Abstract
This study aimed to develop an Internet-based psychiatric nursing intervention, based on Swanson’s theory of caring, that could alleviate post-traumatic stress symptoms and improve the health functioning of adults who had experienced trauma. To evaluate the appropriateness and understanding of the program content, expert advice and content validity were examined using the content validity index. To analyze the participants’ responses and evaluate the appropriateness of conducting Internet-based programs, an online intervention program was implemented with five nurses between February and April 2020. The trauma recovery nursing intervention program was for adults who had experienced trauma and consisted of eight sessions, each lasting 30 min. It included a spoken audio track that was accompanied by visual prompts to provide knowledge on traumatic stress and introduce trauma recovery methods. Its online format made it convenient and widely accessible, and allowed for a low-intensity, cost-effective educational program. The program focused on providing self-help guidelines for clients to develop their mental and physical well-being. The results provide evidence that mental health nurses could develop and implement online programs to care for people who have experienced trauma. Such programs could provide trauma recovery for marginalized people unable to otherwise receive help.
1. Introduction
Psychological trauma refers to mental damage that occurs when one’s ability to overcome or integrate is exceeded as the result of a stress-inducing event []. This is a widely occurring phenomenon that affects people regardless of their region, race, educational level, or socioeconomic status. Psychological trauma is deeply connected to the causes of post-traumatic stress disorder (PTSD), anxiety disorder, sleep disorder, behavior disorder, depression, and suicide [,]. Trauma is both a mental health problem and a serious social problem; however, it can be alleviated through prevention and early treatment [,]. However, if treatment and care period are delayed, trauma can progress into a chronic disease and result in a deterioration in quality of life amid the effects of PTSD [,]; thus, a national-level counter strategy must be developed [,].
Among the noninvasive social psychological treatments that are available for trauma patients, cognitive-behavioral therapy has been confirmed as the most effective intervention []. However, immediately after experiencing trauma, many patients with high anxiety struggle to focus during cognitive-behavioral therapy and do not experience relief from their physical symptoms []. Studies have confirmed that exposure therapy is also effective in treating patients with chronic post-traumatic stress symptoms; however, it is a difficult strategy to apply when patients exhibit multiple physical symptoms. Moreover, the lack of trained professional therapists limits nurses’ ability to learn the treatment []. Recently, studies reported that eye movement desensitization and reprocessing (EMDR) has a therapeutic effect in people who have experienced trauma; however, this technique also has high training costs. Additionally, certification requires thoroughly supervised training at the EMDR Society headquarters in the United States and general nurses lack access to the certification programs. Thus, its use is limited []. As such, there is a need for accessible and effective options for the treatment of post-traumatic symptoms. Therefore, the aim of this study was to develop an Internet-based self-help program for adults who have experienced a traumatic event.
1.1. Background
In various countries, professionals from health-care specialized fields are participating in the respective “Trauma Health” fields within their communities and are striving toward competency development [,]. In particular, therapists who care for people experiencing trauma can easily experience burnout; therefore, there is a great need for training programs within this profession []. For this reason, a national-level response strategy that provided a significant amount of support for building a network of experts and the providing human resource training was developed [,].
In Korea, mental health experts (e.g., doctors, nurses, social workers) are mobilized at the “Community Mental Health Welfare Center” []. Mental health experts perform monitoring, evaluation, crisis counseling, and case management necessary for psychological recovery for those who have experienced traumatic events, and vulnerable people in their families and communities over a long period of time immediately after trauma occurrence [].
Trauma recovery requires an integrated approach, from individual psychological and emotional problems to changes in social structure and environment []. However, the lack of an integrated and systematic education program for mental health nurses at the national level has been shown to make trauma therapy difficult, which further promotes psychological burnout of mental health professionals [,].
Many psychiatric nurses still struggle with deviating from the perspective of psychiatric hospital-oriented trauma treatment. Furthermore, decreased interest in the nursing field has led to a serious lack of nursing personnel who have received systematic trauma treatment training [,]. However, in Korea, although social welfare and clinical psychology college majors actively participate in strengthening their capacity for trauma management and treatment, there are few opportunities to engage in trauma treatment training in the nursing field []. Nurses’ lack of competency in trauma intervention is thought to be a contributing factor towards the lack of participation by nurses [].
