

The Design of a Multistage Monitoring Protocol for Dendritic Cell-Derived Exosome (DEX) Immunotherapy: A Conceptual Framework for Molecular Quality Control and Immune Profiling

 ,
,
Abstract
1. Introduction
2. Results
2.1. Optimization and Characterization in the Molecular Laboratory
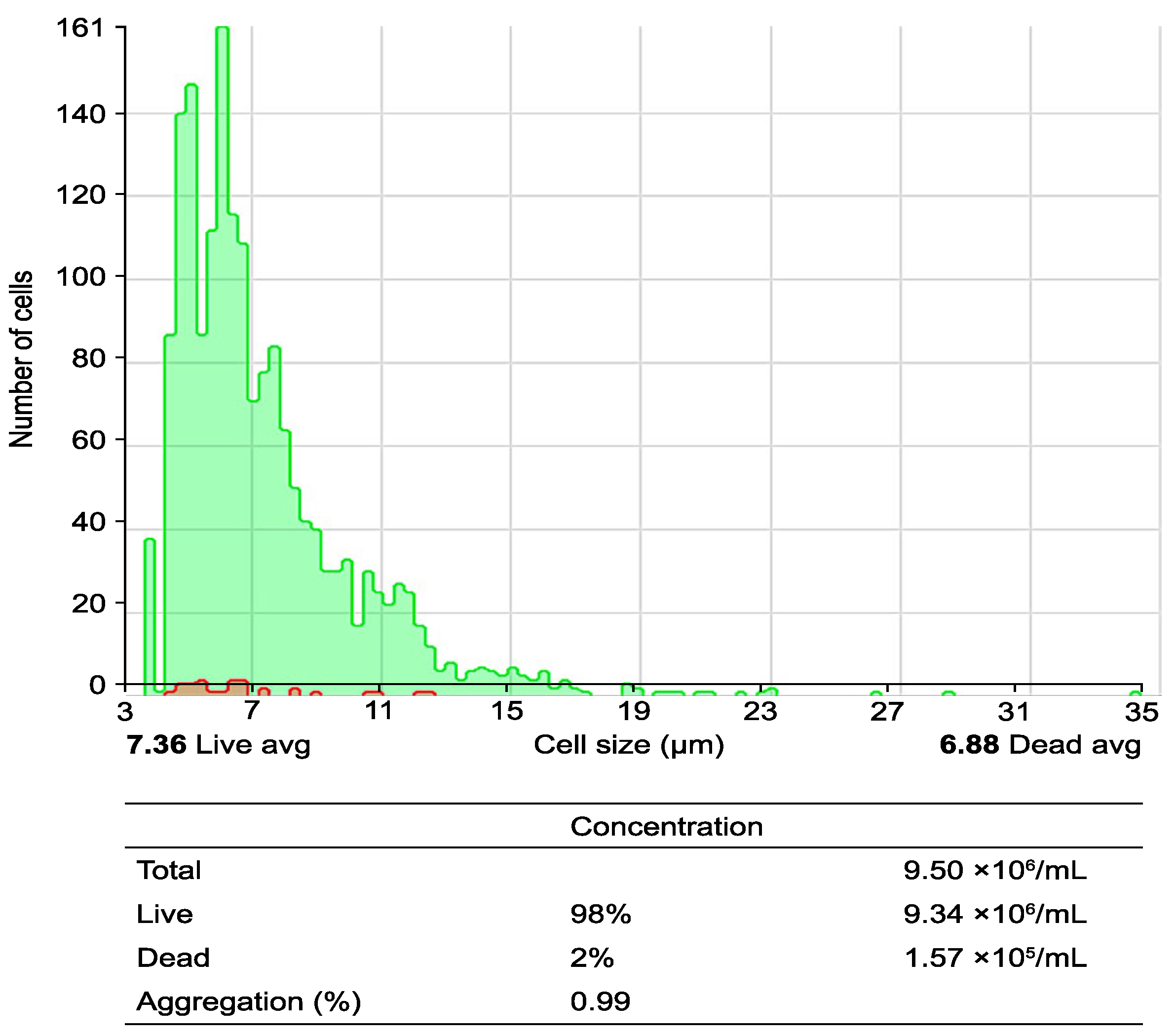
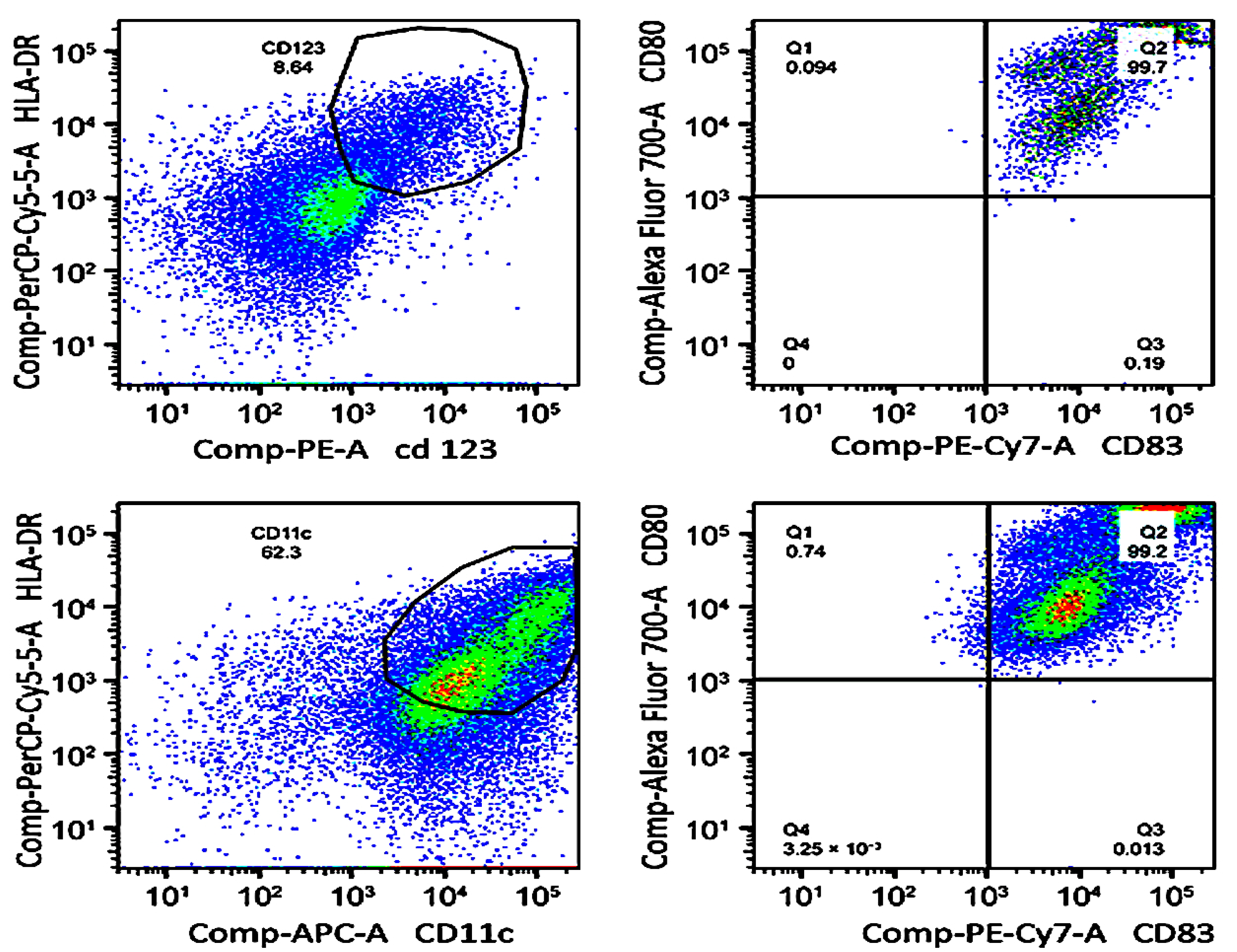
2.1.1. Optimizing Progenitor Cell Isolation and DC Differentiation
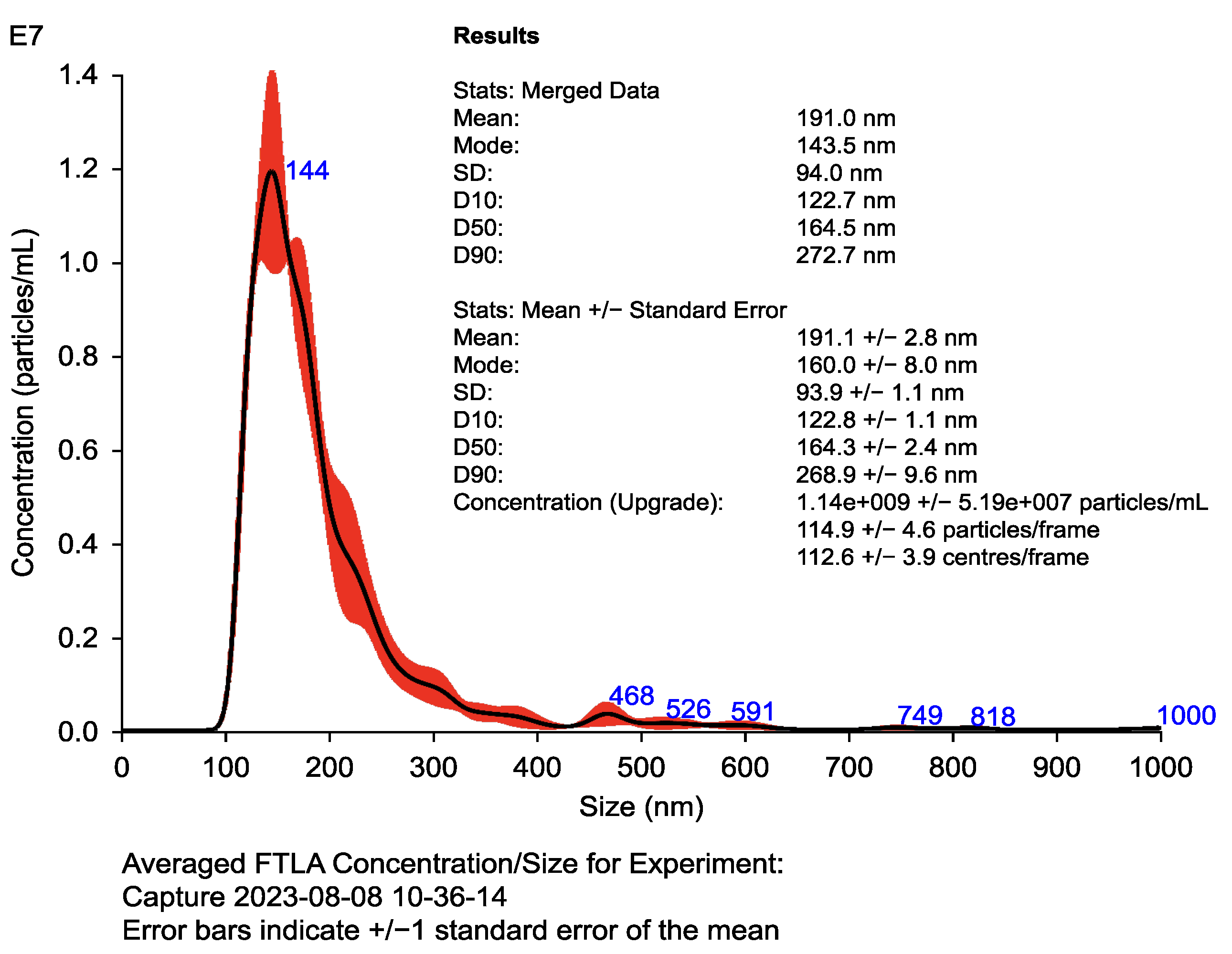
2.1.2. Structural and Functional Characterization of Exosomes
2.1.3. Advanced Quality and Functionality Assessment
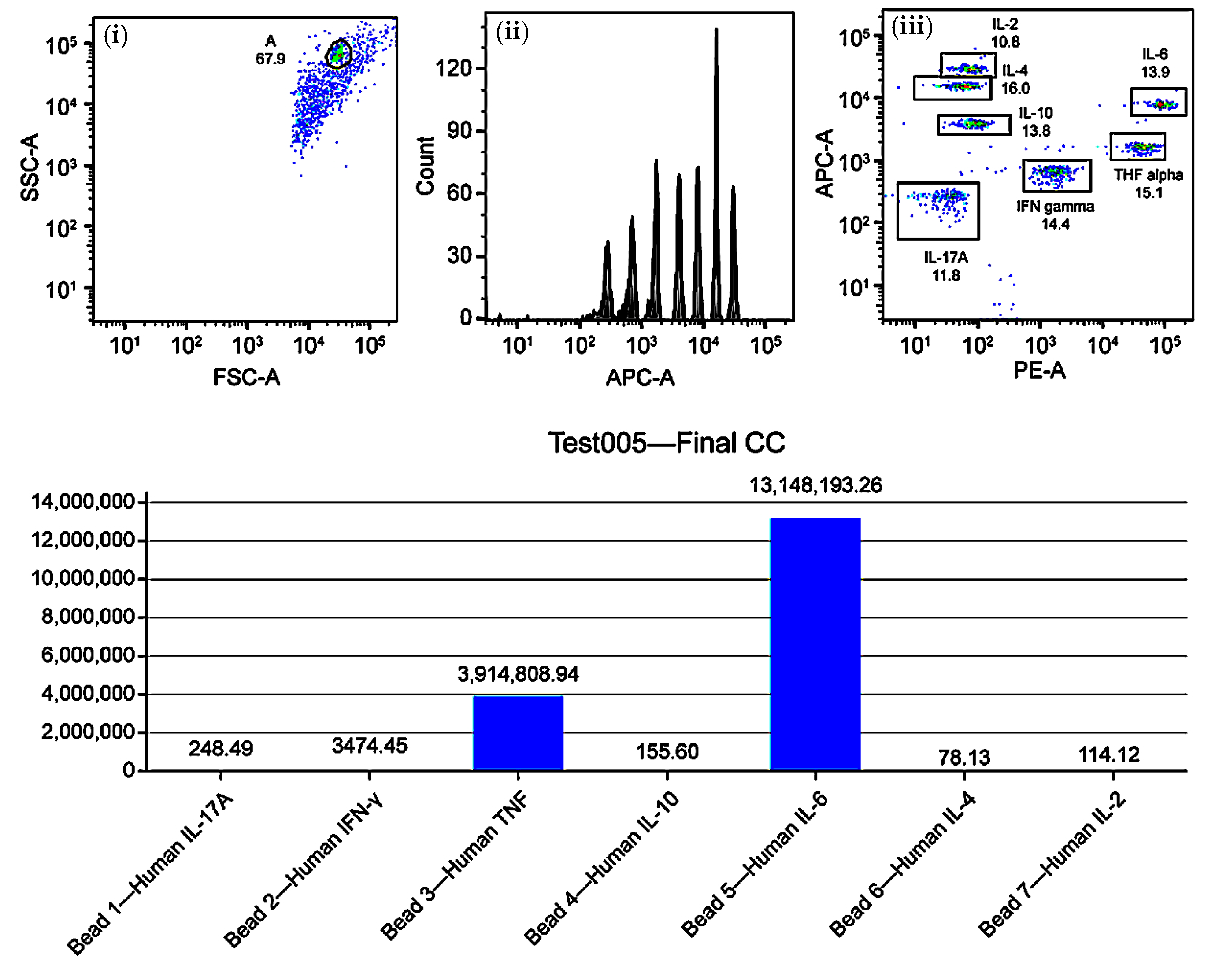
2.1.4. Immune Monitoring Protocol
2.2. Complementary Clinical Follow-Up
3. Discussion
3.1. Impact of Laboratory Results on Treatment Personalization
3.1.1. T-Cell Activation and Treatment Adjustments
3.1.2. Th1, Th2, and Th17 Immune Profiles: Influence on Response
3.1.3. Evaluation of the Quality and Functionality of Exosomes
3.1.4. Adjustments in Immunotherapy Administration
3.1.5. Clinical Translation: Interpretation Framework for Treating Oncologists
Illustrative Clinical Scenarios
3.2. Operational Requirements and Protocol Scalability
3.2.1. Resource Demands and Technical Requirements
3.2.2. Scalability
3.3. Limitations and Future Directions
3.3.1. Limitations in the Immune Response
3.3.2. Future Directions in Research
3.3.3. Interdisciplinary Collaborations
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| APC-A | Allophycocyanin Area |
| CA-125 | Cancer Antigen 125 |
| CBA | Cytometric Bead Array |
| CD | Cluster of Differentiation |
| CD80, CD83, CD63, CD81 | Cell Differentiation Markers |
| CTD | Common Technical Document |
| DC | Dendritic Cell |
| DEX | Dendritic Cell-Derived Exosome |
| ΔC | Change in Confluence (Kinetic Divergence Index) |
| ΔT | Divergence Time (Time to Immunological Shift) |
| FSC-A | Forward Scatter Area |
| FSI | Functional Stratification Index |
| GM-CSF | Granulocyte–Macrophage Colony-Stimulating Factor |
| HLA-DR | Human Leukocyte Antigen–DR Isotype |
| IFN-γ | Interferon Gamma |
| IL-1β | Interleukin 1 Beta |
| IL-4 | Interleukin 4 |
| IL-12 | Interleukin 12 |
| iRECISTs | Immune Response Evaluation Criteria in Solid Tumors |
| LDH | Lactate Dehydrogenase |
| NTA | Nanoparticle Tracking Analysis |
| PBMC | Peripheral Blood Mononuclear Cell |
| PE | Phycoerythrin |
| PET-CT | Positron Emission Tomography–Computed Tomography |
| pg/mL | Picograms per Milliliter |
| PLPC | Phospholipoproteic Complex |
| PSA | Prostate-Specific Antigen |
| QC | Quality Control |
| RA | Real-world Adaptive |
| RECIST | Response Evaluation Criteria in Solid Tumors |
| SSC-A | Side Scatter Area |
| STIP | Structured Immunophenotypic Traceability Platform |
| Th1, Th2, Th17 | T Helper Cell Subtypes |
| TLR | Toll-Like Receptor |
| TNF-α | Tumor Necrosis Factor Alpha |
References
- Zhang, H.; Wang, S.; Sun, M.; Cui, Y.; Xing, J.; Teng, L.; Xi, Z.; Yang, Z. Exosomes as smart drug delivery vehicles for cancer immunotherapy. Front. Immunol. 2023, 13, 1093607. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Yam, J.W.P.; Mao, X. Dendritic cell vaccines: A shift from conventional approach to new generations. Cells 2023, 12, 2147. [Google Scholar] [CrossRef] [PubMed]
- Tojjari, A.; Saeed, A.; Singh, M.; Cavalcante, L.; Sahin, I.H.; Saeed, A. A comprehensive review on cancer vaccines and vaccine strategies in hepatocellular carcinoma. Vaccines 2023, 11, 1357. [Google Scholar] [CrossRef]
