
The Utility of Miniaturized Adsorbers in Exploring the Cellular and Molecular Effects of Blood Purification: A Pilot Study with a Focus on Immunoadsorption in Multiple Sclerosis

 , ,
, , 
Abstract
1. Introduction
2. Results
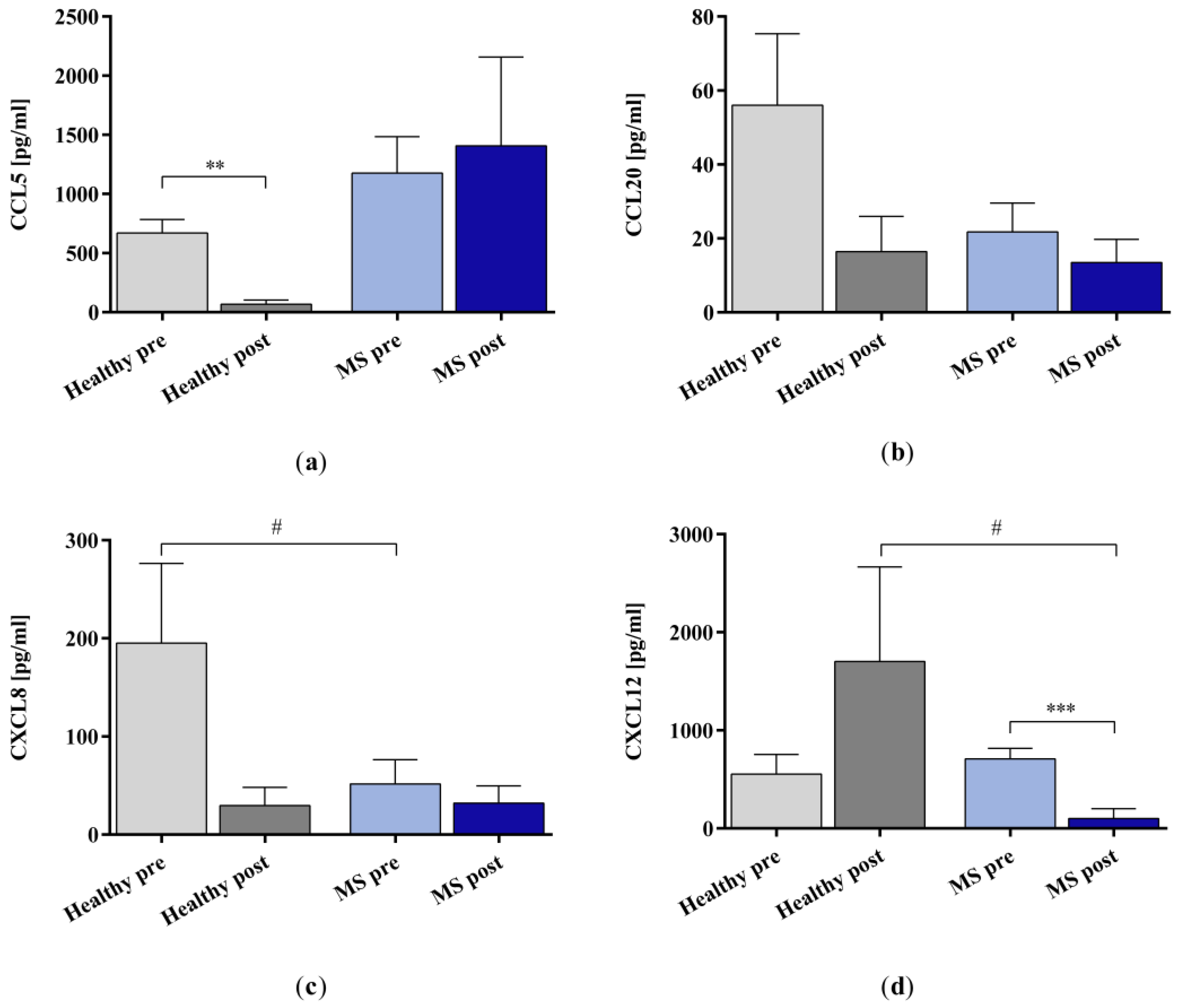
2.1. Removal of Selected Target Molecules by In Vitro IA
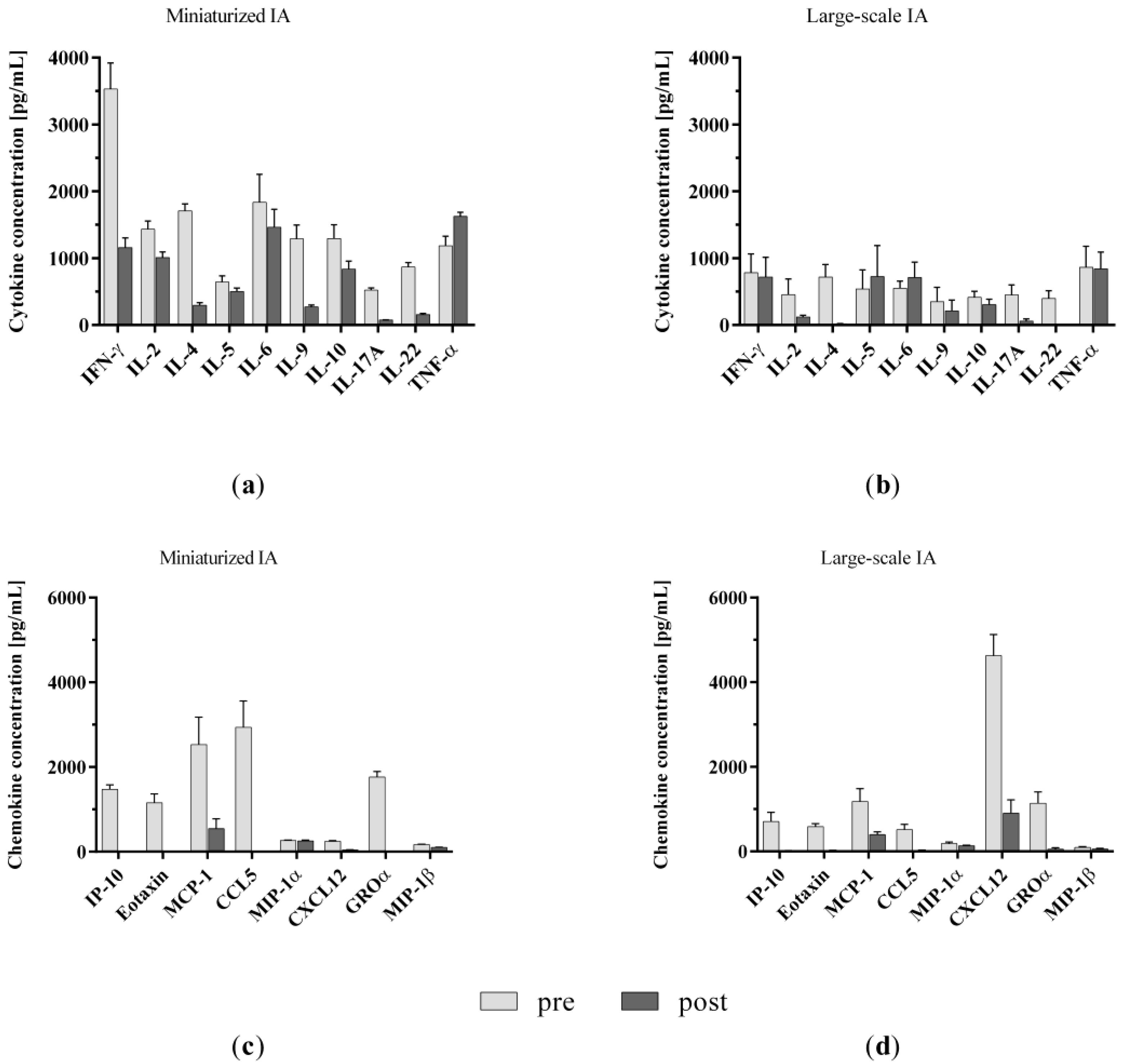
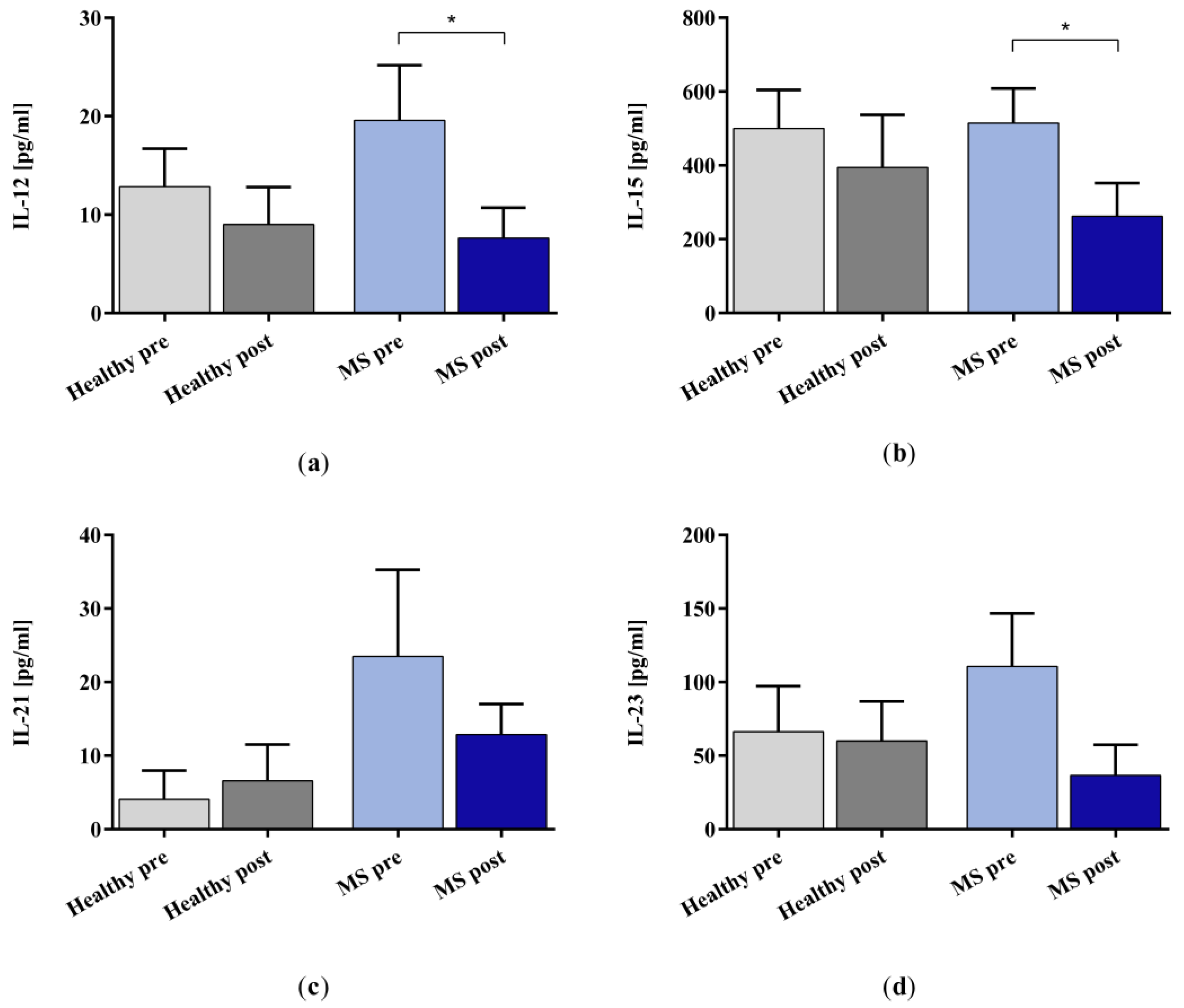
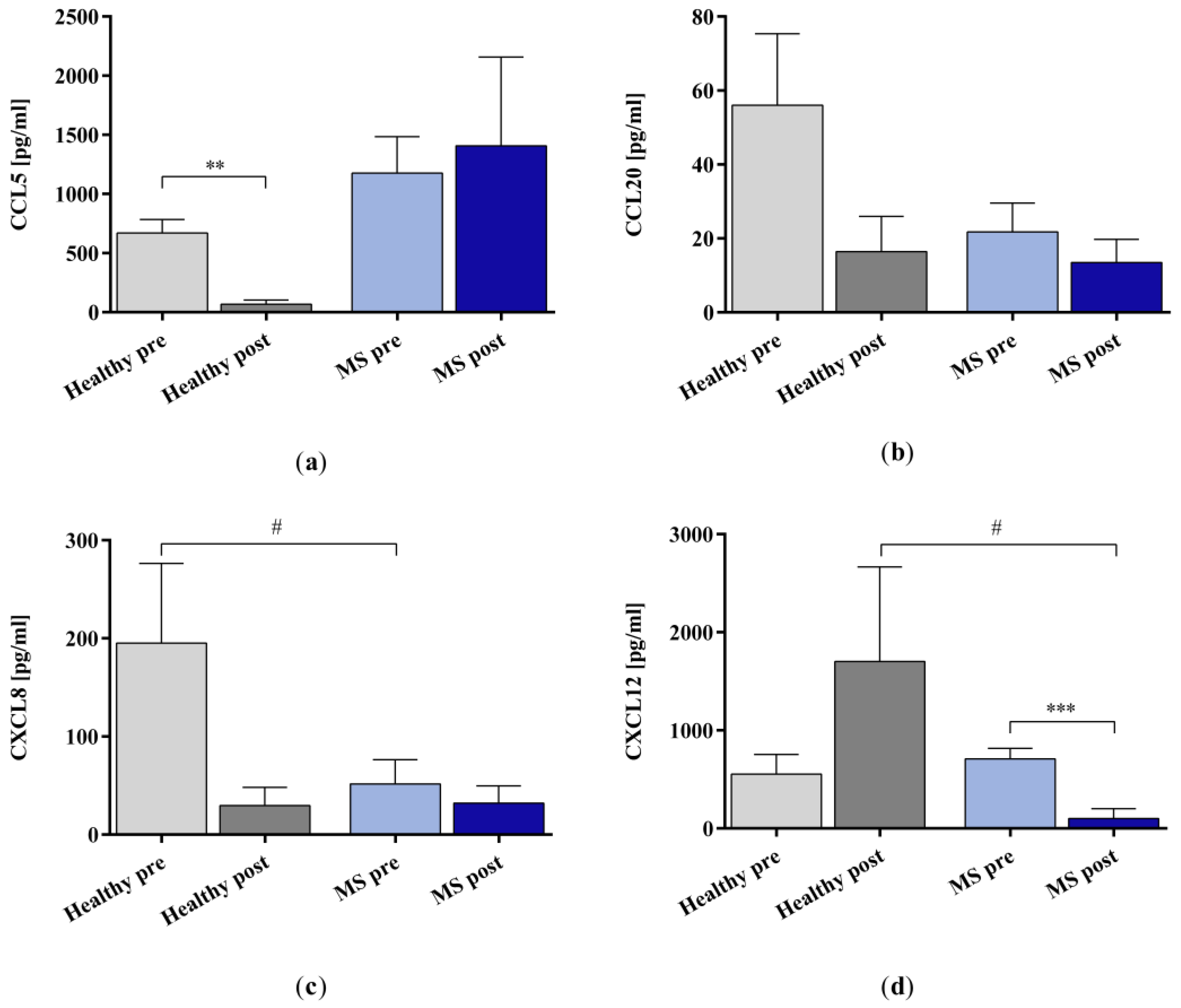
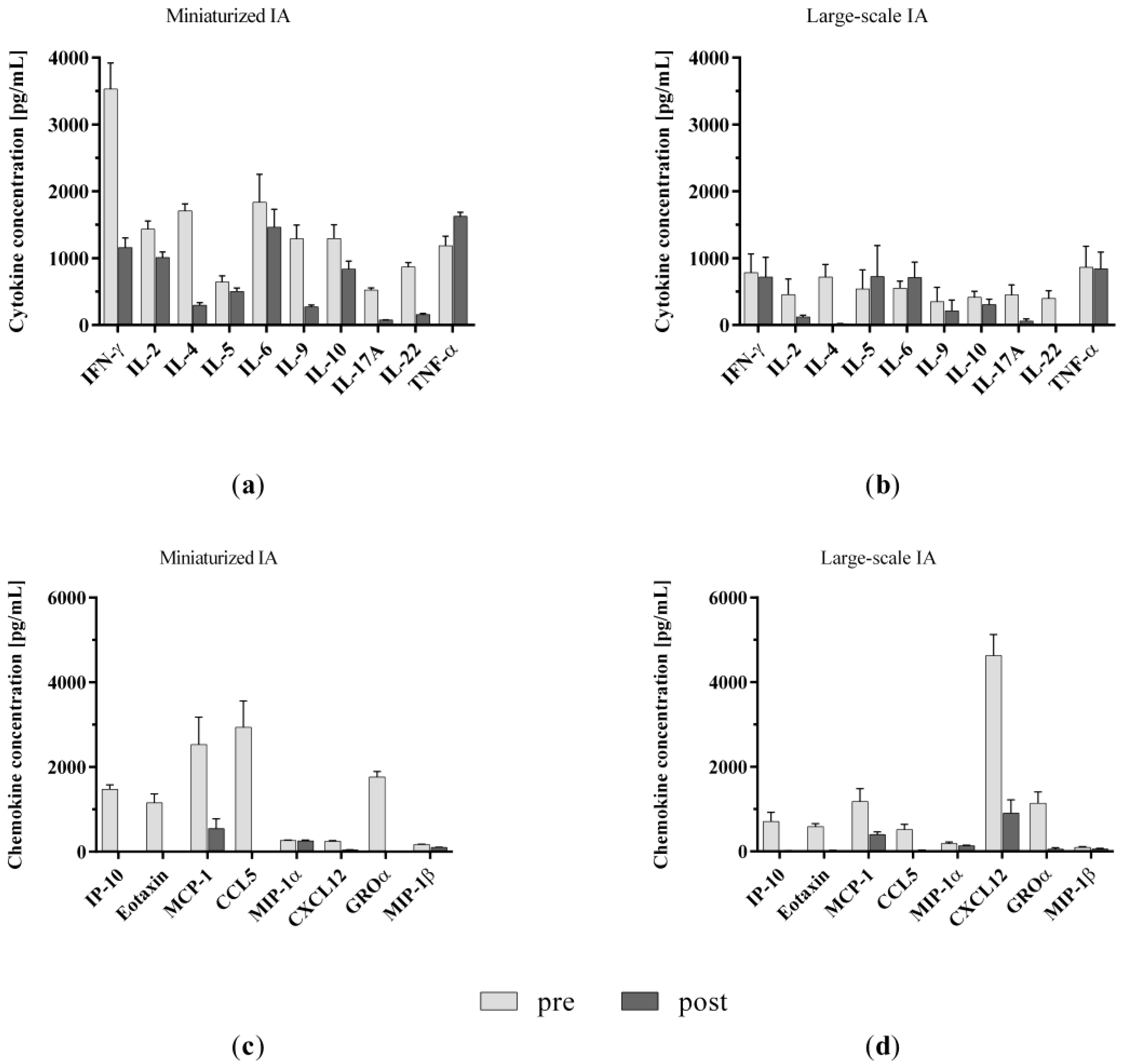
2.1.1. Cytokines and Chemokines
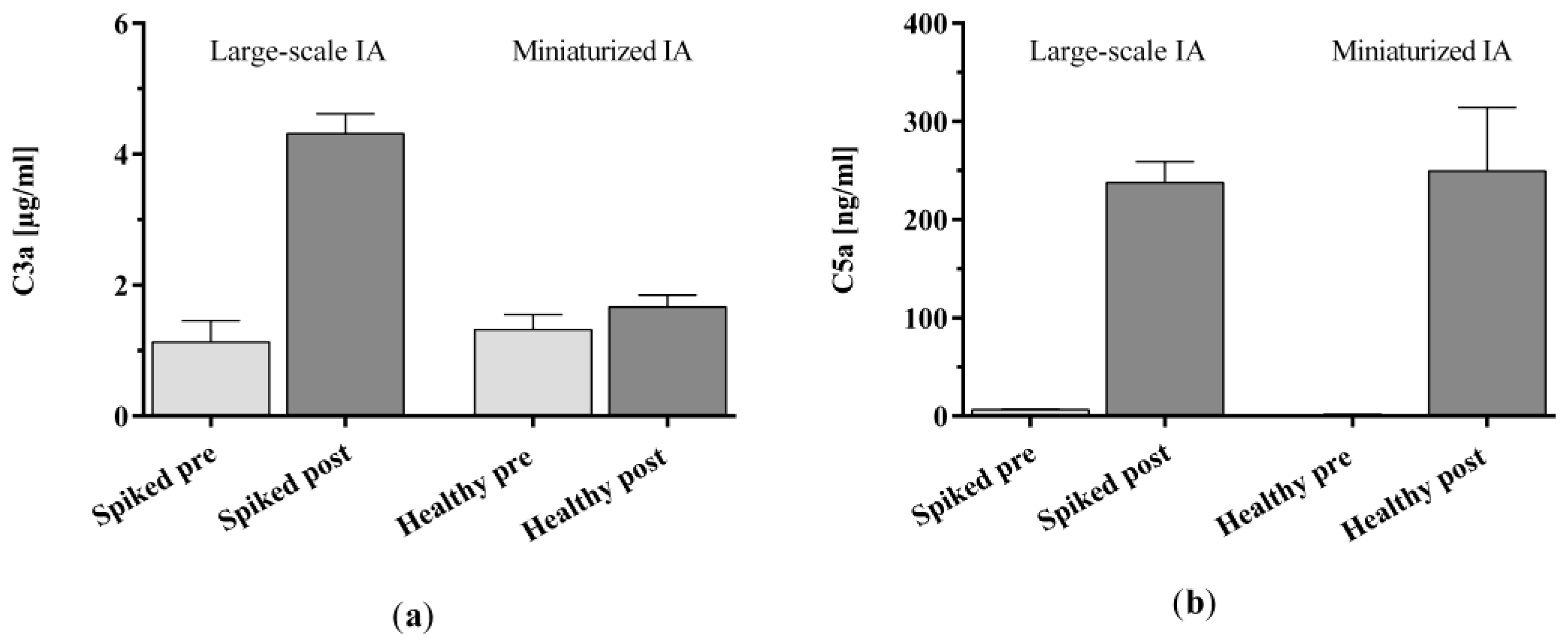
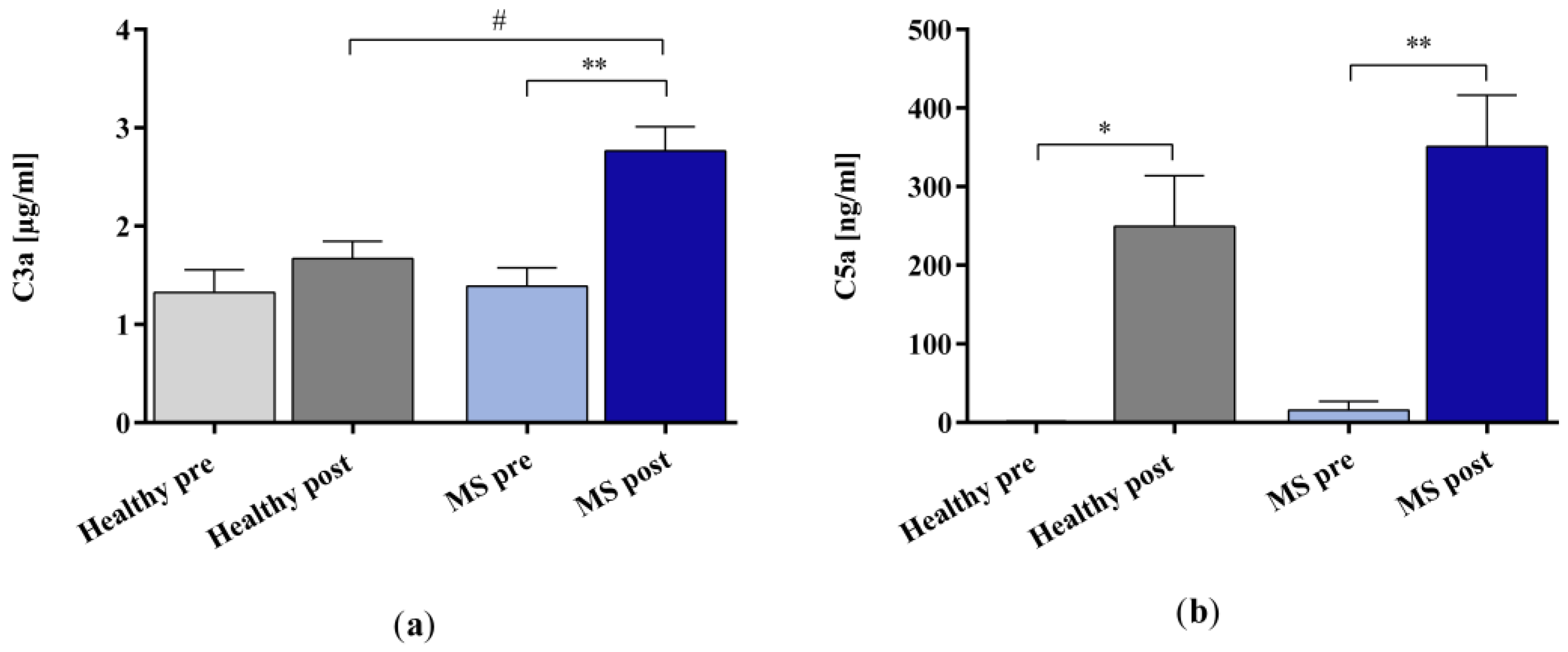
2.1.2. Complement Factors
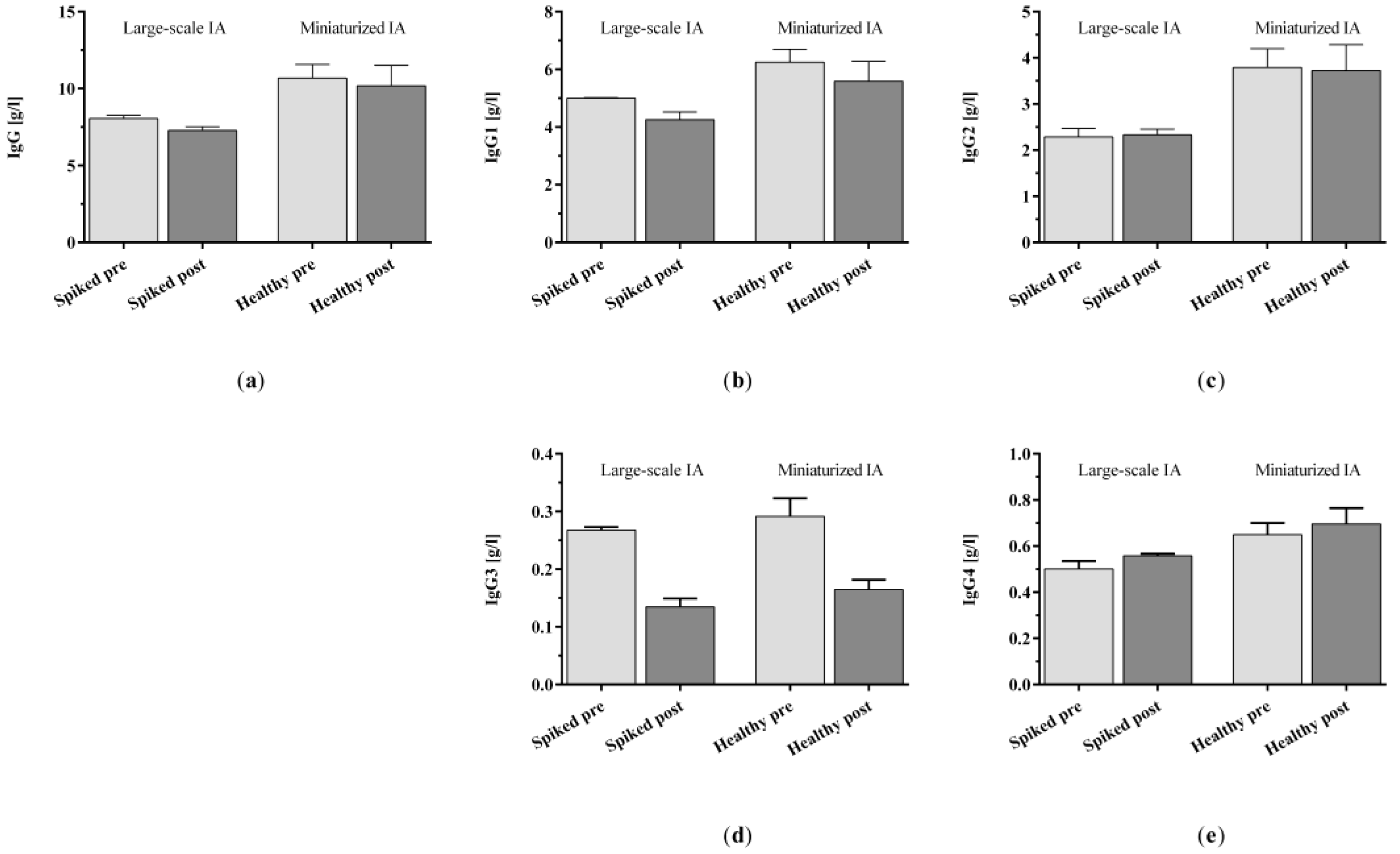
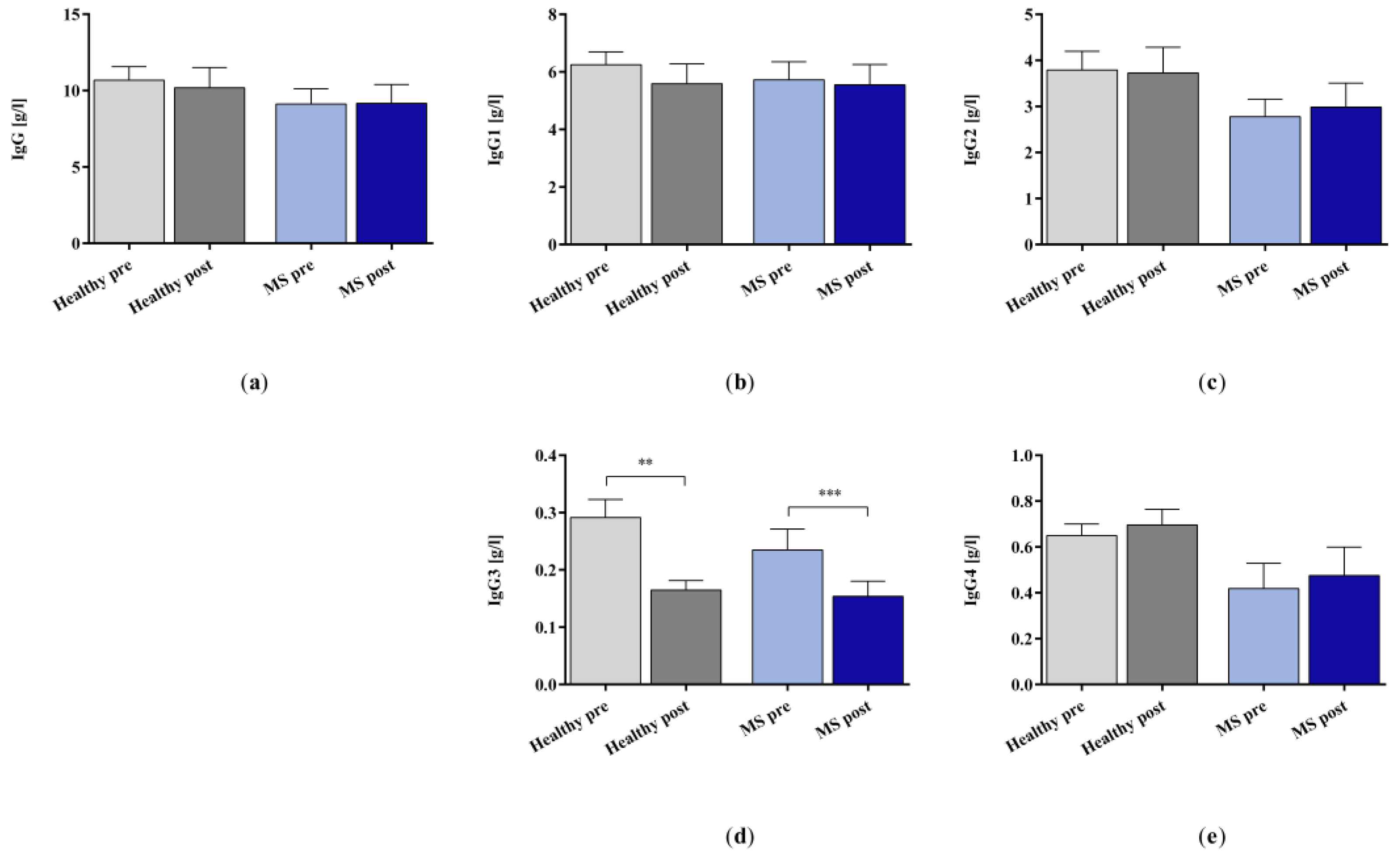
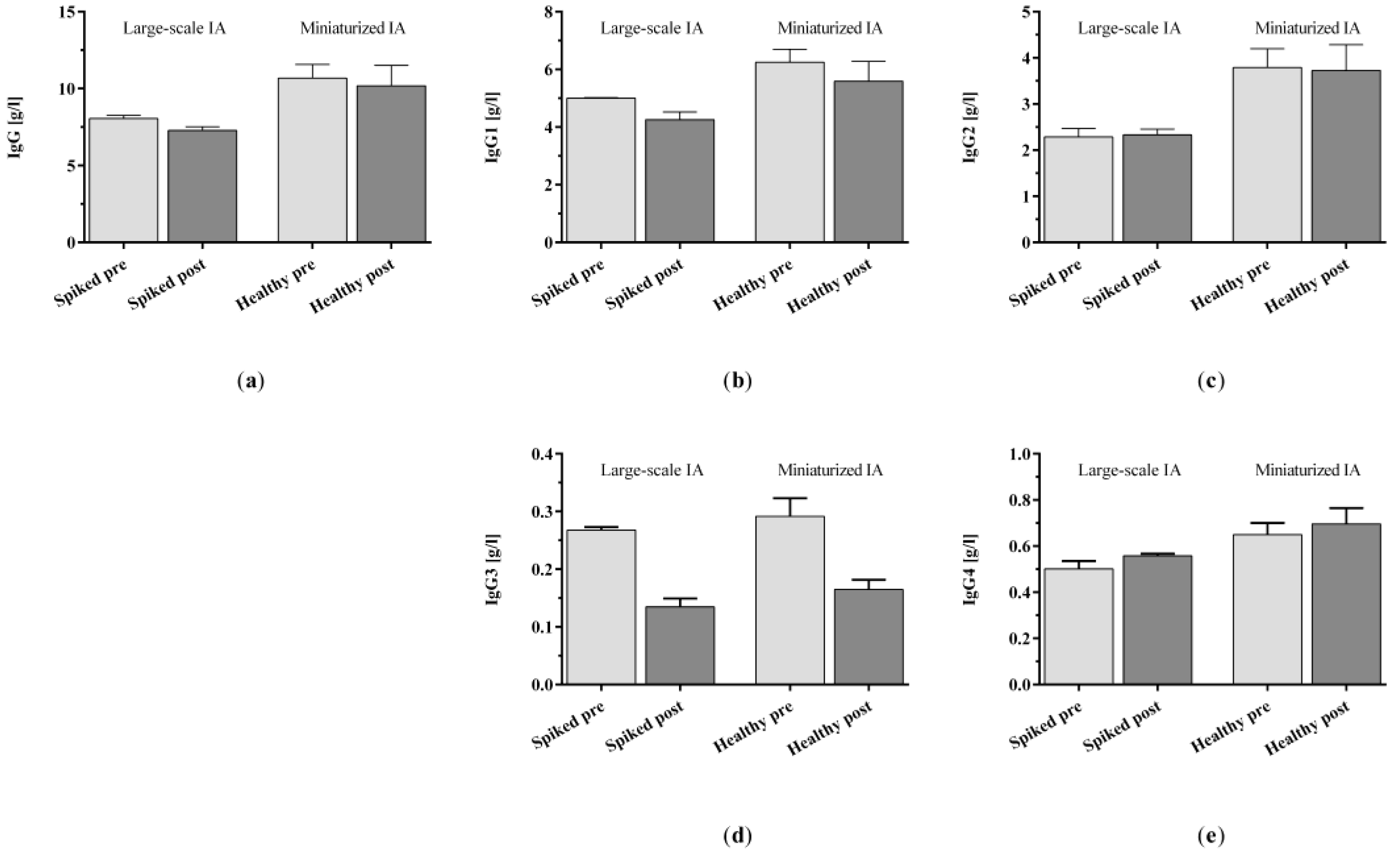
2.1.3. IgG and IgG Subclasses 1–4
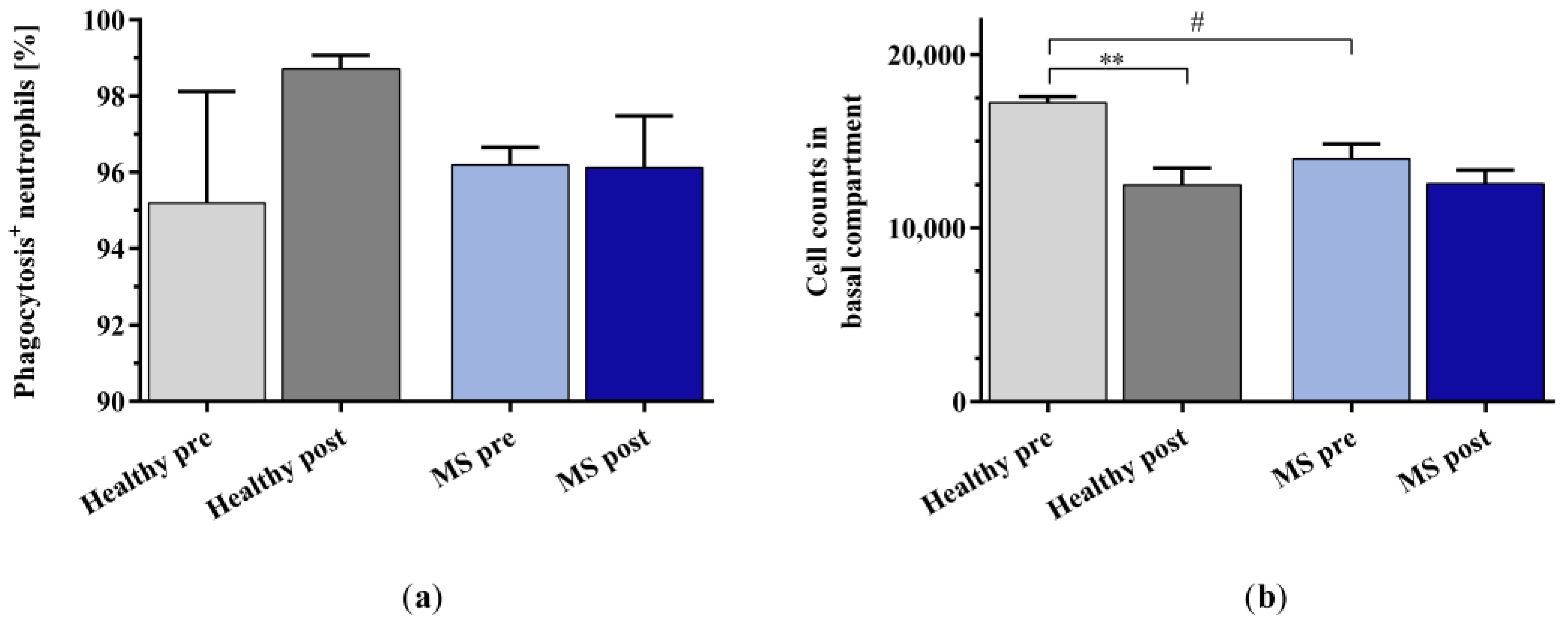
2.2. Effect of In Vitro IA Treatment on Neutrophil Migration
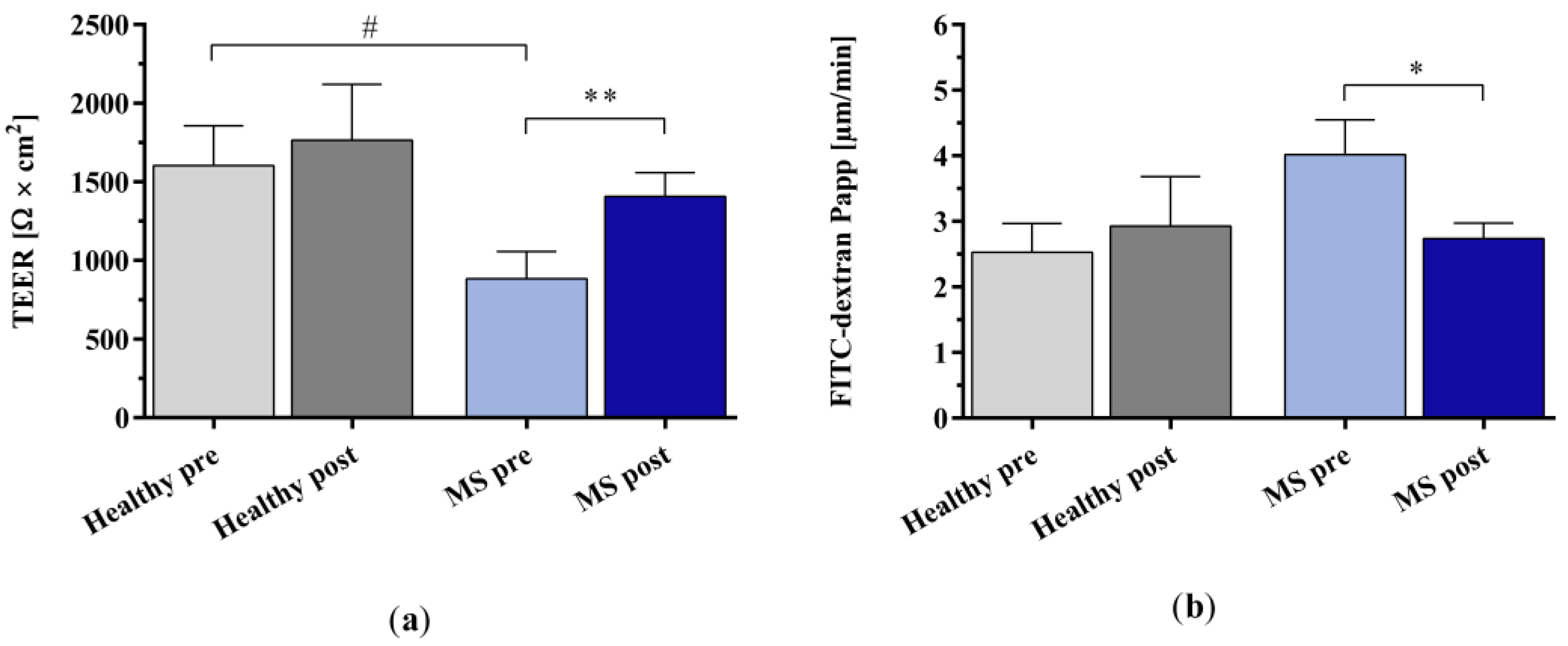
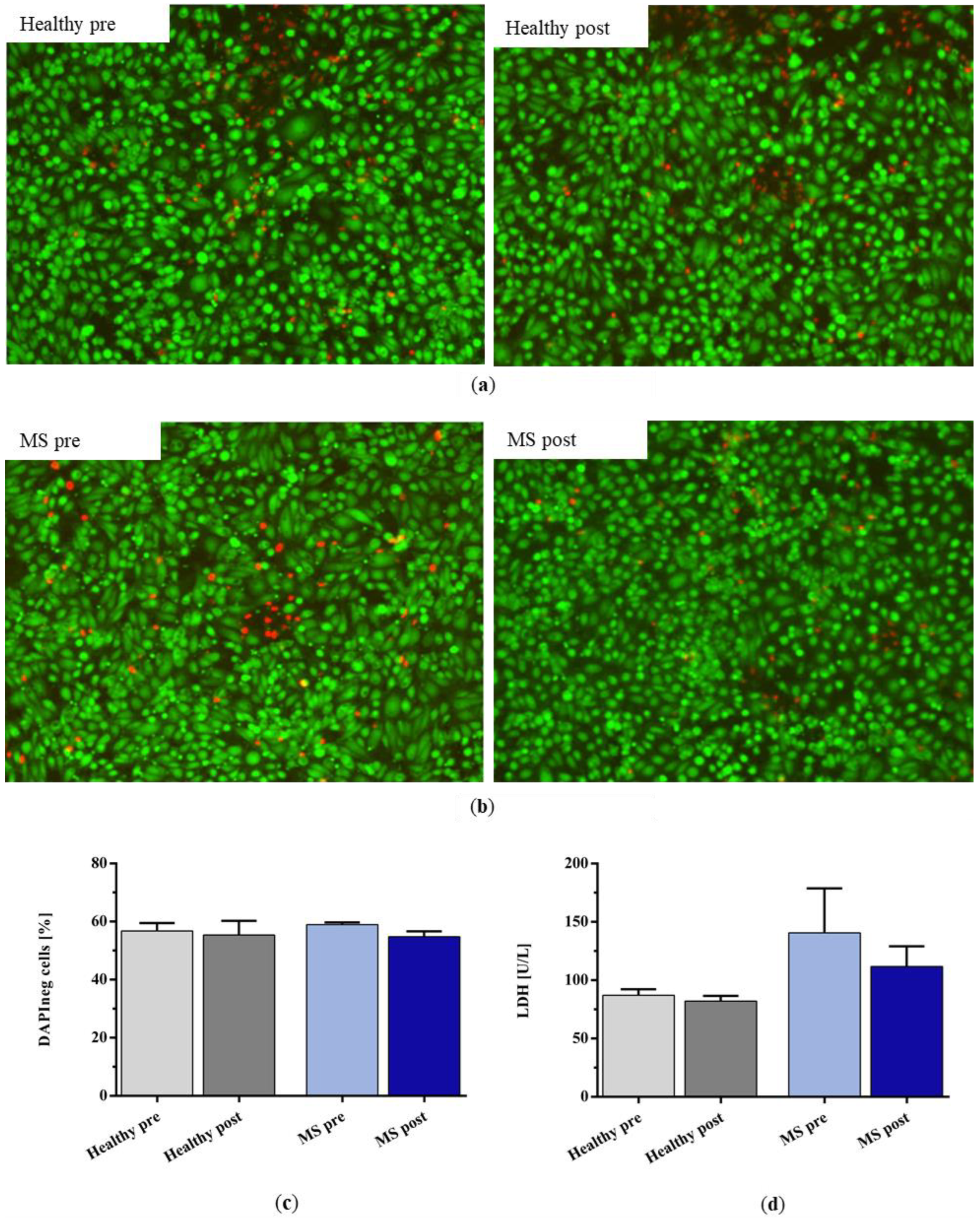
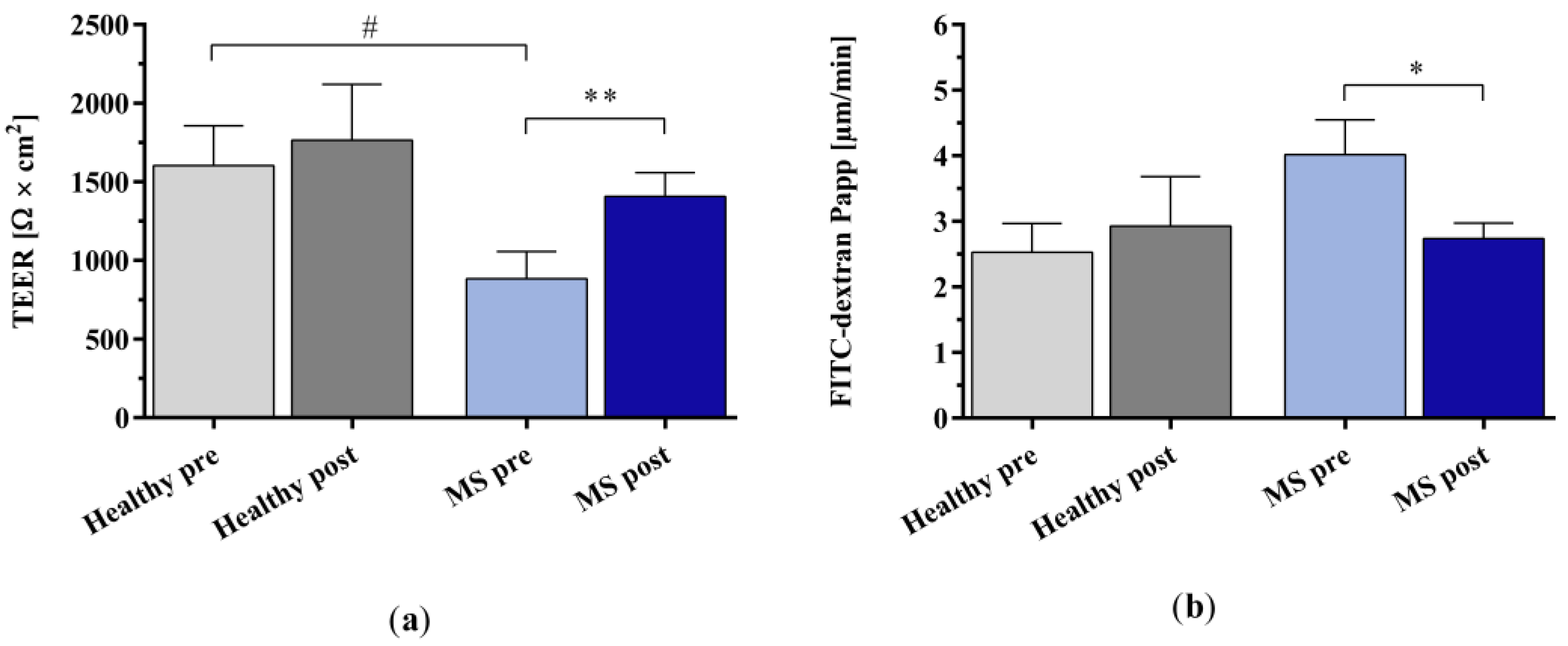
2.3. Effect of In Vitro IA Treatment on Endothelial Cell Barrier Integrity
3. Discussion
4. Materials and Methods
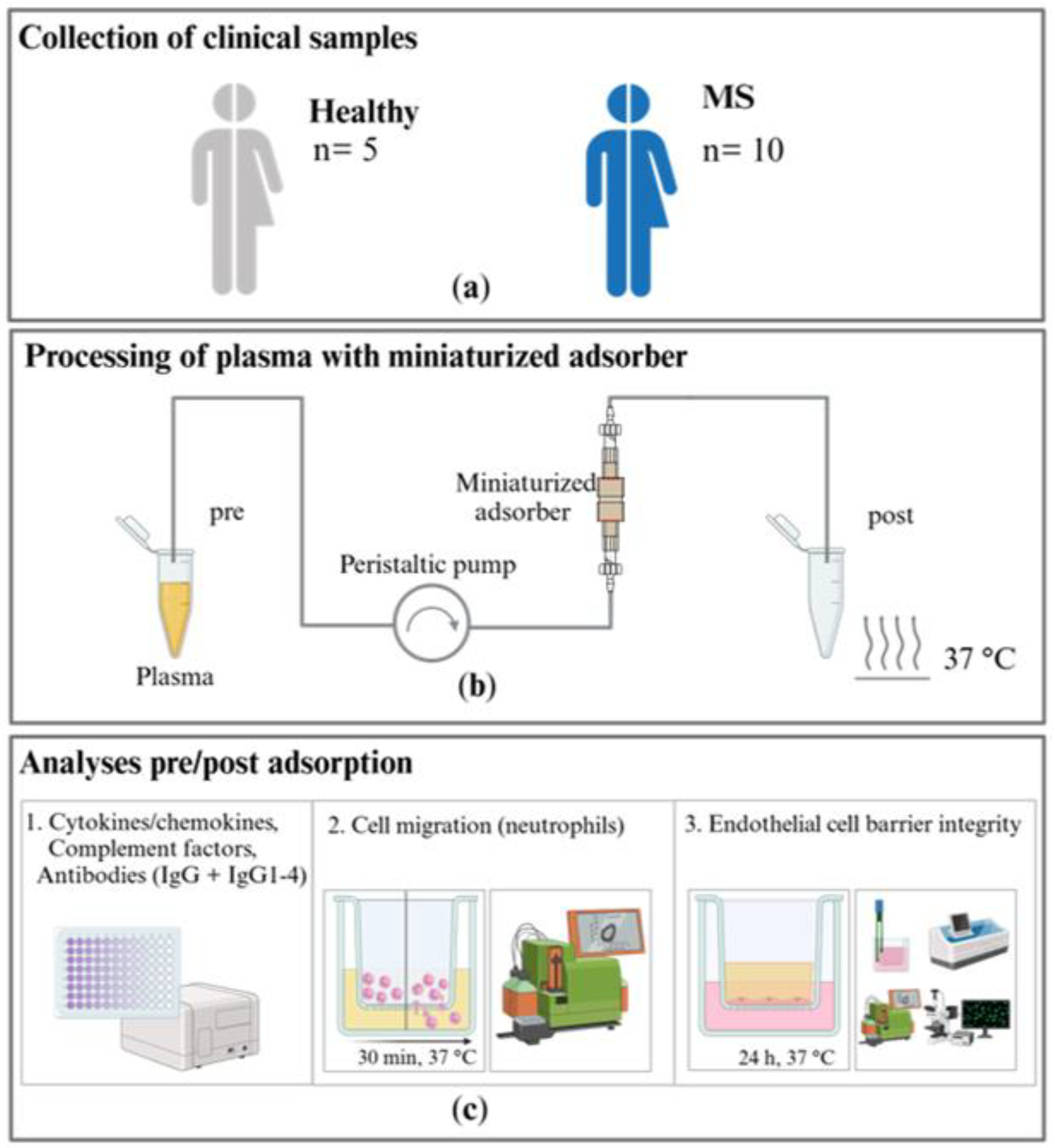
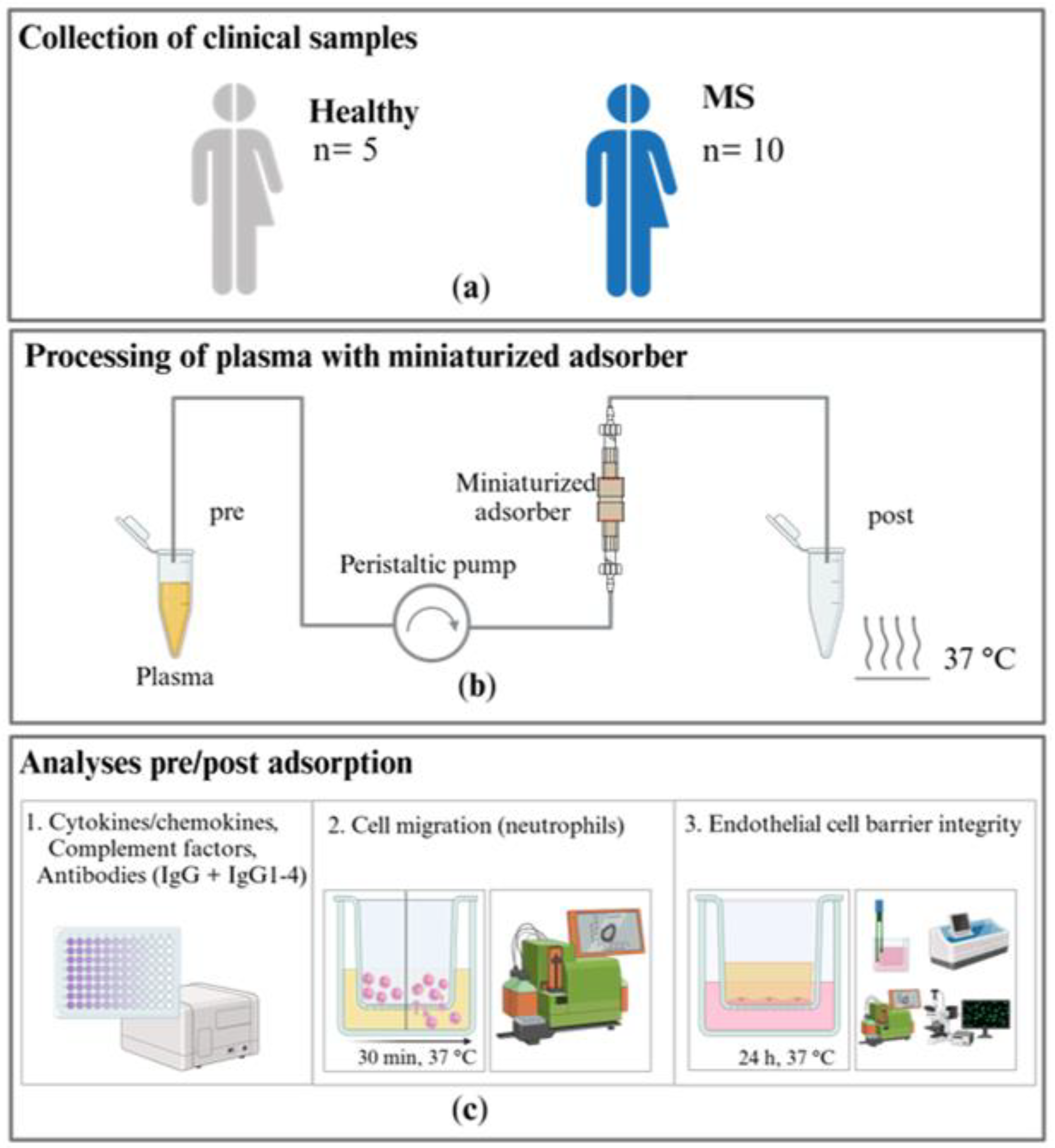
4.1. Collection of Plasma Samples from Patients with Multiple Sclerosis and Healthy Controls
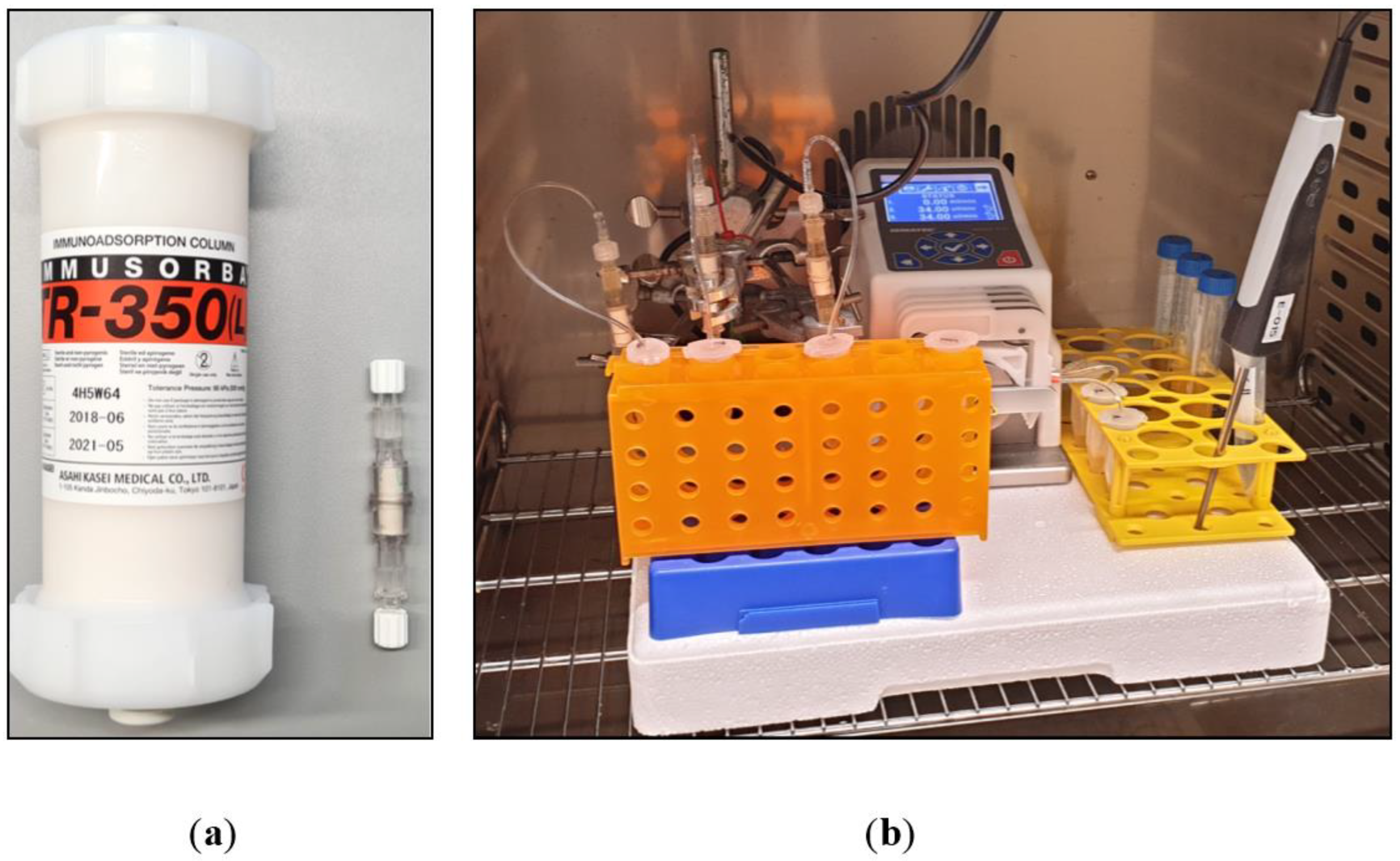
4.2. Processing of Plasma in the Miniaturized Immunoadsorption Model
4.3. Cytokine and Chemokine Analyses
4.4. Complement Factor Analyses
4.5. Antibody Analyses
4.6. Investigation of Neutrophil Migration
4.7. Investigation of Neutrophil Phagocytosis
4.8. Endothelial Cell Barrier Integrity Analyses
4.8.1. Cell Barrier Model
4.8.2. Transepithelial Electrical Resistance
4.8.3. Paracellular Permeability Assay
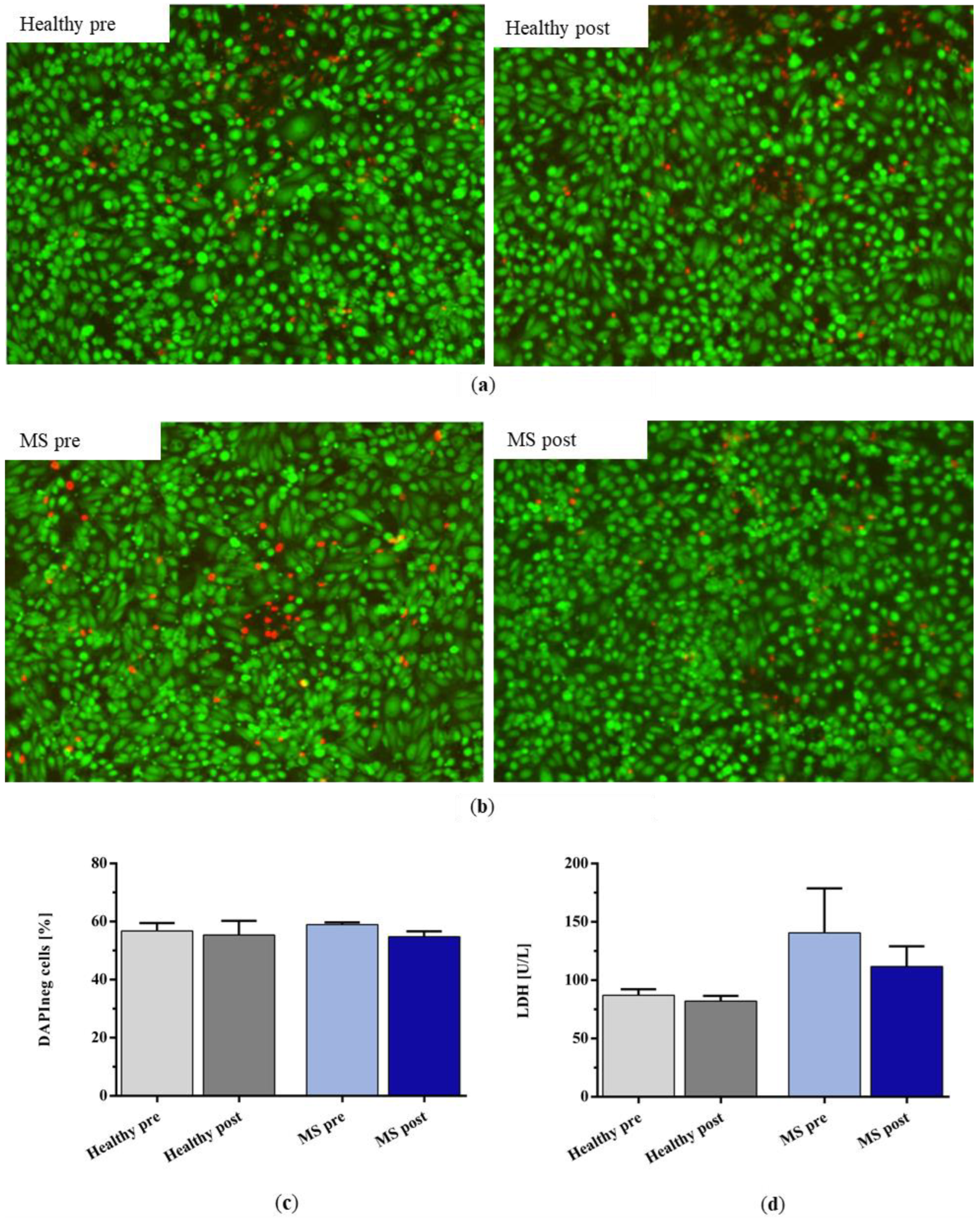
4.9. Endothelial Cell Viability Assessment
4.9.1. Live–Dead Staining
4.9.2. Lactate Dehydrogenase in Cell Culture Supernatant
4.9.3. Cell Viability
4.10. Statistics
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix B

References
- Faissner, S.; Plemel, J.R.; Gold, R.; Yong, V.W. Progressive multiple sclerosis: From pathophysiology to therapeutic strategies. Nat. Rev. Drug Discov. 2019, 18, 905–922. [Google Scholar] [CrossRef] [PubMed]
