
Giant Arachnoid Granulations: A Systematic Literature Review


Abstract
1. Introduction
2. Methods
3. Results
3.1. Reports and GAG Cases
3.2. Demographic Features
3.3. GAG Size and Morphology
3.4. Anatomical Distribution and Frequency
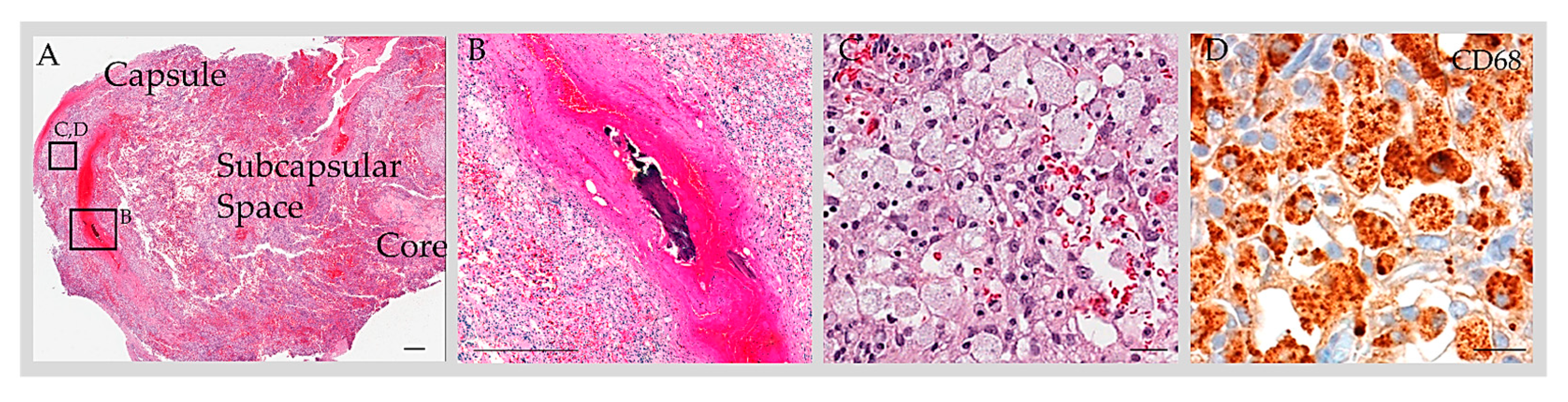
3.5. Reported GAG Histology
3.6. Signs and Symptoms
3.7. Imaging Features
3.8. Clinical Course and Medical Treatment
3.9. Interventional Surgical Treatment
3.10. Surgical Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AG | arachnoid granulation |
| CSF | cerebrospinal fluid |
| CT | computed tomography |
| DVS | dural venous sinus |
| GAG | giant arachnoid granulation |
| MRI | magnetic resonance imaging |
| SSS | superior sagittal sinus |
| TS | transverse sinus |
References
- Shah, T.; Leurgans, S.E.; Mehta, R.I.; Yang, J.; Galloway, C.A.; Bentley, K.L.d.M.; Schneider, J.A.; Mehta, R.I. Arachnoid granulations are lymphatic conduits that communicate with bone marrow and dura-arachnoid stroma. J. Exp. Med. 2023, 220, e20220618. [Google Scholar] [CrossRef] [PubMed]
- Vesalius, A. Fabrica; Singer, C., Translator; Oxford University Press: Oxford, UK, 1952. [Google Scholar]
- Scully, R.B.; Mark, E.J.; McNeely, B.U. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 42-1984. A 29-year-old woman with a lytic lesion of a parietal bone. N. Engl. J. Med. 1984, 311, 1036–1043. [Google Scholar]
- Turner, L. The structure of arachnoid granulations with observations on their physiological and pathological significance. Ann. R. Coll. Surg. Engl. 1961, 29, 237–264. [Google Scholar] [PubMed]
- Willis, T. Cerebri Anatome; cui Accessit Nervorum Descriptio et Usus; Flesher: London, UK, 1664. [Google Scholar]
- Leach, J.L.; Jones, B.V.; Tomsick, T.A.; Stewart, C.A.; Balko, M.G. Normal appearance of arachnoid granulations on contrast-enhanced CT and MR of the brain: Differentiation from dural sinus disease. AJNR Am. J. Neuroradiol. 1996, 17, 1523–1532. [Google Scholar] [PubMed]
- Giraud, P.; Segal, O.; Chauvet, S. Laughing headache with giant pacchionian granulations. Headache 2013, 53, 681–683. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.M.; Shaw, B.H.; Wallace, C.J.; Metz, L. A Pacchionian Puzzle. Can. J. Neurol. Sci. 2020, 47, 231–232. [Google Scholar] [CrossRef] [PubMed]
- Haybaeck, J.; Silye, R.; Soffer, D. Dural arachnoid granulations and “giant” arachnoid granulations. Surg. Radiol. Anat. 2008, 30, 417–421. [Google Scholar] [CrossRef][Green Version]
- Mamourian, A.C.; Towfighi, J. MR of giant arachnoid granulation, a normal variant presenting as a mass within the dural venous sinus. AJNR Am. J. Neuroradiol. 1995, 16, 901–904. [Google Scholar]
- Trimble, C.R.; Harnsberger, H.R.; Castillo, M.; Brant-Zawadzki, M.; Osborn, A.G. “Giant” arachnoid granulations just like CSF?: NOT!! AJNR Am. J. Neuroradiol. 2010, 31, 1724–1728. [Google Scholar] [CrossRef]