- Gutierrez-Sandoval, R.; Rivadeneira, I.; Gutierrez-Castro, F.; Sobarzo, A.; Muñoz, I.; Lagos, A.; Muñoz, N.; Krakowiak, F.; Aguilera, R.; Toledo, A. Decoding NAMPT and TIGAR: A molecular blueprint for reprogramming tumor metabolism and immunity. J. Clin. Oncol. 2025, 43 (Suppl. S16), e14537. [Google Scholar] [CrossRef]
- Cai, Y.; Prochazkova, M.; Kim, Y.S.; Jiang, C.; Ma, J.; Moses, L.; Martin, K.; Pham, V.; Zhang, N.; Highfill, S.L.; et al. Assessment and comparison of viability assays for cellular products. Cytotherapy 2024, 26, 201–209. [Google Scholar] [CrossRef]
- Mulkey, F.; Theoret, M.R.; Keegan, P.; Pazdur, R.; Sridhara, R. Comparison of iRECIST versus RECIST V.1.1 in patients treated with an anti-PD-1 or PD-L1 antibody: Pooled FDA analysis. J. Immunother. Cancer 2020, 8, e000146. [Google Scholar] [CrossRef]
- Ren, L.; Zhang, D.; Pang, L.; Liu, S. Extracellular vesicles for cancer therapy: Potential, progress, and clinical challenges. Front. Bioeng. Biotechnol. 2024, 12, 1476737. [Google Scholar] [CrossRef]
- Gu, Y.Z.; Zhao, X.; Song, X.R. Ex vivo pulsed dendritic cell vaccination against cancer. Acta Pharmacol. Sin. 2020, 41, 959–969. [Google Scholar] [CrossRef]
- Liu, C.; Yang, M.; Zhang, D.; Chen, M.; Zhu, D. Clinical cancer immunotherapy: Current progress and prospects. Front. Immunol. 2022, 13, 961805. [Google Scholar] [CrossRef]
- Connor, L.; Dean, J.; McNett, M.; Tydings, D.M.; Shrout, A.; Gorsuch, P.F.; Hole, A.; Moore, L.; Brown, R.; Melnyk, B.M.; et al. Evidence-based practice improves patient outcomes and healthcare system return on investment: Findings from a scoping review. Worldviews Evid. Based Nurs. 2023, 20, 6–15. [Google Scholar] [CrossRef]
- Gutiérrez-Sandoval, R.; Gutiérrez-Castro, F.; Muñoz-Godoy, N.; Rivadeneira, I.; Sobarzo, A.; Iturra, J.; Krakowiak, F.; Alarcón, L.; Dorado, W.; Lagos, A.; et al. Beyond Exosomes: An Ultrapurified Phospholipoproteic Complex (PLPC) as a Scalable Immunomodulatory Platform for Reprogramming Immune Suppression in Metastatic Cancer. Cancers 2025, 17, 1658. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Sandoval, R.; Gutiérrez-Castro, F.; Muñoz-Godoy, N.; Rivadeneira, I.; Sobarzo, A.; Alarcón, L.; Dorado, W.; Lagos, A.; Montenegro, D.; Muñoz, I.; et al. Phospholipid-Rich DC-Vesicles with Preserved Immune Fingerprints: A Stable and Scalable Platform for Precision Immunotherapy. Biomedicines 2025, 13, 1299. [Google Scholar] [CrossRef]
- Masucci, M.; Karlsson, C.; Blomqvist, L.; Ernberg, I. Bridging the divide: A review on the implementation of personalized cancer medicine. J. Pers. Med. 2024, 14, 561. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Paul, D.; Nath, V. Exosomes: Current knowledge and future perspectives. Tissue Barriers 2024, 12, 2232248. [Google Scholar] [CrossRef] [PubMed]
- Kern, S.; Skoog, I.; Ostling, S.; Kern, J.; Johansson, L.; Gudmundsson, P.; Waern, M.; Hultberg, B.; Rosengren, L.; Blennow, K.; et al. Cytokines for evaluation of chronic inflammatory status in ageing: A multiplex analysis of serum and cerebrospinal fluid. Immun. Ageing 2021, 16, 16. [Google Scholar]
- Mucherino, S.; Lorenzoni, V.; Orlando, V.; Triulzi, I.; Del Re, M.; Capuano, A.; Danesi, R.; Turchetti, G.; Menditto, E. Cost-effectiveness of treatment optimisation with biomarkers for immunotherapy in solid tumours: A systematic review protocol. BMJ Open 2024, 11, e048141. [Google Scholar] [CrossRef]
