
Intrastent Restenosis: A Comprehensive Review

 , and
, and
Abstract
1. Introduction
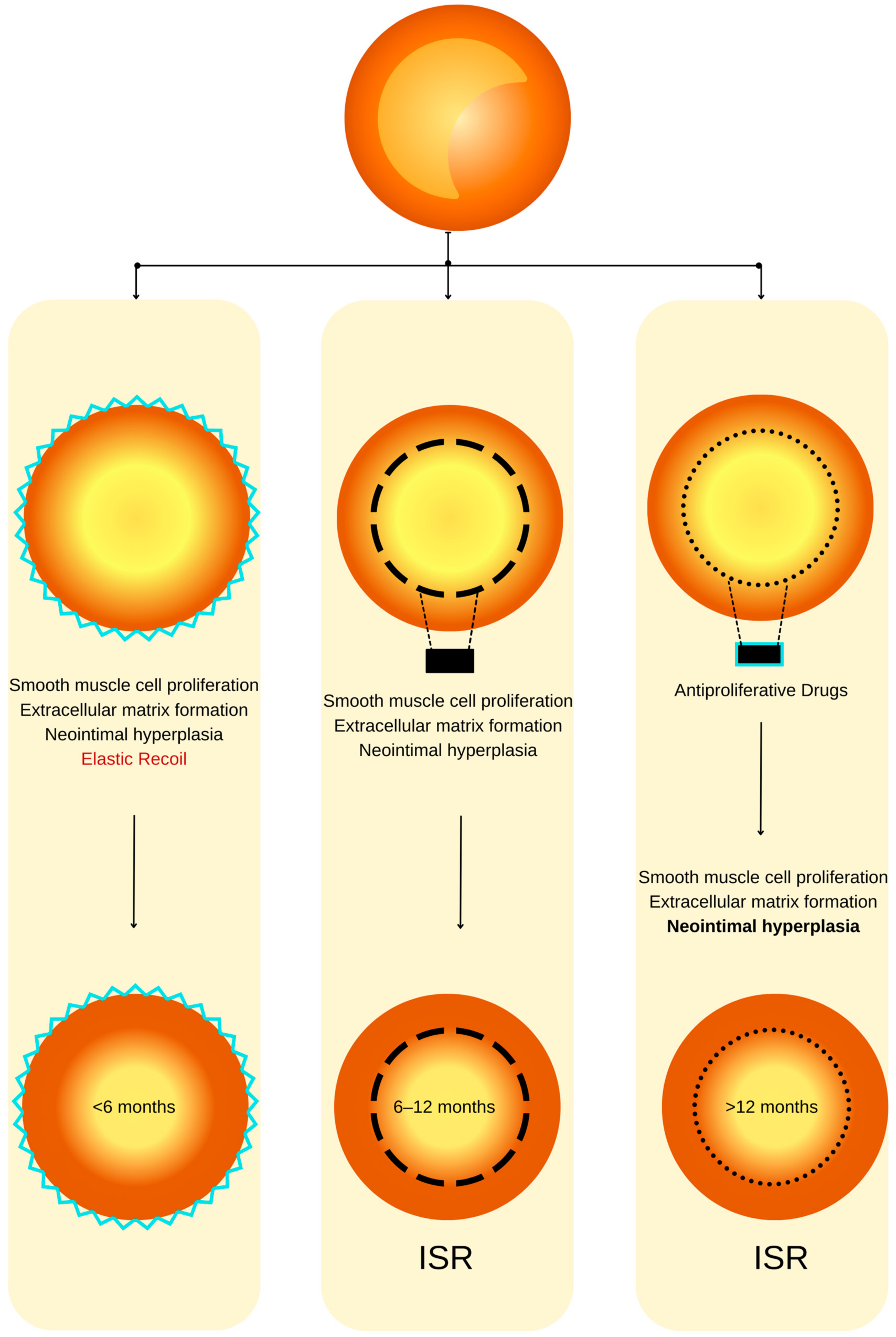
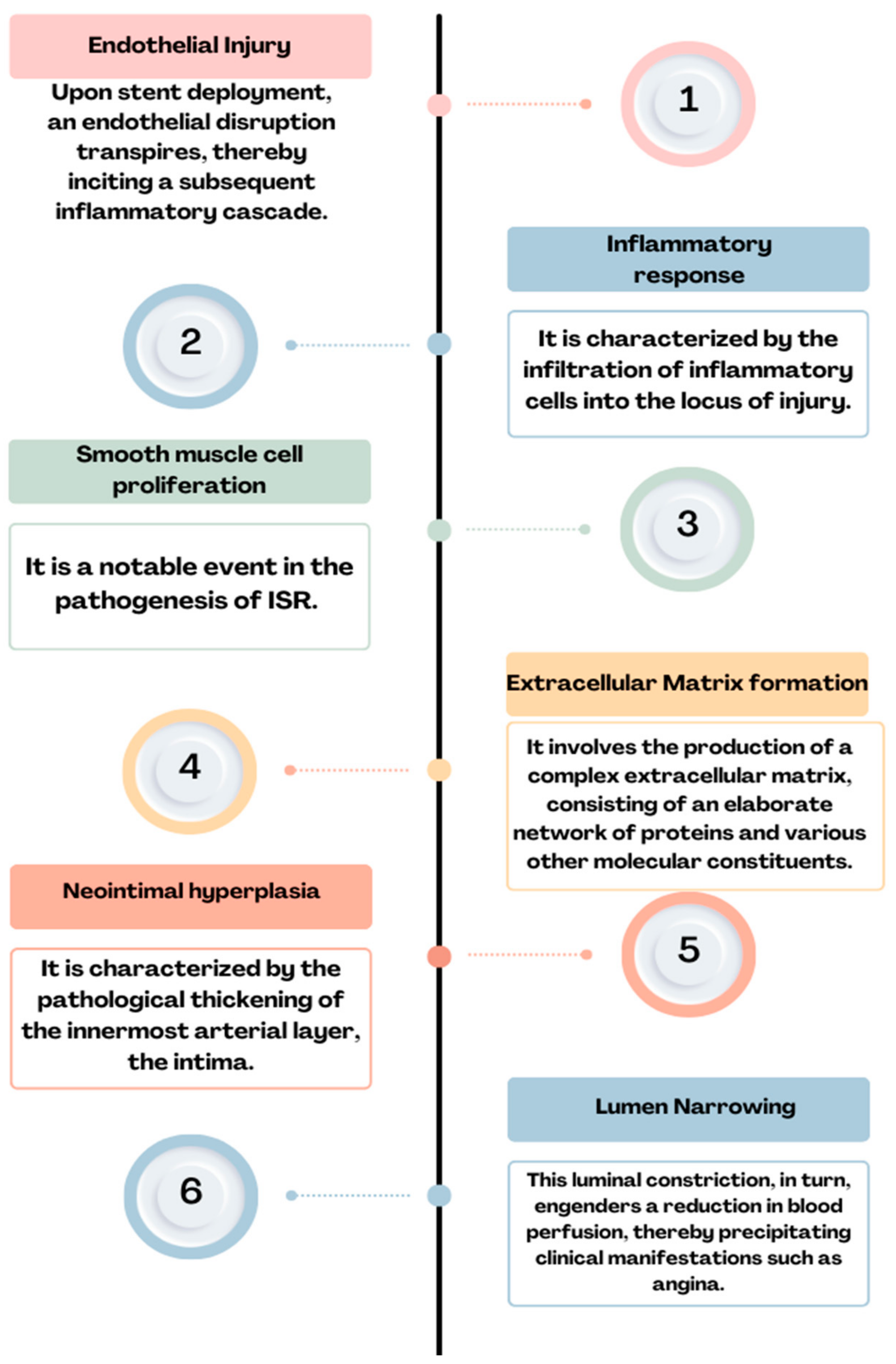
2. ISR—Definition, Incidence, and Pathophysiology
3. Risk Factors for ISR
3.1. Patient-Related Factors
3.2. Clinical Factors
3.3. Angiographic Factors
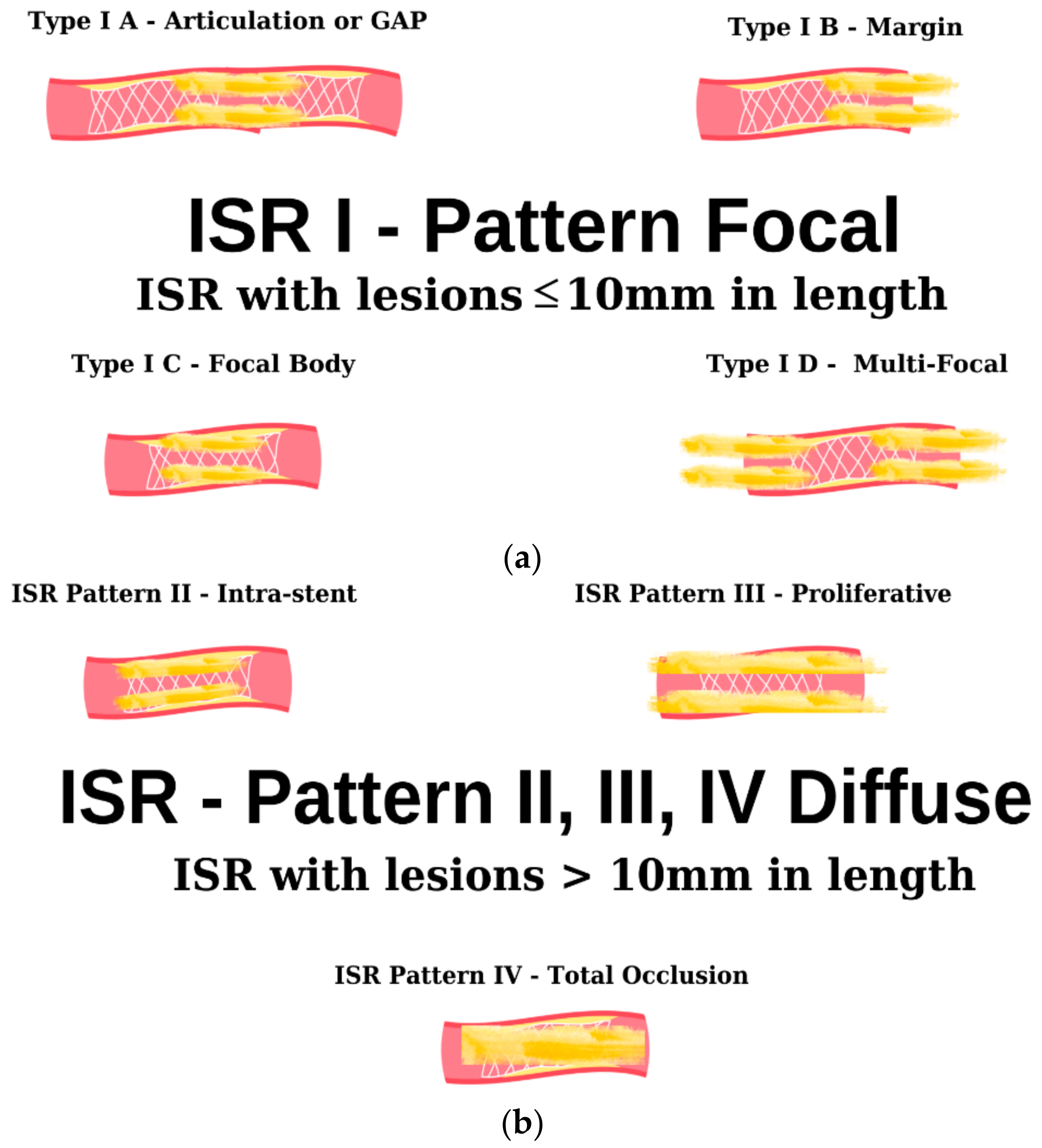
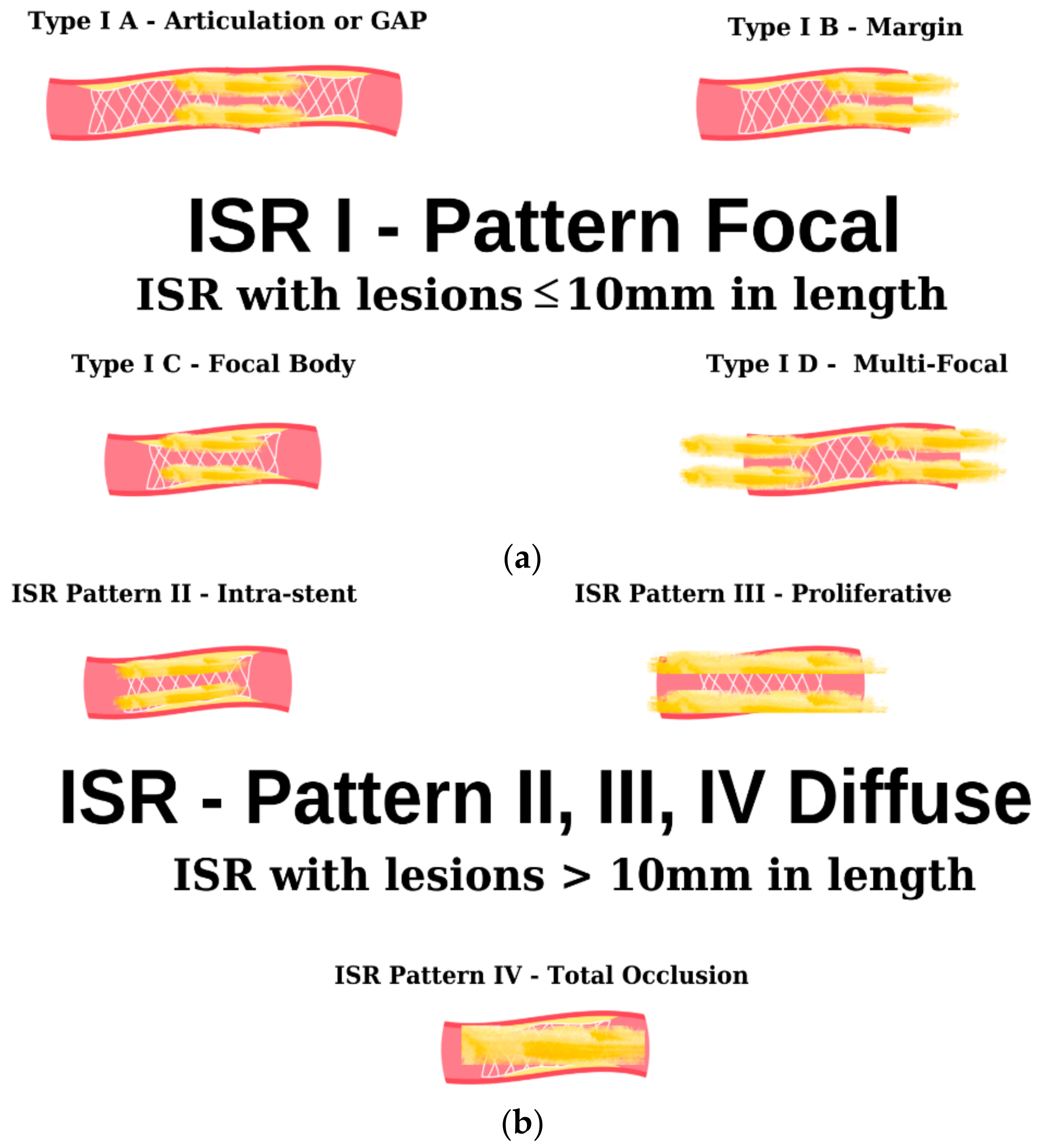
4. Clinical Presentation and Diagnosis
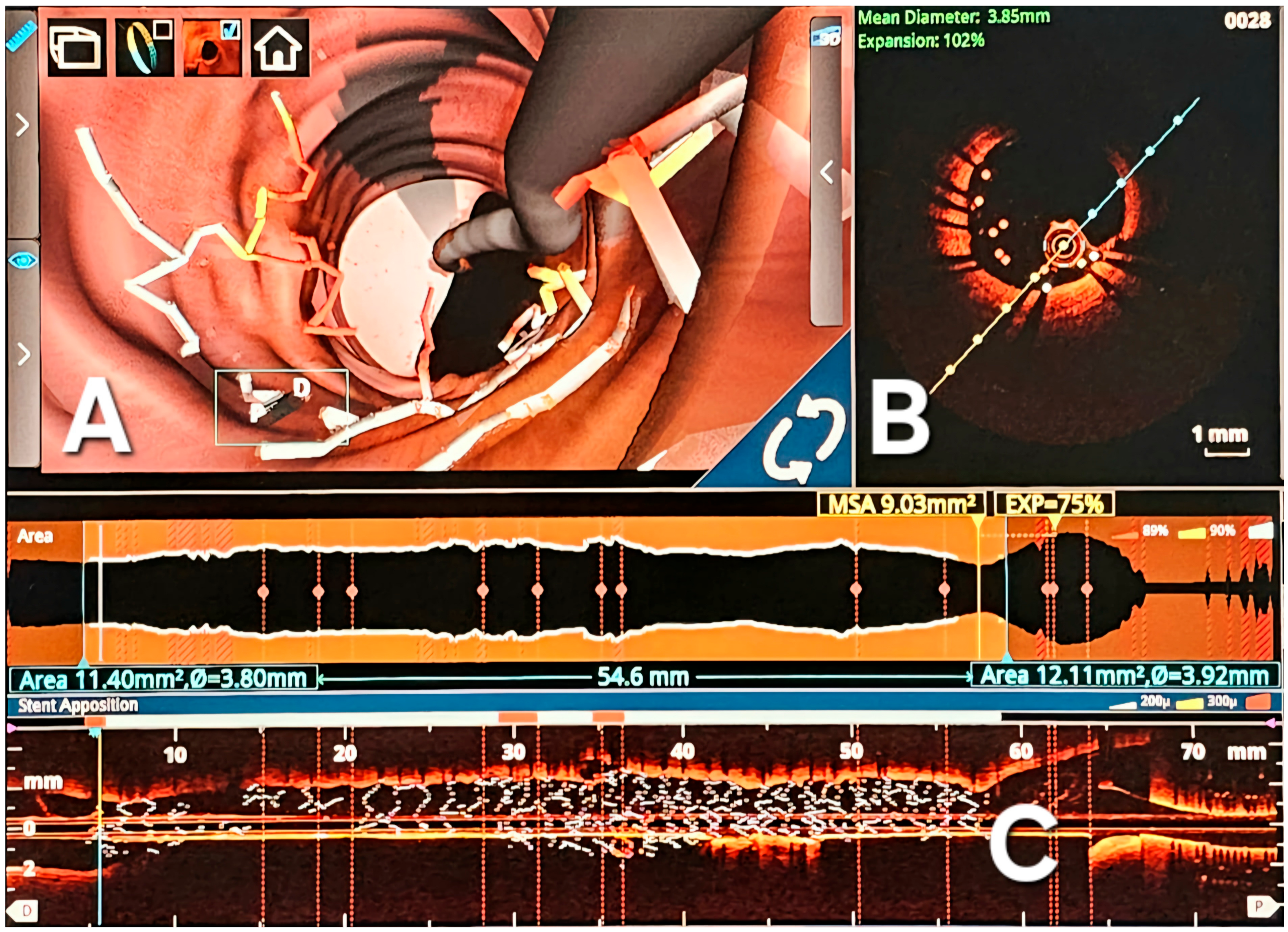
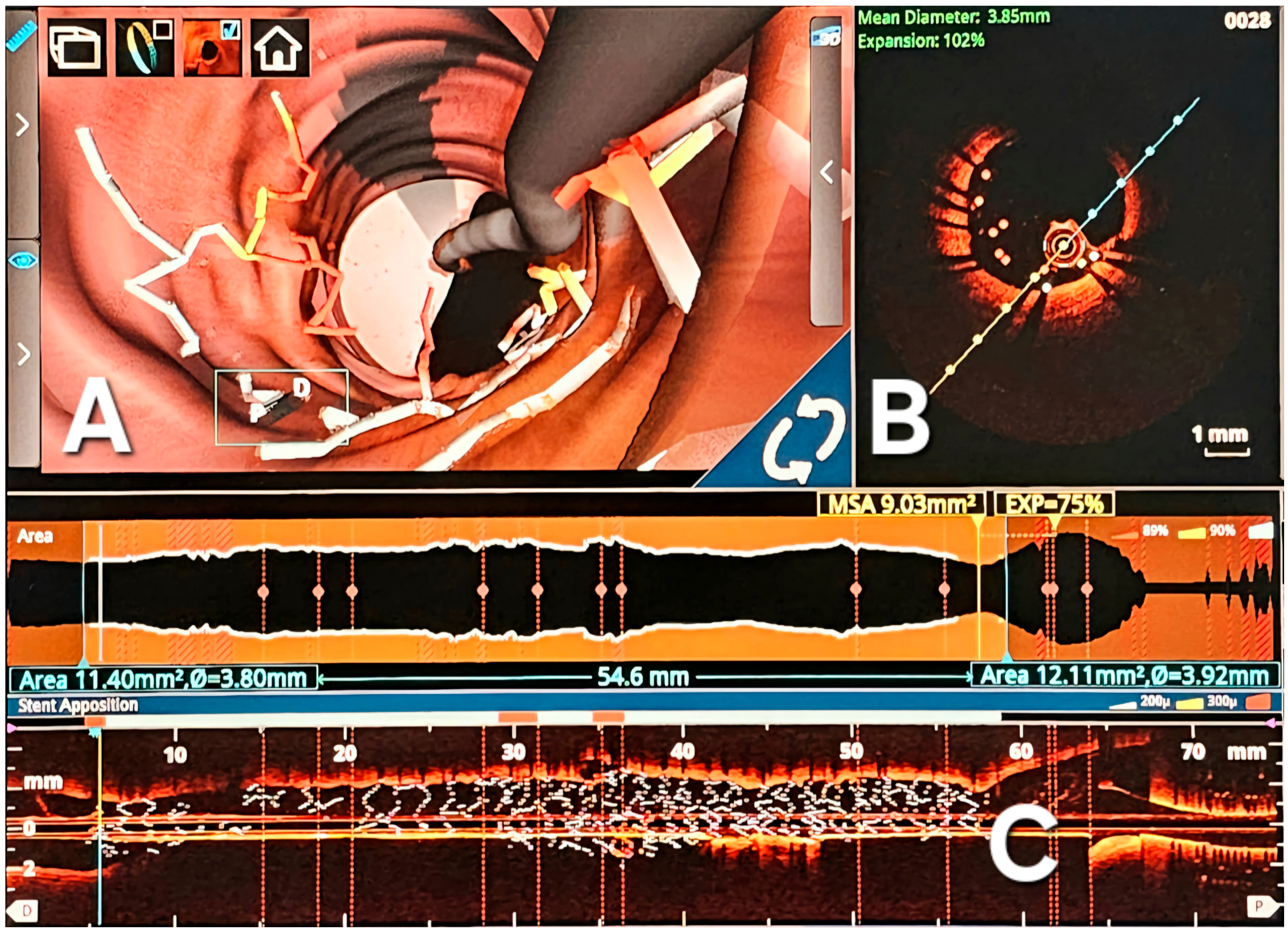
Intravascular Imaging
5. Clinical Outcomes of ISR
6. Treatment
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wassif, H.; Welt, F.G.P. Restenosis of Stented Coronary Arteries; SCAI Interventional Cardiology Board Review: Second Edition; StatPearls: Treasure Island, FL, USA, 2023; pp. 10–15. [Google Scholar]
- Alraies, M.C.; Darmoch, F.; Tummala, R.; Waksman, R. Diagnosis and management challenges of in-stent restenosis in coronary arteries. World J. Cardiol. 2017, 9, 640. [Google Scholar] [CrossRef] [PubMed]
- Elbadawi, A.; Dang, A.T.; Mahana, I.; Elzeneini, M.; Alonso, F.; Banerjee, S.; Kumbhani, D.J.; Elgendy, I.Y.; Mintz, G.S. Outcomes of Percutaneous Coronary Intervention for In-Stent Restenosis Versus De Novo Lesions: A Meta-Analysis. J. Am. Heart Assoc. 2023, 12, 29300. [Google Scholar] [CrossRef] [PubMed]
- Moussa, I.D.; Mohananey, D.; Saucedo, J.; Stone, G.W.; Yeh, R.W.; Kennedy, K.F.; Waksman, R.; Teirstein, P.; Moses, J.W.; Simonton, C. Trends and Outcomes of Restenosis after Coronary Stent Implantation in the United States. J. Am. Coll. Cardiol. 2020, 76, 1521–1531. [Google Scholar] [CrossRef]
- Alexandrescu, D.-M.; Mitu, O.; Costache, I.I.; Macovei, L.; Mitu, I.; Alexandrescu, A.; Arsenescu Georgescu, C. Risk factors associated with intra-stent restenosis after percutaneous coronary intervention. Exp. Ther. Med. 2021, 22, 1141. [Google Scholar] [CrossRef]
- Alfonso, F.; Jose Pérez-Vizcayno, M.; Cárdenas, A.; García del Blanco, B.; Seidelberger, B.; Iñiguez, A.; Gómez-Recio, M.; Masotti, M.; Teresa Velázquez, M.; Sanchís, J.; et al. A Randomized Comparison of Drug-Eluting Balloon Versus Everolimus-Eluting Stent in Patients with Bare-Metal Stent-In-Stent Restenosis The RIBS V Clinical Trial (Restenosis Intra-stent of Bare Metal Stents: Paclitaxel-eluting Balloon vs. Everolimus-eluting Stent). J. Am. Coll. Cardiol. 2014, 63, 1378–1386. [Google Scholar]
- Ullrich, H.; Olschewski, M.; Münzel, T.; Gori, T. Coronary In-Stent Restenosis: Predictors and Treatment. Dtsch. Arztebl. Int. 2021, 118, 637. [Google Scholar] [CrossRef]
- Giustino, G.; Colombo, A.; Camaj, A.; Yasumura, K.; Mehran, R.; Stone, G.W.; Kini, A.; Sharma, S.K. Coronary In-Stent Restenosis: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 80, 348–372. [Google Scholar] [CrossRef] [PubMed]
- Coronary Artery Stent Thrombosis: Clinical Presentation and Management—UpToDate. Available online: https://www.uptodate.com/contents/coronary-artery-stent-thrombosis-clinical-presentation-and-management/print (accessed on 25 November 2023).
- Buccheri, D.; Piraino, D.; Andolina, G.; Cortese, B. Understanding and managing in-stent restenosis: A review of clinical data, from pathogenesis to treatment. J. Thorac. Dis. 2016, 8, E1150. [Google Scholar] [CrossRef]
- Modi, K.; Soos, M.P.; Mahajan, K. Stent Thrombosis; StatPearls Publishing LLC: Treasure Island, FL, USA, 2023. [Google Scholar]
- Li, M.; Hou, J.; Gu, X.; Weng, R.; Zhong, Z.; Liu, S. Incidence and risk factors of in-stent restenosis after percutaneous coronary intervention in patients from southern China. Eur. J. Med. Res. 2022, 27, 12. [Google Scholar] [CrossRef]
