
Translocator Protein Modulation by 4′-Chlorodiazepam and NO Synthase Inhibition Affect Cardiac Oxidative Stress, Cardiometabolic and Inflammatory Markers in Isoprenaline-Induced Rat Myocardial Infarction

 ,
,  ,
,  ,
, 
 , and
, and 
Abstract
1. Introduction
2. Results
2.1. Induction of Acute MI
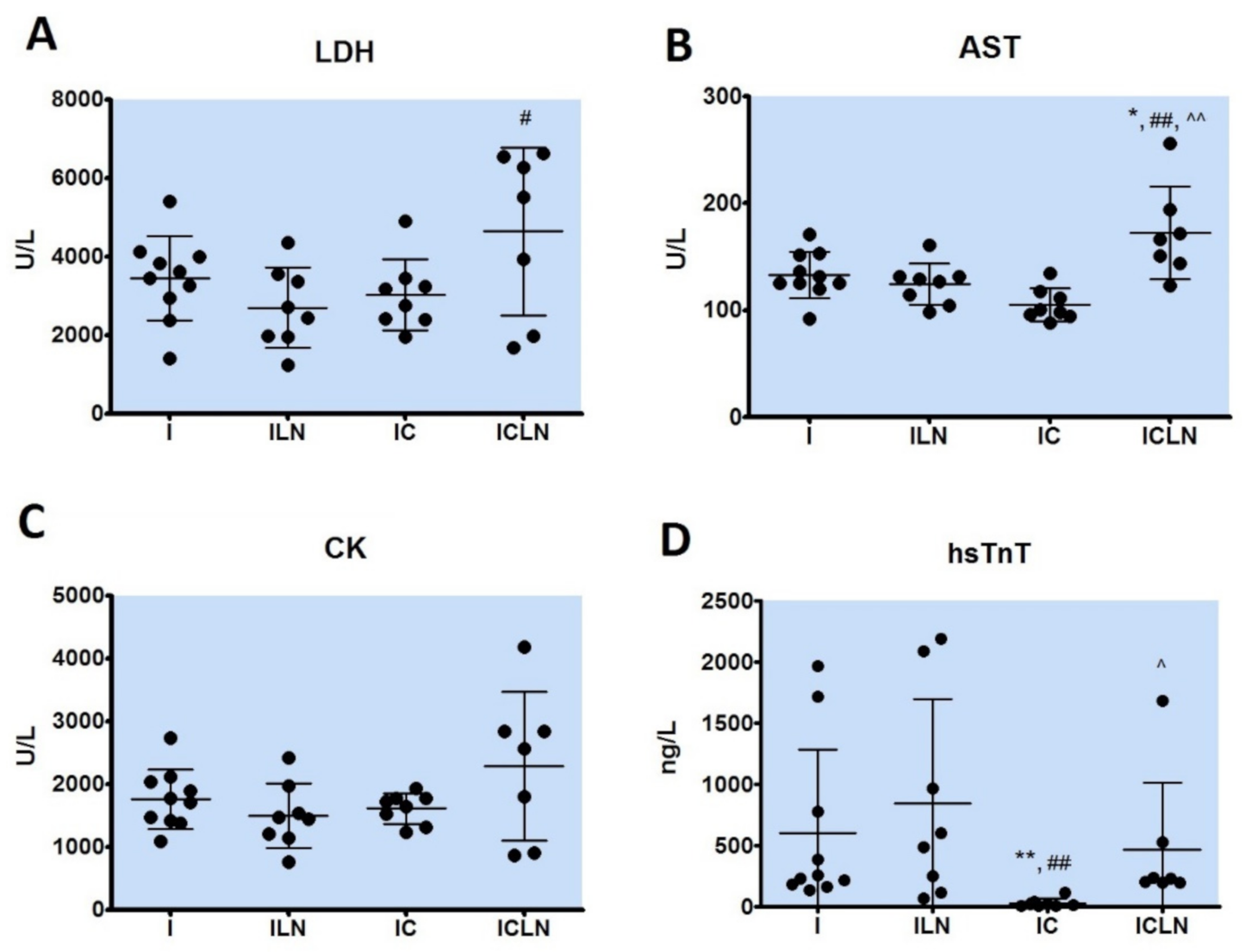
2.2. Cardiac Ischemic Biomarkers
2.3. Biochemical Parameters in Serum or Plasma
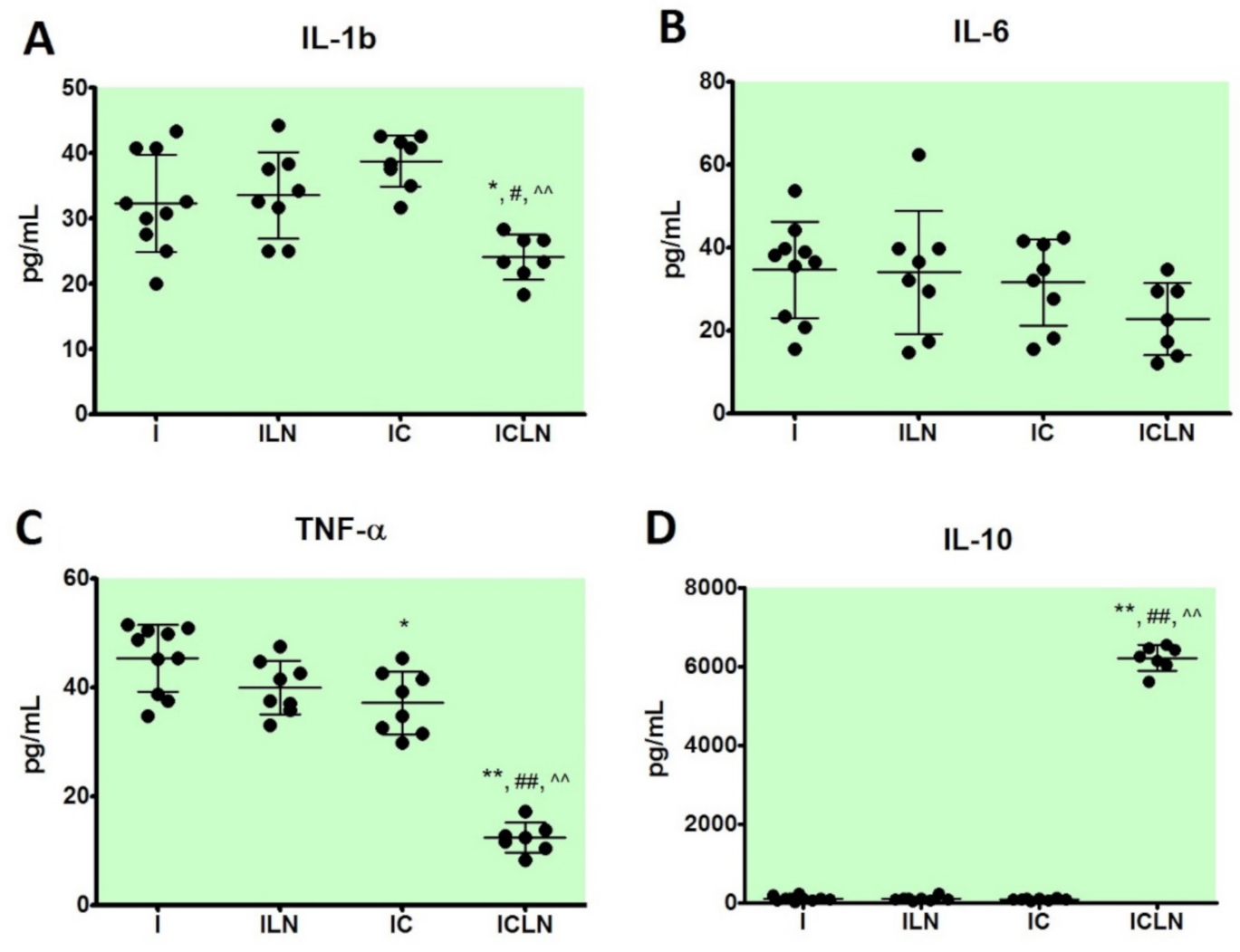
2.4. Cytokine Levels in Serum
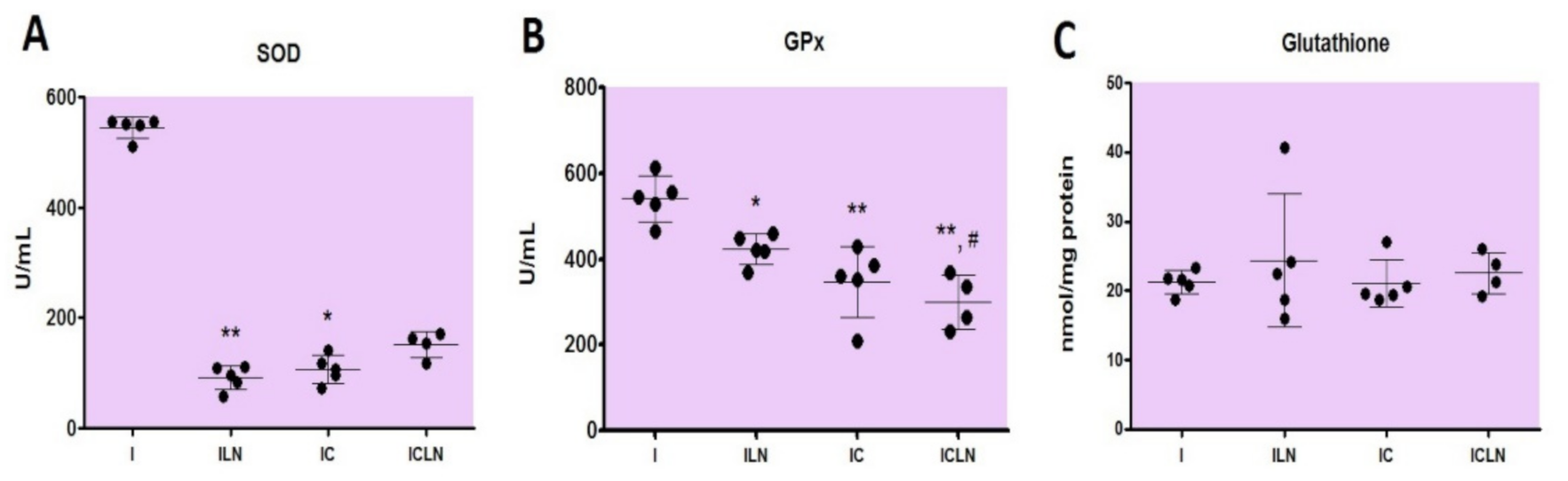
2.5. Oxidative Stress Parameters
2.6. Histopathological Analysis
3. Discussion
4. Materials and Methods
4.1. Animal Ethics Statement
4.2. Experimental Animals
4.3. Experimental Protocol
4.4. Biochemical Parameters Determination in Serum or Plasma
4.5. Cytokine Levels Determination in Serum
4.6. Oxidative Stress Measurements and Preparation of the Cardiac Tissue Samples
4.7. Histopathological Analysis
4.8. Drugs
4.9. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abdallah, M.H.; Arnaout, S.; Karrowni, W.; Dakik, H.A. The management of acute myocardial infarction in developing countries. Int. J. Cardiol. 2006, 111, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Frangogiannis, N.G. Pathophysiology of Myocardial Infarction. Compr. Physiol. 2015, 5, 1841–1875. [Google Scholar] [CrossRef]
- Ithayarasi, A.P.; Devi, C.S. Effect of alpha-tocopherol on lipid peroxidation in isoproterenol induced myocardial infarction in rats. Indian J. Physiol. Pharmacol. 1997, 41, 369–376. [Google Scholar] [PubMed]
- Wexler, B.C. Myocardial infarction in young vs old male rats: Pathophysiologic changes. Am. Heart J. 1978, 96, 70–80. [Google Scholar] [CrossRef]
- Casellas, P.; Galiegue, S.; Basile, A.S. Peripheral benzodiazepine receptors and mitochondrial function. Neurochem. Int. 2002, 40, 475–486. [Google Scholar] [CrossRef]
- McEnery, M.W.; Snowman, A.M.; Trifiletti, R.R.; Snyder, S.H. Isolation of the mitochondrial benzodiazepine receptor: Association with the voltage-dependent anion channel and the adenine nucleotide carrier. Proc. Natl. Acad. Sci. USA 1992, 89, 3170–3174. [Google Scholar] [CrossRef]
- Anholt, R.R.; Pedersen, P.L.; De Souza, E.B.; Snyder, S.H. The peripheral-type benzodiazepine receptor. Localization to the mitochondrial outer membrane. J. Biol. Chem. 1986, 261, 576–583. [Google Scholar] [CrossRef]
- Morin, D.; Musman, J.; Pons, S.; Berdeaux, A.; Ghaleh, B. Mitochondrial translocator protein (TSPO): From physiology to cardioprotection. Biochem. Pharmacol. 2016, 105, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Rupprecht, R.; Papadopoulos, V.; Rammes, G.; Baghai, T.C.; Fan, J.; Akula, N.; Groyer, G.; Adams, D.; Schumacher, M. Translocator protein (18 kDa) (TSPO) as a therapeutic target for neurological and psychiatric disorders. Nat. Rev. Drug Discov. 2010, 9, 971–988. [Google Scholar] [CrossRef]