- Liu, R.; Zhao, Y.; Shi, F.; Zhu, J.; Wu, J.; Huang, M.; Qiu, K. Cost-effectiveness analysis of immune checkpoint inhibitors as first-line therapy in advanced biliary tract cancer. Immunotherapy 2024, 16, 669–678. [Google Scholar] [CrossRef]
- Gutierrez-Sandoval, R.; Gutierrez-Castro, F.; Rivadeneira, I.; Krakowiak, F.; Iturra, J. Advances in the translational application of immunotherapy with pulsed dendritic cell-derived exosomes. J. Clin. Biomed. Res. 2024, 6, 1–8. [Google Scholar] [CrossRef]
- Araujo-Abad, S.; Berna, J.M.; Lloret-Lopez, E.; López-Cortés, A.; Saceda, M.; de Juan Romero, C. Exosomes: From basic research to clinical diagnostic and therapeutic applications in cancer. Cell Oncol. 2025, 48, 269–293. [Google Scholar] [CrossRef]
- Zhang, B.; Xiao, G.; Mao, Y.Q.; Lv, Z.; Huang, R.P. Cytometry multiplex bead antibody array. Methods Mol. Biol. 2021, 2237, 83–92. [Google Scholar]
- Fu, P.; Yin, S.; Cheng, H.; Xu, W.; Jiang, J. Engineered exosomes for drug delivery in cancer therapy: A promising approach and application. Curr. Drug Deliv. 2024, 21, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Marciscano, A.E.; Anandasabapathy, N. The role of dendritic cells in cancer and anti-tumor immunity. Semin. Immunol. 2021, 52, 101481. [Google Scholar] [CrossRef] [PubMed]
- Ganjalikhani Hakemi, M.; Yanikkaya Demirel, G.; Li, Y.; Jayakumar, N. The immunosuppressive tumor microenvironment and strategies to revert its immune regulatory milieu for cancer immunotherapy. Front. Immunol. 2023, 14, 1238698. [Google Scholar] [CrossRef] [PubMed]
- Huangfu, S.; Pan, J. Novel biomarkers for predicting response to cancer immunotherapy. Front. Immunol. 2023, 14, 1179913. [Google Scholar] [CrossRef]
- Karlsen, W.; Akily, L.; Mierzejewska, M.; Teodorczyk, J.; Bandura, A.; Zaucha, R.; Cytawa, W. Is 18F-FDG-PET/CT an optimal imaging modality for detecting immune-related adverse events after immune-checkpoint inhibitor therapy? Pros and cons. Cancers 2024, 16, 1990. [Google Scholar] [CrossRef]
- Khan, F.; Lin, Y.; Ali, H.; Pang, L.; Dunterman, M.; Hsu, W.H.; Frenis, K.; Grant Rowe, R.; Wainwright, D.A.; McCortney, K.; et al. Lactate dehydrogenase A regulates tumor-macrophage symbiosis to promote glioblastoma progression. Nat. Commun. 2023, 15, 1987. [Google Scholar] [CrossRef]
- Sidiropoulos, D.N.; Stein-O’Brien, G.L.; Danilova, L.; Gross, N.E.; Charmsaz, S.; Xavier, S.; Leatherman, J.; Wang, H.; Yarchoan, M.; Jaffee, E.M.; et al. Integrated T cell cytometry metrics for immune-monitoring applications in immunotherapy clinical trials. JCI Insight 2022, 7, e160398. [Google Scholar] [CrossRef]
- Kankeu Fonkoua, L.A.; Sirpilla, O.; Sakemura, R.; Siegler, E.L.; Kenderian, S.S. CAR T cell therapy and the tumor microenvironment: Current challenges and opportunities. Mol. Ther. Oncolytics 2022, 25, 69–77. [Google Scholar] [CrossRef]
- Safaei, S.; Fadaee, M.; Farzam, O.R.; Yari, A.; Poursaei, E.; Aslan, C.; Samemaleki, S.; Shanehbandi, D.; Baradaran, B.; Kazemi, T. Exploring the dynamic interplay between exosomes and the immune tumor microenvironment: Implications for breast cancer progression and therapeutic strategies. Breast Cancer Res. 2024, 26, 57. [Google Scholar] [CrossRef]
- Louie, A.D.; Huntington, K.; Carlsen, L.; Zhou, L.; El-Deiry, W.S. Integrating molecular biomarker inputs into development and use of clinical cancer therapeutics. Front. Pharmacol. 2021, 12, 747194. [Google Scholar] [CrossRef]