- Lu, C.X.; Du, Y.; Xu, X.X.; Li, Y.; Yang, H.F.; Deng, S.Q.; Xiao, D.M.; Li, B.; Tian, Y.H. Multiple occipital defects caused by arachnoid granulations: Emphasis on T2 mapping. World J. Radiol. 2012, 4, 341–344. [Google Scholar] [CrossRef]
- Chan, R.; de Tilly, L.N.; Bilbao, J. Magnetic resonance appearance of a giant cystic arachnoidal granulation presenting as an osteolytic parietal bone lesion: Case report. Can. Assoc. Radiol. J. 1999, 50, 126–129. [Google Scholar]
- Gacek, R.R. Arachnoid granulation cerebrospinal fluid otorrhea. Ann. Otol. Rhinol. Laryngol. 1990, 99, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, A.E.; O’Connell, J.X.; Ojemann, R.G.; Plata, M.J.; Palmer, W.E. Giant cystic arachnoid granulations: A rare cause of lytic skull lesions. Hum. Pathol. 1993, 24, 438–441. [Google Scholar] [CrossRef] [PubMed]
- Beatty, R.M.; Hornig, G.W.; Hanson, E.J., Jr. Protruding arachnoid granulations mimicking dermoid cysts. J. Pediatr. Surg. 1989, 24, 411–413. [Google Scholar] [CrossRef] [PubMed]
- Gozgec, E.; Ogul, H.; Izgi, E.; Kantarci, M. Tissue damage in herniated brain parenchyma into giant arachnoid granulations: Demonstration with high resolution MRI. Acta Radiol. 2021, 62, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Ogul, H.; Guven, F.; Izgi, E.; Kantarci, M. Evaluation of giant arachnoid granulations with high-resolution 3D-volumetric MR sequences at 3T. Eur. J. Radiol. 2019, 121, 108722. [Google Scholar] [CrossRef]
- Park, H.; Lim, G.Y.; Eom, T.H. Giant arachnoid granulation in a child with benign intracranial hypertension: An unusual case. Childs Nerv. Syst. 2018, 34, 2525–2527. [Google Scholar] [CrossRef] [PubMed]
- Sade, R.; Ogul, H. Herniation of the Cerebral Gyrus Into the Giant Arachnoid Granulation in a Child With Intermittent Headache. Headache 2016, 56, 750–752. [Google Scholar] [CrossRef]
- Chin, S.C.; Chen, C.Y.; Lee, C.C.; Chen, F.H.; Lee, K.W.; Hsiao, H.S.; Zimmerman, R.A. Giant arachnoid granulation mimicking dural sinus thrombosis in a boy with headache: MRI. Neuroradiology 1998, 40, 181–183. [Google Scholar] [CrossRef]
- De Keyzer, B.; Bamps, S.; Van Calenbergh, F.; Demaerel, P.; Wilms, G. Giant arachnoid granulations mimicking pathology. A report of three cases. Neuroradiol. J. 2014, 27, 316–321. [Google Scholar] [CrossRef]
- Umeh, R.; Oskouian, R.J.; Loukas, M.; Tubbs, R.S. Giant Arachnoid Granulation Associated with Anomalous Draining Vein: A Case Report. Cureus 2017, 9, e1065. [Google Scholar] [CrossRef] [PubMed]
- Taieb, G.; Dargazanli, C.; Prin, P.; Charif, M.; Ducros, A. Reversible giant arachnoid granulations. Neurology 2018, 91, 1107–1108. [Google Scholar] [CrossRef] [PubMed]
- Kiroglu, Y.; Yaqci, B.; Cirak, B.; Karabulut, N. Giant arachnoid granulation in a patient with benign intracranial hypertension. Eur. Radiol. 2008, 18, 2329–2332. [Google Scholar] [CrossRef] [PubMed]