- Zorov, D.B.; Juhaszova, M.; Yaniv, Y.; Nuss, H.B.; Wang, S.; Sollott, S.J. Regulation and pharmacology of the mitochondrial permeability transition pore. Cardiovasc. Res. 2009, 83, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Liang, D.; Zhang, H.; Liu, Y.; Li, F.; Chen, Y.-H. 4′-Chlorodiazepam, a translocator protein (18 kDa) antagonist, improves cardiac functional recovery during postischemia reperfusion in rats. Exp. Biol. Med. 2010, 235, 478–486. [Google Scholar] [CrossRef] [PubMed]
- Dhalla, N.S.; Yates, J.C.; Lee, S.L.; Singh, A. Functional and subcellular changes in the isolated rat heart perfused with oxidized isoproterenol. J. Mol. Cell. Cardiol. 1978, 10, 31–34. [Google Scholar] [CrossRef]
- Jin, S.; Teng, X.; Xiao, L.; Xue, H.; Guo, Q.; Duan, X.; Chen, Y.; Wu, Y. Hydrogen sulfide ameliorated L-NAME-induced hypertensive heart disease by the Akt/eNOS/NO pathway. Exp. Biol. Med. 2017, 242, 1831–1841. [Google Scholar] [CrossRef]
- Liu, J.-L.; Zucker, I.H. Regulation of Sympathetic Nerve Activity in Heart Failure: A role for nitric oxide and angiotensin II. Circ. Res. 1999, 84, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Cotter, G.; Moshkovitz, Y.; Milovanov, O.; Salah, A.; Blatt, A.; Krakover, R.; Vered, Z.; Kaluski, E. Acute heart failure: A novel approach to its pathogenesis and treatment. Eur. J. Heart Fail. 2002, 4, 227–234. [Google Scholar] [CrossRef]
- Williams, S.; Cooke, G.; Wright, D.; Parsons, W.; Riley, R.; Marshall, P.; Tan, L.-B. Peak exercise cardiac power output; a direct indicator of cardiac function strongly predictive of prognosis in chronic heart failure. Eur. Heart J. 2001, 22, 1496–1503. [Google Scholar] [CrossRef]
- Rajadurai, M.; Prince, P.S.M. Preventive effect of naringin on lipid peroxides and antioxidants in isoproterenol-induced cardiotoxicity in Wistar rats: Biochemical and histopathological evidences. Toxicology 2006, 228, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Halestrap, A.P.; McStay, G.P.; Clarke, S.J. The permeability transition pore complex: Another view. Biochimie 2002, 84, 153–166. [Google Scholar] [CrossRef]
- Qi, X.; Xu, J.; Wang, F.; Xiao, J. Translocator Protein (18 kDa): A Promising Therapeutic Target and Diagnostic Tool for Cardiovascular Diseases. Oxid. Med. Cell. Longev. 2012, 2012, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Upaganlawa, A.; Gandhi, H.; Balaraman, R. Isoproterenol Induced Myocardial Infarction: Protective Role of Natural Products. J. Pharmacol. Toxicol. 2010, 6, 1–17. [Google Scholar] [CrossRef]
