
WISER Survivor Trial: Combined Effect of Exercise and Weight Loss Interventions on Insulin and Insulin Resistance in Breast Cancer Survivors

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
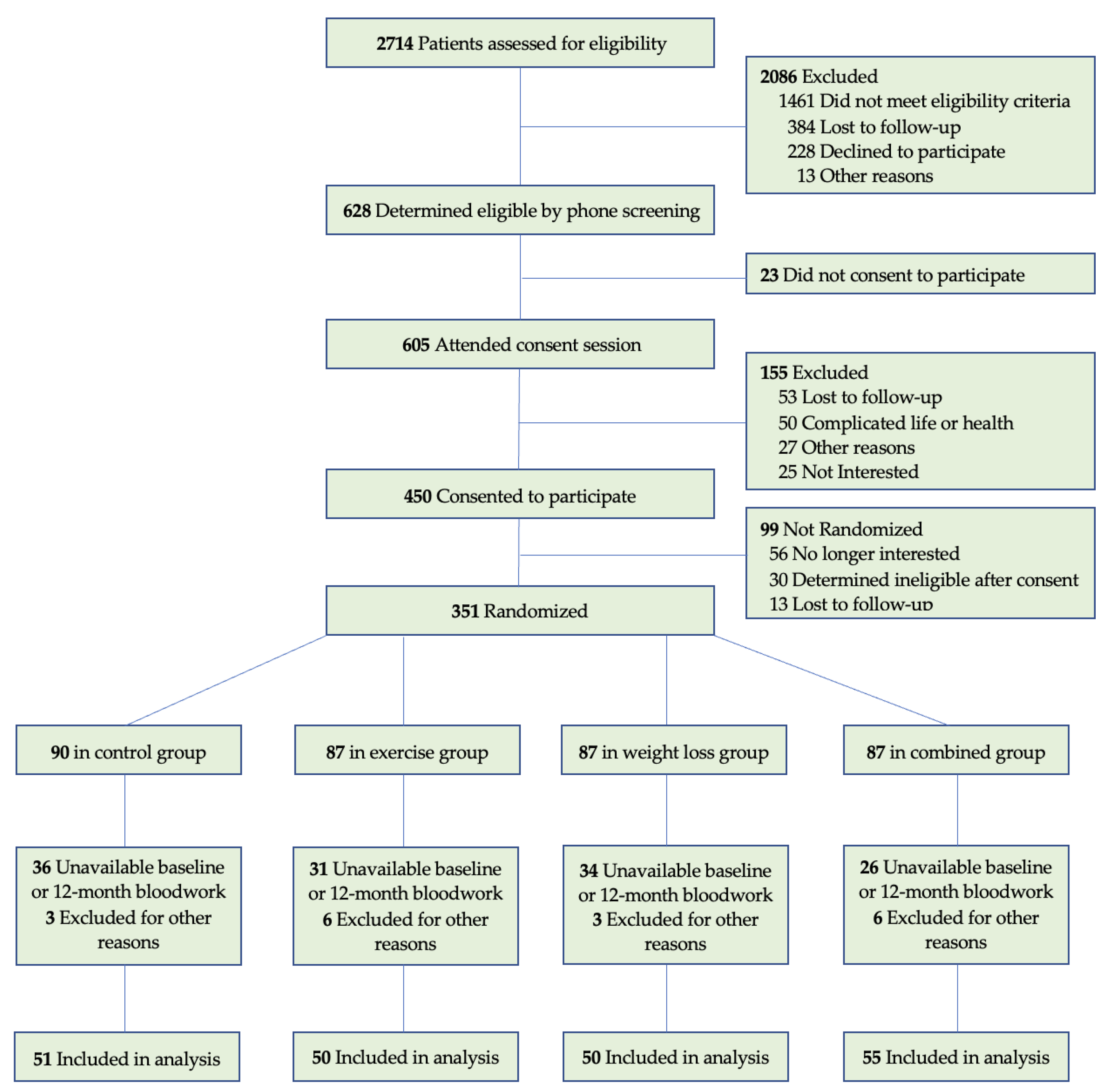
2.2. Participants
2.3. Exercise Intervention
2.4. Weight Loss Intervention
2.5. Exercise and Weight Loss Intervention
2.6. Control Group
2.7. Biomarker Assays
2.8. Measurements
2.9. Statistical Analysis
3. Results
3.1. Intervention Effects
3.1.1. Effects of Change in Body Composition and Treadmill Endurance
3.1.2. Normalization of C-Peptide
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ganz, P.A.; Goodwin, P.J. Breast Cancer Survivorship: Where Are We Today? Stud. Biomark. New Targets Aging Res. Iran 2015, 862, 1–8. [Google Scholar] [CrossRef]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [Green Version]
- Colleoni, M.; Sun, Z.; Price, K.N.; Karlsson, P.; Forbes, J.F.; Thürlimann, B.; Gianni, L.; Castiglione, M.; Gelber, R.D.; Coates, A.S.; et al. Annual Hazard Rates of Recurrence for Breast Cancer During 24 Years of Follow-Up: Results From the Interna-tional Breast Cancer Study Group Trials I to V. J. Clin. Oncol. 2016, 34, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, P.; Downey, L.; Stopeck, A.T. Caring for the Breast Cancer Survivor: A Guide for Primary Care Physicians. Am. J. Med. 2010, 123, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Ewertz, M.; Jensen, M.-B.; Gunnarsdóttir, K.Á.; Højris, I.; Jakobsen, E.H.; Nielsen, D.; Stenbygaard, L.E.; Tange, U.B.; Cold, S. Effect of Obesity on Prognosis After Early-Stage Breast Cancer. J. Clin. Oncol. 2011, 29, 25–31. [Google Scholar] [CrossRef]
- Bergom, C.; Kelly, T.; Bedi, M.; Saeed, H.; Prior, P.; Rein, L.E.; Szabo, A.; Wilson, J.F.; Currey, A.D.; White, J. Association of Locoregional Control With High Body Mass Index in Women Undergoing Breast Conservation Thera-py for Early-Stage Breast Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Pizot, C.; Boniol, M.; Mullie, P.; Koechlin, A.; Boniol, M.; Boyle, P.; Autier, P. Physical activity, hormone replacement therapy and breast cancer risk: A meta-analysis of prospective studies. Eur. J. Cancer 2016, 52, 138–154. [Google Scholar] [CrossRef] [Green Version]
- Renehan, A.G.; Tyson, M.; Egger, M.; Heller, R.F.; Zwahlen, M. Body-mass index and incidence of cancer: A systematic review and meta-analysis of prospective observational studies. Lancet 2008, 371, 569–578. [Google Scholar] [CrossRef]