- Fishman, R.F.; Kuntz, R.E.; Carrozza, J.P.; Miller, M.J.; Senerchia, C.C.; Schnitt, S.J.; Diver, D.J.; Safian, R.D.; Baim, D.S. Long-term results of directional coronary atherectomy: Predictors of restenosis. J. Am. Coll. Cardiol. 1992, 20, 1101–1110. [Google Scholar] [CrossRef]
- Le Feuvre, C.; Bonan, R.; Lespérance, J.; Gosselin, G.; Joyal, M.; Crépeau, J. Predictive factors of restenosis after multivessel percutaneous transluminal coronary angioplasty. Am. J. Cardiol. 1994, 73, 840–844. [Google Scholar] [CrossRef]
- Bakhai, A.; Booth, J.; Delahunty, N.; Nugara, F.; Clayton, T.; McNeill, J.; Davies, S.W.; Cumberland, D.C.; Stables, R.H.; SV Stent Investigators. The SV stent study: A prospective, multicentre, angiographic evaluation of the BiodivYsio phosphorylcholine coated small vessel stent in small coronary vessels. Int. J. Cardiol. 2005, 102, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, P.; Valgimigli, M.; Biondi-Zoccai, G.G.L.; Abbate, A.; Garcia Garcia, H.M.; Anselmi, M.; Turri, M.; McFadden, E.P.; Vassanelli, C.; Serruys, P.W.; et al. Clinical effectiveness of bare-metal stenting compared with balloon angioplasty in total coronary occlusions: Insights from a systematic overview of randomized trials in light of the drug-eluting stent era. Am. Heart J. 2006, 151, 682–689. [Google Scholar] [CrossRef]
- Stettler, C.; Wandel, S.; Allemann, S.; Kastrati, A.; Morice, M.C.; Schömig, A.; Pfisterer, M.E.; Stone, G.W.; Leon, M.B.; de Lezo, J.S.; et al. Outcomes associated with drug-eluting and bare-metal stents: A collaborative network meta-analysis. Lancet 2007, 370, 937–948. [Google Scholar] [CrossRef] [PubMed]
- Kastrati, A.; Mehilli, J.; Pache, J.; Kaiser, C.; Valgimigli, M.; Kelbæk, H.; Menichelli, M.; Sabaté, M.; Suttorp, M.J.; Baumgart, D.; et al. Analysis of 14 trials comparing sirolimus-eluting stents with bare-metal stents. N. Engl. J. Med. 2007, 356, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- García del Blanco, B.; Rumoroso Cuevas, J.R.; Hernández Hernández, F.; Trillo Nouche, R. Spanish cardiac catheterization and coronary intervention registry. 22nd official report of the Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology (1990–2012). Rev. Esp. Cardiol. (Engl. Ed.) 2013, 66, 894–904. [Google Scholar] [CrossRef]
- Moses, J.W.; Leon, M.B.; Popma, J.J.; Fitzgerald, P.J.; Holmes, D.R.; O’Shaughnessy, C.; Caputo, R.P.; Kereiakes, D.J.; Williams, D.O.; Teirstein, P.S.; et al. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N. Engl. J. Med. 2003, 349, 1315–1323. [Google Scholar] [CrossRef]
- Stone, G.W.; Ellis, S.G.; Cox, D.A.; Hermiller, J.; O’Shaughnessy, C.; Mann, J.T.; Turco, M.; Caputo, R.; Bergin, P.; Greenberg, J.; et al. A polymer-based, paclitaxel-eluting stent in patients with coronary artery disease. N. Engl. J. Med. 2004, 350, 221–231. [Google Scholar] [CrossRef]
- Zhao, L.P.; Xu, W.T.; Wang, L.; Li, H.; Shao, C.L.; Gu, H.B.; Chan, S.P.; Xu, H.F.; Yang, X.J. Influence of insulin resistance on in-stent restenosis in patients undergoing coronary drug-eluting stent implantation after long-term angiographic follow-up. Coron. Artery Dis. 2015, 26, 5–10. [Google Scholar] [CrossRef]
- Chiastra, C.; Migliavacca, F. Modeling of Blood Flow in Stented Coronary Arteries. In Heat Transfer and Fluid Flow in Biological Processes; Academic Press: Cambridge, MA, USA, 2015; pp. 335–370. [Google Scholar]