- Huang, H.; Geng, Q.; Yao, H.; Shen, Z.; Wu, Z.; Miao, X.; Shi, P. Protective effect of scutellarin on myocardial infarction induced by isoprenaline in rats. Iran J. Basic Med. Sci. 2018, 21, 267–276. [Google Scholar] [PubMed]
- Saravanan, G.; Ponmurugan, P.; Sathiyavathi, M.; Vadivukkarasi, S.; Sengottuvelu, S. Cardioprotective activity of Amaranthus viridis Linn: Effect on serum marker enzymes, cardiac troponin and antioxidant system in experimental myocardial infarcted rats. Int. J. Cardiol. 2013, 165, 494–498. [Google Scholar] [CrossRef] [PubMed]
- Hammerschmidt, S.; Bell, M.; Büchler, N.; Wahn, H.; Remkes, H.; Lohse, M.J.; Neubauer, S. Acute changes of myocardial creatine kinase gene expression under β-adrenergic stimulation. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2000, 1502, 471–480. [Google Scholar] [CrossRef]
- Li, J.-Y.; Wang, J.-K.; Zeng, Y.-M. Peripheral benzodiazepine receptor agonist Ro5-4864 inhibits mitochondrial permeability transition in rat heart. Sheng Li Xue Bao 2007, 59, 13–18. [Google Scholar]
- Senaratne, M.P.; Griffiths, J.; Nagendran, J. Elevation of plasma homocysteine levels associated with acute myocardial infarction. Clin. Investig. Med. 2000, 23, 220–226. [Google Scholar]
- Hagar, H.H. Folic acid and vitamin B12 supplementation attenuates isoprenaline-induced myocardial infarction in experimental hyperhomocysteinemic rats. Pharmacol. Res. 2002, 46, 213–219. [Google Scholar] [CrossRef]
- Kannan, M.M.; Quine, S.D. Ellagic acid ameliorates isoproterenol induced oxidative stress: Evidence from electrocardiological, biochemical and histological study. Eur. J. Pharmacol. 2011, 659, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Woo, K.; Chook, P.; Lolin, Y.; Cheung, A.; Chan, L.; Sun, Y.; Sanderson, J.; Metreweli, C.; Celermajer, D. Hyperhomocyst(e)inemia Is a Risk Factor for Arterial Endothelial Dysfunction in Humans. Circulation 1997, 96, 2542–2544. [Google Scholar] [CrossRef] [PubMed]
- Stamler, J.S.; Osborne, J.A.; Jaraki, O.; Rabbani, L.E.; Mullins, M.; Singel, D.; Loscalzo, J. Adverse vascular effects of homocysteine are modulated by endothelium-derived relaxing factor and related oxides of nitrogen. J. Clin. Investig. 1993, 91, 308–318. [Google Scholar] [CrossRef]
- Sugino, H.; Shimada, H. Effect of isoproterenol on renal uric acid excretion in rats. Jpn. J. Pharmacol. 1987, 45, 343–348. [Google Scholar] [CrossRef]
- Upaganlawar, A.; Patel, V.; Aman, U. Tomato lycopene attenuates myocardial infarction induced by isoproterenol: Electrocardiographic, biochemical and anti–apoptotic study. Asian Pac. J. Trop. Biomed. 2012, 2, 345–351. [Google Scholar] [CrossRef]