- Kutzelnigg, A.; Lassmann, H. Chapter 2—Pathology of multiple sclerosis and related inflammatory demyelinating diseases. In Handbook of Clinical Neurology: Multiple Sclerosis and Related Disorders; Goodin, D.S., Ed.; Elsevier: Amsterdam, The Netherlands, 2014; pp. 15–58. ISBN 0072-9752. [Google Scholar]
- Dobson, R.; Giovannoni, G. Multiple sclerosis—A review. Eur. J. Neurol. 2019, 26, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Hecker, M.; Bühring, J.; Fitzner, B.; Rommer, P.S.; Zettl, U.K. Genetic, Environmental and Lifestyle Determinants of Accelerated Telomere Attrition as Contributors to Risk and Severity of Multiple Sclerosis. Biomolecules 2021, 11, 1510. [Google Scholar] [CrossRef] [PubMed]
- Stys, P.K.; Zamponi, G.W.; van Minnen, J.; Geurts, J.J.G. Will the real multiple sclerosis please stand up? Nat. Rev. Neurosci. 2012, 13, 507–514. [Google Scholar] [CrossRef]
- Larochelle, C.; Alvarez, J.I.; Prat, A. How do immune cells overcome the blood-brain barrier in multiple sclerosis? FEBS Lett. 2011, 585, 3770–3780. [Google Scholar] [CrossRef] [PubMed]
- Schimrigk, S.; Faiss, J.; Köhler, W.; Günther, A.; Harms, L.; Kraft, A.; Ehrlich, S.; Eberl, A.; Fassbender, C.; Klingel, R.; et al. Escalation Therapy of Steroid Refractory Multiple Sclerosis Relapse with Tryptophan Immunoadsorption—Observational Multicenter Study with 147 Patients. Eur. Neurol. 2016, 75, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Koziolek, M.J.; Tampe, D.; Bähr, M.; Dihazi, H.; Jung, K.; Fitzner, D.; Klingel, R.; Müller, G.A.; Kitze, B. Immunoadsorption therapy in patients with multiple sclerosis with steroid-refractory optical neuritis. J. Neuroinflamm. 2012, 9, 80. [Google Scholar] [CrossRef]
- Lipphardt, M.; Mühlhausen, J.; Kitze, B.; Heigl, F.; Mauch, E.; Helms, H.-J.; Müller, G.A.; Koziolek, M.J. Immunoadsorption or plasma exchange in steroid-refractory multiple sclerosis and neuromyelitis optica. J. Clin. Apher. 2019, 34, 381–391. [Google Scholar] [CrossRef]
- Avenhaus, B.; Avenhaus, W.; Schneider, M.; Domschke, W.; Gaubitz, M. Development of an in vitro miniature model to simulate immunoadsorption in patients with systemic lupus erythematosus. J. Clin. Apher. 2002, 17, 183–189. [Google Scholar] [CrossRef]
- Harvey, G.K.; Schindhelm, K.; Pollard, J.D. IgG immunoadsorption in experimental allergic neuritis: Effect on antibody levels and clinical course. J. Neurol. Neurosurg. Psychiatry 1989, 52, 865–870. [Google Scholar] [CrossRef]
