
Performance of Existing Definitions and Tests for the Diagnosis of Invasive Fungal Diseases other than Invasive Candidiasis and Invasive Aspergillosis in Critically Ill, Adult Patients: A Systematic Review with Qualitative Evidence Synthesis

 ,
, 
 , , , , , ,
, , , , , , 
Abstract
1. Introduction
2. Methods
2.1. Data Sources and Data Management
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
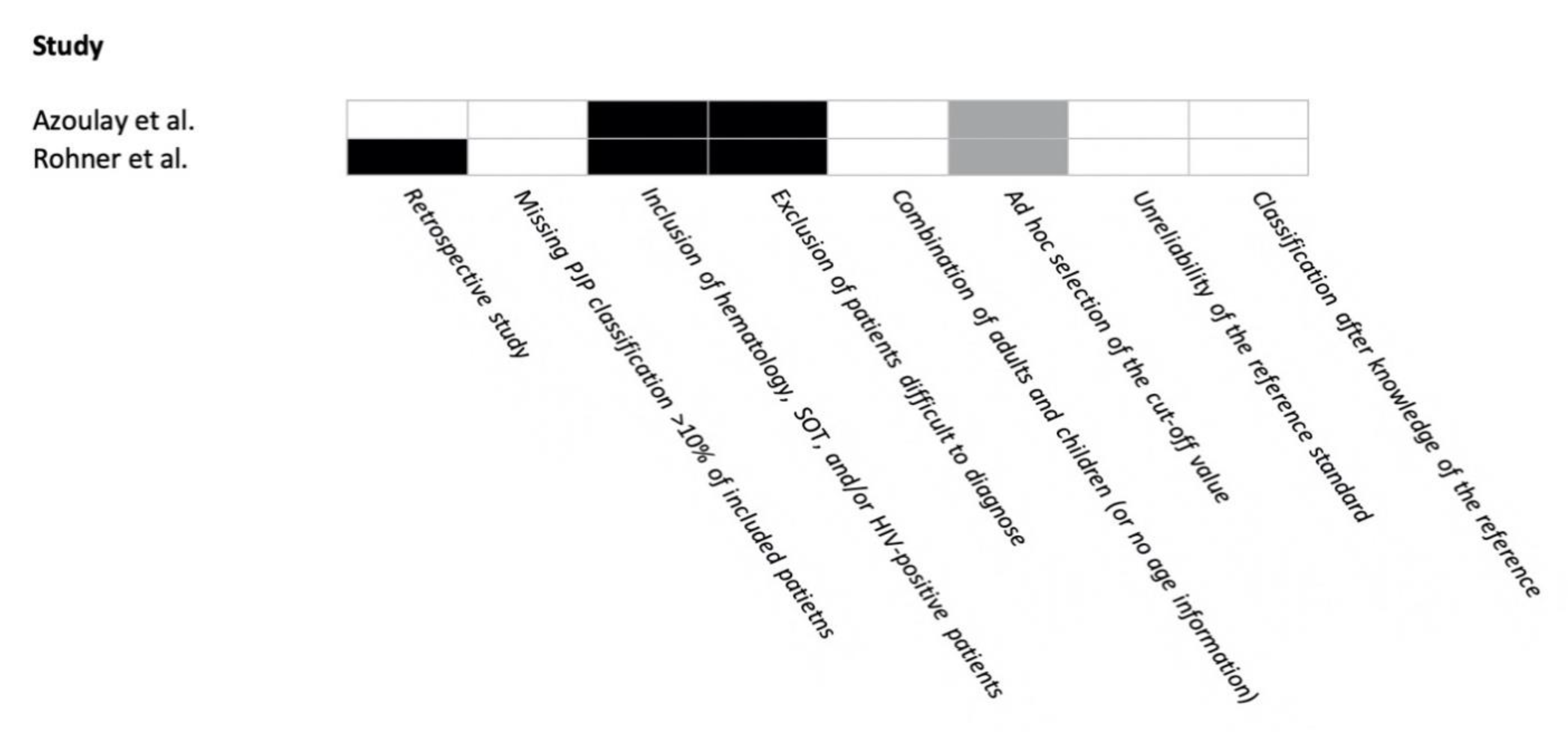
2.4. Risk of Bias
- retrospective design and data collection;
- missing classification for >10% of included patients;
- study population also including hematology/SOT patients (and HIV-positive patients for PJP);
- exclusion of patients with difficult-to-diagnose IFDs;
- mixed population of children and adults with ad hoc selection of the diagnostic cutoff;
- unreliable reference (i.e., any reference standard different from histology or culture from normally sterile sites, or microscopy for PJP);
- classification as IFD after knowledge of the result of the reference standard.