- Ayoub, M.; Eleneen, Y.; Colen, R.R. Cancer imaging in immunotherapy. Adv. Exp. Med. Biol. 2020, 1244, 309–324. [Google Scholar] [PubMed]
- Bergholz, J.S.; Wang, Q.; Kabraji, S.; Zhao, J.J. Integrating immunotherapy and targeted therapy in cancer treatment: Mechanistic insights and clinical implications. Clin. Cancer Res. 2020, 26, 5557–5566. [Google Scholar] [CrossRef] [PubMed]
- Abou-El-Enein, M.; Elsallab, M.; Feldman, S.A.; Fesnak, A.D.; Heslop, H.E.; Marks, P.; Till, B.G.; Bauer, G.; Savoldo, B. Scalable manufacturing of CAR T cells for cancer immunotherapy. Blood Cancer Discov. 2021, 2, 408–422. [Google Scholar] [CrossRef] [PubMed]
- Chapman, N.M.; Boothby, M.R.; Chi, H. Metabolic coordination of T cell quiescence and activation. Nat. Rev. Immunol. 2020, 20, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Sarna, N.S.; Desai, S.H.; Kaufman, B.G.; Curry, N.M.; Hanna, A.M.; King, M.R. Enhanced and sustained T cell activation in response to fluid shear stress. iScience 2024, 27, 109999. [Google Scholar] [CrossRef]
- Ding, Z.; Li, Q.; Zhang, R.; Xie, L.; Shu, Y.; Gao, S.; Wang, P.; Su, X.; Qin, Y.; Wang, Y.; et al. Personalized neoantigen pulsed dendritic cell vaccine for advanced lung cancer. Signal Transduct. Target. Ther. 2021, 6, 26. [Google Scholar] [CrossRef]
- Dong, C. Cytokine regulation and function in T cells. Annu. Rev. Immunol. 2021, 39, 51–76. [Google Scholar] [CrossRef]
- Xu, Z.; Zeng, S.; Gong, Z.; Chen, Y.; Zhang, W.; Liu, T.; Wang, X. Exosome-based immunotherapy: A promising approach for cancer treatment. Mol. Cancer 2020, 19, 160. [Google Scholar] [CrossRef]
- Mishra, R.; Sharma, S.; Arora, N. TLR-5 ligand conjugated with Per a 10 and T cell peptides potentiates Treg/Th1 response through PI3K/mTOR axis. Int. Immunopharmacol. 2022, 113, 109389. [Google Scholar] [CrossRef]
- Wu, J.; Shen, Z. Exosomal miRNAs as biomarkers for diagnostic and prognostic in lung cancer. Cancer Med. 2020, 9, 6909–6922. [Google Scholar] [CrossRef]
- Saida, Y.; Watanabe, S.; Koyama, S.; Togashi, Y.; Kikuchi, T. Strategies to overcome tumor evasion and resistance to immunotherapies by targeting immune suppressor cells. Front. Oncol. 2023, 13, 1240926. [Google Scholar] [CrossRef] [PubMed]
- Sheikhlary, S.; Lopez, D.H.; Moghimi, S.; Sun, B. Recent findings on therapeutic cancer vaccines: An updated review. Biomolecules 2024, 14, 503. [Google Scholar] [CrossRef]
- Bano, A.; Vats, R.; Verma, D.; Yadav, P.; Kamboj, M.; Bhardwaj, R. Exploring salivary exosomes as early predictors of oral cancer in susceptible tobacco consumers: Noninvasive diagnostic and prognostic applications. J. Cancer Res. Clin. Oncol. 2023, 149, 15781–15793. [Google Scholar] [CrossRef] [PubMed]
- Nikolic, T.; Suwandi, J.S.; Wesselius, J.; Laban, S.; Joosten, A.M.; Sonneveld, P.; Mul, D.; Aanstoot, H.J.; Kaddis, J.S.; Zwaginga, J.J.; et al. Tolerogenic dendritic cells pulsed with islet antigen induce long-term reduction in T-cell autoreactivity in type 1 diabetes patients. Front. Immunol. 2022, 13, 1054968. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Zhou, Y.; Yokota, Y.; Matsumoto, Y.; Zhai, B.; Maarouf, N.; Hayashi, H.; Carlson, R.; Zhang, S.; Sousa, A.; et al. Adaptive antitumor immune response stimulated by bio-nanoparticle based vaccine and checkpoint blockade. J. Exp. Clin. Cancer Res. 2022, 41, 132. [Google Scholar] [CrossRef]
- Deng, M.; Wu, S.; Huang, P.; Liu, Y.; Li, C.; Zheng, J. Engineered exosomes-based theranostic strategy for tumor metastasis and recurrence. Asian J. Pharm. Sci. 2023, 18, 100870. [Google Scholar] [CrossRef]
