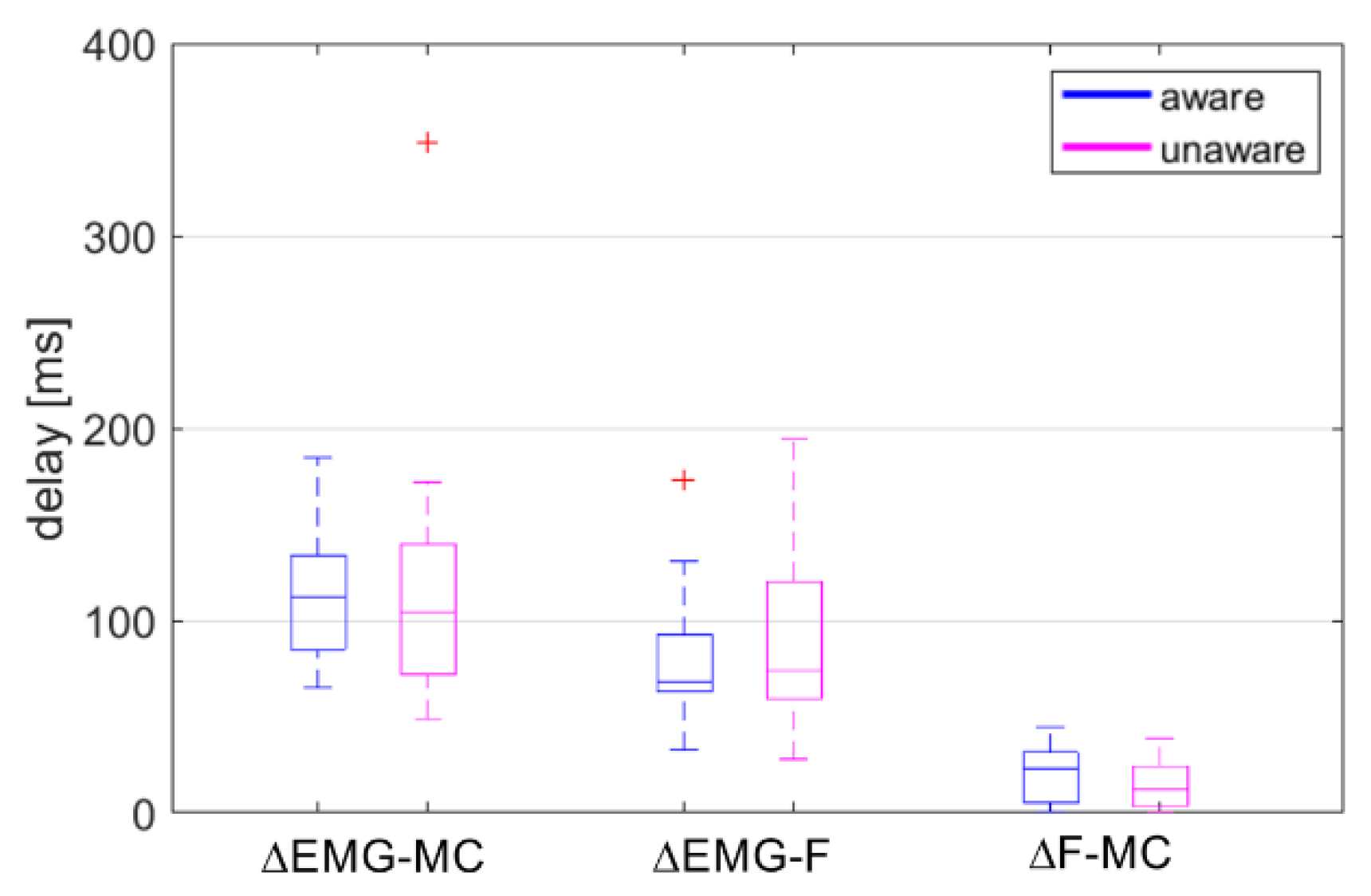
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kato, D.; Nakahira, Y.; Atsumi, N.; Iwamoto, M. Development of human-body model THUMS Version 6 containing muscle controllers and application to injury analysis in frontal collision after brake deceleration. In Proceedings of the IRCOBI Conference, Athens, Greece, 12–14 September 2018. [Google Scholar]
- Correia, M.A.; McLachlin, S.D.; Cronin, D.S. Optimization of muscle activation schemes in a finite element neck model simulating volunteer frontal impact scenarios. J. Biomech. 2020, 104, 109754. [Google Scholar] [CrossRef]
- Putra, I.P.A.; Iraeus, J.; Thomson, R.; Svensson, M.Y.; Linder, A.; Sato, F. Comparison of control strategies for the cervical muscles of an average female head-neck finite element model. Traffic Inj. Prev. 2019, 20 (Suppl. 2), 116–122. [Google Scholar] [CrossRef]
- Yeomans, J.S.; Li, L.; Scott, B.W.; Frankland, P.W. Tactile, acoustic and vestibular systems sum to elicit the startle reflex. Neurosci. Biobehav. Rev. 2002, 26, 1–11. [Google Scholar] [CrossRef]
- Mathews, E.A.; Balasubramanian, S.; Seacrist, T.; Maltese, M.R.; Sterner, R.; Arbogast, K.B. Electromyography responses of pediatric and young adult volunteers in low-speed frontal impacts. J. Electromyogr. Kinesiol. 2013, 23, 1206–1214. [Google Scholar] [CrossRef] [PubMed]
- Han, M.; Choi, H.Y. Elbow joint model with active muscle force. J. Mech. Sci. Technol. 2016, 30, 5847–5853. [Google Scholar] [CrossRef]
- Blouin, J.-S.; Descarreaux, M.; Bélanger-Gravel, A.; Simoneau, M.; Teasdale, N. Attenuation of human neck muscle activity following repeated imposed trunk-forward linear acceleration. Exp. Brain Res. 2003, 150, 458–464. [Google Scholar] [CrossRef]
- Siegmund, G.P.; Inglis, J.T.; Sanderson, D.J. Startle response of human neck muscles sculpted by readiness to perform ballistic head movements. J. Physiol. 2001, 535, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Aruin, A. The organization of anticipatory postural adjustments. J. Autom. Control 2002, 12, 31–37. [Google Scholar] [CrossRef]
- Östh, J.; Eliasson, E.; Happee, R.; Brolin, K. A method to model anticipatory postural control in driver braking events. Gait Posture 2014, 40, 664–669. [Google Scholar] [CrossRef]
- Beeman, S.M.; Kemper, A.R.; Madigan, M.L.; Duma, S.M. Effects of bracing on human kinematics in low-speed frontal sled tests. Ann. Biomed. Eng. 2011, 39, 2998–3010. [Google Scholar] [CrossRef]
- Beeman, S.M.; Kemper, A.R.; Madigan, M.L.; Franck, C.T.; Loftus, S.C. Occupant kinematics in low-speed frontal sled tests: Human volunteers, Hybrid III ATD, and PMHS. Accid. Anal. Prev. 2012, 47, 128–139. [Google Scholar] [CrossRef] [PubMed]