- Nilsson, R.; Lindgren, L.; Lilliehorn, P. Extracorporeal immunoadsorption therapy on rats. In vivo depletion of specific antibodies. Clin. Exp. Immunol. 1990, 82, 440–444. [Google Scholar] [CrossRef]
- Bai, Z.; Chen, D.; Wang, L.; Zhao, Y.; Liu, T.; Yu, Y.; Yan, T.; Cheng, Y. Cerebrospinal Fluid and Blood Cytokines as Biomarkers for Multiple Sclerosis: A Systematic Review and Meta-Analysis of 226 Studies with 13,526 Multiple Sclerosis Patients. Front. Neurosci. 2019, 13, 1026. [Google Scholar] [CrossRef]
- Yang, J.; Ran, M.; Li, H.; Lin, Y.; Ma, K.; Yang, Y.; Fu, X.; Yang, S. New insight into neurological degeneration: Inflammatory cytokines and blood-brain barrier. Front. Mol. Neurosci. 2022, 15, 1013933. [Google Scholar] [CrossRef]
- Ghafouri-Fard, S.; Honarmand, K.; Taheri, M. A comprehensive review on the role of chemokines in the pathogenesis of multiple sclerosis. Metab. Brain Dis. 2021, 36, 375–406. [Google Scholar] [CrossRef]
- Sun, L.; He, C.; Nair, L.; Yeung, J.; Egwuagu, C.E. Interleukin 12 (IL-12) family cytokines: Role in immune pathogenesis and treatment of CNS autoimmune disease. Cytokine 2015, 75, 249–255. [Google Scholar] [CrossRef]
- Waldmann, T.A. Interleukin-15 in the treatment of cancer. Expert Rev. Clin. Immunol. 2014, 10, 1689–1701. [Google Scholar] [CrossRef]
- Schneider, R.; Mohebiany, A.N.; Ifergan, I.; Beauseigle, D.; Duquette, P.; Prat, A.; Arbour, N. B cell-derived IL-15 enhances CD8 T cell cytotoxicity and is increased in multiple sclerosis patients. J. Immunol. 2011, 187, 4119–4128. [Google Scholar] [CrossRef]
- Saikali, P.; Antel, J.P.; Pittet, C.L.; Newcombe, J.; Arbour, N. Contribution of astrocyte-derived IL-15 to CD8 T cell effector functions in multiple sclerosis. J. Immunol. 2010, 185, 5693–5703. [Google Scholar] [CrossRef]
- Zhang, C.; Zhang, J.; Niu, J.; Zhang, J.; Tian, Z. Interleukin-15 improves cytotoxicity of natural killer cells via up-regulating NKG2D and cytotoxic effector molecule expression as well as STAT1 and ERK1/2 phosphorylation. Cytokine 2008, 42, 128–136. [Google Scholar] [CrossRef]
- Wilkinson, P.C.; Liew, F.Y. Chemoattraction of human blood T lymphocytes by interleukin-15. J. Exp. Med. 1995, 181, 1255–1259. [Google Scholar] [CrossRef]
- Li, R.; Rezk, A.; Healy, L.M.; Muirhead, G.; Prat, A.; Gommerman, J.L.; Bar-Or, A. Cytokine-Defined B Cell Responses as Therapeutic Targets in Multiple Sclerosis. Front. Immunol. 2015, 6, 626. [Google Scholar] [CrossRef]