- Berz, A.M.; Dromain, C.; Vietti-Violi, N.; Boughdad, S.; Duran, R. Tumor response assessment on imaging following immunotherapy. Front. Oncol. 2022, 12, 982983. [Google Scholar] [CrossRef]
- Shalaby, N.; Dubois, V.P.; Ronald, J. Molecular imaging of cellular immunotherapies in experimental and therapeutic settings. Cancer Immunol. Immunother. 2021, 71, 1281–1294. [Google Scholar] [CrossRef]
- Reindl, M.; Schanda, K.; Woodhall, M.; Tea, F.; Ramanathan, S.; Sagen, J.; Fryer, J.P.; Mills, J.; Teegen, B.; Mindorf, S.; et al. International multicenter examination of MOG antibody assays. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7, e674. [Google Scholar] [CrossRef]
- Ratziu, V.; Hompesch, M.; Petitjean, M.; Serdjebi, C.; Iyer, J.S.; Parwani, A.V.; Tai, D.; Bugianesi, E.; Cusi, K.; Friedman, S.L.; et al. Artificial intelligence-assisted digital pathology for non-alcoholic steatohepatitis: Current status and future directions. J. Hepatol. 2024, 80, 335–351. [Google Scholar] [CrossRef]
- Das, S.; Dey, M.K.; Devireddy, R.; Gartia, M.R. Biomarkers in cancer detection, diagnosis, and prognosis. Sensors 2023, 24, 37. [Google Scholar] [CrossRef] [PubMed]
- Bhavsar, D.; Raguraman, R.; Kim, D.; Ren, X.; Munshi, A.; Moore, K.; Sikavitsas, V.; Ramesh, R. Exosomes in diagnostic and therapeutic applications of ovarian cancer. J. Ovarian Res. 2024, 17, 113. [Google Scholar] [CrossRef]
- Pham, T.D.; Teh, M.T.; Chatzopoulou, D.; Holmes, S.; Coulthard, P. Artificial intelligence in head and neck cancer: Innovations, applications, and future directions. Curr. Oncol. 2024, 31, 5255–5290. [Google Scholar] [CrossRef]
- Wandrey, M.; Jablonska, J.; Stauber, R.H.; Gül, D. Exosomes in cancer progression and therapy resistance: Molecular insights and therapeutic opportunities. Life 2023, 13, 2033. [Google Scholar] [CrossRef]
- Yao, Y.; Fu, C.; Zhou, L.; Mi, Q.S.; Jiang, A. DC-derived exosomes for cancer immunotherapy. Cancers 2021, 13, 3667. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Lin, Q.; Li, C.; Qiu, Y.; Chen, J.; Zhu, X. Comprehensive analysis of the prognostic implication and immune infiltration of CISD2 in diffuse large B-cell lymphoma. Front. Immunol. 2023, 14, 1277695. [Google Scholar] [CrossRef]
- Mu, W.; Jiang, L.; Shi, Y.; Tunali, I.; Gray, J.E.; Katsoulakis, E.; Tian, J.; Gillies, R.J.; Schabath, M.B. Non-invasive measurement of PD-L1 status and prediction of immunotherapy response using deep learning of PET/CT images. J. Immunother. Cancer 2021, 9, e002118. [Google Scholar] [CrossRef] [PubMed]
- Baughman, D.J.; Botros, P.A.; Waheed, A. Technology in medicine: Improving clinical documentation. FP Essent. 2024, 537, 26–38. [Google Scholar]
- Corbetta, L.; Arru, L.B.; Mereu, C.; Pasini, V.; Patelli, M. Competence and training in interventional pulmonology. Panminerva Med. 2019, 61, 203–231. [Google Scholar]
- Cossarizza, A.; Chang, H.D.; Radbruch, A.; Acs, A.; Adam, D.; Adam-Klages, S.; Agace, W.W.; Aghaeepour, N.; Akdis, M.; Allez, M.; et al. Guidelines for the use of flow cytometry and cell sorting in immunological studies (second edition). Eur. J. Immunol. 2019, 49, 1457–1973. [Google Scholar]
- Pathania, A.S.; Prathipati, P.; Challagundla, K.B. New insights into exosome mediated tumor-immune escape: Clinical perspectives and therapeutic strategies. Biochim. Biophys. Acta Rev. Cancer 2021, 1876, 188624. [Google Scholar] [CrossRef] [PubMed]