- Beeman, S.M.; Kemper, A.R.; Duma, S.M. Neck forces and moments of human volunteers and post mortem human surrogates in low-speed frontal sled tests. Traffic Inj. Prev. 2016, 17 (Suppl. 1), 141–149. [Google Scholar] [CrossRef]
- Kumar, S.; Narayan, Y.; Amell, T. Analysis of low velocity frontal impacts. Clin. Biomech. 2003, 18, 694–703. [Google Scholar] [CrossRef]
- Ejima, S.; Ono, K.; Holcombe, S.; Kaneoka, K.; Fukushima, M. A study on occupant kinematics behaviour and muscle activities during pre-impact braking based on volunteer tests. In Proceedings of the IRCOBI Conference, Maastricht, The Netherlands, 19–21 September 2007; pp. 31–45. [Google Scholar]
- Ejima, S.; Zama, Y.; Ono, K.; Kaneoka, K.; Shiina, I.; Asada, H. Prediction of pre-impact occupant kinematic behavior based on the muscle activity during frontal collision. In Proceedings of the 21st International Technical Conference on the Enhanced Safety Vehicles (ESV), Stuttgart, Germany, 15–18 June 2009. [Google Scholar]
- Bastien, C.; Blundell, M.V.; Neal-Sturgess, N. A study into the kinematic response for unbelted human occupants during emergency braking. Int. J. Crashworthiness 2017, 22, 689–703. [Google Scholar] [CrossRef]
- Iwamoto, M.; Nakahira, Y.; Kimpara, H. Development and validation of the Total HUman Model for Safety (THUMS) toward further understanding of occupant injury mechanisms in precrash and during crash. Traffic Inj. Prev. 2015, 16 (Suppl. 1), 36–48. [Google Scholar] [CrossRef]
- Dibb, A.T.; Cox, C.A.; Nightingale, R.W.; Luck, J.F.; Cutcliffe, H.C.; Myers, B.S.; Arbogast, K.B.; Seacrist, T.; Bass, C.R. Importance of muscle activations for biofidelic pediatric neck response in computational models. Traffic Inj. Prev. 2013, 14, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Ólafsdóttir, J.M.; Östh, J.K.H.; Davidsson, J.; Brolin, K.B. Passenger kinematics and muscle responses in autonomous braking events with standard and reversible pre-tensioned restraints. In Proceedings of the IRCOBI Conference, Gothenburg, Sweden, 11–13 September 2013. [Google Scholar]
- Feller, L.; Kleinbach, C.; Fehr, J.; Schmitt, S. Incorporating Muscle Activation Dynamics into the Global Human Body Model. In Proceedings of the IRCOBI Conference, Malaga, Spain, 14–16 September 2016. [Google Scholar]
- Östh, J.; Brolin, K.; Ólafsdóttir, J.M.; Davidsson, J.; Pipkorn, B.; Jakobsson, L.; Törnvall, F.; Lindkvist, M. Muscle activation strategies in human body models for the development of integrated safety. In Proceedings of the 24th International Techical Conference on the Enhanced Safety of Vehicles (ESV), Gothenburg, Sweden, 8–11 June 2015. [Google Scholar]
