
Persistence of Anti-S1 IgG against SARS-CoV-2 Eight Months after the Booster Dose of Vaccine in Naive and Previously Infected Healthcare Workers

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Krammer, F. SARS-CoV-2 vaccine in development. Nature 2020, 586, 516–527. [Google Scholar] [CrossRef] [PubMed]
- Serrano, L.; Algarate, S.; Herrero-Cortina, B.; Bueno, J.; González-Barriga, M.T.; Ducons, M.; Montero-Marco, J.; Acha, B.; Taboada, A.; Sanz-Burillo, P.; et al. Assessment of humoral immune response to two mRNA SARS-CoV-2 vaccines (Moderna and Pfizer) in healthcare workers fully vaccinated with and without a history of previous infection. J. Appl. Microbiol. 2022, 133, 1969–1974. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 2020, 31, 2603–2615. [Google Scholar] [CrossRef]
- Núñez López, C.; González de Abreu, J.M.; Pérez-Blanco, V.; de Miguel Buckley, R.; Romero Gómez, M.P.; Díaz-Menéndez, M. La Paz Health Care Workers Vaccination Study Group; Appendix. La Paz Health Care Workers Vaccination Study Group. Effectiveness of the BNT162b2 mRNA Covid-19 vaccine in Spanish healthcare workers. Enferm. Infecc. Microbiol. Clin. 2023, 41, 33–35. [Google Scholar] [CrossRef] [PubMed]
- Mestre-Prad, M.T.; Recio-Comí, G.; Molina-Clavero, M.C.; Olona-Cabases, M.M. Reinfection confirmed by SARS-CoV-2 in a healthcare professional detected by an in-hospital infection control program. Enferm. Infecc. Microbiol. Clin. 2023, 41, 50–61. [Google Scholar] [CrossRef] [PubMed]
- Robbiani, D.F.; Gaebler, C.; Muecksch, F.; Lorenzi, J.C.C.; Wang, Z.; Cho, A.; Agudelo, M.; Barnes, C.O.; Gazumyan, A.; Finkin, S.; et al. Convergent antibody responses to SARS-CoV-2 in convalescent individuals. Nature 2020, 584, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef] [PubMed]
- Krammer, F.; Srivastava, K. the PARIS team Simon V. Robust spike antibody responses and increased reactogenicity in seropositive individuals after a 2 single dose of SARS-CoV-2 mRNA vaccine. medRxiv 2021. [CrossRef]
- Krammer, F.; Srivastava, K.; Alshammary, H.; Amoako, A.A.; Awawda, M.H.; Beach, K.F. Antibody responses in seropositive persons after a single dose of SARS-CoV-2 mRNA vaccine. N. Engl. J. Med. 2021, 384, 1372–1374. [Google Scholar] [CrossRef] [PubMed]
- Ren, S.Y.; Wang, W.B.; Gao, R.D.; Zhou, A.M. Omicron variant (B.1.1.529) of SARS-CoV-2: Mutation, infectivity, transmission, and vaccine resistance. World J. Clin. Cases 2022, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanitad. Grupo de Trabajo Técnico de Vacunación COVID-19, Ponencia de Programa y Registro de Vacunaciones de España. Actualización 9 de 2 de Noviembre de 2021. Available online: https://www.sanidad.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/vacunaCovid19.htm (accessed on 25 January 2022).

{kind=link}
{kind=link}