Previous studies have found that resilience and the ability to cope with stress buffer the negative symptoms associated with trauma experiences and contribute to improving mental health [,]. In addition, guided self-help nursing interventions can assist in the management of various psychiatric conditions, such as depression and anxiety, in patients with PTSD, and help these patients find satisfaction and happiness in life while gaining a deeper understanding of themselves []. Nursing interventions are based on a holistic understanding of human beings; however, interventions that can integrate physical, mental, social, and behavioral interventions within effective therapeutic strategies must still be developed [].
This study used Swanson’s theory of caring [], a middle-range theory, as its theoretical basis. Swanson’s theory of caring was initially developed for parents who experienced fetal miscarriages; however, it has been used in various situations, including for parents of premature babies, and has been used as the theoretical basis for several previous studies []. In addition, researchers have reported that level of care and patient safety improved when Swanson’s theory of caring was used as the theoretical basis for supporting nursing practice in several hospitals in the United States, as did the level of satisfaction in the care provided to patients by nurses []. Swanson’s theory of caring suggests that “client well-being” can be maintained while executing a five-step process: “maintaining belief,” “knowing,” “being with,” “doing for,” and “enabling” []. This process is applicable to both those who have experienced trauma and for the nursing staff.
People often do not receive early professional treatment following traumatic experiences because they are not aware of the negative impact that trauma can have on their mental health. Moreover, patients can present with a wide variety of symptoms, including physical symptoms and sleep disturbances []. Patients may be concerned that they could re-experience trauma during the course of the treatment, and may struggle to connect with the appropriate therapist [,,]. Additionally, face-to-face treatment is time-consuming and expensive, and appropriate services are difficult to provide in isolated places, such as rural areas [,].
When it comes to overcoming these limitations, Internet-based interventions are promising treatment options compared to face-to-face interventions. According to Lewis et al. [], Internet-based interventions require much less time from therapists and clients, and guided psychological interventions are a treatment option that could help broaden access to effective interventions. In their study, the Internet-based intervention group reported significantly lower PTSD, depression, anxiety, and dysfunction scores than the face-to-face intervention group. Based on such previous research, this study aimed to contribute to ease of management and low-cost operation by utilizing popular existing Internet media such as e-mail, video calls, and video lectures.
1.2. Aim
The aim of this study was to develop an Internet-based psychiatric nursing intervention that could alleviate post-traumatic stress symptoms and improve the health functioning of adults who have experienced trauma.
2. Materials and Methods
2.1. Design
This was a methodological research study that developed an Internet-based program based on Swanson’s theory of caring []. The process involved developing the program’s content, and then evaluating its Internet-based implementation. The evaluation was performed using five nurses as a convenience sample who role played as clients for the purposes of developing this intervention. The nurses worked in nonmental health-related areas and had more than three years of nursing experience. The five participating nurses assessed the appropriateness of the program’s online configuration and provided feedback on their experience with the program. The researchers conducted the program in the role of the therapist. The program was run individually online.
2.2. Ethical Considerations
Approval for this study was obtained from the institutional review board of Yonsei University (Y-2019-0083). The participants expressed their intention to voluntarily participate through the recruitment announcement and were provided with a description of the study. This material explained the study’s purpose, potential risks, and benefits. Participants were informed that participation was voluntary and they could withdraw from the study at any time.
2.3. Conceptual Framework
Swanson’s theory of caring is based on the experiences of women who had undergone abortions or given birth to a premature baby []. The theory emphasizes that the focus of nursing is not on human illnesses but on helping patients achieve, maintain, and recover optimal levels of well-being []. In addition, as a middle-range theory, it provides the basis for nursing practice and applies each caring process to nursing. This theory describes five caring processes: “maintaining belief,” “being with,” “knowing,” “doing for,” and “enabling” (Figure 1).
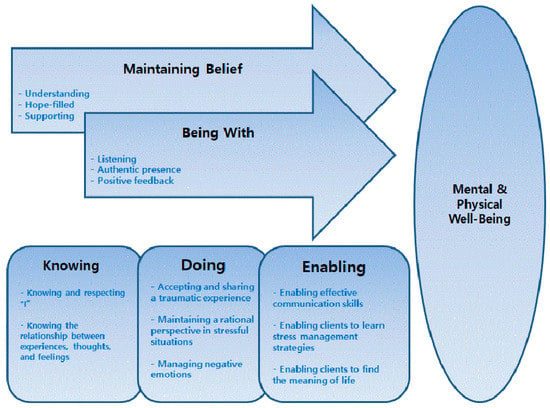
Figure 1.