- Gadot, R.; Hoang, A.N.; Raper, D.M.S.; Sweeney, A.D.; Juliano, M.; Lustrin, E.; Tanweer, O. Arachnoid Granulation Causing Unilateral Pulsatile Tinnitus Treated With Dural Venous Sinus Stenting. Otol. Neurotol. 2023, 44, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.A.; Frombach, E.; Heyer, C.M. Giant arachnoid granulation: Differential diagnosis of acute headache. Australas. Radiol. 2007, 51, B18–B20. [Google Scholar] [CrossRef] [PubMed]
- Deep, N.L.; Hoxworth, J.M.; Stevens, C.J.; Link, M.J.; Driscoll, C.L.; Wood, C.P. Giant Posterior Temporal Bone Arachnoid Granulations: CT and MRI Findings. Otol. Neurotol. 2016, 37, 963–966. [Google Scholar] [CrossRef] [PubMed]
- Pereira, V.M.; Cancelliere, N.M.; Najafi, M.; MacDonald, D.; Natarajan, T.; Radovanovic, I.; Krings, T.; Rutka, J.; Nicholson, P.; Steinman, D.A. Torrents of torment: Turbulence as a mechanism of pulsatile tinnitus secondary to venous stenosis revealed by high-fidelity computational fluid dynamics. J. Neurointerv. Surg. 2021, 13, 732–737. [Google Scholar] [CrossRef]
- Ayaz, E.; Atalay, B.; Baysal, B.; Senturk, S.; Aslan, A. Giant arachnoid granulation mimicking dural sinus thrombosis. North. Clin. Istanb. 2017, 4, 185–187. [Google Scholar] [CrossRef][Green Version]
- Mamaliga, T.; Hadi, M. An unusual vermiform giant arachnoid granulation. Radiol. Case Rep. 2019, 14, 1525–1528. [Google Scholar] [CrossRef]
- Blaauw, G. Cranial extradural cyst. Acta Neurochir. 1979, 49, 81–86. [Google Scholar] [CrossRef]
- Deprez, F.C.; Hernalsteen, D.; Bosschaert, P. Arachnoid Pacchioni’s granulation bulging in a transverse sinus of the brain. JBR-BTR 2010, 93, 104. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kan, P.; Stevens, E.A.; Couldwell, W.T. Incidental giant arachnoid granulation. AJNR Am. J. Neuroradiol. 2006, 27, 1491–1492. [Google Scholar] [PubMed]
- Choi, H.J.; Cho, C.W.; Kim, Y.S.; Cha, J.H. Giant arachnoid granulation misdiagnosed as transverse sinus thrombosis. J. Korean Neurosurg. Soc. 2008, 43, 48–50. [Google Scholar] [CrossRef] [PubMed]
- Sunbulli, M.; Zak, I.; Chaturvedi, S. Giant arachnoid granulations. Neurology 2005, 64, 2150. [Google Scholar] [CrossRef] [PubMed]
- Monté, A.S.; De Bleecker, J.L.; Buccauw, K.; Boulanger, T.; De Cocker, L.J. Giant arachnoid granulation of the posterior temporal bone wall mimicking a jugular foramen mass. Acta Neurol. Belg. 2015, 115, 421–422. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, J.R.; Santos, G.R. Brain Herniation into Giant Arachnoid Granulation: An Unusual Case. Case Rep. Radiol. 2017, 2017, 8532074. [Google Scholar] [CrossRef] [PubMed]
- Karegowda, L.H.; Rajagopal, K.; Krishnamurthy, S.K.; Lakshmana, S. Giant arachnoid granulation with a thrombosed dural arteriovenous fistula. BMJ Case Rep. 2018, 2018, bcr2018224851. [Google Scholar] [CrossRef]
- Arjona, A.; Delgado, F.; Fernandez-Romero, E. Intracranial hypertension secondary to giant arachnoid granulations. J. Neurol. Neurosurg. Psychiatry 2003, 74, 418. [Google Scholar] [CrossRef]