- Khalil, I.; Ahmmed, I.; Ahmed, R.; Tanvir, E.M.; Afroz, R.; Paul, S.; Gan, S.H.; Alam, N. Amelioration of Isoproterenol-Induced Oxidative Damage in Rat Myocardium byWithania somniferaLeaf Extract. BioMed Res. Int. 2015, 2015, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kareem, M.; Krushna, G.; Hussain, S.; Devi, K. Effect of Aqueous Extract of Nutmeg on Hyperglycaemia, Hyperlipidaemia and Cardiac Histology Associated with Isoproterenol-induced Myocardial Infarction in Rats. Trop. J. Pharm. Res. 2009, 8, 337–344. [Google Scholar] [CrossRef]
- Graham, A. Mitochondrial regulation of macrophage cholesterol homeostasis. Free. Radic. Biol. Med. 2015, 89, 982–992. [Google Scholar] [CrossRef] [PubMed]
- Kurian, G.A.; Philip, S.; Varghese, T. Effect of aqueous extract of the Desmodium gangeticum DC root in the severity of myocardial infarction. J. Ethnopharmacol. 2005, 97, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.-S.; Chen, W.-L.; Chang, H.-Y.; Kuo, H.-Y.; Chang, Y.-C.; Chu, H. Diagnostic Performance of Initial Salivary Alpha-Amylase Activity for Acute Myocardial Infarction in Patients with Acute Chest Pain. J. Emerg. Med. 2012, 43, 553–560. [Google Scholar] [CrossRef]
- Peyvandi, F.; Garagiola, I.; Baronciani, L. Role of von Willebrand factor in the haemostasis. High Speed Blood Transfus. Equip. 2011, 9, s3–s8. [Google Scholar]
- Wilhelmsen, L.; Svärdsudd, K.; Korsan-Bengtsen, K.; Larsson, B.; Welin, L.; Tibblin, G. Fibrinogen as a Risk Factor for Stroke and Myocardial Infarction. N. Engl. J. Med. 1984, 311, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Danesh, J.; Lewington, S.; Thompson, S.G.; Lowe, G.D.O.; Collins, R.N.; Kostis, J.B.; Wilson, A.C.; Folsom, A.R.; Wu, K.; Benderly, M.; et al. Plasma Fibrinogen Level and the Risk of Major Cardiovascular Diseases and Nonvascular Mortality. JAMA 2005, 294, 1799–1809. [Google Scholar] [CrossRef]
- Ghazouani, L.; Khdhiri, E.; Elmufti, A.; Feriani, A.; Tir, M.; Baaziz, I.; Hajji, R.; Ben Mansour, H.; Ammar, H.; Abid, S.; et al. Cardioprotective effects of (E)-4-hydroxy-N′-(1-(3-oxo-3H-benzo[f]chromen-2-yl)ethylidene)benzohydrazide: A newly synthesized coumarin hydrazone against isoproterenol-induced myocardial infarction in a rat model. Can. J. Physiol. Pharmacol. 2019, 97, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Moreno, H.; Metze, K.; Bento, A.C.; Antunes, E.; Zatz, R.; Nucci, G. Chronic nitric oxide inhibition as a model of hypertensive heart muscle disease. Basic Res. Cardiol. 1996, 91, 248–255. [Google Scholar] [CrossRef]
- Liu, P.; Xu, B.; Forman, L.J.; Carsia, R.; Hock, C.E. L-Name Enhances Microcirculatory Congestion and Cardiomyocyte Apoptosis During Myocardial Ischemia-Reperfusion in Rats. Shock 2002, 17, 185–192. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Radomski, M.W.; Palmer, R.M.; Moncada, S. An L-arginine/nitric oxide pathway present in human platelets regulates aggregation. Proc. Natl. Acad. Sci. USA 1990, 87, 5193–5197. [Google Scholar] [CrossRef] [PubMed]