2.5. Quantitative Data Synthesis
3. Results
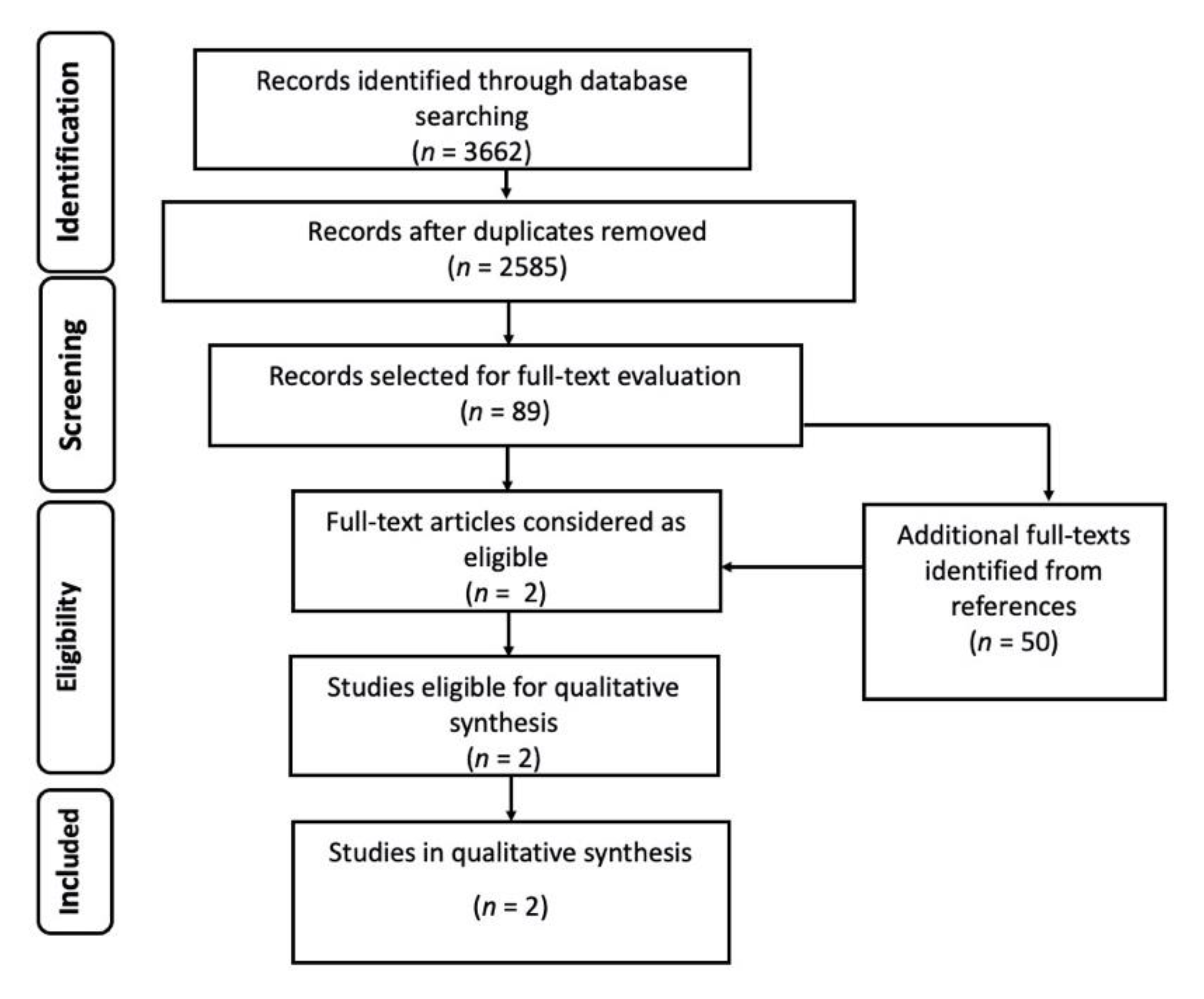
3.1. Pneumocystis jirovecii Pneumonia
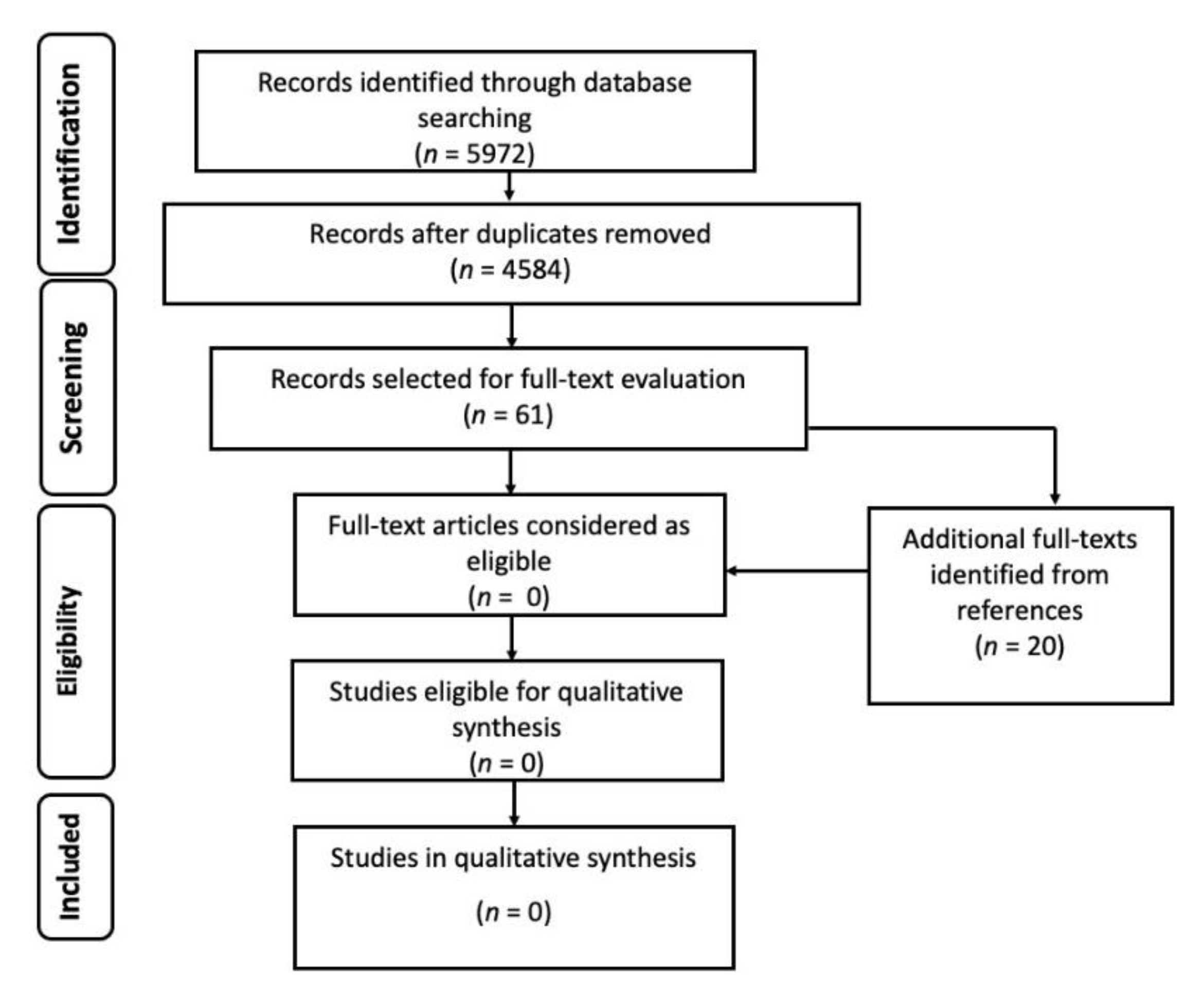
3.2. Other Non-IA, Non-IC IFDs
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bouza, E.; Munoz, P. Epidemiology of candidemia in intensive care units. Int. J. Antimicrob. Agents 2008, 32, S87–S91. [Google Scholar] [CrossRef]
- Taccone, F.S.; Van den Abeele, A.M.; Bulpa, P.; Misset, B.; Meersseman, W.; Cardoso, T.; Paiva, J.A.; Blasco-Navalpotro, M.; De Laere, E.; Dimopoulos, G.; et al. Epidemiology of invasive aspergillosis in critically ill patients: Clinical presentation, underlying conditions, and outcomes. Crit. Care 2015, 19, 7. [Google Scholar] [CrossRef]
- Bassetti, M.; Bouza, E. Invasive mould infections in the ICU setting: Complexities and solutions. J. Antimicrob. Chemother. 2017, 72, i39–i47. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Giacobbe, D.R.; Vena, A.; Trucchi, C.; Ansaldi, F.; Antonelli, M.; Adamkova, V.; Alicino, C.; Almyroudi, M.P.; Atchade, E.; et al. Incidence and outcome of invasive candidiasis in intensive care units (ICUs) in Europe: Results of the EUCANDICU project. Crit. Care 2019, 23, 219. [Google Scholar] [CrossRef]
- Montravers, P.; Dupont, H.; Gauzit, R.; Veber, B.; Auboyer, C.; Blin, P.; Hennequin, C.; Martin, C. Candida as a risk factor for mortality in peritonitis. Crit. Care Med. 2006, 34, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Blot, S.I.; Taccone, F.S.; Van den Abeele, A.M.; Bulpa, P.; Meersseman, W.; Brusselaers, N.; Dimopoulos, G.; Paiva, J.A.; Misset, B.; Rello, J.; et al. A clinical algorithm to diagnose invasive pulmonary aspergillosis in critically ill patients. Am. J. Respir. Crit. Care Med. 2012, 186, 56–64. [Google Scholar] [CrossRef]