- Janssens, R.; Struyf, S.; Proost, P. Pathological roles of the homeostatic chemokine CXCL12. Cytokine Growth Factor Rev. 2018, 44, 51–68. [Google Scholar] [CrossRef]
- Janssens, R.; Struyf, S.; Proost, P. The unique structural and functional features of CXCL12. Cell. Mol. Immunol. 2018, 15, 299–311. [Google Scholar] [CrossRef]
- Gouwy, M.; Struyf, S.; Catusse, J.; Proost, P.; van Damme, J. Synergy between proinflammatory ligands of G protein-coupled receptors in neutrophil activation and migration. J. Leukoc. Biol. 2004, 76, 185–194. [Google Scholar] [CrossRef]
- Struyf, S.; Gouwy, M.; Dillen, C.; Proost, P.; Opdenakker, G.; van Damme, J. Chemokines synergize in the recruitment of circulating neutrophils into inflamed tissue. Eur. J. Immunol. 2005, 35, 1583–1591. [Google Scholar] [CrossRef]
- Mai, C.-L.; Tan, Z.; Xu, Y.-N.; Zhang, J.-J.; Huang, Z.-H.; Wang, D.; Zhang, H.; Gui, W.-S.; Zhang, J.; Lin, Z.-J.; et al. CXCL12-mediated monocyte transmigration into brain perivascular space leads to neuroinflammation and memory deficit in neuropathic pain. Theranostics 2021, 11, 1059–1078. [Google Scholar] [CrossRef]
- Boedecker, S.C.; Luessi, F.; Engel, S.; Kraus, D.; Klimpke, P.; Holtz, S.; Meinek, M.; Marczynski, P.; Weinmann, A.; Weinmann-Menke, J. Immunoadsorption and plasma exchange-Efficient treatment options for neurological autoimmune diseases. J. Clin. Apher. 2022, 37, 70–81. [Google Scholar] [CrossRef]
- Pfeuffer, S.; Rolfes, L.; Wirth, T.; Steffen, F.; Pawlitzki, M.; Schulte-Mecklenbeck, A.; Gross, C.C.; Brand, M.; Bittner, S.; Ruck, T.; et al. Immunoadsorption versus double-dose methylprednisolone in refractory multiple sclerosis relapses. J. Neuroinflamm. 2022, 19, 220. [Google Scholar] [CrossRef]
- Ohkubo, A.; Okado, T.; Miyamoto, S.; Goto, K.; Yamamoto, M.; Maeda, T.; Itagaki, A.; Seshima, H.; Kurashima, N.; Sohara, E.; et al. Removal Characteristics of Immunoadsorption With the Immusorba TR-350 Column Using Conventional and Selective Plasma Separators. Ther. Apher. Dial. 2016, 20, 360–367. [Google Scholar] [CrossRef]
- Ohkubo, A.; Okado, T.; Sakurasawa, T.; Maeda, T.; Itagaki, A.; Yamamoto, H.; Miyamoto, S.; Seshima, H.; Kurashima, N.; Mori, T.; et al. Removal Characteristics of Immunoadsorption with the Tryptophan-Immobilized Column Using Conventional and Selective Plasma Separators in the Treatment of Myasthenia Gravis. Ther. Apher. Dial. 2019, 23, 271–278. [Google Scholar] [CrossRef]