- Crozier, J.A.; Crozier, J.A.; Moreno-Aspitia, A.; Ballman, K.V.; Dueck, A.C.; Pockaj, B.A.; Perez, E.A. Effect of body mass index on tumor characteristics and disease-free survival in patients from the HER2-positive ad-juvant trastuzumab trial N9831. Cancer 2013, 119, 2447–2454. [Google Scholar] [CrossRef] [Green Version]
- Cleveland, R.J.; Eng, S.M.; Abrahamson, P.E.; Britton, J.A.; Teitelbaum, S.L.; Neugut, A.I.; Gammon, M.D. Weight Gain Prior to Diagnosis and Survival from Breast Cancer. Cancer Epidemiol. Biomark. Prev. 2007, 16, 1803–1811. [Google Scholar] [CrossRef] [Green Version]
- Vance, V.; Hanning, R.; Mourtzakis, M.; McCargar, L. Weight gain in breast cancer survivors: Prevalence, pattern and health consequences. Obes. Rev. 2010, 12, 282–294. [Google Scholar] [CrossRef] [PubMed]
- Nichols, H.B.; Trentham-Dietz, A.; Egan, K.M.; Titus-Ernstoff, L.; Holmes, M.D.; Bersch, A.J.; Holick, C.N.; Hampton, J.M.; Stampfer, M.J.; Willett, W.C.; et al. Body Mass Index Before and After Breast Cancer Diagnosis: Associations with All-Cause, Breast Cancer, and Cardiovascular Disease Mortality. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1403–1409. [Google Scholar] [CrossRef] [Green Version]
- Van Kruijsdijk, R.C.M.; Van Der Wall, E.; Visseren, F. Obesity and Cancer: The Role of Dysfunctional Adipose Tissue. Cancer Epidemiol. Biomark. Prev. 2009, 18, 2569–2578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, D.P.; Haffner, S.M.; Baillargeon, J. Adiposity, the Metabolic Syndrome, and Breast Cancer in African-American and White American Women. Endocr. Rev. 2007, 28, 763–777. [Google Scholar] [CrossRef] [PubMed]
- Duggan, C.; Irwin, M.L.; Xiao, L.; Henderson, K.D.; Smith, A.W.; Baumgartner, R.N.; Baumgartner, K.B.; Bernstein, L.; Ballard-Barbash, R.; McTiernan, A. Associations of Insulin Resistance and Adiponectin With Mortality in Women With Breast Cancer. J. Clin. Oncol. 2011, 29, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Pan, K.; Chlebowski, R.T.; Mortimer, J.E.; Gunther, M.J.; Rohan, T.; Vitolins, M.Z.; Adams-Campbell, L.L.; Ho, G.Y.F.; Cheng, T.D.; Nelson, R.A. Insulin resistance and breast cancer incidence and mortality in postmenopausal women in the Women’s Health Initiative. Cancer 2020, 126, 3638–3647. [Google Scholar] [CrossRef] [PubMed]