Conceptual framework for the program.
The concept of “maintaining belief” emphasizes the trust between the client and the nurse. To maintain hope and recovery, clients should help and respect themselves [,]. In this study, the research team used response letters, which aided in developing a strong and deep trust between the therapist and client, that were related to “maintaining belief” from the first to the last session. Therapists aimed to provide an understanding and supportive attitude, as well as hope, in the response letters.
In the “being with” stage, the nurse reports on the necessity behind recognizing the client’s feelings by allowing them space to share their feelings and experiences. One study reported that nurses should communicate clearly with clients and not feel burdened []. In this study, the “being with” aspect of the interaction between the client and therapist was also applied to the response letter through interactive communication. From the response letter, clients could recognize that the therapist was listening to their experiences and feelings. When clients who had experienced trauma were treated by nurses, they found that they were able to accept and respect their existence.
The “knowing” stage aims to develop the client’s understanding of the meaning of the events that have occurred in their lives. From this perspective, the nurse and client try to create knowing and understanding around the human responses to recovery, rather than emphasizing or avoiding traumatic experiences [,]. In this study, “knowing” focused on getting to know and respect the clients themselves: grasping experiences, thoughts, and feelings, and grasping their mutual relationships.
The “doing” stage is characterized by the nurse caring for the client. One study reported that nurses should help maintain client well-being by allowing the nurses to protect and care for clients and by allowing clients to set goals for themselves []. In this study, “doing” emphasized the client’s self-help process by recognizing their traumatic experiences, maintaining rational recognition in stressful situations, and controlling negative emotions.
In the “enabling” stage, nurses allow clients to change their daily routine and solve problems on their own as they encounter new events [,]. In this study, the concept of “enabling” provided the perspective that clients could solve their problems and find meaning in life. To find gratefulness and satisfaction in daily life, clients learned effective communication skills and stress management strategies.
2.4. Program Development Process
2.4.1. Stage I. Program Content Development Process
Based on the theoretical framework and literature review, the research team set the goals, theme, and main content of the intervention program, and determined the duration of the eight-session program. The qualification requirements for the researchers who conducted the program were identified.
To confirm the content for each session, the content that we developed was reviewed, revised, and supplemented by experts on the program draft in paper documents. The experts comprised one trauma counselor at a counseling center and six mental health nurses at mental health services and mental health rehabilitation centers. Experts assessed the effectiveness of each session’s purpose and content using a four-point Likert scale, where 1 = completely inappropriate, 2 = not appropriate, 3 = appropriate, and 4 = very appropriate. The content validity index (CVI) was also calculated.
To evaluate the appropriateness and understanding of the program content, expert advice and the CVI were checked.
The suitability of the overall purpose of the program and the goals for each session were verified. The CVI was 3.2 points (86.1%), thus verifying the content validity of the program. Moreover, the program was modified and supplemented based on the expert advice.
2.4.2. Stage II. Internet-Based Program Execution Process Development Process
Through evaluation of the adequacy of the online program, we analyzed the participants’ responses to the Internet-based eight-session program. We confirmed the corrections and supplementations with the participants to establish their understanding of the composition and content of the program, the difficulty of the vocabulary, and the adequacy of the time provided. The final program was developed by applying the feedback that was received. Table 1 shows the feedback from the participants and the revisions that were made that reflected their feedback. During the evaluation of the feedback, the research team recognized that the participants wanted more active interaction with the therapists. Therefore, the research team developed a response letter for each session. Following the correction and supplementation of the content, and the online application of the program using the method developed from participants’ responses in the evaluation, the program was finalized.

Table 1.
Participant feedback and revisions to the eight-session Internet-based program.
3. Results
We developed a trauma recovery nursing intervention program for adults who have experienced trauma. This Internet-based program consisted of eight 30 min sessions. The program included a spoken-audio track that was accompanied by visual prompts. It aimed to provide knowledge on traumatic stress and introduce methods to recover from trauma. We chose an online format to make it convenient and widely accessible, and to allow for a low-intensity, cost-effective educational program. The theoretical framework for this study was based on Swanson’s theory of caring [] and a literature review of trauma interventions. The specific topics covered in the training program are outlined in Table 2. The detailed content of each session is described below.