- Oji, S.; Nomura, K. Immunoadsorption in neurological disorders. Transfus. Apher. Sci. 2017, 56, 671–676. [Google Scholar] [CrossRef]
- Snyder, H.W.; Balint, J.P.; Jones, F.R. Modulation of immunity in patients with autoimmune disease and cancer treated by extracorporeal immunoadsorption with PROSORBA columns. Semin. Hematol. 1989, 26, 31–41. [Google Scholar]
- Palm, M.; Behm, E.; Schmitt, E.; Buddenhagen, F.; Hitzschke, B.; Kracht, M.; Kundt, G.; Meyer-Rienecker, H.; Klinkmann, H. Immunoadsorption and plasma exchange in multiple sclerosis: Complement and plasma protein behaviour. Biomater. Artif. Cells Immobil. Biotechnol. 1991, 19, 283–296. [Google Scholar] [CrossRef]
- Grob, D.; Simpson, D.; Mitsumoto, H.; Hoch, B.; Mokhtarian, F.; Bender, A.; Greenberg, M.; Koo, A.; Nakayama, S. Treatment of myasthenia gravis by immunoadsorption of plasma. Neurology 1995, 45, 338–344. [Google Scholar] [CrossRef]
- Ota, K.; Ikusaka, M.; Shimizu, Y.; Akiyama, N.; Iwata, M. Increase in Peripheral Blood Leukocytes and Chemokines During Immunoadsorbent Therapy. Jpn. J. Apher. 1997, 16, 309–310. [Google Scholar]
- Fadul, J.E.M.; Alarabi, A.A.; Wikström, B.; Danielson, B.G.; Nilsson, B. Identification of complement activators and elucidation of the fate of complement activation products during extracorporeal plasma purification therapy. J. Clin. Apher. 1998, 13, 167–173. [Google Scholar] [CrossRef]
- Kadar, J.G.; Parusel, M.; Spaeth, P.J. Immunological effects of therapeutic immunoadsorption with respect to biocompatibility. Transfus. Sci. 1998, 19 (Suppl. 1), 9–23. [Google Scholar] [CrossRef]
- Shiga, Y.; Fujihara, K.; Onodera, H.; Nagata, T.; Itoyama, Y. Complement activation as a cause of transient hypotension during plasmapheresis. Artif. Organs 1998, 22, 1067–1069. [Google Scholar] [CrossRef]
- Pták, J.; Lochman, J. Immunoadsorption therapy and complement activation. Transfus. Apher. Sci. 2005, 32, 263–267. [Google Scholar] [CrossRef]
- Ingram, G.; Hakobyan, S.; Hirst, C.L.; Harris, C.L.; Loveless, S.; Mitchell, J.P.; Pickersgill, T.P.; Robertson, N.P.; Morgan, B.P. Systemic complement profiling in multiple sclerosis as a biomarker of disease state. Mult. Scler. 2012, 18, 1401–1411. [Google Scholar] [CrossRef]