- Nian, M.; Lee, P.; Khaper, N.; Liu, P. Inflammatory Cytokines and Postmyocardial Infarction Remodeling. Circ. Res. 2004, 94, 1543–1553. [Google Scholar] [CrossRef]
- Mann, D.L. Stress activated cytokines and the heart. Cytokine Growth Factor Rev. 1996, 7, 341–354. [Google Scholar] [CrossRef]
- Seta, Y.; Shan, K.; Bozkurt, B.; Oral, H.; Mann, D.L. Basic mechanisms in heart failure: The cytokine hypothesis. J. Card. Fail. 1996, 2, 243–249. [Google Scholar] [CrossRef]
- Dinarello, C.A. Proinflammatory Cytokines. Chest 2000, 118, 503–508. [Google Scholar] [CrossRef]
- Stumpf, C.; Petzi, S.; Seybold, K.; Wasmeier, G.; Arnold, M.; Raaz, D.; Yilmaz, A.; Daniel, W.G.; Garlichs, C.D. Atorvastatin enhances interleukin-10 levels and improves cardiac function in rats after acute myocardial infarction. Clin. Sci. 2008, 116, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Frangogiannis, N.G.; Mendoza, L.H.; Lindsey, M.L.; Ballantyne, C.M.; Michael, L.H.; Smith, C.W.; Entman, M.L. IL-10 Is Induced in the Reperfused Myocardium and May Modulate the Reaction to Injury. J. Immunol. 2000, 165, 2798–2808. [Google Scholar] [CrossRef]
- Fujimura, Y.; Hwang, P.M.; Iii, H.T.; Kozloff, L.; Imaizumi, M.; Innis, R.B.; Fujita, M. Increased peripheral benzodiazepine receptors in arterial plaque of patients with atherosclerosis: An autoradiographic study with [3H]PK 11195. Atherosclerosis 2008, 201, 108–111. [Google Scholar] [CrossRef]
- Park, J.-G.; Oh, G.-T. The role of peroxidases in the pathogenesis of atherosclerosis. BMB Rep. 2011, 44, 497–505. [Google Scholar] [CrossRef]
- Bird, J.; Izquierdo-Garcia, D.; Davies, J.; Rudd, J.; Probst, K.; Figg, N.; Clark, J.; Weissberg, P.; Davenport, A.; Warburton, E. Evaluation of translocator protein quantification as a tool for characterising macrophage burden in human carotid atherosclerosis. Atherosclerosis 2010, 210, 388–391. [Google Scholar] [CrossRef] [PubMed]
- Laitinen, I.; Marjamäki, P.; Någren, K.; Laine, V.J.O.; Wilson, I.; Leppänen, P.; Ylä-Herttuala, S.; Roivainen, A.; Knuuti, J. Uptake of inflammatory cell marker [11C]PK11195 into mouse atherosclerotic plaques. Eur. J. Nucl. Med. Mol. Imaging 2008, 36, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Gaemperli, O.; Shalhoub, J.; Owen, D.R.; Lamare, F.; Johansson, S.; Fouladi, N.; Davies, A.H.; Rimoldi, O.E.; Camici, P.G. Imaging intraplaque inflammation in carotid atherosclerosis with 11C-PK11195 positron emission tomography/computed tomography. Eur. Heart J. 2012, 33, 1902–1910. [Google Scholar] [CrossRef]
