Estimation of 3D Knee Joint Angles during Cycling Using Inertial Sensors: Accuracy of a Novel Sensor-to-Segment Calibration Procedure Based on Pedaling Motion


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Set Up
2.2.1. Motion Capture Equipment
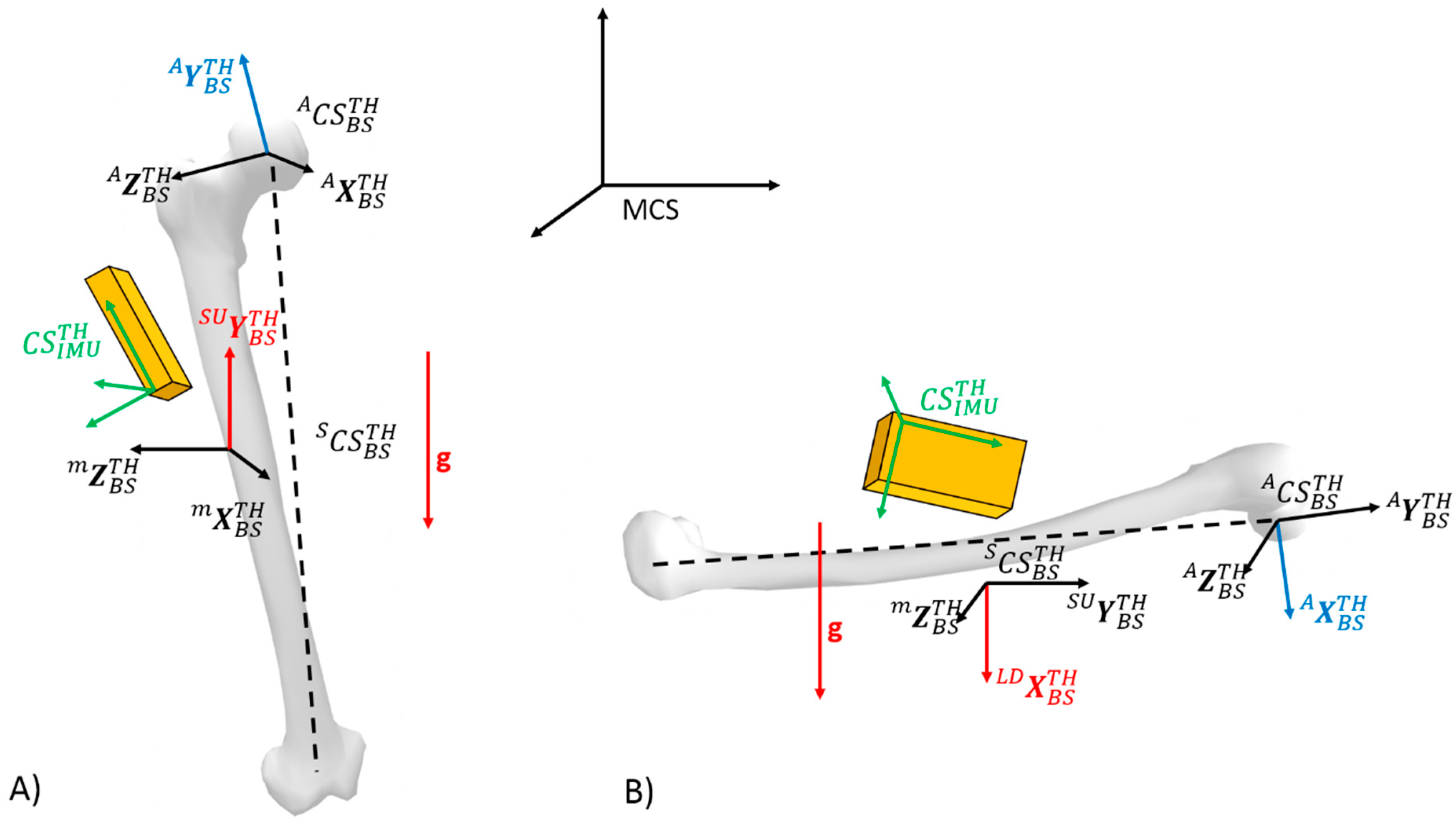
2.2.2. Definition of the Coordinate Systems
2.3. IMU-to-Body Alignment Methods
2.3.1. Calibration Tasks
- Standing up posture (SU): Static standing upright posture with feet apart in line with the hip and knee stretched. In this posture, the longitudinal axis of the thigh and shank are assumed to be vertical. The lower limb posture is similar to the one used during the T-pose or N-pose [30].