- Schneidewind, J.M.; Haase, C.G.; Zettl, U.K.; Ramlow, W.; Tiess, M.; Hertel, U.; Matic, G.B.; Hebestreit, G.; Michelsen, A.; Prophet, H.; et al. Is complement activation combined with antibody removal the mystery of successful immunoadsorption in multiple sclerosis? Transfus. Apher. Sci. 2001, 24, 191–192. [Google Scholar] [CrossRef]
- Balasa, R.; Barcutean, L.; Mosora, O.; Manu, D. Reviewing the Significance of Blood-Brain Barrier Disruption in Multiple Sclerosis Pathology and Treatment. Int. J. Mol. Sci. 2021, 22, 8370. [Google Scholar] [CrossRef]
- Appelt-Menzel, A.; Cubukova, A.; Günther, K.; Edenhofer, F.; Piontek, J.; Krause, G.; Stüber, T.; Walles, H.; Neuhaus, W.; Metzger, M. Establishment of a Human Blood-Brain Barrier Co-culture Model Mimicking the Neurovascular Unit Using Induced Pluri- and Multipotent Stem Cells. Stem Cell Rep. 2017, 8, 894–906. [Google Scholar] [CrossRef]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and Treatment of Multiple Sclerosis: A Review. JAMA 2021, 325, 765–779. [Google Scholar] [CrossRef]
- Rodríguez Murúa, S.; Farez, M.F.; Quintana, F.J. The Immune Response in Multiple Sclerosis. Annu. Rev. Pathol. 2022, 17, 121–139. [Google Scholar] [CrossRef]
- Nguyen, K.; Juillard, P.; Hawke, S.; Grau, G.E.; Marsh-Wakefield, F. Trans-Endothelial Migration of Memory T Cells Is Impaired in Alemtuzumab-Treated Multiple Sclerosis Patients. J. Clin. Med. 2022, 11, 6266. [Google Scholar] [CrossRef]
- Hawke, S.; Zinger, A.; Juillard, P.-G.; Holdaway, K.; Byrne, S.N.; Grau, G.E. Selective modulation of trans-endothelial migration of lymphocyte subsets in multiple sclerosis patients under fingolimod treatment. J. Neuroimmunol. 2020, 349, 577392. [Google Scholar] [CrossRef]
- Lou, J.; Gasche, Y.; Zheng, L.; Giroud, C.; Morel, P.; Clements, J.; Ythier, A.; Grau, G.E. Interferon-beta inhibits activated leukocyte migration through human brain microvascular endothelial cell monolayer. Lab. Investig. J. Tech. Methods Pathol. 1999, 79, 1015–1025. [Google Scholar]
- Floris, S.; Ruuls, S.R.; Wierinckx, A.; van der Pol, S.M.A.; Döpp, E.; van der Meide, P.H.; Dijkstra, C.D.; De Vries, H.E. Interferon-beta directly influences monocyte infiltration into the central nervous system. J. Neuroimmunol. 2002, 127, 69–79. [Google Scholar] [CrossRef]