- Bertolone, D.T.; Gallinoro, E.; Esposito, G.; Paolisso, P.; Bermpeis, K.; De Colle, C.; Fabbricatore, D.; Mileva, N.; Valeriano, C.; Munhoz, D.; et al. Contemporary Management of Stable Coronary Artery Disease. High Blood Press. Cardiovasc. Prev. 2022, 29, 207. [Google Scholar] [CrossRef]
- Pham, V.; Moroni, A.; Gall, E.; Benedetti, A.; Zivelonghi, C.; Picard, F. Revascularization and Medical Therapy for Chronic Coronary Syndromes: Lessons Learnt from Recent Trials, a Literature Review. J. Clin. Med. 2023, 12, 2833. [Google Scholar] [CrossRef]
- Shlofmitz, E.; Iantorno, M.; Waksman, R. Restenosis of Drug-Eluting Stents A New Classification System Based on Disease Mechanism to Guide Treatment and State-of-the-Art Review Circulation: Cardiovascular Interventions. Circ. Cardiovasc. Interv. 2019, 12, 7023. [Google Scholar] [CrossRef]
- Lee, M.S.; Banka, G. In-stent Restenosis. Interv. Cardiol. Clin. 2016, 5, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Zain, M.A.; Jamil, R.T.; Siddiqui, W.J. Neointimal Hyperplasia; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Dangas, G.D.; Claessen, B.E.; Caixeta, A.; Sanidas, E.A.; Mintz, G.S.; Mehran, R. In-stent restenosis in the drug-eluting stent era. J. Am. Coll. Cardiol. 2010, 56, 1897–1907. [Google Scholar] [CrossRef] [PubMed]
- Nolan, D.R.; Lally, C. An investigation of damage mechanisms in mechanobiological models of in-stent restenosis. J. Comput. Sci. 2018, 24, 132–142. [Google Scholar] [CrossRef]
- He, R.; Zhao, L.; Silberschmidt, V.V.; Liu, Y. Mechanistic evaluation of long-term in-stent restenosis based on models of tissue damage and growth. Biomech. Model Mechanobiol. 2020, 19, 1425–1446. [Google Scholar] [CrossRef] [PubMed]
- Torrado, J.; Buckley, L.; Durán, A.; Trujillo, P.; Toldo, S.; Valle Raleigh, J.; Abbate, A.; Biondi-Zoccai, G.; Guzmán, L.A. Restenosis, Stent Thrombosis, and Bleeding Complications: Navigating between Scylla and Charybdis. J. Am. Coll. Cardiol. 2018, 71, 1676–1695. [Google Scholar] [CrossRef] [PubMed]
- Timmis, A.; Townsend, N.; Gale, C.; Grobbee, R.; Maniadakis, N.; Flather, M.; Wilkins, E.; Wright, L.; Vos, R.; Bax, J.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2017. Eur. Heart J. 2018, 39, 508–577. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.C.K.; Lian, S.S.; Zhong, L.; Collet, C.; Foin, N.; Ang, H.Y. Stent malapposition generates stent thrombosis: Insights from a thrombosis model. Int. J. Cardiol. 2022, 353, 43–45. [Google Scholar] [CrossRef]
- Nusca, A.; Viscusi, M.M.; Piccirillo, F.; De Filippis, A.; Nenna, A.; Spadaccio, C.; Nappi, F.; Chello, C.; Mangiacapra, F.; Grigioni, F.; et al. In Stent Neo-Atherosclerosis: Pathophysiology, Clinical Implications, Prevention, and Therapeutic Approaches. Life 2022, 12, 393. [Google Scholar] [CrossRef]
- Virmani, R.; Farb, A. Pathology of in-stent restenosis. Curr. Opin. Lipidol. 1999, 10, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Yutani, C.; Ishibashi-Ueda, H.; Suzuki, T.; Kojima, A. Histologic evidence of foreign body granulation tissue and de novo lesions in patients with coronary stent restenosis. Cardiology 1999, 92, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Clare, J.; Ganly, J.; Bursill, C.A.; Sumer, H.; Kingshott, P.; de Haan, J.B. The Mechanisms of Restenosis and Relevance to Next Generation Stent Design. Biomolecules 2022, 12, 430. [Google Scholar] [CrossRef] [PubMed]
- Marx, S.O.; Totary-Jain, H.; Marks, A.R. Vascular Smooth Muscle Cell Proliferation in Restenosis. Circ. Cardiovasc. Interv. 2011, 4, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Becker, R.C.; Sexton, T.; Smyth, S.S. Translational Implications of Platelets as Vascular First Responders. Circ. Res. 2018, 122, 506–522. [Google Scholar] [CrossRef] [PubMed]