- Zheng, H.; Zhou, M.; Zhao, B.; Zhou, D.; He, L. Pseudotumor cerebri syndrome and giant arachnoid granulation: Treatment with venous sinus stenting. J. Vasc. Interv. Radiol. 2010, 21, 927–929. [Google Scholar] [CrossRef]
- Yang, I.H.; Pereira, V.M.; Lenck, S.; Nicholson, P.; Orru, E.; Klostranec, J.M.; Krings, T.; Tsang, A.C.O. Endovascular treatment of debilitating tinnitus secondary to cerebral venous sinus abnormalities: A literature review and technical illustration. J. Neuro-Interv. Surg. 2019, 11, 841–846. [Google Scholar] [CrossRef]
- Rosenberg, K.I.; Banik, R. Pseudotumor cerebri syndrome associated with giant arachnoid granulation. J. Neuro-Ophthalmol. 2013, 33, 417–419. [Google Scholar] [CrossRef]
- Esposito, G.; Della Pepa, G.M.; Sturiale, C.L.; Gaudino, S.; Anile, C.; Pompucci, A. Hypertrophic arachnoid granulation of the occipital bone: Neuroradiological differential diagnosis. Clin. Neuroradiol. 2011, 21, 239–243. [Google Scholar] [CrossRef]
- Mehta, R.I.; Mehta, R.I. Giant arachnoid granulations: Diagnostic workup and characterization in three symptomatic adults. Int. J. Mol. Sci. 2023, 24, 11410. [Google Scholar] [CrossRef]
- Browder, J.; Kaplan, H.A.; Howard, E.M. Hyperplasia of pacchionian granulations. Arch. Pathol. 1973, 95, 315–316. [Google Scholar]
- le Gros Clark, W.E. On the Pacchionian Bodies. J. Anat. 1920, 55, 40–48. [Google Scholar]
- Dinkin, M.J.; Patsalides, A. Idiopathic Intracranial Venous Hypertension: Toward a Better Understanding of Venous Stenosis and the Role of Stenting in Idiopathic Intracranial Hypertension. J. Neuroophthalmol. 2023. ahead of print. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age * | |
| Range *, years | 0.33–91 |
| Mean *, years (SD) | 43 ± 20 |
| Gender, n (%) | |
| Male | 67/169 (40%) |
| Female | 80/169 (47%) |
| Unknown | 22/169 (13%) |
| Comorbidities/Past Medical History | |
| Obesity (low to moderate) | 4/169 (2%) |
| Cerebral small vessel disease | 4/169 (2%) |
| Systemic hypertension | 3/169 (2%) |
| Nonspecific white matter change | 2/169 (1%) |
| Intracranial hypertension | 2/169 (1%) |
| Parkinson’s disease | 2/169 (1%) |
| Carcinoma, colonic type | 1/169 (1%) |
| Cerebral aneurysm | 1/169 (1%) |
| Diabetes mellitus, type II | 1/169 (1%) |
| Hypothyroidism | 1/169 (1%) |
| Meningioma | 1/169 (1%) |
| Retrobulbar neuritis | 1/169 (1%) |
| Seizure disorder | 1/169 (1%) |
| Tonsillectomy | 1/169 (1%) |
| Number of GAG | |
| One GAG | 149/169 (88%) |
| At least two GAG | 18/169 (11%) |
| Evidence of more than two GAG | 3/169 (2%) |
| Associated vascular abnormality | 5/169 (3%) |
| Anterior cerebral artery aneurysm | 1/169 (1%) |
| Arteriovenous fistula | 1/169 (1%) |
| Benign intracranial venous hypertension | 1/169 (1%) |
| High-riding jugular bulb | 1/169 (1%) |
| Hypoplastic left jugular and left transverse veins | 1/169 (1%) |