- Pollak, M.N.; Chapman, J.W.; Shepherd, L.; Meng, D.; Richardson, P.; Orme, C.W.; Pritchard, K.I. Insulin resistance, estimated by serum C-peptide level, is associated with reduced event-free survival for postmeno-pausal women in NCIC CTG MA.14 adjuvant breast cancer trial. J. Clin. Oncol. 2006, 24, 524. [Google Scholar] [CrossRef]
- Formica, V.; Tesauro, M.; Cardillo, C.; Roselli, M. Insulinemia and the risk of breast cancer and its relapse. Diabetes Obes. Metab. 2012, 14, 1073–1080. [Google Scholar] [CrossRef]
- Kim, J.; Choi, W.J.; Jeong, S.H. The Effects of Physical Activity on Breast Cancer Survivors after Diagnosis. J. Cancer Prev. 2013, 18, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Holmes, M.D. Physical Activity and Survival after Breast Cancer Diagnosis. JAMA 2005, 293, 2479–2486. [Google Scholar] [CrossRef] [Green Version]
- Schmitz, K.H.; Campbell, A.M.; Stuiver, M.M.; Pinto, B.M.; Schwartz, A.L.; Morris, G.S.; Ligibel, J.A.; Cheville, A.; Galvão, D.A.; Alfano, C.M.; et al. Exercise is medicine in oncology: Engaging clinicians to help patients move through cancer. CA A Cancer J. Clin. 2019, 69, 468–484. [Google Scholar] [CrossRef] [Green Version]
- Maliniak, M.L.; Patel, A.V.; McCullough, M.L.; Campbell, P.T.; Leach, C.R.; Gapstur, S.M.; Gaudet, M.M. Obesity, physical activity, and breast cancer survival among older breast cancer survivors in the Cancer Preven-tion Study-II Nutrition Cohort. Breast Cancer Res. Treat. 2018, 167, 133–145. [Google Scholar] [CrossRef]
- Shaikh, H.; Bradhurst, P.; Ma, L.X.; Tan, S.Y.; Egger, S.J.; Vardy, J.L. Body weight management in overweight and obese breast cancer survivors. Cochrane Database Syst. Rev. 2020, 2020, CD012110. [Google Scholar] [CrossRef]
- Viskochil, R.; Blankenship, J.M.; Makari-Judson, G.; Staudenmayer, J.; Freedson, P.S.; Hankinson, S.E.; Braun, B. Metrics of Diabetes Risk Are Only Minimally Improved by Exercise Training in Postmenopausal Breast Cancer Survivors. J. Clin. Endocrinol. Metab. 2020, 105, e1958–e1966. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.S.; Kim, T.H.; Kong, I.D. Exercise intervention lowers aberrant serum WISP-1 levels with insulin resistance in breast cancer survivors: A randomized controlled trial. Sci. Rep. 2020, 10, 10898. [Google Scholar] [CrossRef]