- Hytönen, J.; Leppänen, O.; Braesen, J.H.; Schunck, W.H.; Mueller, D.; Jung, F.; Mrowietz, C.; Jastroch, M.; Von Bergwelt-Baildon, M.; Kappert , K.; et al. Activation of Peroxisome Proliferator-Activated Receptor-δ as Novel Therapeutic Strategy to Prevent In-Stent Restenosis and Stent Thrombosis. Arter. Thromb. Vasc. Biol. 2016, 36, 1534–1548. [Google Scholar] [CrossRef]
- Reinthaler, M.; Jung, F.; Landmesser, U.; Lendlein, A. Trend to move from permanent metals to degradable, multifunctional polymer or metallic implants in the example of coronary stents. Expert. Rev. Med. Devices 2016, 13, 1001–1003. [Google Scholar] [CrossRef]
- Factors Inducing In-Stent Restenosis: An In-Vitro Model|Request PDF. Available online: https://www.researchgate.net/publication/8246560_Factors_inducing_in-stent_restenosis_An_in-vitro_model (accessed on 25 November 2023).
- Jung, F.; Raghunath, M.; Blocki, A.; Gori, T. Restenosis after Coronary Stent Implantation: Cellular Mechanisms and Potential of Endothelial Progenitor Cells (A Short Guide for the Interventional Cardiologist). Cells 2022, 11, 2094. [Google Scholar]
- Fang, Y.I.; Namiki, H.; Tsunoda, E.; Shioda, S.; Shibata, M.; Nakatani, M.; Katagiri, T.; Takeyama, Y.; Ohata, H.; Honda, K.; et al. Marked increase in the histamine content of neointima after stent implantation of pig coronary artery and growth-promoting effects of histamine in cultured smooth muscle cells. Life Sci. 2005, 77, 241–251. [Google Scholar] [CrossRef]
- Vajen, T.; Benedikter, B.J.; Heinzmann, A.C.A.; Vasina, E.M.; Henskens, Y.; Parsons, M.; Maguire, P.B.; Stassen, F.R.; Heemskerk, J.W.M.; Schurgers, L.J.; et al. Platelet extracellular vesicles induce a pro-inflammatory smooth muscle cell phenotype. J. Extracell. Vesicles 2017, 6, 1322454. [Google Scholar] [CrossRef]
- Yan, J.; Bao, H.; Fan, Y.J.; Jiang, Z.L.; Qi, Y.X.; Han, Y. Platelet-derived microvesicles promote endothelial progenitor cell proliferation in intimal injury by delivering TGF-β1. FEBS J. 2020, 287, 5196–5217. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Qiu, H.; Lin, Z.; Fan, L.; Guo, Y.; Zhang, Y.; Chen, L. The Early Predictive Value of Circulating Monocytes and Eosinophils in Coronary DES Restenosis. Front. Cardiovasc. Med. 2022, 9, 764622. [Google Scholar] [CrossRef]
- Kennedy, S.; Wu, J.; Wadsworth, R.M.; Lawrence, C.E.; Maffia, P. Mast cells and vascular diseases. Pharmacol. Ther. 2013, 138, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Niccoli, G.; Montone, R.A.; Sabato, V.; Crea, F. Role of Allergic Inflammatory Cells in Coronary Artery Disease. Circulation 2018, 138, 1736–1748. [Google Scholar] [CrossRef] [PubMed]
- Takai, S.; Miyazaki, M. Development and Application of Chymase Inhibitors: Effect of Chymase Inhibitor on Vascular Proliferation. Jpn. J. Pharmacol. 2002, 90, 223–227. [Google Scholar] [CrossRef]
- Zhang, C.; Zhang, B.; Wang, H.; Tao, Q.; Ge, S.; Zhai, Z. Tumor necrosis factor alpha-stimulated gene-6 (TSG-6) inhibits the inflammatory response by inhibiting the activation of P38 and JNK signaling pathway and decreases the restenosis of vein grafts in rats. Heart Vessel. 2017, 32, 1536–1545. [Google Scholar] [CrossRef]
- Pelliccia, F.; Zimarino, M.; Niccoli, G.; Morrone, D.; De Luca, G.; Miraldi, F.; De Caterina, R. In-stent restenosis after percutaneous coronary intervention: Emerging knowledge on biological pathways. Eur. Heart J. Open 2023, 3, oead083. [Google Scholar] [CrossRef]