- Bassetti, M.; Marchetti, M.; Chakrabarti, A.; Colizza, S.; Garnacho-Montero, J.; Kett, D.H.; Munoz, P.; Cristini, F.; Andoniadou, A.; Viale, P.; et al. A research agenda on the management of intra-abdominal candidiasis: Results from a consensus of multinational experts. Intensive Care Med. 2013, 39, 2092–2106. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, J.P.; Chen, S.C.; Kauffman, C.A.; Steinbach, W.J.; Baddley, J.W.; Verweij, P.E.; Clancy, C.J.; Wingard, J.R.; Lockhart, S.R.; Groll, A.H.; et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clin. Infect. Dis. 2020, 71, 1367–1376. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Giacobbe, D.R.; Grecchi, C.; Rebuffi, C.; Zuccaro, V.; Scudeller, L.; investigators, F. Performance of existing definitions and tests for the diagnosis of invasive aspergillosis in critically ill, adult patients: A systematic review with qualitative evidence synthesis. J. Infect. 2020, 81, 131–146. [Google Scholar] [CrossRef]
- Bassetti, M.; Scudeller, L.; Giacobbe, D.R.; Lamoth, F.; Righi, E.; Zuccaro, V.; Grecchi, C.; Rebuffi, C.; Akova, M.; Alastruey-Izquierdo, A.; et al. Developing definitions for invasive fungal diseases in critically ill adult patients in intensive care units. Protocol of the FUNgal infections Definitions in ICU patients (FUNDICU) project. Mycoses 2019, 62, 310–319. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Azoulay, E.; Bergeron, A.; Chevret, S.; Bele, N.; Schlemmer, B.; Menotti, J. Polymerase chain reaction for diagnosing pneumocystis pneumonia in non-HIV immunocompromised patients with pulmonary infiltrates. Chest 2009, 135, 655–661. [Google Scholar] [CrossRef]
- Rohner, P.; Jacomo, V.; Studer, R.; Schrenzel, J.; Graf, J.D. Detection of Pneumocystis jirovecii by two staining methods and two quantitative PCR assays. Infection 2009, 37, 261–265. [Google Scholar] [CrossRef]