- Lying down (LD): Static lying face down posture. Hence, the anteroposterior axis of the segments is assumed to be aligned with the vertical axis. Hands are placed between the ground and chin.
- Knee flexion/extension (KFE): Dynamic task with the participant performing four knee flexions/extensions from about 10° to 90° of flexion, in a single leg up-right posture. Participants were asked to avoid any thigh movement. This task allowed estimation of the knee flexion axis.
- Hip abduction/adduction (HAA): Dynamic task with the participant performing four hip abductions/adductions in a single leg up-right posture. Participants were asked to avoid hip external rotations with the foot pointing forward. This task allowed estimation of the anteroposterior axis of the thigh.
2.3.2. Calibration Methods
2.4. Joint Angles Computation
2.5. Data Analysis
2.5.1. Alignment Error between the IMU and the Body Segment Frames
2.5.2. 3D Knee Joint Angle Accuracy
2.6. Statistical Analysis
3. Results
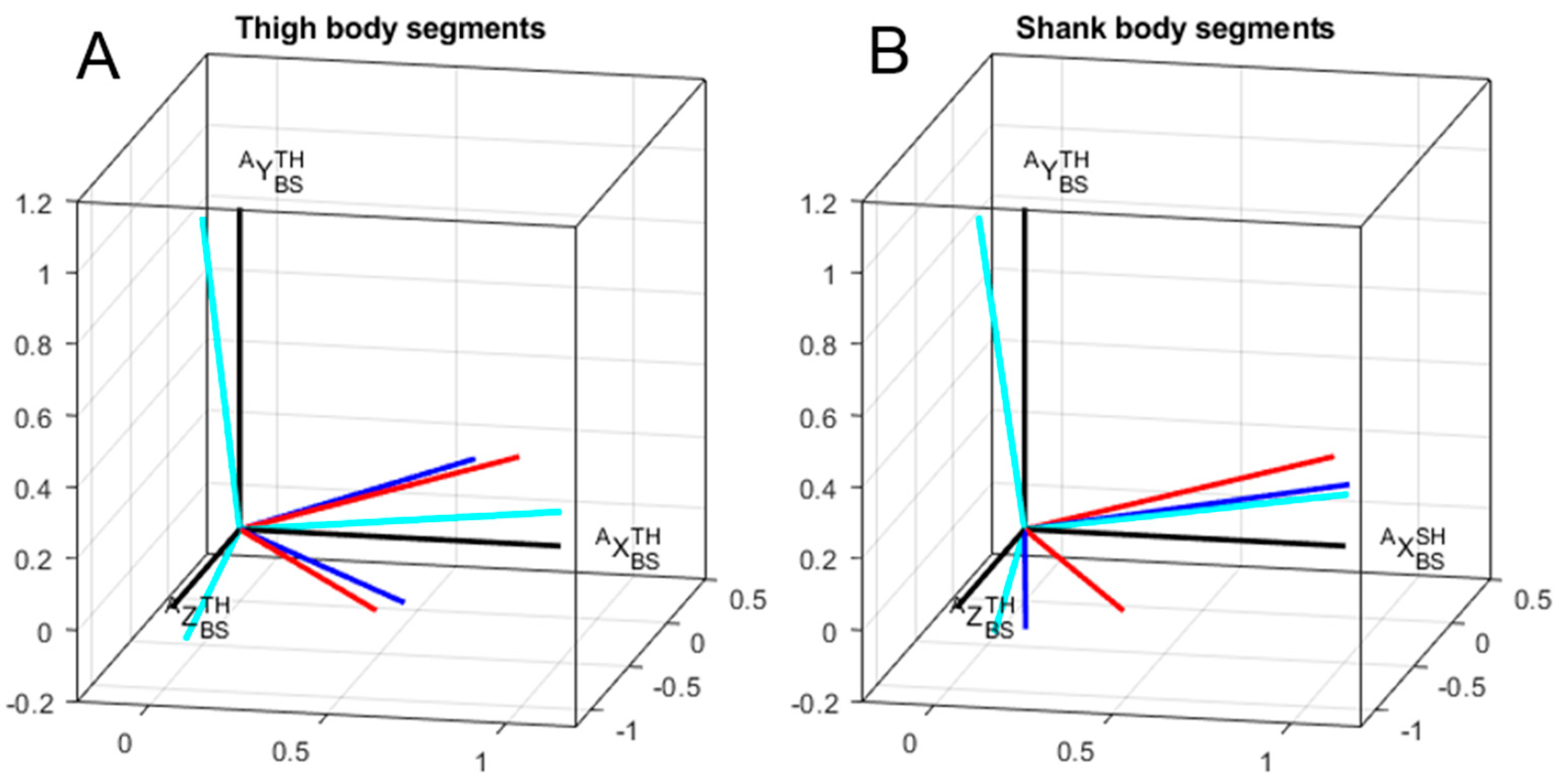
3.1. Accuracy of the Segment Orientation
3.2. Effects of the Calibration Methods on 3D Knee Joint Angles
4. Discussion
4.1. Differences Between Calibration Methods—Comparisons with the Literature
4.2. Variability of Calibration Tasks
4.3. Limitations and Perspectives
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gregersen, C.S.; Hull, M.L. Non-driving intersegmental knee moments in cycling computed using a model that includes three-dimensional kinematics of the shank/foot and the effect of simplifying assumptions. J. Biomech. 2003, 36, 803–813. [Google Scholar] [CrossRef]
- Bailey, M.P.; Maillardet, F.J.; Messenger, N. Kinematics of cycling in relation to anterior knee pain and patellar tendinitis. J. Sports Sci. 2003, 21, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Peveler, W.W.P.; Green, J.M.G. Effect of saddle height on economy and anaerobic power in well-trained cyclists. J. Strength Cond. Res. 2011, 25, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Bini, R.R.; Di Alencar, T.A. Non-traumatic Injuries in Cycling. In Biomechanics of Cycling; Springer International Publishing: Cham, Switzerland, 2014; pp. 55–62. [Google Scholar]
- Bini, R.R.; Dagnese, F.; Rocha, E.; Silveira, M.C.; Carpes, F.P.; Mota, C.B. Three-dimensional kinematics of competitive and recreational cyclists across different workloads during cycling. Eur. J. Sport Sci. 2016, 16, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Silberman, M.R. Bicycling injuries. Curr. Sports Med. Rep. 2013, 12, 337–345. [Google Scholar] [CrossRef]
- Bini, R.R.; Tamborindeguy, A.C.; Mota, C.B. Effects of saddle height, pedaling cadence, and workload on joint kinetics and kinematics during cycling. J. Sport Rehabil. 2010, 19, 301–314. [Google Scholar] [CrossRef]