- Vu, S.H.; Vetrivel, P.; Kim, J.; Lee, M.S. Cancer resistance to immunotherapy: Molecular mechanisms and tackling strategies. Int. J. Mol. Sci. 2022, 23, 10906. [Google Scholar] [CrossRef] [PubMed]
- Zanotta, S.; Galati, D.; De Filippi, R.; Pinto, A. Enhancing dendritic cell cancer vaccination: The synergy of immune checkpoint inhibitors in combined therapies. Int. J. Mol. Sci. 2024, 25, 7509. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari Laleh, N.; Ligero, M.; Perez-Lopez, R.; Kather, J.N. Facts and hopes on the use of artificial intelligence for predictive immunotherapy biomarkers in cancer. Clin. Cancer Res. 2023, 29, 316–323. [Google Scholar] [CrossRef]
- Lai, J.J.; Chau, Z.L.; Chen, S.Y.; Hill, J.J.; Korpany, K.V.; Liang, N.W.; Lin, L.H.; Liu, J.K. Exosome processing and characterization approaches for research and technology development. Adv. Sci. 2022, 9, e2103222. [Google Scholar] [CrossRef]
- Bhinder, B.; Gilvary, C.; Madhukar, N.S.; Elemento, O. Artificial intelligence in cancer research and precision medicine. Cancer Discov. 2021, 11, 900–915. [Google Scholar] [CrossRef]
- Walcher, L.; Kistenmacher, A.K.; Suo, H.; Kitte, R.; Dluczek, S.; Strauß, A.; Blaudszun, A.R.; Yevsa, T.; Fricke, S.; Kossatz-Boehlert, U. Cancer stem cells—Origins and biomarkers: Perspectives for targeted personalized therapies. Front. Immunol. 2020, 11, 1280. [Google Scholar] [CrossRef]
- Zhou, Z.; Wang, J.; Wang, J.; Yang, S.; Wang, R.; Zhang, G.; Li, Z.; Shi, R.; Wang, Z.; Lu, Q. Deciphering the tumor immune microenvironment from a multidimensional omics perspective: Insight into next-generation CAR-T cell immunotherapy and beyond. Mol. Cancer 2024, 23, 131. [Google Scholar] [CrossRef]
- Song, M.S.; Nam, J.H.; Noh, K.E.; Lim, D.S. Dendritic cell-based immunotherapy: The importance of dendritic cell migration. J. Immunol. Res. 2024, 2024, 7827246. [Google Scholar] [CrossRef]
- Jendle, J.; Reznik, Y. Use of insulin pumps and closed-loop systems among people living with diabetes: A narrative review of clinical and cost-effectiveness to enable access to technology and meet the needs of payers. Diabetes Obes. Metab. 2023, 25 (Suppl. S2), 21–32. [Google Scholar] [CrossRef]
- Makler, A.; Asghar, W. Exosomal biomarkers for cancer diagnosis and patient monitoring. Expert Rev. Mol. Diagn. 2020, 20, 387–400. [Google Scholar] [CrossRef] [PubMed]
- Chow, A.; Perica, K.; Klebanoff, C.A.; Wolchok, J.D. Clinical implications of T cell exhaustion for cancer immunotherapy. Nat. Rev. Clin. Oncol. 2022, 19, 775–790. [Google Scholar] [CrossRef]
- Liu, Q.; Li, S.; Dupuy, A.; Mai, H.L.; Sailliet, N.; Logé, C.; Robert, J.H.; Brouard, S. Exosomes as new biomarkers and drug delivery tools for the prevention and treatment of various diseases. Int. J. Mol. Sci. 2021, 22, 7763. [Google Scholar] [CrossRef]
- Hato, L.; Vizcay, A.; Eguren, I.; Pérez-Gracia, J.L.; Rodríguez, J.; Gállego Pérez-Larraya, J.; Sarobe, P.; Inogés, S.; Díaz de Cerio, A.L.; Santisteban, M. Dendritic cells in cancer immunology and immunotherapy. Cancers 2024, 16, 981. [Google Scholar] [CrossRef]
- Sajan, A.; Lamane, A.; Baig, A.; Floch, K.L.; Dercle, L. The emerging role of AI in enhancing intratumoral immunotherapy care. Oncotarget 2024, 15, 635–637. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, Q.; Qin, F.; Chen, J. Exosomes: A promising avenue for cancer diagnosis beyond treatment. Front. Cell Dev. Biol. 2024, 12, 1344705. [Google Scholar] [CrossRef] [PubMed]