- Festic, E.; Gajic, O.; Limper, A.H.; Aksamit, T.R. Acute respiratory failure due to pneumocystis pneumonia in patients without human immunodeficiency virus infection: Outcome and associated features. Chest 2005, 128, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Monnet, X.; Vidal-Petiot, E.; Osman, D.; Hamzaoui, O.; Durrbach, A.; Goujard, C.; Miceli, C.; Bouree, P.; Richard, C. Critical care management and outcome of severe Pneumocystis pneumonia in patients with and without HIV infection. Crit. Care 2008, 12, R28. [Google Scholar] [CrossRef] [PubMed]
- Zahar, J.R.; Robin, M.; Azoulay, E.; Fieux, F.; Nitenberg, G.; Schlemmer, B. Pneumocystis carinii pneumonia in critically ill patients with malignancy: A descriptive study. Clin. Infect. Dis. 2002, 35, 929–934. [Google Scholar] [CrossRef]
- Lee, E.H.; Kim, E.Y.; Lee, S.H.; Roh, Y.H.; Leem, A.Y.; Song, J.H.; Kim, S.Y.; Chung, K.S.; Jung, J.Y.; Kang, Y.A.; et al. Risk factors and clinical characteristics of Pneumocystis jirovecii pneumonia in lung cancer. Sci. Rep. 2019, 9, 2094. [Google Scholar] [CrossRef]
- Doyle, L.; Vogel, S.; Procop, G.W. Pneumocystis PCR: It Is Time to Make PCR the Test of Choice. Open Forum Infect. Dis. 2017, 4, ofx193. [Google Scholar] [CrossRef]
- Guegan, H.; Robert-Gangneux, F. Molecular diagnosis of Pneumocystis pneumonia in immunocompromised patients. Curr. Opin. Infect. Dis. 2019, 32, 314–321. [Google Scholar] [CrossRef]
- Muhlethaler, K.; Bogli-Stuber, K.; Wasmer, S.; von Garnier, C.; Dumont, P.; Rauch, A.; Muhlemann, K.; Garzoni, C. Quantitative PCR to diagnose Pneumocystis pneumonia in immunocompromised non-HIV patients. Eur. Respir. J. 2012, 39, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.L.; Wen, Y.H.; Wu, Y.S.; Wang, M.C.; Chang, P.Y.; Yang, S.; Lu, J.J. Diagnosis of Pneumocystis pneumonia by real-time PCR in patients with various underlying diseases. J. Microbiol. Immunol. Infect. 2020, 53, 785–790. [Google Scholar] [CrossRef]
- Mercier, T.; Guldentops, E.; Patteet, S.; Beuselinck, K.; Lagrou, K.; Maertens, J. Beta-d-Glucan for Diagnosing Pneumocystis Pneumonia: A Direct Comparison between the Wako beta-Glucan Assay and the Fungitell Assay. J. Clin. Microbiol. 2019, 57. [Google Scholar] [CrossRef] [PubMed]