- Östh, J.; Brolin, K.; Bråse, D. A human body model with active muscles for simulation of pretensioned restraints in autonomous braking interventions. Traffic Inj. Prev. 2015, 16, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Ito, D.; Ejima, S.; Kitajima, S.; Katoh, R.; Ito, H.; Sakane, M.; Nishino, T.; Nakayama, K.; Ato, T.; Kimura, T. Occupant kinematic behavior and effects of a motorized seatbelt on occupant restraint of human volunteers during low speed frontal impact: Mini-sled tests with mass production car seat. In Proceedings of the IRCOBI Conference, Gothenburg, Sweden, 11–13 September 2013. [Google Scholar]
- Östmann, M.; Jacobsson, L. An examination of pre-crash braking influence on occupant crash response using an active human body model. In Proceedings of the IRCOBI Conference, Malaga, Spain, 14–16 September 2016. [Google Scholar]
- De Luca, C.J. The use of surface electromyography in biomechanics. J. Appl. Biomech. 1997, 13, 135–163. [Google Scholar] [CrossRef]
- De Luca, G. Fundamental Concepts in EMG Signal Acquisition; Rev. 2.1; DelSys Inc.: Boston, MA, USA, 2003. [Google Scholar]
- Hedenstierna, S.; Halldin, P.; Siegmund, G.P. Neck muscle load distribution in lateral, frontal and rear-end impacts. A three dimensional finite element analysis. Spine 2009, 34, 2626–2633. [Google Scholar] [CrossRef]
- Staudenmann, D.; Roeleveld, K.; Stegeman, D.F.; van Dieën, J.H. Methodological aspects of SEMG recordings for force estimation—A tutorial and review. J. Electromyogr. Kinesiol. 2010, 20, 375–387. [Google Scholar] [CrossRef]
- Hug, F. Can muscle coordination be precisely studied by surface electromyography? J. Electromyogr. Kinesiol. 2011, 21, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, T.S.; Lloyd, D.G.; Manal, K.; Besier, T.F. Neuromusculoskeletal modeling: Estimation of muscle forces and joint moments and movements from measurements of neural command. J. Appl. Biomech. 2004, 20, 367–395. [Google Scholar] [CrossRef] [PubMed]
- Desplenter, T.; Trejos, A.L. Evaluating muscle activation models for elbow motion estimation. Sensors 2018, 18, 1004. [Google Scholar] [CrossRef] [PubMed]
- Zajac, F.E. Muscle and tendon: Properties, models, scaling, and application to biomechanics and motor control. Crit. Rev. Biomed. Eng. 1989, 17, 359–410. [Google Scholar] [PubMed]
- Đorđević, S.; Stančin, S.; Meglič, A.; Milutinović, V.; Tomažič, S. MC sensor—A novel method for measurement of muscle tension. Sensors 2011, 11, 9411–9425. [Google Scholar] [CrossRef]
- Đorđević, S.; Tomažič, S.; Narici, M.; Pišot, R.; Meglič, A. In-vivo measurement of muscle tension: Dynamic properties of the MC sensor during isometric muscle contraction. Sensors 2014, 14, 17848–17863. [Google Scholar] [CrossRef]
- Krašna, S.; Đorđević, S.; Hribernik, M.; Trajkovski, A. A novel approach to measuring muscle mechanics in vehicle collision conditions. Sensors 2017, 17, 1389. [Google Scholar] [CrossRef]
- Challis, J.H. A procedure for determining rigid body transformation. J. Biomech. 1995, 28, 733–737. [Google Scholar] [CrossRef]