- Callaghan, M.J. Lower body problems and injury in cycling. J. Bodyw. Mov. Ther. 2005, 9, 226–236. [Google Scholar] [CrossRef]
- Pouliquen, C.; Nicolas, G.; Bideau, B.; Garo, G.; Megret, A.; Delamarche, P.; Bideau, N. Spatiotemporal analysis of 3D kinematic asymmetry in professional cycling during an incremental test to exhaustion. J. Sports Sci. 2018, 36, 2155–2163. [Google Scholar] [CrossRef] [PubMed]
- Windolf, M.; Götzen, N.; Morlock, M. Systematic accuracy and precision analysis of video motion capturing systems-exemplified on the Vicon-460 system. J. Biomech. 2008, 41, 2776–2780. [Google Scholar] [CrossRef]
- Ahmad, N.; Ghazilla, R.A.R.; Khairi, N.M.; Kasi, V. Reviews on Various Inertial Measurement Unit (IMU) Sensor Applications. Int. J. Signal. Process. Syst. 2013, 1, 256–262. [Google Scholar] [CrossRef]
- Picerno, P. 25 years of lower limb joint kinematics by using inertial and magnetic sensors: A review of methodological approaches. Gait Posture 2017, 51, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Marin, F.; Fradet, L.; Lepetit, K.; Hansen, C.; Ben, K. Inertial measurement unit in biomechanics and sport biomechanics: Past, present, future. In Proceedings of the 33 International Conference of Biomechanics in Sports (2015), Poitiers, France, 29 June–3 July 2015; pp. 1422–1424. [Google Scholar]
- Sabatini, A.M. Estimating three-dimensional orientation of human body parts by inertial/magnetic sensing. Sensors 2011, 11, 1489–1525. [Google Scholar] [CrossRef] [PubMed]
- Bergamini, E.; Ligorio, G.; Summa, A.; Vannozzi, G.; Cappozzo, A.; Sabatini, A.M. Estimating orientation using magnetic and inertial sensors and different sensor fusion approaches: Accuracy assessment in manual and locomotion tasks. Sensors 2014, 14, 18625–18649. [Google Scholar] [CrossRef]
- de Vries, W.H.K.; Veeger, H.E.J.; Baten, C.T.M.; van der Helm, F.C.T. Magnetic distortion in motion labs, implications for validating inertial magnetic sensors. Gait Posture 2009, 29, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Cockcroft, J. An Evaluation of Inertial Motion Capture Technology for Use in the Analysis and Optimization of Road Cycling Kinematics. Master’s Thesis, Stellenbosch University, Stellenbosch, South Africa, 2011. [Google Scholar]
- O’Donovan, K.J.; Kamnik, R.; O’Keeffe, D.T.; Lyons, G.M. An inertial and magnetic sensor based technique for joint angle measurement. J. Biomech. 2007, 40, 2604–2611. [Google Scholar] [CrossRef] [PubMed]
- Beravs, T.; Rebersek, P.; Novak, D.; Podobnik, J.; Munih, M. Development and validation of a wearable inertial measurement system for use with lower limb exoskeletons. In Proceedings of the 2011 11th IEEE-RAS International Conference on Humanoid Robots, Bled, Slovenia, 26–28 October 2011; pp. 212–217. [Google Scholar]