- Travier, N.; Buckland, G.; Vendrell, J.J.; Fernandez-Veledo, S.; Peiró, I.; Del Barco, S.; Pernas, S.; Zamora, E.; Bellet, M.; Margeli, M.; et al. Changes in metabolic risk, insulin resistance, leptin and adiponectin following a lifestyle intervention in overweight and obese breast cancer survivors. Eur. J. Cancer Care 2018, 27, e12861. [Google Scholar] [CrossRef]
- Dittus, K.L.; Harvey, J.R.; Bunn, J.Y.; Kokinda, N.D.; Wilson, K.M.; Priest, J.; Pratley, R.E. Impact of a behaviorally-based weight loss intervention on parameters of insulin resistance in breast cancer survivors. BMC Cancer 2018, 18, 351. [Google Scholar] [CrossRef] [Green Version]
- Winkels, R.M.; Sturgeon, K.M.; Kallan, M.J.; Dean, L.T.; Zhang, Z.; Evangelisti, M.; Brown, J.C.; Sarwer, D.B.; Troxel, A.B.; Denlinger, C.; et al. The women in steady exercise research (WISER) survivor trial: The innovative transdisciplinary design of a ran-domized controlled trial of exercise and weight-loss interventions among breast cancer survivors with lymphedema. Contemp. Clin. Trials 2017, 61, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Schmitz, S.H.; Troxel, A.B.; Dean, L.T.; DeMichele, A.; Brown, J.C.; Sturgeon, K.; Zhang, Z.; Evangelisti, M.; Spinelli, B.; Kallan, M.J.; et al. Effect of Home-Based Exercise and Weight Loss Programs on Breast Cancer-Related Lymphedema Outcomes Among Overweight Breast Cancer Survivors: The WISER Survivor Randomized Clinical Trial. JAMA Oncol. 2019, 5, 1605–1613. [Google Scholar] [CrossRef] [PubMed]
- Sturgeon, K.M.; Bs, R.H.; Fornash, A.; Dean, L.T.; Laudermilk, M.; Brown, J.C.; Sarwer, D.B.; DeMichele, A.M.; Troxel, A.B.; Schmitz, K.H. Strategic recruitment of an ethnically diverse cohort of overweight survivors of breast cancer with lymphedema. Cancer 2017, 124, 95–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruce, R.A.; Kusumi, F.; Hosmer, D. Maximal oxygen intake and nomographic assessment of functional aerobic impairment in car-diovascular disease. Am. Heart J. 1973, 85, 546–562. [Google Scholar] [CrossRef]
- Wallace, T.M.; Levy, J.; Matthews, D.R. Use and Abuse of HOMA Modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pagana, K.D.; Pagana, T.J.; Pagana, T. Mosby’s Diagnostic & Laboratory Test Reference, 14th ed.; Mosby: St. Louis, MO, USA, 2018. [Google Scholar]