Table 2.
The eight-session program.
The Eight-Session Program
First, before the start of the main program, the background and purpose were explained to participants and an overall introduction on how the program would be conducted was provided.
Session 1 emphasized self-understanding and self-respect. Clients had time to understand themselves by remembering things that were either sad or happy and recording them. Clients were provided with information on PTSD, and we confirmed that the clients were not experiencing PTSD without support. In addition, clients were encouraged to determine their undiscovered strengths. They were also encouraged to consider how they could use their strengths in their lives. After Session 1, clients practiced abdominal breathing to calm their minds, which they may have been struggling with due to the task of recalling painful memories.
Session 2 helped clients be more vulnerable than in the first session. Clients thought of people who had hurt them in their lives and faced the negative emotions they felt. To turn their negative emotions into positive ones, they were reminded of the aspects of their life for which they could be grateful. The clients were given information on flashbacks and how to cope with them if they experienced any. After Session 2, the clients practiced gradual muscle relaxation, a type of body stabilization. Body stabilization focuses on physical and emotional sensations, and on the present rather than the past.
Session 3 focused on clients accepting and sharing trauma experiences on their own. Through self-exposure, clients were encouraged to understand and share how the difficult situations that were addressed in the second session affected their feelings, thoughts, and behavior. It helped evoke and discharge negative emotions and thoughts. In addition, clients were trained to control their emotions by turning negative thoughts into positive ones. After Session 3, clients practiced using their imagination. Imagination training calms emotions through the repeated, intermittent flashing of negative events or emotions on a computer screen.
Session 4 highlighted the benefits of maintaining a rational viewpoint in stressful situations. Clients could look at their situation objectively and identified the benefits of rational thinking. Through examples of irrational thoughts (e.g., black and white logic, exaggeration/reduction, mind reading), they recognized that they were often irrational themselves. Clients learned that, through a rational worldview and perspective, they could have positive emotions. After Session 4, body stabilization exercise was performed.
Session 5 emphasized the management of the negative emotions felt by clients who experienced trauma. Clients checked the emotions they often felt to determine whether they experienced positive or negative emotions more frequently. Clients learned the benefits of positive emotions and were trained to distinguish between the thoughts and emotions experienced in certain situations through examples. They were also trained to change their emotions and behaviors by reminding themselves of stressful situations and transforming the emotions and thoughts that they were experiencing at that time into rational thinking. After completing the Session 5, the abdominal breathing exercises were repeated.
Session 6 focused on developing effective communication skills. Clients learned the communication skills required to their express emotions and thoughts and change their behavior. After identifying their communication types and habits, clients shared their difficulties and conflicts related to communication with their therapists via response letters. They also learned to express negative emotions or deal with negative situations using “I-message” language. Through the use of examples of inefficient communication, clients became committed to avoiding inefficient communication. After Session 6, body stabilization exercise was repeated.
Session 7 focused on managing stress and leading a healthy lifestyle. Clients were asked to learn four strategies that would assist with stress management: cognitive control, behavior control, physiological relaxation, and daily life management. Clients identified a situation and planned strategies to reduce stress. In addition, the application of a stress response strategy through identification of automatic thinking and adjustment to alternative and rational thinking was suggested. Finally, clients learned the “butterfly embrace” for physiological relaxation.
In Session 8, clients were empowered to find meaning in their everyday lives. They recognized that they could enjoy a peaceful life by solidifying their strengths and that they could find happiness and meaning in their own lives. Through summarizing the information in Session 1–7, clients could confirm what had changed recently in their daily lives. They were provided with a perspective of gratitude and satisfaction in daily life. Through integration of the “knowing,” “doing for,” and “enabling” topics, clients who had difficult experiences could recover from trauma. At the end of the Session 8, the body stabilization exercise was repeated.
During each of the aforementioned program sessions, the research team sent individual response letters to the clients. The response letter was created based on the evaluation feedback. To ensure mutual communication between the therapist and client, the therapist interacted with the client continuously and fulfilled the “maintaining belief” and “being with” domains for the client. Response letters were provided at the end of each session. Based on the content of the client’s responses throughout the program, we communicated with clients individually to provide support and hope through positive feedback. In addition, we motivated clients to continue participating in the program without giving up. The standardized response letter provided a framework for therapists and we expected that it would improve the service quality. In addition, we provided a guide in the responses to address each client’s individual circumstances or feelings.