- Klein, L.W.; Nathan, S.; Maehara, A.; Messenger, J.; Mintz, G.S.; Ali, Z.A.; Rymer, J.; Sandoval, Y.; Al-Azizi, K.; Mehran, R.; et al. SCAI Expert Consensus Statement on Management of In-Stent Restenosis and Stent Thrombosis. J. Soc. Cardiovasc. Angiogr. Interv. 2023, 2, 100971. [Google Scholar] [CrossRef]
- Ninno, F.; Tsui, J.; Balabani, S.; Díaz-Zuccarini, V. A systematic review of clinical and biomechanical engineering perspectives on the prediction of restenosis in coronary and peripheral arteries. JVS Vasc. Sci. 2023, 4, 100128. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, J.; Serruys, P.W.; Silber, S.; Kelbaek, H.; Richardt, G.; Morel, M.A.; Negoita, M.; Buszman, P.E.; Windecker, S. Comparison of zotarolimus- and everolimus-eluting coronary stents: Final 5-year report of the RESOLUTE all-comers trial. Circ. Cardiovasc. Interv. 2015, 8, e002230. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Jiang, M.; Feng, H.; Han, Y.; Zhang, X.; Chen, Y.; Gao, L. The effect of sex differences on neointimal characteristics of in-stent restenosis in drug-eluting stents: An optical coherence tomography study. Heliyon 2023, 9, e19073. [Google Scholar] [CrossRef]
- Bajdechi, M.; Gurghean, A.; Bataila, V.; Scafa-Udriște, A.; Bajdechi, G.E.; Radoi, R.; Oprea, A.C.; Chioncel, V.; Mateescu, I.; Zekra, L.; et al. Particular Aspects Related to CD4+ Level in a Group of HIV-Infected Patients and Associated Acute Coronary Syndrome. Diagnostics 2023, 13, 2682. [Google Scholar] [CrossRef]
- Hajar, R. Risk Factors for Coronary Artery Disease: Historical Perspectives. Heart Views 2017, 18, 109. [Google Scholar] [CrossRef]
- Tocci, G.; Barbato, E.; Coluccia, R.; Modestino, A.; Pagliaro, B.; Mastromarino, V.; Giovannelli, F.; Berni, A.; Volpe, M. Blood Pressure Levels at the Time of Percutaneous Coronary Revascularization and Risk of Coronary In-Stent Restenosis. Am. J. Hypertens. 2016, 29, 509. [Google Scholar] [CrossRef] [PubMed]
- Alexandrescu, D.; Crisan, A.; Mitu, O.; Macovei, L.; Costache, I.I.; Ivona, M.I.; Frasinariu, O.; Alexandrescu, A.; Georgescu, C.A. Antiplatelet Therapy and Inflammatory Status Associated with Intra Stent Restenosis after Percutaneous Coronary Intervention. Med.-Surg. J. 2021, 125, 335–342. Available online: https://www.revmedchir.ro/index.php/revmedchir/article/view/2446 (accessed on 25 November 2023). [CrossRef]
- Singh, M.; Gersh, B.J.; McClelland, R.L.; Ho, K.K.L.; Willerson, J.T.; Penny, W.F.; Holmes, D.R. Clinical and angiographic predictors of restenosis after percutaneous coronary intervention: Insights from the Prevention of Restenosis with Tranilast and Its Outcomes (PRESTO) trial. Circulation 2004, 109, 2727–2731. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Zhang, Q.; Zhao, K.; Bian, Y.J.; Liu, Y.; Xue, Y.T. Risk factors for in-stent restenosis after coronary stent implantation in patients with coronary artery disease: A retrospective observational study. Medicine 2022, 101, E31707. [Google Scholar] [CrossRef]
- Ochijewicz, D.; Tomaniak, M.; Opolski, G.; Kochman, J. Inflammation as a determinant of healing response after coronary stent implantation. Int. J. Cardiovasc. Imaging 2021, 37, 791. [Google Scholar] [CrossRef]
- Mehran, R.; Dangas, G.; Abizaid, A.S.; Mintz, G.S.; Lansky, A.J.; Satler, L.F.; Pichard, A.D.; Kent, K.M.; Stone, G.W.; Leon, M.B. Angiographic Patterns of In-Stent Restenosis. Circulation 1999, 100, 1872–1878. [Google Scholar] [CrossRef]