- Cornely, O.A.; Alastruey-Izquierdo, A.; Arenz, D.; Chen, S.C.A.; Dannaoui, E.; Hochhegger, B.; Hoenigl, M.; Jensen, H.E.; Lagrou, K.; Lewis, R.E.; et al. Global guideline for the diagnosis and management of mucormycosis: An initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect. Dis. 2019, 19, e405–e421. [Google Scholar] [CrossRef]
- Devauchelle, P.; Jeanne, M.; Frealle, E. Mucormycosis in Burn Patients. J. Fungi 2019, 5, 25. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, D.R.; Riccardi, N.; Vena, A.; Bassetti, M. Mould Infections of Traumatic Wounds: A Brief Narrative Review. Infect. Dis. Ther. 2020, 9, 1–15. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study, Year [Reference] (Test vs. Reference) | Design | Reference Categories N/Total (Prevalence) | Sensitivity | Specificity | PPV | NPV | LR+ | LR− | DOR | Population |
|---|---|---|---|---|---|---|---|---|---|---|
| Azoulay et al., 2009 1 [12] (PCR vs. conventional stains on BALF or sputum) | Cohort Prospective Single -center | Pos/Neg 39/448 patients (8.7%) | 87.2% (IS plus BALF) 84% (BALF) | 92.2% (IS plus BALF) 93% (BALF) | 51.5% (IS plus BALF) 53.1% (BALF) | 98.7% (IS plus BALF) 87.2% (BALF) | 11 (IS plus BALF) 12 (BALF) | 0.14 (IS plus BALF) 0.17 (BALF) | NR | Non-HIV immunocompromised patients admitted to the ICU or pulmonology wards with pulmonary infiltrates and respiratory failure |
| Rohner et al., 2009 2 [13] (PCR vs. microscopy on BALF) | Cross-sectional Retrospective Single -center | Pos/Neg 33/186 samples (17.7%) | 100% (BALF) | 92.4% (BALF) | 63.4% (BALF) | 100% (BALF) | 13.5 (BALF) | 0 (BALF) | NR | Patients had signs and symptoms and/or radiological abnormalities that included PJP as the differential diagnosis. Mixed patient cohort, including ICU |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giacobbe, D.R.; Cortegiani, A.; Karaiskos, I.; Mercier, T.; Tejada, S.; Peghin, M.; Grecchi, C.; Rebuffi, C.; Asperges, E.; Zuccaro, V.; et al. Performance of Existing Definitions and Tests for the Diagnosis of Invasive Fungal Diseases other than Invasive Candidiasis and Invasive Aspergillosis in Critically Ill, Adult Patients: A Systematic Review with Qualitative Evidence Synthesis. J. Fungi 2021, 7, 176. https://doi.org/10.3390/jof7030176
Giacobbe DR, Cortegiani A, Karaiskos I, Mercier T, Tejada S, Peghin M, Grecchi C, Rebuffi C, Asperges E, Zuccaro V, et al. Performance of Existing Definitions and Tests for the Diagnosis of Invasive Fungal Diseases other than Invasive Candidiasis and Invasive Aspergillosis in Critically Ill, Adult Patients: A Systematic Review with Qualitative Evidence Synthesis. Journal of Fungi. 2021; 7(3):176. https://doi.org/10.3390/jof7030176
Chicago/Turabian StyleGiacobbe, Daniele R., Andrea Cortegiani, Ilias Karaiskos, Toine Mercier, Sofia Tejada, Maddalena Peghin, Cecilia Grecchi, Chiara Rebuffi, Erika Asperges, Valentina Zuccaro, and et al. 2021. "Performance of Existing Definitions and Tests for the Diagnosis of Invasive Fungal Diseases other than Invasive Candidiasis and Invasive Aspergillosis in Critically Ill, Adult Patients: A Systematic Review with Qualitative Evidence Synthesis" Journal of Fungi 7, no. 3: 176. https://doi.org/10.3390/jof7030176
APA StyleGiacobbe, D. R., Cortegiani, A., Karaiskos, I., Mercier, T., Tejada, S., Peghin, M., Grecchi, C., Rebuffi, C., Asperges, E., Zuccaro, V., Scudeller, L., Bassetti, M., & the FUNDICU investigators. (2021). Performance of Existing Definitions and Tests for the Diagnosis of Invasive Fungal Diseases other than Invasive Candidiasis and Invasive Aspergillosis in Critically Ill, Adult Patients: A Systematic Review with Qualitative Evidence Synthesis. Journal of Fungi, 7(3), 176. https://doi.org/10.3390/jof7030176