- Hodges, P.W.; Bui, B.H. A comparison of computer-based methods for the determination of onset of muscle contraction using electromyography. Electroencephalogr. Clin. Neurophyiol. 1996, 101, 511–519. [Google Scholar]
- Tillin, N.A. Neuromuscular performance of explosive power athletes versus untrained individuals. Med. Sci. Sports 2010, 42, 781–790. [Google Scholar] [CrossRef]
- Tenan, M.S.; Tweedell, A.J.; Haynes, C.A. Analysis of statistical and standard algorithms for detecting muscle onset with surface electromyography. PLoS ONE 2017, 12, e0177312. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Valdes, F.J.; Lau, A.; Lamp, J.; Riley, P.; Lessley, D.J.; Damon, A.; Kindig, M.; Kent, R.; Balasubramanian, S.; Seacrist, T.; et al. Analysis of spinal motion and loads during frontal impacts. Comparison between PMHS and ATD. Ann. Adv. Autom. Med. 2010, 54, 61–78. [Google Scholar]
- Seacrist, T.; Arbogast, K.B.; Maltese, M.R.; Garcıa-Espana, J.F.; Lopez-Valdes, F.J.; Kent, R.W.; Tanji, H.; Higuchi, K.; Balasubramanian, S. Kinetics of the cervical spine in pediatric and adult volunteers during low speed frontal impacts. J. Biomech. 2012, 45, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Yoganandan, N.; Pintar, F.A.; Zhang, J.; Baisden, J.L. Physical properties of the human head: Mass, center of gravity and moment of inertia. J. Biomech. 2009, 42, 1177–1192. [Google Scholar] [CrossRef] [PubMed]
- Anderst, W.J.; Donaldson, W.F., III; Lee, J.Y.; Kang, J.D. Subject-specific inverse dynamics of the head and cervical spice during in vivo dynamic flexion-extension. J. Biomech. Eng. 2013, 135, 061007. [Google Scholar] [CrossRef] [PubMed]
- Öner, M.; Kocakoç, I.D. JMASM 49: A compilation of some popular goodness of fit tests for normal distribution: Their algorithms and MATLAB codes (MATLAB). J. Mod. Appl. Stat. Methods 2017, 16, 547–575. [Google Scholar] [CrossRef]
- Kemper, A.R.; Beeman, S.M.; Madigan, M.L.; Duma, S.M. Human occupants in low-speed frontal sled tests: Effects of pre-impact bracing on chest compression, reaction forces, and subject acceleration. Traffic Inj. Prev. 2014, 15 (Suppl. 1), 141–150. [Google Scholar] [CrossRef]
- Latash, M.L. Muscle coactivation: Definitions, mechanisms, and functions. J. Neurophysiol. 2018, 120, 88–104. [Google Scholar] [CrossRef]
- Trajkovski, A.; Omerović, S.; Krašna, S.; Prebil, I. Loading rate effect on mechanical properties of cervical spine ligaments. Acta Bioeng. Biomech. 2014, 16, 13–20. [Google Scholar]
- Östh, J.; Brolin, K.; Svensson, M.Y.; Linder, A. A female ligamentous cervical spine finite element model validated for physiological loads. J. Biomech. Eng. 2016, 138, 061005. [Google Scholar] [CrossRef]
- Blouin, J.-S.; Siegmund, G.P.; Carpenter, M.G.; Inglis, J.T. Neural control of superficial and deep neck muscles in humans. J. Neurophysiol. 2007, 98, 920–928. [Google Scholar] [CrossRef]