- Prat, A.; Biernacki, K.; Antel, J.P. Th1 and Th2 lymphocyte migration across the human BBB is specifically regulated by interferon beta and copolymer-1. J. Autoimmun. 2005, 24, 119–124. [Google Scholar] [CrossRef]
- Jimenez, J.; Jy, W.; Mauro, L.M.; Horstman, L.L.; Ahn, E.R.; Ahn, Y.S.; Minagar, A. Elevated endothelial microparticle-monocyte complexes induced by multiple sclerosis plasma and the inhibitory effects of interferon-beta 1b on release of endothelial microparticles, formation and transendothelial migration of monocyte-endothelial microparticle complexes. Mult. Scler. 2005, 11, 310–315. [Google Scholar] [CrossRef]
- Weber, M.S.; Starck, M.; Wagenpfeil, S.; Meinl, E.; Hohlfeld, R.; Farina, C. Multiple sclerosis: Glatiramer acetate inhibits monocyte reactivity in vitro and in vivo. Brain 2004, 127, 1370–1378. [Google Scholar] [CrossRef]
- Zhao, Y.; Chen, C.; Xiao, X.; Fang, L.; Cheng, X.; Chang, Y.; Peng, F.; Wang, J.; Shen, S.; Wu, S.; et al. Teriflunomide Promotes Blood-Brain Barrier Integrity by Upregulating Claudin-1 via the Wnt/β-catenin Signaling Pathway in Multiple Sclerosis. Mol. Neurobiol. 2023, 1–17. [Google Scholar] [CrossRef]
- Aubé, B.; Lévesque, S.A.; Paré, A.; Chamma, É.; Kébir, H.; Gorina, R.; Lécuyer, M.-A.; Alvarez, J.I.; De Koninck, Y.; Engelhardt, B.; et al. Neutrophils mediate blood-spinal cord barrier disruption in demyelinating neuroinflammatory diseases. J. Immunol. 2014, 193, 2438–2454. [Google Scholar] [CrossRef]
- Santos-Lima, B.; Pietronigro, E.C.; Terrabuio, E.; Zenaro, E.; Constantin, G. The role of neutrophils in the dysfunction of central nervous system barriers. Front. Aging Neurosci. 2022, 14, 965169. [Google Scholar] [CrossRef]
- Baggi, F.; Ubiali, F.; Nava, S.; Nessi, V.; Andreetta, F.; Rigamonti, A.; Maggi, L.; Mantegazza, R.; Antozzi, C. Effect of IgG immunoadsorption on serum cytokines in MG and LEMS patients. J. Neuroimmunol. 2008, 201–202, 104–110. [Google Scholar] [CrossRef]
- Lippmann, E.S.; Al-Ahmad, A.; Azarin, S.M.; Palecek, S.P.; Shusta, E.V. A retinoic acid-enhanced, multicellular human blood-brain barrier model derived from stem cell sources. Sci. Rep. 2014, 4, 4160. [Google Scholar] [CrossRef]