- Tsutsui, H.; Kinugawa, S.; Matsushima, S. Mitochondrial oxidative stress and dysfunction in myocardial remodelling. Cardiovasc. Res. 2008, 81, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Maulik, S.K.; Kumar, S. Oxidative stress and cardiac hypertrophy: A review. Toxicol. Mech. Methods 2012, 22, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.-X.; Kimura, S.; Nishiyama, A.; Shokoji, T.; Rahman, M.; Yao, L.; Nagai, Y.; Fujisawa, Y.; Miyatake, A.; Abe, Y. Cardiac oxidative stress in acute and chronic isoproterenol-infused rats. Cardiovasc. Res. 2005, 65, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Bagatini, M.D.; Martins, C.C.; Battisti, V.; Gasparetto, D.; Da Rosa, C.S.; Spanevello, R.M.; Ahmed, M.; Schmatz, R.; Schetinger, M.R.C.; Morsch, V.M. Oxidative stress versus antioxidant defenses in patients with acute myocardial infarction. Heart Vessel. 2010, 26, 55–63. [Google Scholar] [CrossRef]
- Dalle-Donne, I.; Rossi, R.; Giustarini, D.; Milzani, A.; Colombo, R. Protein carbonyl groups as biomarkers of oxidative stress. Clin. Chim. Acta 2003, 329, 23–38. [Google Scholar] [CrossRef]
- Lazzarino, G.; Raatikainen, P.; Nuutinen, M.; Nissinen, J.; Tavazzi, B.; Di Pierro, D.; Giardina, B.; Peuhkurinen, K. Myocardial release of malondialdehyde and purine compounds during coronary bypass surgery. Circulation 1994, 90, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, A.; Kumar, S.; Enjamoori, R.; Seth, S.; Dinda, A.K.; Maulik, S.K. Peripheral benzodiazepine receptor ligand Ro5-4864 inhibits isoprenaline-induced cardiac hypertrophy in rats. Eur. J. Pharmacol. 2010, 644, 146–153. [Google Scholar] [CrossRef]
- Dhalla, N.S.; Elmoselhi, A.B.; Hata, T.; Makino, N. Status of myocardial antioxidants in ischemia–reperfusion injury. Cardiovasc. Res. 2000, 47, 446–456. [Google Scholar] [CrossRef]
- Kumar, M.; Kasala, E.R.; Bodduluru, L.N.; Dahiya, V.; Lahkar, M. Baicalein protects isoproterenol induced myocardial ischemic injury in male Wistar rats by mitigating oxidative stress and inflammation. Inflamm. Res. 2016, 65, 613–622. [Google Scholar] [CrossRef]
- Nikolic-Heitzler, V.; Rabuzin, F.; Tatzber, F.; Vrkic, N.; Bulj, N.; Borovic, S.; Wonisch, W.; Sunko, B.M.; Zarkovic, N. Persistent Oxidative Stress after Myocardial Infarction Treated by Percutaneous Coronary Intervention. Tohoku J. Exp. Med. 2006, 210, 247–255. [Google Scholar] [CrossRef]
- Weinbrenner, T.; Cladellas, M.; Covas, M.I.; Fitó, M.; Tomás, M.; Sentí, M.; Bruguera, J.; Marrugat, J. High oxidative stress in patients with stable coronary heart disease. Atherosclerosis 2003, 168, 99–106. [Google Scholar] [CrossRef]
- Hemalatha, K.L.; Prince, P.S.M. Preventive effects of zingerone on cardiac mitochondrial oxidative stress, calcium ion overload and adenosine triphosphate depletion in isoproterenol induced myocardial infarcted rats. RSC Adv. 2016, 6, 112332–112339. [Google Scholar] [CrossRef]