{kind=link}
| IgG ANTI-S1 | |||
|---|---|---|---|
| Patients | Positive | Mean AU/mL (SD) | Range |
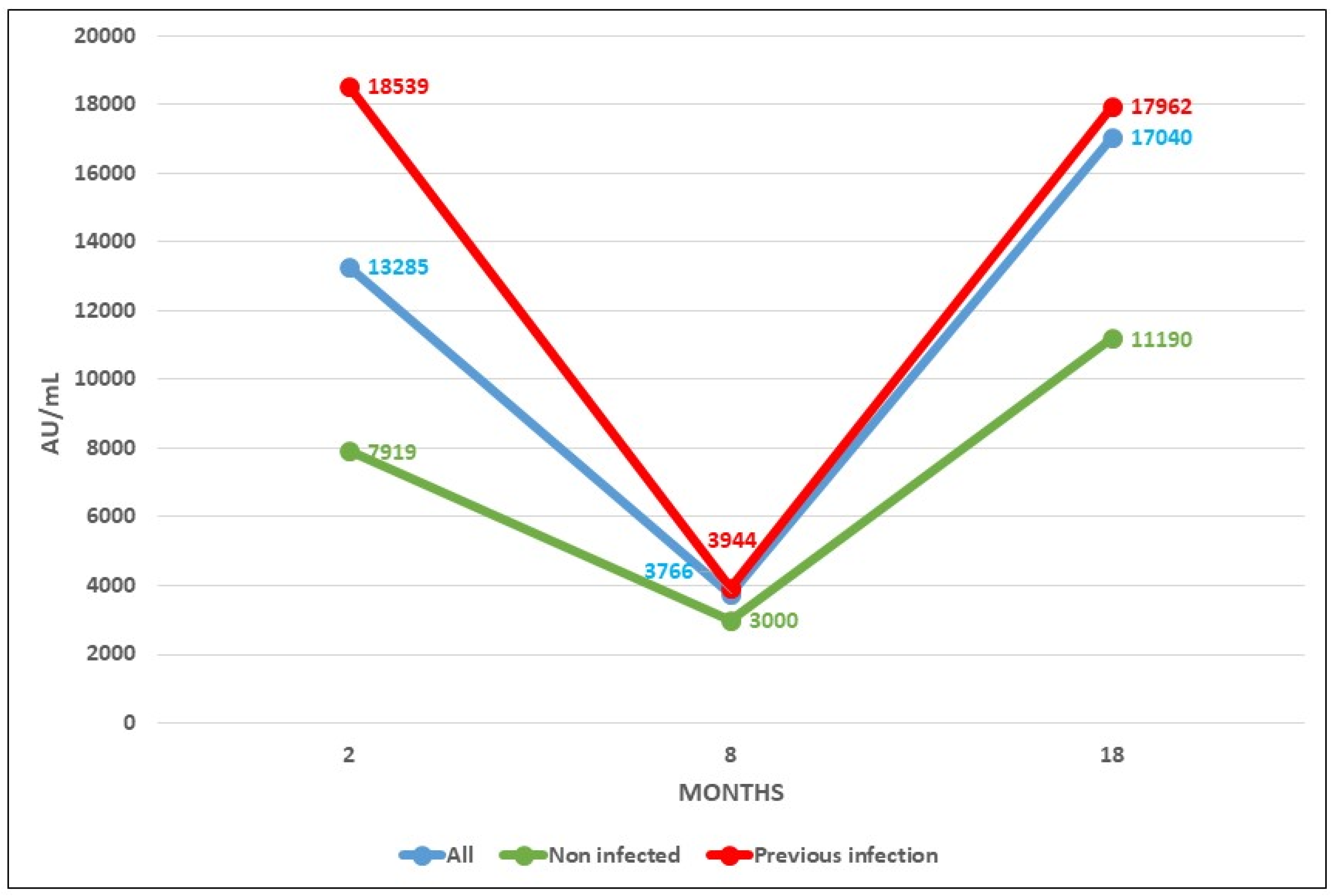
| Total (389) | 389 (100%) | 17,040 (13,413.09) | 483–>40,000 |
| Uninfected (53) | 53 (100%) | 11,190 (11,013.24) | 483–>40,000 |
| Previously infected (336) | 336 (100%) | 17,962 (13,538.07) | 969–>40,000 |
| IgG Anti-S1 | |||
|---|---|---|---|
| Patients | Dose 1st2nd3rd | Mean AU/mL (SD) | Range |
| 15 | MMM | 12,084 (10,307.99) | 919–>40,000 |
| 34 | PPM | 11,502 (11,804.34) | 1291–>40,000 |
| 4 | PPP | 5180 (4528.49) | 483–9933 |
| Sex (%) Mean Age (SD) [Range] | Previous Infection | |
|---|---|---|
| Yes | No | |
| 55 male (14.14%) 46.34 (12.02) [22–65] | 51 (13.11%) | 4 (1.03%) |
| 334 female (85.86%) 48.12 (11.16) [24–65] | 285 (73.26%) | 49 (12.60%) |
| Dose 1st2nd3rd | No. of Patients | Mean AU/mL (SD) [Range] | Sex (M/F) |
|---|---|---|---|
| MMM | 15 | 52.66 (10.21) [29–60] | 0/15 |
| PPM | 34 | 53.74 (7.79) [35–55] | 3/31 |
| PPP | 4 | 61.5 (3.69) [55–64] | 1/3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Algarate, S.; Serrano, L.; Bueno, J.; Herrero-Cortina, B.; Alvarado, E.; González-Barriga, M.T.; Ducons, M.; Montero-Marco, J.; Arnal, S.; Acha, B.; et al. Persistence of Anti-S1 IgG against SARS-CoV-2 Eight Months after the Booster Dose of Vaccine in Naive and Previously Infected Healthcare Workers. Int. J. Mol. Sci. 2023, 24, 10713. https://doi.org/10.3390/ijms241310713
Algarate S, Serrano L, Bueno J, Herrero-Cortina B, Alvarado E, González-Barriga MT, Ducons M, Montero-Marco J, Arnal S, Acha B, et al. Persistence of Anti-S1 IgG against SARS-CoV-2 Eight Months after the Booster Dose of Vaccine in Naive and Previously Infected Healthcare Workers. International Journal of Molecular Sciences. 2023; 24(13):10713. https://doi.org/10.3390/ijms241310713
Chicago/Turabian StyleAlgarate, Sonia, Laura Serrano, Jessica Bueno, Beatriz Herrero-Cortina, Elena Alvarado, María T. González-Barriga, María Ducons, Jesica Montero-Marco, Sara Arnal, Beatriz Acha, and et al. 2023. "Persistence of Anti-S1 IgG against SARS-CoV-2 Eight Months after the Booster Dose of Vaccine in Naive and Previously Infected Healthcare Workers" International Journal of Molecular Sciences 24, no. 13: 10713. https://doi.org/10.3390/ijms241310713
APA StyleAlgarate, S., Serrano, L., Bueno, J., Herrero-Cortina, B., Alvarado, E., González-Barriga, M. T., Ducons, M., Montero-Marco, J., Arnal, S., Acha, B., Riesgo, M., Taboada, A., Sanz-Burillo, P., Yuste, C., Benito, R., & on behalf of the RIPOVAC Study Group. (2023). Persistence of Anti-S1 IgG against SARS-CoV-2 Eight Months after the Booster Dose of Vaccine in Naive and Previously Infected Healthcare Workers. International Journal of Molecular Sciences, 24(13), 10713. https://doi.org/10.3390/ijms241310713