- Siegmund, G.P.; Blouin, J.-P.; Brault, J.R.; Hedenstierna, S.; Inglis, J. Electromyography of superficial and deep neck muscles during isometric, voluntary, and reflex contractions. J. Biomech. Eng. 2007, 129, 66–77. [Google Scholar] [CrossRef]
- Siegmund, G.P.; Blouin, J.-S.; Carpenter, M.G.; Brault, J.R.; Inglis, J.T. Are cervical multifidus muscles active during whiplash and startle? An initial experimental study. BMC Musculoskelet. Disord. 2008, 9, 80. [Google Scholar] [CrossRef] [PubMed]
- Ólafsdóttir, J.M.; Brolin, K.; Blouin, J.-S.; Siegmund, G.P. Dynamic Spatial Tuning of Cervical Muscle Reflexes to Multidirectional Seated Perturbations. Spine 2015, 40, 211–219. [Google Scholar] [CrossRef]
- Derrick, T.R.; van den Bogert, A.J.; Cereatti, A.; Dumas, R.; Fantozzi, S.; Leardini, A. ISB recommendations on the reporting of intersegmental forces and moments during human motion analysis. J. Biomech. 2019, 99, 109533. [Google Scholar] [CrossRef] [PubMed]
- Siegmund, G.P.; Danderson, D.J.; Myers, B.S.; Inglis, J.T. Awareness affects the response of human subjects exposed to a single whiplash-like perturbation. Spine 2003, 28, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Vishton, P.M.; Reardon, K.M.; Stevens, J.A. Timing of anticipatory muscle tensing control: Responses before and after expected impact. Exp. Brain Res. 2010, 202, 661–667. [Google Scholar] [CrossRef]
- Mohapatra, S.; Krishnan, V.; Aruin, A.S. Postural control in response to an external perturbation: Effect of altered proprioceptive information. Exp. Brain Res. 2012, 217, 197–208. [Google Scholar] [CrossRef]
- Sanders, O.P.; Savin, D.N.; Creath, R.A.; Rogers, M.W. Protective balance and startle responses to sudden freefall in standing humans. Neurosci. Lett. 2015, 586, 8–12. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Vos, E.J.; Mullender, M.; van Ingen Schenau, G.J. Electromechanical delay in the vastus lateralis muscle during dynamic isometric contractions. Eur. J. Appl. Physiol. Occup. Physiol. 1990, 60, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Blanpied, P.; Oksendahl, H. Reaction times and electromechanical delay in reactions of increasing and decreasing force. Percept. Mot. Ski. 2006, 103, 743–754. [Google Scholar] [CrossRef]
- Johns, G.; Morin, E.; Hashtrudi-Zaad, K. The role of electromechanical delay in modelling the EMG-force relationship during quasi-dynamic contractions of the upper-limb. In Proceedings of the 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 3634–3637. [Google Scholar]
- Mahaki, M.; Souto De Sá E Souza, G.; Mimar, R.; Fraga Vieira, M. The comparison of ground reaction forces and lower limb muscles correlation and activation time delay between forward and backward walking. Gait Posture 2017, 58, 380–385. [Google Scholar] [CrossRef]