4. Discussion
This study developed an Internet-based psychiatric nursing intervention for trauma recovery based on Swanson’s theory of caring [], a middle-range theory that can be applied directly to nursing practice in the mental health field. Swanson’s theory of caring provides a conceptual framework for a therapeutic approach to those suffering from trauma. The program that was developed was constructed based on five key concepts that ultimately aimed to maintain the client’s state of well-being: “maintaining belief”, “knowing”, “being with”, “doing for”, and “enabling”. The concepts were not mutually exclusive, and each concept was incorporated into each session. Thus, they acted as an overlapping process and influenced and interacted with each other. Swanson’s theory of caring is considered both incredibly relevant and applicable to the field of nursing practice with respect to the views that it presents of humans and the relationship between therapist and client [,]. The program that was developed in this study did not provide symptom-oriented interventions that only focused on traumatic events or experiences from the therapist’s professional standpoint. We focused on providing a self-help guideline for the clients that would allow them to develop their mental and physical well-being.
The participants were anonymous, and the researchers promised that their information would never be leaked in the study. In each session, the participants were asked several questions on the difficulties that they experienced. The researchers provided individual feedback on their answers using response letters. A previous study reported that nursing interventions that were provided based on the theory of caring for individuals who had experienced intimate partner violence had a therapeutic effect []. As the participants of that study had recently experienced difficulty with self-exposure and needed to develop their beliefs with the nurses, the nurses continued to maintain the patient’s belief throughout the nursing intervention [].
For the “maintaining belief” and “being with” domains, response letters were sent to the clients individually after each session. The response letters were developed at the request of the participants during the evaluation. The participants proposed that interaction and support with the therapist would be effective. The response letter was created to facilitate interactive communication with the client and clients were provided feedback on their answers to the questions. The “being with” domain emphasizes the intimate relationship with the client as the center of care []; that is, it is based on the client’s bonding and attachment []. Using themselves as therapeutic tools, nurses must be emotionally open to client reactions and be able to reassure clients with a warm attitude [,]. The reasons for failure in psychiatric counseling have been reported to include clients’ lack of trust, intimacy, and motivation in relation to the therapist []. In this study, after the end of each session, based on the client’s responses, they were sent a supportive and positive response letter to give them a sense of intimacy and hope. Moreover, the response letters played a role in motivating and encouraging clients to continue their participation in the program without giving up.
In the Session 1 and 2, for the “knowing” dimension, clients were helped to understand their current state of mind, past traumatic experiences, moods, thoughts, and strengths. Specifically, clients were made aware of their strengths and ability to overcome the effects of trauma. It is imperative that nurses understand and respect clients from a holistic perspective. The patient can overcome a crisis by getting to know and respecting themselves through the process of knowing []. The sessions helped clients to become familiar with and respect themselves through knowledge of their strengths. Finding strengths is a positive psychological intervention that can relieve depression and lead to improved well-being. Its effectiveness has been demonstrated in several studies [,]. Clients increase their happiness in life by finding and enhancing their strengths.
In Sessions 3−5, the concept of “doing for” focused on enhancing the clients’ competencies. Clients in this program could accept and share their traumatic experiences through self-disclosure. To do this, clients were asked multiple questions through noninvasive techniques. Moreover, they were provided with a wealth of knowledge on trauma that enabled them to strengthen their own capabilities through constant training. The characteristics of competence included knowledge, ongoing adjustment to learning collective skills, and self-confidence [,]. This program provided a self-help guide for clients. It allowed them to accept trauma-related experiences by themselves and develop a rational perspective while controlling negative emotions. Previous studies reported that Internet-based, self-help interventions for patients with PTSD and eating disorders were less expensive than face-to-face treatment [,]; however, they were effective in reducing negative emotions such as depression and alleviating its symptoms. In particular, they may have had a better effect during early treatment [].