- Cassese, S.; Byrne, R.A.; Tada, T.; Pinieck, S.; Joner, M.; Ibrahim, T.; King, L.A.; Fusaro, M.; Laugwitz, K.L.; Kastrati, A. Incidence and predictors of restenosis after coronary stenting in 10 004 patients with surveillance angiography. Heart 2014, 100, 153–159. [Google Scholar] [CrossRef]
- De Luca, L.; Rosano, G.M.C.; Spoletini, I. Post-percutaneous coronary intervention angina: From physiopathological mechanisms to individualized treatment. Cardiol. J. 2022, 29, 850. [Google Scholar] [CrossRef] [PubMed]
- Elwany, M.N.; Abskharoun, M.; Dawood, M.; Al-Tahan, S.M.; Sanhoury, M. The utility and effectiveness of the newer generation high-resolution coronary computed tomography angiography in the evaluation of coronary in-stent restenosis. Curr. Probl. Cardiol. 2024, 49, 102212. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.S.; John, J.M.; Chew, D.P.; Lee, D.S.; Ellis, S.G.; Bhatt, D.L. Bare metal stent restenosis is not a benign clinical entity. Am. Heart J. 2006, 151, 1260–1264. [Google Scholar] [CrossRef]
- Walters, D.L.; Harding, S.A.; Walsh, C.R.; Wong, P.; Pomerantsev, E.; Jang, I.K. Acute coronary syndrome is a common clinical presentation of in-stent restenosis. Am. J. Cardiol. 2002, 89, 491–494. [Google Scholar] [CrossRef]
- Mishkel, G.J.; Moore, A.L.; Markwell, S.; Shelton, M.C.; Shelton, M.E. Long-term outcomes after management of restenosis or thrombosis of drug-eluting stents. J. Am. Coll. Cardiol. 2007, 49, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Fineschi, M.; Gori, T.; Pierli, C.; Casini, S.; Sinicropi, G.; Buti, A.; Iadanza, A.; Bravi, A. Symptomatic failure after sirolimus-eluting stent implantation: A rare but challenging condition. Can. J. Cardiol. 2007, 23, 139. [Google Scholar] [CrossRef] [PubMed]
- Abouelnour, A.; Gori, T. Intravascular imaging in coronary stent restenosis: Prevention, characterization, and management. Front. Cardiovasc. Med. 2022, 9, 843734. [Google Scholar] [CrossRef]
- Perera, D.; Postema, P.; Rashid, R.; Patel, S.; Blows, L.; Marber, M.; Redwood, S. Does a well developed collateral circulation predispose to restenosis after percutaneous coronary intervention? An intravascular ultrasound study. Heart 2006, 92, 763. [Google Scholar] [CrossRef]
- Koskinas, K.C.; Mach, F.; Räber, L. Lipid-lowering therapy and percutaneous coronary interventions. EuroIntervention 2021, 16, 1389–1403. [Google Scholar] [CrossRef]
- Sousa-Uva, M.; Neumann, F.J.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef]
- Byrne, R.A.; Colleran, R.; Kastrati, A. Strengths and limitations of real world data in patients treated with coronary stents. Circ. Cardiovasc. Interv. 2018, 11, 7239. [Google Scholar] [CrossRef]
- Rykowska, I.; Nowak, I.; Nowak, R. Drug-Eluting Stents and Balloons—Materials, Structure Designs, and Coating Techniques: A Review. Molecules 2020, 25, 4624. [Google Scholar] [CrossRef]
- Tan, Q.; Wang, Q.; Yang, H.; Jing, Z.; Ming, C. Clinical outcomes of drug-eluting balloon for treatment of small coronary artery in patients with acute myocardial infarction. Intern. Emerg. Med. 2021, 16, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Hildick-Smith, D.; Arunothayaraj, S.; Stankovic, G.; Chen, S.L. Percutaneous coronary intervention of bifurcation lesions. EuroIntervention 2022, 18, E273–E291. [Google Scholar] [CrossRef] [PubMed]
- Alfonso, F.; Coughlan, J.J.; Giacoppo, D.; Kastrati, A.; Byrne, R.A. Management of in-stent restenosis. EuroIntervention 2022, 18, E103–E123. [Google Scholar] [CrossRef] [PubMed]
- Study Details|SELUTION SLRTM 014 In-Stent Restenosis|ClinicalTrials.gov. Available online: https://clinicaltrials.gov/study/NCT04280029 (accessed on 20 January 2024).