- Zhao, N.; Yi, Y.; Cao, W.; Fu, X.; Mei, N.; Li, C. Serum cytokine levels for predicting immune-related adverse events and the clinical response in lung cancer treated with immunotherapy. Front. Oncol. 2022, 12, 923531. [Google Scholar] [CrossRef]
- Kamigaki, T.; Takimoto, R.; Okada, S.; Ibe, H.; Oguma, E.; Goto, S. Personalized dendritic-cell-based vaccines targeting cancer neoantigens. Anticancer Res. 2024, 44, 3713–3724. [Google Scholar] [CrossRef]
- Wolf, D.M.; Yau, C.; Wulfkuhle, J.; Brown-Swigart, L.; Gallagher, R.I.; Lee, P.R.E.; Zhu, Z.; Magbanua, M.J.; Sayaman, R.; O’Grady, N.; et al. Redefining breast cancer subtypes to guide treatment prioritization and maximize response: Predictive biomarkers across 10 cancer therapies. Cancer Cell 2022, 40, 609–623.e6. [Google Scholar] [CrossRef]
- Luo, S.; Chen, J.; Xu, F.; Chen, H.; Li, Y.; Li, W. Dendritic cell-derived exosomes in cancer immunotherapy. Pharmaceutics 2023, 15, 2070. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Marker | Description | Evaluation Method | Expected Value |
|---|---|---|---|
| CD69 | Early marker of T-cell activation | Flow cytometry | >70% activated lymphocytes |
| CD25 | Late activation marker; α-chain of IL-2 receptor | Flow cytometry | >60% activated lymphocytes |
| HLA-DR | Maturation marker for dendritic cells | Flow cytometry | High expression (>80%) |
| IFN-γ | Key cytokine for Th1 polarization | Cytometric Bead Array (CBA) | 100–150 pg/mL |
| IL-12 | Cytokine for induction of Th1 immune profile | CBA | >80 pg/mL |
| Parameter | Description | Evaluation Method | Optimal Range |
|---|---|---|---|
| Size | Average diameter of exosomes | NTA | 100–150 nm |
| Concentration | Number of exosomes per mL of sample | NTA | >109 particles/mL |
| CD63 | Exosome-specific surface marker | Western blotting | Positive expression |
| CD81 | Extracellular vesicle marker | Western blotting | Positive expression |
| Alix | Marker of exosome integrity and biogenesis | Western blotting | Positive expression |
| Calnexin | Negative control for exosomal purity | Western blotting | Not detected |
| Parameter | Expected Value | Clinical Meaning | Suggested Action |
|---|---|---|---|
| CD69 < 50% | Low T-cell activation | Suboptimal immune engagement | Increase DC dose or adjuvant |
| IFN-γ < 80 pg/mL | Weak Th1 response | Reduced cytotoxicity | Consider IL-12 co-stimulation |
| IL-10 > 200 pg/mL | Dominant Th2 suppression | Risk of immune escape | Adjust antigen load or regimen |
| IL-6 > 500 pg/mL | Inflammatory toxicity | Excessive immune activation | Delay next dose; modulate cytokines |
| Monitoring Technique | Operational Complexity | Functional Contribution |
|---|---|---|
| Flow cytometry | High | High-resolution quantification of immune activation markers (e.g., CD69, CD25, and HLA-DR) |
| PET-CT with 18F-FDG | Very high | Sensitive detection of early metabolic tumor responses and treatment-associated dynamics |
| Nanoparticle Tracking Analysis | Moderate | Characterization of exosome size distribution and concentration (standardized QC metric) |
| No. | Stage | Day | Sample | Exam | Purpose |
|---|---|---|---|---|---|
| 1 | Isolation of PBMCs | Day 1 | Peripheral blood | Ficoll density gradient separation | Obtain viable PBMCs suitable for DC differentiation and immunomonitoring workflows |
| 2 | Cell viability and integrity | Day 1 | Isolated PBMNCs | Trypan Blue or Annexin V assay | Confirm cell viability (>95%) and baseline functional status |