For the “enabling” dimension, the client’s changes were identified, and clients were encouraged to continue to take care of themselves through intrinsic motivation in Sessions 6−8. “Enabling” emphasizes the need for continuous validation and confirms the appropriate results of caring [,]. Engagement, meaning, positive relationships, and achievement-based interventions are effective strategies for increasing well-being and improving depressive symptoms []. Clients were encouraged to feel a sense of accomplishment for the changes they had made and to praise and reward themselves. In addition, based on what they had gained through this program, they were encouraged to practice appropriate communication in negative relationships and situations in their daily lives and continue their stress management strategies. Thus, the importance of finding meaning in their daily lives and maintaining a sense of happiness was emphasized.
This study was also significant because it was an online nursing intervention program. Although online treatment and intervention programs are provided in various clinical fields, there are few online nursing interventions in the mental health nursing field [,,]. The greatest advantage of online programs is the lack of time and space constraints. Face-to-face counseling has become increasingly difficult since the onset of the coronavirus disease 2019 pandemic []. In place of face-to-face counseling, Internet-based intervention programs are expected to help greater numbers of people who have experienced trauma. Online intervention programs have the advantage of being more cost effective than face-to-face consultations [,]. They also allow for 1:1 interaction and can provide interventions through two-way communication [,].
Often in psychiatric counseling cases, patients avoid counseling due to the fear of stigma []. The stigma associated with mental health problems such as traumatic stress can act as a barrier to mental health treatment and positive outcomes []. Online programs are advantageous as they reduce the stigma and the burden of face-to-face counseling, allowing clients to be completely vulnerable and face their own problems.
Although Internet-based therapies have posed technical difficulties [,], the development of such interventions is incredibly advantageous because it contributes to the spread of standardization. The trauma recovery intervention program that was developed in this study presented a standardized framework and material for eight sessions. We expect that a standardized intervention program will improve the quality of nursing intervention services and enhance the nursing intervention competency []. One study that provided education programs to nurses based on Swanson’s theory of caring found that nurses who were trained according to the caring framework had much higher levels of care than those who were not []. Moreover, both patients and nurses expressed greater satisfaction due to the reinforcing of the relationship between nurses and patients []. We also expect that this program will enhance satisfaction not only for clients who have experienced trauma but also for the nurses who provide nursing care.
Limitations
A limitation of the study is that it was not possible to evaluate the effectiveness of the program. Another limitation is the small number of participants.
5. Conclusions
The trauma recovery program that was developed in this study was based on Swanson’s theory of caring []. Caring has long been recognized as the center of nursing care and is increasingly becoming a key concept []. Therefore, this study is of great significance as it provides evidence that mental health nurses could develop and implement programs to care for people who have experienced trauma. The program will help to alleviate PTSD symptoms and, ultimately, allow for patients to live happy and meaningful lives. An online program could even provide nursing interventions for trauma recovery for marginalized people who are unable to receive help from nurses for physical reasons, such as distance and time. In addition, as one of the advantages of online programs is the characteristically swift dissemination of information, we propose that nurses in various regions could easily learn from trauma intervention programs and provide high-quality nursing interventions to their clients. The program will need to be administered to clients who have experienced trauma, and continued research will need to confirm whether they experience symptom relief and for how long. In addition, it will be important to widely disseminate the program, educate nurses on trauma and use of the program, and investigate whether there is an increase in nurses’ trauma intervention competency as a result.