- Alonge, F.; Cucco, E.; D’Ippolito, F.; Pulizzotto, A. The use of accelerometers and gyroscopes to estimate hip and knee angles on gait analysis. Sensors 2014, 14, 8430–8446. [Google Scholar] [CrossRef]
- Miezal, M.; Taetz, B.; Schmitz, N.; Bleser, G. Ambulatory inertial spinal tracking using constraints. In Proceedings of the 9th International Conference on Body Area Networks, London, UK, 29 September–01 October 2014; pp. 1–4. [Google Scholar]
- Taetz, B.; Bleser, G.; Miezal, M. Towards self-calibrating inertial body motion capture. In Proceedings of the 19th International Conference on Information Fusion (FUSION), Heidelberg, Germany, 5–8 July 2016; pp. 1751–1759. [Google Scholar]
- Seel, T.; Raisch, J.; Schauer, T. IMU-Based Joint Angle Measurement for Gait Analysis. Sensors 2014, 14, 6891–6909. [Google Scholar] [CrossRef]
- Bouvier, B.; Duprey, S.; Claudon, L.; Dumas, R.; Savescu, A. Upper limb kinematics using inertial and magnetic sensors: Comparison of sensor-to-segment calibrations. Sensors 2015, 15, 18813–18833. [Google Scholar] [CrossRef]
- Picerno, P.; Cereatti, A.; Cappozzo, A. Joint kinematics estimate using wearable inertial and magnetic sensing modules. Gait Posture 2008, 28, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Laidig, D.; Seel, T. Automatic anatomical calibration for IMU- based elbow angle measurement in disturbed magnetic fields. Curr. Directions Biomed. Eng. 2017, 3, 167–170. [Google Scholar] [CrossRef]
- Küderle, A.; Becker, S.; Disselhorst-Klug, C. Increasing the Robustness of the automatic IMU calibration for lower Extremity Motion Analysis. Curr. Directions Biomed. Eng. 2018, 4, 439–442. [Google Scholar] [CrossRef]
- Olsson, F.; Seel, T.; Lehmann, D.; Halvorsen, K. Joint axis estimation for fast and slow movements using weighted gyroscope and acceleration constraints. arXiv 2019, arXiv:1903.07353. [Google Scholar]
- McGrath, T.; Fineman, R.; Stirling, L. An auto-calibrating knee flexion-extension axis estimator using principal component analysis with inertial sensors. Sensors 2018, 18, 1882. [Google Scholar] [CrossRef] [PubMed]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Accuracy and repeatability of single-pose calibration of inertial measurement units for whole-body motion analysis. Gait Posture 2017, 54, 80–86. [Google Scholar] [CrossRef]
- Palermo, E.; Rossi, S.; Marini, F.; Patane, F.; Cappa, P. Experimental evaluation of accuracy and repeatability of a novel body-to-sensor calibration procedure for inertial sensor-based gait analysis. Measurement 2014, 52, 145–155. [Google Scholar] [CrossRef]
- Cutti, A.G.; Ferrari, A.; Garofalo, P.; Raggi, M.; Cappello, A.; Ferrari, A. “Outwalk”: A protocol for clinical gait analysis based on inertial and magnetic sensors. Med. Biol. Eng. Comput. 2010, 48, 17–25. [Google Scholar] [CrossRef]