- Brown, D.A.; Aon, M.A.; Frasier, C.R.; Sloan, R.C.; Maloney, A.H.; Anderson, E.J.; O’Rourke, B. Cardiac arrhythmias induced by glutathione oxidation can be inhibited by preventing mitochondrial depolarization. J. Mol. Cell. Cardiol. 2010, 48, 673–679. [Google Scholar] [CrossRef]
- Filho, H.G.L.; Ferreira, N.L.; De Sousa, R.B.; De Carvalho, E.R.; Lobo, P.L.D.; Filho, J.G.L. Modelo experimental de infarto do miocárdio induzido por isoproterenol em ratos. Braz. J. Cardiovasc. Surg. 2011, 26, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.-T.; Gong, Y.; Zhou, B.; Yang, J.-J.; Cheng, Y.; Zhao, J.-G.; Qi, M.-Y. Ursolic acid ameliorates oxidative stress, inflammation and fibrosis in diabetic cardiomyopathy rats. Biomed. Pharmacother. 2018, 97, 1461–1467. [Google Scholar] [CrossRef] [PubMed]
- Misra, H.P.; Fridovich, I. The Role of Superoxide Anion in the Autoxidation of Epinephrine and a Simple Assay for Superoxide Dismutase. J. Biol. Chem. 1972, 247, 3170–3175. [Google Scholar] [CrossRef]
- Günzler, W.A.; Kremers, H.; Flohé, L. An Improved Coupled Test Procedure for Glutathione Peroxidase (EC 1.11.1.9.) in Blood. Clin. Chem. Lab. Med. 1974, 12, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Ravindranath, V. Animal models and molecular markers for cerebral ischemia-reperfusion injury in brain. Cellulases 1994, 233, 610–619. [Google Scholar] [CrossRef]
- Bertinchant, J.P.; Robert, E.; Polge, A.; Marty-Double, C.; Fabbro-Peray, P.; Poirey, S.; Aya, G.; Juan, J.M.; Ledermann, B.; De La Coussaye, J.E.; et al. Comparison of the diagnostic value of cardiac troponin I and T determinations for detecting early myocardial damage and the relationship with histological findings after isoprenaline-induced cardiac injury in rats. Clin. Chim. Acta 2000, 298, 13–28. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| I | ILN | IC | ICLN | |
|---|---|---|---|---|
| Hcy (μmol/L) | 26.93 (23.52–29.39) | 28.6 (22.10–33.61) | 13.63 (8.47–18.29) ** | 18.94 (15.67–31.63) ^ |
| UA (μmol/L) | 66.5 (56.0–72.0) | 63.5 (60.2–68.2) | 70.5 (65.5–84.5) | 90.0 (80.0–97.5) **, ##, ^ |
| UREA (mmol/L) | 10.0 (9.4–10.5) | 9.9 (7.2–9.0) | 7.7 (7.2–9.0) ** | 9.8 (8.6–13.6) ^^ |
| CREA (μmol/L) | 27.5 (26.7–30.2) | 24.5 (21.0–27.2) | 17.0 (15.7–21.0) ** | 42.0 (37.5–46.7) **, ##, ^^ |
| TC (mmol/L) | 1.7 (1.5–1.9) | 1.9 (1.8–2.1) * | 1.6 (1.3–2.1) | 2.2 (2.1–2.6) **, #, ^ |
| HDL-C (mmol/L) | 1.0 (0.9–1.1) | 1.2 (1.0–1.3) | 0.9 (0.8–1.4) | 0.6 (0.6–0.7) **, ##, ^^ |
| TG (mmol/L) | 0.37 (0.32–0.45) | 0.43 (0.37–0.55) | 0.48 (0.44–0.48) ** | 0.47 (0.38–0.80) * |
| ALT (U/L) | 39.1 (36.4–43.1) | 61.5 (53.2–81.8) ** | 53.9 (47.1–60.6) ** | 84.0 (75.0–132.0) **, #, ^^ |
| ALP (U/L) | 167.0 (159.5–178.0) | 192.5 (125.5–210.8) | 209.0 (172.5–242.3) * | 258.5 (224.3–279.3) **, ##, ^ |