- Study Details|Treatment of In-Stent Restenosis 2 Study|ClinicalTrials.gov. Available online: https://clinicaltrials.gov/study/NCT03667313 (accessed on 20 January 2024).
- Study Details|Treatment of Coronary In-Stent Restenosis (ISR) by a Sirolimus Coated or a Paclitaxel Coated Balloon|ClinicalTrials.gov. Available online: https://clinicaltrials.gov/study/NCT03242096 (accessed on 20 January 2024).
- Study Details|Treatment of In-Stent Restenosis by Paclitaxel Coated PTCA Balloons (PACCOCATH-ISR I)|ClinicalTrials.gov. (n.d.). Available online: https://clinicaltrials.gov/study/NCT00106587 (accessed on 28 January 2024).
- Study Details|Treatment of in-Stent Restenosis by Paclitaxel Coated PTCA Balloons (PACCOCATH-ISR II)|ClinicalTrials.gov. (n.d.). Available online: https://clinicaltrials.gov/study/NCT00409981 (accessed on 28 January 2024).
- Scheller, B.; Hehrlein, C.; Bocksch, W.; Rutsch, W.; Haghi, D.; Dietz, U.; Böhm, M.; Speck, U. Treatment of coronary in-stent restenosis with a paclitaxel-coated balloon catheter. N. Engl. J. Med. 2006, 355, 2113–2124. [Google Scholar] [CrossRef] [PubMed]
- Kheifets, M.; Rahat, O.; Bental, T.; Levi, A.; Vaknin-Assa, H.; Greenberg, G.; Codner, P.; Witberg, G.; Kornowski, R.; Perl, L. Outcomes of Drug Eluting Balloons for In-Stent Restenosis: Large Cohort Analysis and Single Center Clinical Experience. Can. J. Cardiol. 2024, in press. [Google Scholar] [CrossRef] [PubMed]
- Alfonso, F.; Byrne, R.A.; Rivero, F.; Kastrati, A. Current Treatment of In-Stent Restenosis. J. Am. Coll. Cardiol. 2014, 63, 2659–2673. [Google Scholar] [CrossRef] [PubMed]
- Giacoppo, D.; Gargiulo, G.; Aruta, P.; Capranzano, P.; Tamburino, C.; Capodanno, D. Treatment strategies for coronary in-stent restenosis: Systematic review and hierarchical Bayesian network meta-analysis of 24 randomised trials and 4880 patients. BMJ 2015, 351, h5392. [Google Scholar] [CrossRef]
- Siontis, G.C.M.; Stefanini, G.G.; Mavridis, D.; Siontis, K.C.; Alfonso, F.; Pérez-Vizcayno, M.J.; Byrne, R.A.; Kastrati, A.; Meier, B.; Salanti, G.; et al. Percutaneous coronary interventional strategies for treatment of in-stent restenosis: A network meta-analysis. Lancet 2015, 386, 655–664. [Google Scholar] [CrossRef]
- Sousa-Uva, M.; Neumann, F.J.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. J. Cardiothoracic Surg. 2019, 55, 4–90. [Google Scholar] [CrossRef]
- Cassese, S.; Byrne, R.A.; Schulz, S.; Hoppman, P.; Kreutzer, J.; Feuchtenberger, A.; Ibrahim, T.; Ott, I.; Fusaro, M.; Schunkert, H.; et al. Prognostic role of restenosis in 10 004 patients undergoing routine control angiography after coronary stenting. Eur. Heart J. 2015, 36, 94–99. [Google Scholar] [CrossRef]
- Giacoppo, D.; Alfonso, F.; Xu, B.; Claessen, B.E.P.M.; Adriaenssens, T.; Jensen, C.; Pérez-Vizcayno, M.J.; Kang, D.Y.; Degenhardt, R.; Pleva, L.; et al. Paclitaxel-coated balloon angioplasty vs. drug-eluting stenting for the treatment of coronary in-stent restenosis: A comprehensive, collaborative, individual patient data meta-analysis of 10 randomized clinical trials (DAEDALUS study). Eur. Heart J. 2020, 41, 3715–3728. [Google Scholar] [CrossRef]
- Holmes, D.R.; Teirstein, P.; Satler, L.; Sketch, M.; O’Malley, J.; Popma, J.J.; Kuntz, R.E.; Fitzgerald, P.J.; Wang, H.; Caramanica, E.; et al. Sirolimus-eluting stents vs vascular brachytherapy for in-stent restenosis within bare-metal stents: The SISR randomized trial. JAMA 2006, 295, 1264–1273. [Google Scholar] [CrossRef]
- Stone, G.W.; Ellis, S.G.; O’Shaughnessy, C.D.; Martin, S.L.; Satler, L.; McGarry, T.; Turco, M.A.; Kereiakes, D.J.; Kelley, L.; Popma, J.J.; et al. Paclitaxel-eluting stents vs vascular brachytherapy for in-stent restenosis within bare-metal stents: The TAXUS V ISR randomized trial. JAMA 2006, 295, 1253–1263. [Google Scholar] [CrossRef]
- Park, S.W.; Lee, S.W.; Koo, B.K.; Park, D.W.; Lee, S.W.; Kim, Y.H.; Lee, C.W.; Hong, M.K.; Kim, J.J.; Mori, K.; et al. Treatment of diffuse IN-stent restenosis with Drug-Eluting stents vs. intracoronary bEta-raDiation therapy: INDEED Study. Int. J. Cardiol. 2008, 131, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Kastrati, A.; Mehilli, J.; Von Beckerath, N.; Dibra, A.; Hausleiter, J.; Pache, J.; Schühlen, H.; Schmitt, C.; Dirschinger, J.; Schömig, A. Sirolimus-eluting stent or paclitaxel-eluting stent vs balloon angioplasty for prevention of recurrences in patients with coronary in-stent restenosis: A randomized controlled trial. JAMA 2005, 293, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Alfonso, F.; Pérez-Vizcayno, M.J.; Hernandez, R.; Bethencourt, A.; Martí, V.; López-Mínguez, J.R.; Angel, J.; Mantilla, R.; Morís, C.; Cequier, A.; et al. A randomized comparison of sirolimus-eluting stent with balloon angioplasty in patients with in-stent restenosis: Results of the Restenosis Intrastent: Balloon Angioplasty versus Elective Sirolimus-Eluting Stenting (RIBS-II) trial. J. Am. Coll. Cardiol. 2006, 47, 2152–2160. [Google Scholar] [CrossRef] [PubMed]
- Chevalier, B.; Moulichon, R.; Teiger, E.; Brunel, P.; Metzger, J.P.; Pansieri, M.; Carrie, D.; Stoll, H.P.; Wittebols, K.; Spaulding, C.; et al. One-year results of the CRISTAL Trial, a randomized comparison of cypher sirolimus-eluting coronary stents versus balloon angioplasty for restenosis of drug-eluting stents. J. Interv. Cardiol. 2012, 25, 586–595. [Google Scholar] [CrossRef]
- Byrne, R.A.; Joner, M.; Alfonso, F.; Kastrati, A. Drug-coated balloon therapy in coronary and peripheral artery disease. Nat. Rev. Cardiol. 2014, 11, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Hamm, C.W.; Dörr, O.; Wöhrle, J.; Krackhardt, F.; Ince, H.; Zeus, T.; Berland, J.; Piot, C.; Roubille, F.; Schult, I.; et al. A multicentre, randomised controlled clinical study of drug-coated balloons for the treatment of coronary in-stent restenosis. EuroIntervention 2020, 16, E328–E334. [Google Scholar] [CrossRef]