- de Vries, W.H.K.; Veeger, H.E.J.; Cutti, A.G.; Baten, C.; van der Helm, F.C.T. Functionally interpretable local coordinate systems for the upper extremity using inertial & magnetic measurement systems. J. Biomech. 2010, 43, 1983–1988. [Google Scholar] [CrossRef] [PubMed]
- Favre, J.; Aissaoui, R.; Jolles, B.M.; de Guise, J.A.; Aminian, K. Functional calibration procedure for 3D knee joint angle description using inertial sensors. J. Biomech. 2009, 42, 2330–2335. [Google Scholar] [CrossRef]
- Luinge, H.J.; Veltink, P.H.; Baten, C.T.M. Ambulatory measurement of arm orientation. J. Biomech. 2007, 40, 78–85. [Google Scholar] [CrossRef]
- Cooper, G.; Sheret, I.; McMillian, L.; Siliverdis, K.; Sha, N.; Hodgins, D.; Kenney, L.; Howard, D. Inertial sensor-based knee flexion/extension angle estimation. J. Biomech. 2009, 42, 2678–2685. [Google Scholar] [CrossRef]
- Lambrecht, J.M.; Kirsch, R.F. Miniature low-power inertial sensors: Promising technology for implantable motion capture systems. IEEE Trans. Neural Syst. Rehabil. Eng. 2014, 22, 1138–1147. [Google Scholar] [CrossRef]
- Fradet, L.; Nez, A.; Monnet, T.; Lacouture, P. Which functional movements for sensor-to-segment calibration for lower-limb movement analysis with inertial sensors? Comput. Methods Biomech. Biomed. Eng. 2017, 20, 77–78. [Google Scholar] [CrossRef]
- Brennan, A.; Deluzio, K.; Li, Q. Assessment of anatomical frame variation effect on joint angles: A linear perturbation approach. J. Biomech. 2011, 44, 2838–2842. [Google Scholar] [CrossRef]
- Fasel, B.; Spörri, J.; Schütz, P.; Lorenzetti, S.; Aminian, K. Validation of functional calibration and strap-down joint drift correction for computing 3D joint angles of knee, hip, and trunk in alpine skiing. PLoS ONE 2017, 12, e0181446. [Google Scholar] [CrossRef]
- Marin-Perianu, R.; Marin-Perianu, M.; Havinga, P.; Taylor, S.; Begg, R.; Palaniswami, M.; Rouffet, D. A performance analysis of a wireless body-area network monitoring system for professional cycling. Pers. Ubiquit. Comput. 2013, 17, 197–209. [Google Scholar] [CrossRef]
- Lin, T.; Chen, H.; Chen, A.; Wang, H. Poster: SaFePlay + – A Wearable Cycling Measurement and Analysis System of Lower Limbs. In Proceedings of the 24th Annual International Conference on Mobile Computing and Networking, New Delhi, India, 29 October–02 November 2018; pp. 744–746. [Google Scholar]
- Wiesener, C.; Schauer, T. The Cybathlon RehaBike: Inertial-Sensor-Driven Functional Electrical Stimulation Cycling by Team Hasomed. IEEE Robot. Autom. Mag. 2017, 24, 49–57. [Google Scholar] [CrossRef]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H.; et al. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: Ankle, hip, and spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Wu, G.; Cavanagh, P.R. ISB Recommendations in the Reporting for Standardization of Kinematic Data. J. Biomech. 1995, 28, 1257–1261. [Google Scholar] [CrossRef]