| Size | |
| Range, cm | 0.4–6.0 |
| Mean, cm (SD) | 1.9 ± 1.1 |
| Location | |
| Intrasinus or DVS type | 162/195 (83%) |
| Calvarial or diploic type | 31/195 (16%) |
| Symptoms | |
| Absent (incidental) | 9/169 (5%) |
| Present (symptomatic) | 68/169 (40%) |
| Not Specified | 93/169 (55%) |
| Onset/Exacerbating Factor | 9/169 (5%) |
| With head position | 2/169 (1%) |
| Head-down tilt Right-sided head turn | 1/169 (1%) 1/169 (1%) |
| With acute event | 8/169 (5%) |
| Acute head injury | 3/169 (2%) |
| Acute exertion | 3/169 (2%) |
| Acute heat exhaustion | 1/169 (1%) |
| Laughing | 1/169 (1%) |
| Sneezing | 1/169 (1%) |
| Coughing | 2/169 (1%) |
| With chronic event | 2/169 (1%) |
| Remote head injury | 3/169 (2%) |
| Relieving Factor | 6/169 (4%) |
| I/L Jugular vein compression | 6/169 (4%) |
| Myringotomy tube drainage | 1/169 (1%) |
| Complications | 38/169 (22%) |
| Intraocular peripapillary hemorrhage | 1/169 (1%) |
| Brain herniation | 38/169 (22%) |
| Cerebellum involvement | 16/169 (9%) |
| Cerebrum involvement | 13/169 (8%) |
| With brain atrophy | 11/169 (7%) |
| With brain gliosis | 6/169 (4%) |
| With brain infarction | 1/169 (1%) |
| Headache | 32/169 (19%) |
| Vision change | 10/169 (6%) |
| Hearing Change | 9/169 (5%) |
| Vertigo | 6/169 (4%) |
| Intracranial hypertension | 4/169 (2%) |
| Mental status change or change in consciousness | 4/169 (2%) |
| Other, NOS * | 4/169 (2%) |
| Papilledema | 4/169 (2%) |
| Paresthesia | 4/169 (2%) |
| Mass | 3/169 (2%) |
| Seizure | 3/169 (2%) |
| Syncope or loss of consciousness | 3/169 (2%) |
| Anxiety | 2/169 (1%) |
| Nausea | 2/169 (1%) |
| Neck pain | 2/169 (1%) |
| Facial droop | 1/169 (1%) |
| Chronic ataxia | 1/169 (1%) |
| Elevated opening CSF pressure | 1/169 (1%) |
| Low-grade fever | 1/169 (1%) |
| Meningism | 1/169 (1%) |
| Meningitis | 1/169 (1%) |
| Optic disc nasal effacement | 1/169 (1%) |
| Otitis media | 1/169 (1%) |
| Otitis media, serous | 1/169 (1%) |
| Pain, NOS | 1/169 (1%) |
| Repetitive hemorrhagic episodes, NOS | 1/169 (1%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mehta, R.I.; Mehta, R.I. Giant Arachnoid Granulations: A Systematic Literature Review. Int. J. Mol. Sci. 2023, 24, 13014. https://doi.org/10.3390/ijms241613014
Mehta RI, Mehta RI. Giant Arachnoid Granulations: A Systematic Literature Review. International Journal of Molecular Sciences. 2023; 24(16):13014. https://doi.org/10.3390/ijms241613014
Chicago/Turabian StyleMehta, Rupal I., and Rashi I. Mehta. 2023. "Giant Arachnoid Granulations: A Systematic Literature Review" International Journal of Molecular Sciences 24, no. 16: 13014. https://doi.org/10.3390/ijms241613014
APA StyleMehta, R. I., & Mehta, R. I. (2023). Giant Arachnoid Granulations: A Systematic Literature Review. International Journal of Molecular Sciences, 24(16), 13014. https://doi.org/10.3390/ijms241613014