- Lorentz, K.; Klauke, R.; Schmidt, E. Recommendation for the determination of the catalytic concentration of lactate dehydrogenase at 37 degrees C. Standardization Committee of the German Society for Clinical Chemistry, Enzyme Working Group of the German Society for Clinical Chemistry. Eur. J. Clin. Chem. Clin. Biochem. J. Forum Eur. Clin. Chem. Soc. 1993, 31, 897–899. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy | MS | |
|---|---|---|
| n | 5 | 10 |
| female | 3 | 9 |
| mean age in years (±SD) | 32.4 (5.9) | 36.5 (12.9) |
| mean EDSS score (±SD) | n.a. | 2.3 (1.7) 1 |
| mean time from MS diagnosis in years (±SD) | n.a. | 8.8 (8.4) |
| patients on DMT | n.a. | 7 |
| patients with acute relapse | n.a. | 2 |
| median time since last relapse in months (range) | n.a. | 36 (0–190) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Körtge, A.; Breitrück, A.; Doß, S.; Hofrichter, J.; Nelz, S.-C.; Krüsemann, H.; Wasserkort, R.; Fitzner, B.; Hecker, M.; Mitzner, S.; et al. The Utility of Miniaturized Adsorbers in Exploring the Cellular and Molecular Effects of Blood Purification: A Pilot Study with a Focus on Immunoadsorption in Multiple Sclerosis. Int. J. Mol. Sci. 2024, 25, 2590. https://doi.org/10.3390/ijms25052590
Körtge A, Breitrück A, Doß S, Hofrichter J, Nelz S-C, Krüsemann H, Wasserkort R, Fitzner B, Hecker M, Mitzner S, et al. The Utility of Miniaturized Adsorbers in Exploring the Cellular and Molecular Effects of Blood Purification: A Pilot Study with a Focus on Immunoadsorption in Multiple Sclerosis. International Journal of Molecular Sciences. 2024; 25(5):2590. https://doi.org/10.3390/ijms25052590
Chicago/Turabian StyleKörtge, Andreas, Anne Breitrück, Sandra Doß, Jacqueline Hofrichter, Sophie-Charlotte Nelz, Horst Krüsemann, Reinhold Wasserkort, Brit Fitzner, Michael Hecker, Steffen Mitzner, and et al. 2024. "The Utility of Miniaturized Adsorbers in Exploring the Cellular and Molecular Effects of Blood Purification: A Pilot Study with a Focus on Immunoadsorption in Multiple Sclerosis" International Journal of Molecular Sciences 25, no. 5: 2590. https://doi.org/10.3390/ijms25052590
APA StyleKörtge, A., Breitrück, A., Doß, S., Hofrichter, J., Nelz, S.-C., Krüsemann, H., Wasserkort, R., Fitzner, B., Hecker, M., Mitzner, S., & Zettl, U. K. (2024). The Utility of Miniaturized Adsorbers in Exploring the Cellular and Molecular Effects of Blood Purification: A Pilot Study with a Focus on Immunoadsorption in Multiple Sclerosis. International Journal of Molecular Sciences, 25(5), 2590. https://doi.org/10.3390/ijms25052590