- Madgwick, S.O.H.; Harrison, A.J.L.; Vaidyanathan, R. Estimation of IMU and MARG orientation using a gradient descent algorithm. In Proceedings of the IEEE International Conference on Rehabilitation Robotics Rehab Week Zurich, ETH Zurich Science City, Switzerlan, 29 June–1 July 2011. [Google Scholar] [CrossRef]
- Van Den Noort, J.C.; Ferrari, A.; Cutti, A.G.; Becher, J.G.; Harlaar, J. Gait analysis in children with cerebral palsy via inertial and magnetic sensors. Med. Biol. Eng. Comput. 2013, 51, 377–386. [Google Scholar] [CrossRef]
- Teufl, W.; Miezal, M.; Taetz, B.; Fröhlich, M.; Bleser, G. Validity, test-retest reliability and long-term stability of magnetometer free inertial sensor based 3D joint kinematics. Sensors 2018, 18, 1980. [Google Scholar] [CrossRef]
- Yu, B.; Gabriel, D.; Noble, L.; An, K.-N. Estimate of the Optimum Cutoff Frequency for the Butterworth Low-Pass Digital Filter. J. Appl. Biomech. 1999, 15, 318–329. [Google Scholar] [CrossRef]
- Cappozzo, A.; Della Croce, U.; Leardini, A.; Chiari, L. Human movement analysis using stereophotogrammetry. Gait Posture 2005, 21, 186–196. [Google Scholar] [CrossRef]
- Vargas-Valencia, L.; Elias, A.; Rocon, E.; Bastos-Filho, T.; Frizera, A. An IMU-to-Body Alignment Method Applied to Human Gait Analysis. Sensors 2016, 16, 2090. [Google Scholar] [CrossRef] [PubMed]
- Luinge, H.J.; Veltink, P.H. Measuring orientation of human body segments using miniature gyroscopes and accelerometers. Med. Biol. Eng. Comput. 2005, 43, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Ehrig, R.M.; Taylor, W.R.; Duda, G.N.; Heller, M.O. A survey of formal methods for determining functional joint axes. J. Biomech. 2007, 40, 2150–2157. [Google Scholar] [CrossRef] [PubMed]
- Mecheri, H.; Robert-Lachaine, X.; Larue, C.; Plamondon, A. Evaluation of Eight Methods for Aligning Orientation of Two Coordinate Systems. J. Biomech. Eng. 2016, 138, 084501. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Jung, W.C. Quaternion-Based Local Frame Alignment between an Inertial Measurement Unit and a Motion Capture System. Sensors 2018, 18, 4003. [Google Scholar] [CrossRef] [PubMed]
- Leardini, A.; Lullini, G.; Giannini, S.; Berti, L.; Ortolani, M.; Caravaggi, P. Validation of the angular measurements of a new inertial-measurement-unit based rehabilitation system: Comparison with state-of-the-art gait analysis. J. Neuroeng. Rehabil. 2014, 11, 136. [Google Scholar] [CrossRef]
- Takeda, R.; Tadano, S.; Natorigawa, A.; Todoh, M.; Yoshinari, S. Gait posture estimation by wearable acceleration and gyro sensor. In IFMBE Proceedings, Proceedings of the World Congress on Medical Physics and Biomedical Engineering, 7–12 September 2009, Munich, Germany; Dössel, O., Schlegel, W.C., Eds.; Springer: Berlin, Heidelberg, 2009; Volume 25, pp. 111–114. [Google Scholar]