| 3 | DC differentiation | Day 7 | PBMC culture | Flow cytometry: HLA-DR, CD123, CD11c | Verify phenotypic markers indicating effective differentiation into immature DCs |
| 4 | DC maturation | Day 10 | Immature DCs | Flow cytometry: CD80, CD83, CD86 | Confirm maturation capacity and readiness for lymphocyte co-culture |
| 5 | Exosome harvest and QC | Day 12 | DC secretome | NTA for size/concentration | Validate exosome yield and structural uniformity (90–120 nm) |
| 6 | Immunopotency profiling | Day 12 | DC secretome | CBA: Th1, Th2, Th17 cytokines | Evaluate cytokine patterns supporting immune polarization capacity |
| 7 | Lymphocyte activation | Day 14 | DCs and/or exosomes co-cultured with T cells | Flow cytometry: CD69, CD25 | Confirm T-cell activation and effector induction |
| 8 | Tumor apoptosis induction | Day 14 | Activated T cells + tumor cell co-culture | LDH, caspase activity assays | Measure tumor cell apoptosis as endpoint of immune activation |
| 9 | Final product validation | Day 14 | Enriched exosome concentrate | Safety, membrane integrity, surface marker validation | Ensure compliance with quality and biosafety standards prior to clinical use |
| Immune Profile | Key Cytokines | Impact on Therapy |
|---|---|---|
| Th1 | IFN-γ, IL-12 | Promotes robust cytotoxic response; enhances T-cell activation and tumor clearance |
| Th2 | IL-4, IL-10 | May suppress cytotoxic responses; potentially reduces therapeutic efficacy |
| Th17 | IL-6, IL-17A | Associated with pro-inflammatory responses; requires modulation to minimize adverse effects |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez-Sandoval, R.; Gutiérrez-Castro, F.; Muñoz-Godoy, N.; Rivadeneira, I.; Sobarzo, A.; Alarcón, L.; Dorado, W.; Lagos, A.; Montenegro, D.; Muñoz, I.; et al. The Design of a Multistage Monitoring Protocol for Dendritic Cell-Derived Exosome (DEX) Immunotherapy: A Conceptual Framework for Molecular Quality Control and Immune Profiling. Int. J. Mol. Sci. 2025, 26, 5444. https://doi.org/10.3390/ijms26125444
Gutiérrez-Sandoval R, Gutiérrez-Castro F, Muñoz-Godoy N, Rivadeneira I, Sobarzo A, Alarcón L, Dorado W, Lagos A, Montenegro D, Muñoz I, et al. The Design of a Multistage Monitoring Protocol for Dendritic Cell-Derived Exosome (DEX) Immunotherapy: A Conceptual Framework for Molecular Quality Control and Immune Profiling. International Journal of Molecular Sciences. 2025; 26(12):5444. https://doi.org/10.3390/ijms26125444
Chicago/Turabian StyleGutiérrez-Sandoval, Ramón, Francisco Gutiérrez-Castro, Natalia Muñoz-Godoy, Ider Rivadeneira, Adolay Sobarzo, Luis Alarcón, Wilson Dorado, Andy Lagos, Diego Montenegro, Ignacio Muñoz, and et al. 2025. "The Design of a Multistage Monitoring Protocol for Dendritic Cell-Derived Exosome (DEX) Immunotherapy: A Conceptual Framework for Molecular Quality Control and Immune Profiling" International Journal of Molecular Sciences 26, no. 12: 5444. https://doi.org/10.3390/ijms26125444
APA StyleGutiérrez-Sandoval, R., Gutiérrez-Castro, F., Muñoz-Godoy, N., Rivadeneira, I., Sobarzo, A., Alarcón, L., Dorado, W., Lagos, A., Montenegro, D., Muñoz, I., Aguilera, R., Iturra, J., Krakowiak, F., Peña-Vargas, C., & Toledo, A. (2025). The Design of a Multistage Monitoring Protocol for Dendritic Cell-Derived Exosome (DEX) Immunotherapy: A Conceptual Framework for Molecular Quality Control and Immune Profiling. International Journal of Molecular Sciences, 26(12), 5444. https://doi.org/10.3390/ijms26125444