- Rittger, H.; Brachmann, J.; Sinha, A.M.; Waliszewski, M.; Ohlow, M.; Brugger, A.; Thiele, H.; Birkemeyer, R.; Kurowski, V.; Breithardt, O.A.; et al. A Randomized, Multicenter, Single-Blinded Trial Comparing Paclitaxel-Coated Balloon Angioplasty With Plain Balloon Angioplasty in Drug-Eluting Stent Restenosis: The PEPCAD-DES Study. J. Am. Coll. Cardiol. 2012, 59, 1377–1382. [Google Scholar] [CrossRef]
- Habara, S.; Iwabuchi, M.; Inoue, N.; Nakamura, S.; Asano, R.; Nanto, S.; Hayashi, Y.; Shiode, N.; Saito, S.; Ikari, Y.; et al. A multicenter randomized comparison of paclitaxel-coated balloon catheter with conventional balloon angioplasty in patients with bare-metal stent restenosis and drug-eluting stent restenosis. Am. Heart J. 2013, 166, 527–533.e2. [Google Scholar] [CrossRef]
- Freisinger, E.; Koeppe, J.; Gerss, J.; Goerlich, D.; Malyar, N.M.; Marschall, U.; Faldum, A.; Reinecke, H. Mortality after use of paclitaxel-based devices in peripheral arteries: A real-world safety analysis. Eur. Heart J. 2020, 41, 3732–3739. [Google Scholar] [CrossRef]
- Verheye, S.; Vrolix, M.; Kumsars, I.; Erglis, A.; Sondore, D.; Agostoni, P.; Cornelis, K.; Janssens, L.; Maeng, M.; Slagboom, T.; et al. The SABRE Trial (Sirolimus Angioplasty Balloon for Coronary In-Stent Restenosis): Angiographic Results and 1-Year Clinical Outcomes. JACC Cardiovasc. Interv. 2017, 10, 2029–2037. [Google Scholar] [CrossRef]
- Katsanos, K.; Spiliopoulos, S.; Kitrou, P.; Krokidis, M.; Karnabatidis, D. Risk of Death Following Application of Paclitaxel-Coated Balloons and Stents in the Femoropopliteal Artery of the Leg: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Am. Heart Assoc. 2018, 7, e011245. [Google Scholar] [CrossRef] [PubMed]
- Cortese, B.; di Palma, G.; Latini, R.A.; Elwany, M.; Orrego, P.S.; Seregni, R.G. Immediate and short-term performance of a novel sirolimus-coated balloon during complex percutaneous coronary interventions. The FAtebenefratelli SIrolimus COated-balloon (FASICO) registry. Cardiovasc. Revasc Med. 2017, 18, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Palop, R.; Pinar, E.; Lozano, Í.; Saura, D.; Picó, F.; Valdés, M. Utility of the fractional flow reserve in the evaluation of angiographically moderate in-stent restenosis. Eur. Heart J. 2004, 25, 2040–2047. [Google Scholar] [CrossRef]
- Waksman, R.; Chitturi, K.R. Myths and Truths in the Management of Drug-Eluting Stent In-Stent Restenosis. JACC Cardiovasc. Interv. 2024, 17, 14–16. [Google Scholar] [CrossRef]
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.A.; Dweck, M.R.; Galbraith, M. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cell Type | Role in ISR | Mechanism/Effect |
|---|---|---|
| Smooth muscle cells | Primary contributors to neointimal hyperplasia | Proliferate and migrate, contributing to luminal narrowing; transition from contractile to synthetic phenotype. |
| Platelets | Initial responders to stent placement | Release thromboxane A2 and PDGF, inducing oxidative stress and smooth muscle cell transition. |
| Mast cells | Role in neointimal formation | Release chymase, influencing angiotensin II and TGF-β production, leading to fibroblast proliferation. |
| Monocytes | Involved in the inflammatory response and late ISR risk | Elevated levels post-PCI are indicative of late ISR risk. Participate in cytokine secretion. |
| Eosinophils | Associated with late ISR | Elevated levels post-PCI are predictive of late ISR. |
| Macrophages | Part of the inflammatory response | Infiltrate subendothelial space, involved in neo-atherosclerosis and neointimal formation. |
| Endothelial cells | Affected by stent deployment | Disruption leads to exposure of the intimal layer and a prothrombotic effect. |
| Bone marrow progenitor cells (BMPCs) | Contribute to neointimal formation | Recruitment and proliferation within the extracellular matrix. |
| Fibroblasts | Involved in neointimal formation | Proliferation influenced by mast cell-released chymase and TGF-β. |
| ClinicalTrials.gov Identifier | Official Title | Intervention/Treatment | References |
|---|---|---|---|
| NCT04280029 | SELUTION SLR™ 014 In-stent Restenosis | Device: SELUTION SLR™ DEB; Device: Control | [82] |
| NCT03667313 | Treatment of In-Stent Restenosis 2 Study | Combination Product: sirolimus-eluting balloon (SEB) Magic Touch Combination Product: paclitaxel-eluting balloon (PEB) Sequent Please | [83] |
| NCT03242096 | Treatment of Coronary In-stent Restenosis (ISR) by a Sirolimus Coated or a Paclitaxel Coated Balloon | Combination Product: Sirolimus-coated balloon Combination Product: Paclitaxel-coated balloon | [84] |
| NCT00106587 | Treatment of In-Stent Restenosis by Paclitaxel Coated PTCA Balloons (PACCOCATH—ISR I) | Device: PTCA Combination Product: Paclitaxel-coated balloon catheter (device with drug) | [85] |
| NCT00409981 | Treatment of in-Stent Restenosis by Paclitaxel Coated PTCA Balloons (PACCOCATH—ISR II) | Device: Paclitaxel-coated balloon catheter (device with drug) | [86] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bajeu, I.-T.; Niculescu, A.-G.; Scafa-Udriște, A.; Andronescu, E. Intrastent Restenosis: A Comprehensive Review. Int. J. Mol. Sci. 2024, 25, 1715. https://doi.org/10.3390/ijms25031715
Bajeu I-T, Niculescu A-G, Scafa-Udriște A, Andronescu E. Intrastent Restenosis: A Comprehensive Review. International Journal of Molecular Sciences. 2024; 25(3):1715. https://doi.org/10.3390/ijms25031715
Chicago/Turabian StyleBajeu, Ioan-Teodor, Adelina-Gabriela Niculescu, Alexandru Scafa-Udriște, and Ecaterina Andronescu. 2024. "Intrastent Restenosis: A Comprehensive Review" International Journal of Molecular Sciences 25, no. 3: 1715. https://doi.org/10.3390/ijms25031715
APA StyleBajeu, I.-T., Niculescu, A.-G., Scafa-Udriște, A., & Andronescu, E. (2024). Intrastent Restenosis: A Comprehensive Review. International Journal of Molecular Sciences, 25(3), 1715. https://doi.org/10.3390/ijms25031715