- Besier, T.F.; Sturnieks, D.L.; Alderson, J.A.; Lloyd, D.G. Repeatability of gait data using a functional hip joint centre and a mean helical knee axis. J. Biomech. 2003, 36, 1159–1168. [Google Scholar] [CrossRef]
- Marin, F.; Mannel, H.; Claes, L.; Dürselen, L. Correction of axis misalignment in the analysis of knee rotations. Hum. Mov. Sci. 2003, 22, 285–296. [Google Scholar] [CrossRef]
- Ricci, L.; Formica, D.; Sparaci, L.; Romana Lasorsa, F.; Taffoni, F.; Tamilia, E.; Guglielmelli, E. A new calibration methodology for thorax and upper limbs motion capture in children using magneto and inertial sensors. Sensors 2014, 14, 1057–1072. [Google Scholar] [CrossRef] [PubMed]
- Kapandji, I.A.; Kapandji, I.A. The Physiology of the Joints; Churchill Livingstone: London, UK, 1987; ISBN 9780702039423. [Google Scholar]
- Blankevoort, L.; Huiskes, R.; de Lange, A. The envelope of passive knee joint motion. J. Biomech. 1988, 21, 705–720. [Google Scholar] [CrossRef]
- Moglo, K.E.; Shirazi-Adl, A. Cruciate coupling and screw-home mechanism in passive knee joint during extension–flexion. J. Biomech. 2005, 38, 1075–1083. [Google Scholar] [CrossRef] [PubMed]
- Mannel, H.; Marin, F.; Claes, L.; Dürselen, L. Establishment of a knee-joint coordinate system from helical axes analysis—A kinematic approach without anatomical referencing. IEEE Trans. Biomed. Eng. 2004, 51, 1341–1347. [Google Scholar] [CrossRef]
- Cappello, A.; Cappozzo, A.; La Palombara, P.F.; Lucchetti, L.; Leardini, A. Multiple anatomical landmark calibration for optimal bone pose estimation. Hum. Mov. Sci. 1997, 16, 259–274. [Google Scholar] [CrossRef]
- Cockcroft, J.; Muller, J.H.; Scheffer, C. A novel complimentary filter for tracking hip angles during cycling using wireless inertial sensors and dynamic acceleration estimation. IEEE Sens. J. 2014, 14, 2864–2871. [Google Scholar] [CrossRef]
- Leardini, A.; Chiari, A.; Della Croce, U.; Cappozzo, A. Human movement analysis using stereophotogrammetry Part 3. Soft tissue artifact assessment and compensation. Gait Posture 2005, 21, 212–225. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Benedetti, M.G.; Pavan, E.; Frigo, C.; Bettinelli, D.; Rabuffetti, M.; Crenna, P.; Leardini, A. Quantitative comparison of five current protocols in gait analysis. Gait Posture 2008, 28, 207–216. [Google Scholar] [CrossRef]
- Al-Amri, M.; Nicholas, K.; Button, K.; Sparkes, V.; Sheeran, L.; Davies, J.L. Inertial measurement units for clinical movement analysis: Reliability and concurrent validity. Sensors 2018, 18, 719. [Google Scholar] [CrossRef]
- Zhang, J.-T.; Novak, A.C.; Brouwer, B.; Li, Q. Concurrent validation of Xsens MVN measurement of lower limb joint angular kinematics. Physiol. Meas. 2013, 34, N63–N69. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Task. | SU | LD | HAA | KFE | P |