| α-AMY (U/L) | 1986 (1773–2546) | 3094 (2343–3476) * | 3677 (2082–4898) * | 1077 (762–1493) **, ##, ^^ |
| TP (g/L) | 48.1 (46.7–50.5) | 49.0 (47.4–51.2) | 45.5 (44.3–51.2) | 46.0 (45.0–48.0) *, # |
| ALB (g/L) | 31.7 (30.7–32.4) | 32.9 (31.0–35.2) | 32.7 (29.9–34.2) | 22.0 (22.0–23.0) **, ##, ^^ |
| FIB (g/L) | 3.1 (2.6–3.5) | 2.4 (2.2–3.3) | 3.1 (2.8–3.5) | 2.3 (2.2–2.5) **, ^^ |
| vWF (%) | 212.5 (114.9–228.6) | 217.3 (205.1–242.8) | 201.8 (190.0–219.3) | 247.1 (238.1–310.7) **, #, ^^ |
| Grade 0 | Grade 1 | Grade 2 | Grade 3 | Σ | |
|---|---|---|---|---|---|
| I | 0 (0%) | 0 (0%) | 1 (20%) | 4 (80%) | 5 (100%) |
| ILN | 0 (0%) | 0 (0%) | 3 (75%) | 1 (25%) | 4 (100%) |
| IC * | 4 (80%) | 1 (20%) | 0 (0%) | 0 (0%) | 5 (100%) |
| ICLN ^ | 0 (0%) | 0 (0%) | 2 (50%) | 2 (50%) | 4 (100%) |
| Σ | 4 (22.2%) | 1 (5.6%) | 6 (33.3%) | 7 (38.9%) | 18 (100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilic, A.; Todorovic, D.; Mutavdzin, S.; Boricic, N.; Bozic Nedeljkovic, B.; Stankovic, S.; Simic, T.; Stevanovic, P.; Celic, V.; Djuric, D. Translocator Protein Modulation by 4′-Chlorodiazepam and NO Synthase Inhibition Affect Cardiac Oxidative Stress, Cardiometabolic and Inflammatory Markers in Isoprenaline-Induced Rat Myocardial Infarction. Int. J. Mol. Sci. 2021, 22, 2867. https://doi.org/10.3390/ijms22062867
Ilic A, Todorovic D, Mutavdzin S, Boricic N, Bozic Nedeljkovic B, Stankovic S, Simic T, Stevanovic P, Celic V, Djuric D. Translocator Protein Modulation by 4′-Chlorodiazepam and NO Synthase Inhibition Affect Cardiac Oxidative Stress, Cardiometabolic and Inflammatory Markers in Isoprenaline-Induced Rat Myocardial Infarction. International Journal of Molecular Sciences. 2021; 22(6):2867. https://doi.org/10.3390/ijms22062867
Chicago/Turabian StyleIlic, Ana, Dusan Todorovic, Slavica Mutavdzin, Novica Boricic, Biljana Bozic Nedeljkovic, Sanja Stankovic, Tatjana Simic, Predrag Stevanovic, Vera Celic, and Dragan Djuric. 2021. "Translocator Protein Modulation by 4′-Chlorodiazepam and NO Synthase Inhibition Affect Cardiac Oxidative Stress, Cardiometabolic and Inflammatory Markers in Isoprenaline-Induced Rat Myocardial Infarction" International Journal of Molecular Sciences 22, no. 6: 2867. https://doi.org/10.3390/ijms22062867
APA StyleIlic, A., Todorovic, D., Mutavdzin, S., Boricic, N., Bozic Nedeljkovic, B., Stankovic, S., Simic, T., Stevanovic, P., Celic, V., & Djuric, D. (2021). Translocator Protein Modulation by 4′-Chlorodiazepam and NO Synthase Inhibition Affect Cardiac Oxidative Stress, Cardiometabolic and Inflammatory Markers in Isoprenaline-Induced Rat Myocardial Infarction. International Journal of Molecular Sciences, 22(6), 2867. https://doi.org/10.3390/ijms22062867