Author Contributions
Conceptualization, methodology, and formal analysis: S.K., G.-U.K., and J.P.; investigation: S.K., G.-U.K., and W.L.; writing—original draft preparation, writing—review and editing: S.K., G.-U.K., and J.P.; project administration and funding acquisition: S.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Research Foundation of Korea, grant number 2018R1A2B6001504.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Yonsei University (Y-2019-0083).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kessler, R.C. Posttraumatic stress disorder: The burden to the individual and to society. J. Clin. Psychiatry 2000, 61 (Suppl. 5), 4–14. [Google Scholar] [PubMed]
- Magruder, K.M.; McLaughlin, K.A.; Elmore Borbon, D.L. Trauma is a public health issue. Eur. J. Psychotraumatol. 2017, 8, 1375338. [Google Scholar] [CrossRef]
- Simblett, S.; Birch, J.; Matcham, F.; Yaguez, L.; Morris, R. A systematic review and meta-analysis of e-mental health interventions to treat symptoms of posttraumatic stress. JMIR Ment. Health 2017, 4, e14. [Google Scholar] [CrossRef]
- Paik, J.-W.; Kim, H.-S.; Sim, M.; Lee, H.-K.; Woo, Y.S.; Chung, C.; Lee, S.-H.; Seok, J.-H.; Jeon, H.J.; Lee, S.-M.; et al. The Sewol ferry accident and early mental health care response by volunteer activities of Korean disaster mental health committee and members of Korean neuropsychiatric association. J. Korean Neuropsychiatr. Assoc. 2015, 54, 1–5. [Google Scholar] [CrossRef]
- Yang, H.J.; Cheong, H.K.; Choi, B.Y.; Shin, M.-H.; Yim, H.W.; Kim, D.-H.; Kim, G.; Lee, S.Y. Community mental health status six months after the Sewol ferry disaster in Ansan, Korea. Epidemiol. Health 2015, 37, e2015046. [Google Scholar] [CrossRef]
- Sijbrandij, M.; Olff, M.; Reitsma, J.B.; Carlier, I.V.; de Vries, M.H.; Gersons, B.P. Treatment of acute posttraumatic stress disorder with brief cognitive behavioral therapy: A randomized controlled trial. Am. J. Psychiatry 2007, 164, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.A.; Moulds, M.L.; Nixon, R.V. Cognitive behaviour therapy of acute stress disorder: A four-year follow-up. Behav. Res. Ther. 2003, 41, 489–494. [Google Scholar] [CrossRef]
- Mabey, L.; van Servellen, G. Treatment of post-traumatic stress disorder in patients with severe mental illness: A review. Int. J. Ment. Health Nurs. 2014, 23, 42–50. [Google Scholar] [CrossRef]
- Bride, B.E. Prevalence of secondary traumatic stress among social workers. Soc. Work 2007, 52, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Atkins, C.D.; Burnett, H.J., Jr. Specialized disaster behavioral health training: Its connection with response, practice, trauma health, and resilience. Disaster Health 2016, 3, 57–65. [Google Scholar] [CrossRef]
- Bruce, M.M.; Kassam-Adams, N.; Rogers, M.; Anderson, K.M.; Sluys, K.P.; Richmond, T.S. Trauma providers’ knowledge, views and practice of trauma-informed care. J. Trauma Nurs. 2018, 25, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Kim, S.A.; Kong, S. Resilience mediates impact of some childhood maltreatment on post-traumatic stress symptoms in conscripted marines in the Republic of Korea. Res. Nurs. Health 2017, 40, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Kong, S.S.; Kim, H.R. Impact of childhood trauma and social support on dissociative symptoms in Marines. J. Korean Acad. Psychiatr. Ment. Health Nurs. 2016, 24, 257–266. [Google Scholar] [CrossRef]
- Lewis, C.E.; Farewell, D.; Groves, V.; Kitchiner, N.J.; Roberts, N.P.; Vick, T.; Bisson, J.I. Internet-based guided self-help for posttraumatic stress disorder (PTSD): Randomized controlled trial. Depress. Anxiety 2017, 34, 555–565. [Google Scholar] [CrossRef]
- Silva Butcher, R.G.C.; Jones, D.A. An integrative review of comprehensive nursing assessment tools developed based on Gordon’s Eleven Functional Health Patterns. Int. J. Nurs. Knowl. 2021. [Google Scholar] [CrossRef]
- Swanson, K.M. Empirical development of a middle range theory of caring. Nurs. Res. 1991, 40, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Kavanaugh, K.; Roscigno, C.I.; Swanson, K.M.; Savage, T.A.; Kimura, R.E.; Kilpatrick, S.J. Perinatal palliative care: Parent perceptions of caring in interactions surrounding counseling for risk of delivering an extremely premature infant. Palliat. Support. Care 2015, 13, 145–155. [Google Scholar] [CrossRef]