- The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care 2003, 26, 3160–3167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ligibel, J.A.; Campbell, N.; Partridge, A.; Chen, W.Y.; Salinardi, T.; Chen, H.; Adloff, K.; Keshaviah, A.; Winer, E.P. Impact of a Mixed Strength and Endurance Exercise Intervention on Insulin Levels in Breast Cancer Survivors. J. Clin. Oncol. 2008, 26, 907–912. [Google Scholar] [CrossRef]
- Fabian, C.J.; Kimler, B.F.; Donnelly, J.E.; Sullivan, D.K.; Klemp, J.R.; Petroff, B.K.; Phillips, T.A.; Metheny, T.; Aversman, S.; Yeh, H.-W.; et al. Favorable modulation of benign breast tissue and serum risk biomarkers is associated with >10% weight loss in postmenopausal women. Breast Cancer Res. Treat. 2013, 142, 119–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yee, L.D.; Mortimer, J.E.; Natarajan, R.; Dietze, E.C.; Seewaldt, V.L. Metabolic Health, Insulin, and Breast Cancer: Why Oncologists Should Care About Insulin. Front. Endocrinol. 2020, 11, 58. [Google Scholar] [CrossRef] [Green Version]
- Mason, C.; Foster-Schubert, K.E.; Imayama, I.; Kong, A.; Xiao, L.; Bain, C.; Campbell, K.L.; Wang, C.-Y.; Duggan, C.; Ulrich, C.M.; et al. Dietary Weight Loss and Exercise Effects on Insulin Resistance in Postmenopausal Women. Am. J. Prev. Med. 2011, 41, 366–375. [Google Scholar] [CrossRef]


{kind=link}
| Cohort n = 206 | Control n = 51 | Exercise n = 50 | Weight Loss n = 50 | Combined n = 55 | p Value | |
|---|---|---|---|---|---|---|
| Age, y | 59.9 ± 8.9 | 60.5 ± 8.9 | 59.3 ± 8.8 | 59.7 ± 8.8 | 60.2 ± 9.2 | 0.90 |
| BMI, kg/m2 | 33.8 ± 5.9 | 33.3 ± 5.3 | 34.5 ± 7.0 | 34.1 ± 5.7 | 33.4 ± 5.8 | 0.86 |
| Time since diagnosis, y | 7.8 ± 5.3 | 8.8 ± 5.4 | 7.4 ± 5.3 | 7.6 ± 5.6 | 7.4 ± 4.9 | 0.41 |
| Race | ||||||
| Non-Hispanic White | 138 (67) | 37 (72.5) | 33 (66.0) | 34 (68.0) | 34 (61.8) | |
| Black | 61 (29.6) | 12 (23.5) | 16 (32.0) | 16 (32.0) | 17 (30.9) | |
| Other | 7 (3.4) | 2 (3.9) | 1 (2.0) | 0 | 4 (7.3) | 0.45 |
| Education | ||||||
| High school diploma | 36 (17.5) | 11 (21.6) | 7 (14.0) | 5 (10.0) | 13 (23.6) | |
| Some college | 67 (32.5) | 16 (31.4) | 14 (28.0) | 21 (42.0) | 16 (29.1) | |
| College education | 103 (50) | 24 (47.1) | 29 (58.0) | 24 (48.0) | 26 (47.3) | 0.38 |
| Endocrine therapy | ||||||
| Aromatase inhibitors | 70 (33) | 17 (33.3) | 16 (32.0) | 19 (38.0) | 18 (32.7) | 0.92 |
| Tamoxifen | 20 (9.7) | 4 (7.8) | 8 (16.0) | 5 (10.0) | 3 (5.4) | 0.31 |
| Anti-Diabetes Medication | 17 (8.2) | 1 (2.0) | 4 (8.0) | 7 (14.0) | 5 (9.1) | 0.18 |
| Control | Exercise | Weight Loss | Combined | |