|---|---|---|---|---|---|
| Illustration |  |  |  |  |  |
| Unit vector identified for thigh | |||||
| Unit vector identified for shank |
| Method | First Task | Second Task | Thigh Frame | Shank Frame |
|---|---|---|---|---|
| SU | P | |||
| SU | LD | |||
| SU | HAA/KFE | |||
| SU | P |
| Orientation Error for Each Method (Deg) | p-Values | ||||||
|---|---|---|---|---|---|---|---|
| Segment | Angle | Static | Mixed | Cycling | S vs. M | S vs. C | M vs. C |
| Thigh | TOTAL | 20.0 ± 6.6 | 22.2 ± 7.9 | 10.9 ± 1.6 | 0.78 | 0.003 | 0.001 |
| around X | −2.6 ± 2.2 | −2.6 ± 2.2 | −2.6 ± 2.2 | n/a | n/a | n/a | |
| around Y | −16.2 ± 8.9 | −19.1 ± 9.3 | −1.7 ± 2.3 | 0.74 | < 0.001 | < 0.001 | |
| around Z | −8.9 ± 2.1 | −8.9 ± 2.1 | −8.9 ± 2.1 | n/a | n/a | n/a | |
| Shank | TOTAL | 17.4 ± 8.4 | 13.4 ± 3.5 | 11.8 ± 2.8 | 0.110 | 0.069 | 0.449 |
| around X | −4.6 ± 2.2 | −4.6 ± 2.2 | −4.6 ± 2.2 | n/a | n/a | n/a | |
| around Y | −14.4 ± 9.8 | −10.0 ± 4.3 | −8.1 ± 2.5 | 0.152 | 0.548 | 0.089 | |
| around Z | −5.9 ± 2.4 | −5.9 ± 2.4 | −5.9 ± 2.4 | n/a | n/a | n/a | |
| RMS Error in the Knee Angle for Each Method (deg) | p-Values | |||||
|---|---|---|---|---|---|---|
| DOF | Static | Mixed | Cycling | S vs. M | S vs. C | M vs. C |
| Flexion/Extension | 4.79 ± 3.03 | 3.65 ± 2.23 | 3.74 ± 2.99 | 0.38 | 0.82 | 1 |
| Abduction/Adduction | 11.18 ± 6.62 | 7.51 ± 4.13 | 5.92 ± 2.85 | 0.062 | 0.035 | 0.346 |
| Internal/External Rotation | 15.37 ± 5.38 | 18.80 ± 8.05 | 6.65 ± 1.94 | 0.357 | <0.001 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cordillet, S.; Bideau, N.; Bideau, B.; Nicolas, G. Estimation of 3D Knee Joint Angles during Cycling Using Inertial Sensors: Accuracy of a Novel Sensor-to-Segment Calibration Procedure Based on Pedaling Motion. Sensors 2019, 19, 2474. https://doi.org/10.3390/s19112474
Cordillet S, Bideau N, Bideau B, Nicolas G. Estimation of 3D Knee Joint Angles during Cycling Using Inertial Sensors: Accuracy of a Novel Sensor-to-Segment Calibration Procedure Based on Pedaling Motion. Sensors. 2019; 19(11):2474. https://doi.org/10.3390/s19112474
Chicago/Turabian StyleCordillet, Sébastien, Nicolas Bideau, Benoit Bideau, and Guillaume Nicolas. 2019. "Estimation of 3D Knee Joint Angles during Cycling Using Inertial Sensors: Accuracy of a Novel Sensor-to-Segment Calibration Procedure Based on Pedaling Motion" Sensors 19, no. 11: 2474. https://doi.org/10.3390/s19112474
APA StyleCordillet, S., Bideau, N., Bideau, B., & Nicolas, G. (2019). Estimation of 3D Knee Joint Angles during Cycling Using Inertial Sensors: Accuracy of a Novel Sensor-to-Segment Calibration Procedure Based on Pedaling Motion. Sensors, 19(11), 2474. https://doi.org/10.3390/s19112474