- Currie, S.J.; Myers, C.A.; Krishnamurty, A.; Enebo, B.A.; Davidson, B.S. Methods of muscle activation onset timing recorded during spinal manipulation. J. Manip. Physiol. Ther. 2016, 39, 279–287. [Google Scholar] [CrossRef]
- Nikooyan, A.A.; Veeger, H.E.J.; Westerhoff, P.; bolsterlee, B.; Graichen, F.; Bergmannn, G.; van der Helm, F.C.T. An EMG-driven musculoskeletal model for shoulder. Hum. Mov. Sci. 2012, 31, 429–447. [Google Scholar] [CrossRef]
- Vigotsky, A.D.; Halperin, I.; Lehman, G.J.; Trajano, G.S.; Vieira, T.M. Interpreting signal amplitudes in surface electromyography studies in sport and rehabilitation sciences. Front. Physiol. 2018, 8, 985. [Google Scholar] [CrossRef] [PubMed]
- Pizzolato, C.; Lloyd, D.G.; Sartori, M.; Ceseracciu, E.; Besier, T.F.; Fregly, B.J.; Reggiani, M. CEINMS: A toolbox to investigate the influence of different neural control solutions on the prediction of muscle excitation and joint moments during dynamics motor tasks. J. Biomech. 2015, 48, 3929–3936. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Peak Values | Aware | Unaware | p-Value | ||
|---|---|---|---|---|---|
| Mean ± SD | Median (min/max) | Mean ± SD | Median (min/max) | ||
| head excursion [mm] | 140.8 ± 38.0 | 130.4 (89.5/209.1) | 182.6 ± 71.0 | 166.9 (71.5/382.2) | 0.049a |
| head-neck flexion [°] | 18.3 ± 9.6 | 16.8 (3.2/41.0) | 30.2 ± 17.1 | 25.3 (9.7/69.0) | 0.001a |
| head acc. [m/s2] | 32.6 ± 2.7 | 32.3 (28.3/38.9) | 33.3 ± 3.7 | 34.1 (26.1/39.2) | 0.412 |
| angular acc. [rad/s2] | −51.5 ± 22.9 | −48.8 (−103.0/−10.7) | −64.0 ± 20.0 | −61.6 (−114.2/−21.4) | 0.028 |
| axial force [N] | 13.0 ± 12.3 | 12.6 (−17.7/33.5) | 10.8 ± 14.8 | 13.8 (−37.2/25.9) | 0.307 a |
| shear force [N] | 103.9 ± 12.1 | 105.0 (80.5/130.9) | 105.4 ± 16.3 | 106.9 (77.1/131.6) | 0.682 |
| bending moment [Nm] | −6.37 ± 1.02 | −6.21 (−8.26/−4.21) | −6.40 ± 1.20 | −6.44 (−8.53/−4.17) | 0.808 a |
| neck-muscle load [N] | 149.6 ± 29.4 | 144.6 (95.2/207.6) | 157.4 ± 34.5 | 149.6 (99.9/237.7) | 0.258 |
| seatbelt force [N] | 725.3 ± 316.0 | 768.2 (263.4/1572) | 869.3 ± 400.6 | 897.0 (47.2/1521) | 0.030 |
| EMG neck [−] | 0.791 ± 0.181 | 0.807 (0.469/1) | 0.849 ± 0.136 | 0.843 (0.613/1) | 0.211 a |
| MC neck [−] | 0.878 ± 0.128 | 0.891 (0.508/1) | 0.874 ± 0.136 | 0.919 (0.546/1) | 0.685 a |
| MC v. medialis [−] | 0.901 ± 0.100 | 0.899 (0.676/1) | 0.772 ± 0.203 | 0.797 (0.347/1) | 0.031a |
| head init. position x [mm] | 22.0 ± 25.5 | 22.4 (−36.8/65.4) | 12.1 ± 25.5 | 14.4 (−36.8/52.9) | 0.022 |
| head-neck init. flexion [°] | 2.9 ± 5.4 | 2.3 (−3.4/10.0) | −1.3 ± 8.1 | −0.5 (−18.8/12.4) | 0.015 |
| Timing [ms] | Aware | Unaware | p-Value | ||
|---|---|---|---|---|---|
| Mean ± SD | Median (min/max) | Mean ± SD | Median (min/max) | ||