|---|---|---|---|---|
| Insulin (uIU/mL) | ||||
| Baseline | 17.8 ± 11.5 | 16.5 ± 10.2 | 17.5 ± 8.3 | 16.2 ± 11.4 |
| 12-Months | 18.1 ± 10.6 | 16.8 ± 9.9 | 13.5 ± 7.3 a | 13.2 ± 9.6 a |
| Change | 0.3 | 0.3 | −4.0 | −3.0 |
| C-peptide (ng/mL) | ||||
| Baseline | 2.4 ± 1.0 | 2.3 ±1.0 | 2.4 ± 1.0 | 2.3 ± 1.2 |
| 12-Months | 2.5 ± 0.9 | 2.5 ± 1.1 | 2.0 ± 0.9 a | 2.0 ± 1.1 a |
| Change | 0.1 | 0.2 | −0.4 | −0.3 |
| Glucose (mg/dL) | ||||
| Baseline | 103 ± 14.5 | 111 ± 31.7 | 110 ±14.9 | 102 ± 12.7 |
| 12-Months | 99.7 ± 15.1 | 116 ± 40.6 a | 106 ±17.5 | 101 ± 14.0 |
| Change | −3.3 | 5.0 | −4.0 | −1.0 |
| HOMA2-IR | ||||
| Baseline | 2.0 ± 1.3 | 1.9 ± 1.2 | 2.0 ± 0.95 | 1.8 ± 1.3 |
| 12-Months | 2.0 ± 1.2 | 2.0 ± 1.2 | 1.6 ± 0.8 a | 1.5 ± 1.1 a |
| Change | 0 | 0.1 | −0.4 | −0.3 |
| HOMA2-β | ||||
| Baseline | 110 ± 35.4 | 103 ± 33.8 | 97.2 ± 31.8 | 107 ± 38.1 |
| 12-Months | 121 ± 38.1 | 99.7 ± 34.4 a | 95.1 ± 32.6 a | 101 ± 39.5 a |
| Change | 11 | −3.3 | −2.1 | −6.0 |
| Weight Loss (%) * | |||
|---|---|---|---|
| <0–5 (Reference) | ≥5–10 | ≥10 | |
| n | 70 | 30 | 47 |
| Δ Insulin (uIU/mL) | −2.79 (8.5) | −3.16 (6.7) | −5.03 (7.7) a |
| Δ C-peptide (ng/mL) | −0.08 (0.7) | −0.17 (0.6) | −0.55 (0.7) a |
| Δ Glucose (mg/dL) | −0.20 (26.1) | 0.07 (12.8) | −8.08 (11.6) |
| Δ HOMA2-IR | −0.31 (0.9) | −0.36 (0.8) | −0.60 (0.9) a |
| Δ HOMA2-β | 1.20 (35.8) | −4.69 (23.4) | −4.35 (21.9) |
| Δ Fat Mass (kg) ** | |||
| Tertile | 1 (Reference) | 2 | 3 |
| Range (kg) | +15.5 to −1.2 | −1.3 to −4.9 | −5.0 to −30 |
| Mean, [Median (SD)] | 1.4, [0.95 (2.6)] | −2.7, [−2.6 (0.97)] | −9.1, [−7.7 (4.3)] |
| n | 66 | 66 | 67 |
| Δ Insulin (uIU/mL) | 2.78 (7.9) | −2.39 (8.1) a | −5.52 (7.6) a |
| Δ C-peptide (ng/mL) | 0.32 (0.7) | −0.08 (0.73) a | −0.53 (0.66) a |
| Δ Glucose (mg/dL) | 3.82 (27.1) | 0.15 (13.4) | −5.87 (12.3) |
| Δ HOMA2-IR | 0.33 (0.91) | −0.26 (0.89) a | −0.65 (0.86) a |
| Δ HOMA2-β | 5.45 (27.6) | −0.43 (35.1) | −6.33 (23.4) a |
| Δ Lean Body Mass (kg) ** | |||
| Tertile | 1 (Reference) | 2 | 3 |
| Range (kg) | −7.7 to −1.298 | −1.297 to 0.68 | 0.7 to 13.3 |
| Mean, [Median (SD)] | −3.1, [−2.8 (1.4)] | −0.4, [−0.4 (0.5)] | 2.3, [1.8 (1.8)] |
| n | 67 | 66 | 66 |
| Δ Insulin (uIU/mL) | −3.18 (7.6) | −1.6 (9.1) | −0.38 (8.8) a |
| Δ C-peptide (ng/mL) | −0.26 (0.8) | −0.08 (0.8) | 0.04 (0.7) a |
| Δ Glucose (mg/dL) | −6.95 (19.7) | 2.16 (20.9) a | 2.9 (15.1) a |