- Higdon, K.; Shirey, M. Implementation of a caring theoretical framework in a multihospital system. J. Nurs. Adm. 2012, 42, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Tonges, M.; Ray, J. Translating caring theory into practice: The carolina care Model. J. Nurs. Adm. 2011, 41, 374–381. [Google Scholar] [CrossRef]
- Choi, Y.K. Evidence-based treatment of posttraumatic stress disorder. Korean J. Clin. Psychol. 2017, 36, 526–549. [Google Scholar] [CrossRef]
- Marshall, J.M.; Dunstan, D.A.; Bartik, W. The role of digital mental health resources to treat trauma symptoms in Australia during COVID-19. Psychol. Trauma 2020, 12 (Suppl. 1), S269–S271. [Google Scholar] [CrossRef] [PubMed]
- Price, M.; Sawyer, T.; Harris, M.; Skalka, C. Usability evaluation of a mobile monitoring system to assess symptoms after a traumatic injury: A mixed-methods study. JMIR Ment. Health 2016, 3, e3. [Google Scholar] [CrossRef] [PubMed]
- Lewis, C.; Roberts, N.P.; Bethell, A.; Robertson, L.; Bisson, J.I. Internet-based cognitive and behavioural therapies for post-traumatic stress disorder (PTSD) in adults. Cochrane Database Syst. Rev. 2018, CD011710. [Google Scholar] [CrossRef]
- Kalfoss, M.; Owe, J. Empirical verification of Swanson’s caring processes found in nursing actions: Systematic review. Open J. Nurs. 2015, 5, 976–986. [Google Scholar] [CrossRef][Green Version]
- Swanson, K.M.; Chen, H.T.; Graham, J.C.; Wojnar, D.M.; Petras, A. Resolution of depression and grief during the first year after miscarriage: A randomized controlled clinical trial of couples-focused interventions. J. Women’s Health 2009, 18, 1245–1257. [Google Scholar] [CrossRef]
- Finfgeld-Connett, D. Meta-synthesis of caring in nursing. J. Clin. Nurs. 2008, 17, 196–204. [Google Scholar] [CrossRef]
- Huynh, T.; Alderson, M.; Thompson, M. Emotional labour underlying caring: An evolutionary concept analysis. J. Adv. Nurs. 2008, 64, 195–208. [Google Scholar] [CrossRef]
- Schlosser, D.; Campellone, T.; Kim, D.; Truong, B.; Vergani, S.; Ward, C.; Vinogradov, S. Feasibility of PRIME: A cognitive neuroscience-informed mobile app intervention to enhance motivated behavior and improve quality of life in recent onset schizophrenia. JMIR Res. Protoc. 2016, 5, e77. [Google Scholar] [CrossRef]
- Gander, F.; Proyer, R.T.; Ruch, W. Positive psychology interventions addressing pleasure, engagement, meaning, positive relationships, and accomplishment increase well-being and ameliorate depressive symptoms: A randomized, placebo-controlled online study. Front. Psychol. 2016, 7, 686. [Google Scholar] [CrossRef]
- Proyer, R.T.; Gander, F.; Wellenzohn, S.; Ruch, W. Strengths-based positive psychology interventions: A randomized placebo-controlled online trial on long-term effects for a signature strengths-vs. a lesser strengths-intervention. Front. Psychol. 2015, 6, 456. [Google Scholar] [CrossRef]
- Hudon, C.; Tribble, D.S.; Bravo, G.; Poitras, M.E. Enablement in health care context: A concept analysis. J. Eval. Clin. Pract. 2011, 17, 143–149. [Google Scholar] [CrossRef] [PubMed]
- de Zwaan, M.; Herpertz, S.; Zipfel, S.; Svaldi, J.; Friederich, H.C.; Schmidt, F.; Mayr, A.; Lam, T.; Schade-Brittinger, C.; Hilbert, A. Effect of internet-based guided self-help vs individual face-to-face treatment on full or subsyndromal binge eating disorder in overweight or obese patients: The interbed randomized clinical trial. JAMA Psychiatry 2017, 74, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Kim, G.-U.; Yoon, H.J.; Kim, S. A systematic review of the effect of web-based trauma-education programs for mental-health professionals. J. Korean Acad. Psychiatr. Ment. Health Nurs. 2020, 29, 325–338. [Google Scholar] [CrossRef]
- Andrews, G.; Cuijpers, P.; Craske, M.G.; McEvoy, P.; Titov, N. Computer therapy for the anxiety and depressive disorders is effective, acceptable and practical health care: A meta-analysis. PLoS ONE 2010, 5, e13196. [Google Scholar] [CrossRef] [PubMed]
- Donker, T.; Petrie, K.; Proudfoot, J.; Clarke, J.; Birch, M.R.; Christensen, H. Smartphones for smarter delivery of mental health programs: A systematic review. J. Med. Internet Res. 2013, 15, e247. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).