| head excursion | 331.2 ± 26.4 | 327.5 (292/401) | 351.3 ± 47.1 | 339.5 (269/468) | 0.095 |
| head-neck flexion | 389.2 ± 40.0 | 379.5 (337/472) | 457.1 ± 88.2 | 451.0 (334/584) | 0.007 |
| head acc. | 288.0 ± 15.9 | 287.0 (265/316) | 294.4 ± 45.5 | 282.0 (241/412) | 0.876 |
| angular acc. | 327.3 ± 19.5 | 330.5 (291/363) | 331.8 ± 41.9 | 333.5 (235/424) | 0.670 |
| axial force | 323.4 ± 82.2 | 283.5 (227/477) | 188.6 ± 46.8 | 174.5 (152/340) | 0.079 a |
| shear force | 291.7 ± 19.1 | 291.5 (255/337) | 301.1 ± 46.0 | 285.5 (241/426) | 0.615 a |
| bending moment | 307.3 ± 17.6 | 304.5 (283/357) | 333.5 ± 60.2 | 313.5 (252/484) | 0.081 |
| neck-muscle load | 310.2 ± 17.0 | 306.5 (288/357) | 342.1 ± 66.0 | 315.5 (252/484) | 0.095 a |
| seatbelt force | 259.7 ± 16.5 | 261.1 (230/301) | 256.3 ± 36.4 | 250.0 (213.9/370) | 0.183 a |
| EMG | 232.0 ± 53.4 | 243.0 (73/281) | 266.5 ± 87.4 | 251.0 (200/457) | 0.284 a |
| MC neck | 319.6 ± 39.6 | 310.5 (271/449) | 351.6 ± 90.7 | 327.0 (259/601) | 0.263 a |
| MC v. medialis | 262.2 ± 22.3 | 259.0 (233/328) | 259.3 ± 21.3 | 254.5 (228/318) | 0.304 a |
| Condition | Mean ± SD | Median (min/max) | |
|---|---|---|---|
| rEMG-MC | aware | 0.78 ± 0.09 | 0.78 (0.56/0.92) |
| unaware | 0.77 ± 0.12 a | 0.82 (0.54/0.91) | |
| rEMG-F | aware | 0.80 ± 0.10 | 0.80 (0.52/0.96) |
| unaware | 0.81 ± 0.09 | 0.81 (0.60/0.95) | |
| rF-MC | aware | 0.89 ± 0.07 | 0.89 (0.71/0.97) |
| unaware | 0.89 ± 0.06 | 0.90 (0.77/0.98) |
| Condition | Mean ± SD | Median (min/max) | p-Value | |
|---|---|---|---|---|
| EMG neck | aware | 42.5 ± 38.2 | 55.5 (−77/93) | 0.001a |
| unaware | 91.1 ± 57.3 | 78.3 (2/230) | ||
| MC neck | aware | 62.8 ± 39.1 | 67.0 (−76/104) | <0.001a |
| unaware | 124.9 ± 55.9 | 105.5 (55/263) | ||
| MC v. medialis | aware | −36.0 ± 112.6 | −13.0 (−352/52) | 0.003 |
| unaware | 36.1 ± 42.0 | 48.0 (−85/83) | ||
| F neck | aware | 142.5 ± 54.0 | 148.0 (17/224) | 0.060 |
| unaware | 180.5 ± 45.6 | 181.5 (79/244) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krašna, S.; Đorđević, S. Estimating the Effects of Awareness on Neck-Muscle Loading in Frontal Impacts with EMG and MC Sensors. Sensors 2020, 20, 3942. https://doi.org/10.3390/s20143942
Krašna S, Đorđević S. Estimating the Effects of Awareness on Neck-Muscle Loading in Frontal Impacts with EMG and MC Sensors. Sensors. 2020; 20(14):3942. https://doi.org/10.3390/s20143942
Chicago/Turabian StyleKrašna, Simon, and Srđan Đorđević. 2020. "Estimating the Effects of Awareness on Neck-Muscle Loading in Frontal Impacts with EMG and MC Sensors" Sensors 20, no. 14: 3942. https://doi.org/10.3390/s20143942
APA StyleKrašna, S., & Đorđević, S. (2020). Estimating the Effects of Awareness on Neck-Muscle Loading in Frontal Impacts with EMG and MC Sensors. Sensors, 20(14), 3942. https://doi.org/10.3390/s20143942