| Δ HOMA2-IR | −0.38 (0.9) | −0.17 (1.0) | −0.03 (1.0) a |
| Δ HOMA2-β | −0.26 (25.2) | −2.08 (25.3) | 0.93 (36.6) |
| Δ Time on Treadmill (s) *** | |||
| Tertile | 1 (Reference) | 2 | 3 |
| Range (sec) | −711 to −65 | −64 to 28 | 31 to 752 |
| Mean, [Median (SD)] | −194, [−166 (133)] | −13.4, [−0.5 (27.8)] | 163, [117 (151)] |
| n | 62 | 62 | 62 |
| Δ Insulin (uIU/mL) | 0.11 (8.6) | −1.67 (9.5) | −4.17 (7.3) a |
| Δ C-peptide (ng/mL) | −0.03 (0.7) | −0.07 (0.9) | −0.26 (0.6) |
| Δ Glucose (mg/dL) | −0.43 (14.7) | −0.76 (27.0) | −1.57 (13.4) |
| Δ HOMA2-IR | 0.01 (1.0) | −0.19 (1.0) | −0.48 (0.1) a |
| Δ HOMA2-β | 2.54 (26.7) | 0.20 (34.9) | −4.65 (22.1) |
| Adjusted Model C-Peptide | Adjusted Model Glucose | |
|---|---|---|
| Control | 1.0 n = 33 b, 37 c | 1.0 n = 28 b, 25 c |
| Exercise | 2.3 (0.8–6.6) n = 32 b, 29 c | 0.44 (0.2–1.2) n = 27 b, 32 c |
| Diet | 2.9 (1.0–9.0) n = 32 b, 23 c | 0.86 (0.3–2.4) n = 39 b, 31 c |
| Combined | 4.5 (1.4–14.1) a n = 31 b, 23 c | 0.75 (0.3–2.2) n = 29 b, 28 c |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Alonzo, N.J.; Qiu, L.; Sears, D.D.; Chinchilli, V.; Brown, J.C.; Sarwer, D.B.; Schmitz, K.H.; Sturgeon, K.M. WISER Survivor Trial: Combined Effect of Exercise and Weight Loss Interventions on Insulin and Insulin Resistance in Breast Cancer Survivors. Nutrients 2021, 13, 3108. https://doi.org/10.3390/nu13093108
D’Alonzo NJ, Qiu L, Sears DD, Chinchilli V, Brown JC, Sarwer DB, Schmitz KH, Sturgeon KM. WISER Survivor Trial: Combined Effect of Exercise and Weight Loss Interventions on Insulin and Insulin Resistance in Breast Cancer Survivors. Nutrients. 2021; 13(9):3108. https://doi.org/10.3390/nu13093108
Chicago/Turabian StyleD’Alonzo, Nicholas J., Lin Qiu, Dorothy D. Sears, Vernon Chinchilli, Justin C. Brown, David B. Sarwer, Kathryn H. Schmitz, and Kathleen M. Sturgeon. 2021. "WISER Survivor Trial: Combined Effect of Exercise and Weight Loss Interventions on Insulin and Insulin Resistance in Breast Cancer Survivors" Nutrients 13, no. 9: 3108. https://doi.org/10.3390/nu13093108
APA StyleD’Alonzo, N. J., Qiu, L., Sears, D. D., Chinchilli, V., Brown, J. C., Sarwer, D. B., Schmitz, K. H., & Sturgeon, K. M. (2021). WISER Survivor Trial: Combined Effect of Exercise and Weight Loss Interventions on Insulin and Insulin Resistance in Breast Cancer Survivors. Nutrients, 13(9), 3108. https://doi.org/10.3390/nu13093108