
Influence of Serum Vitamin D Levels on Survival Rate and Marginal Bone Loss in Dental Implants: A Systematic Review

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Review Development and Focused Question
2.2. Eligibility Criteria
2.2.1. Inclusion Criteria
2.2.2. Exclusion Criteria
2.3. Type of Intervention and Comparisons
2.4. Data Collection
2.5. Sources and Search Strategy
2.6. Study Selection and Screening Methods
2.7. Clinical Data Extraction
2.8. Risk of Bias Analysis
3. Results
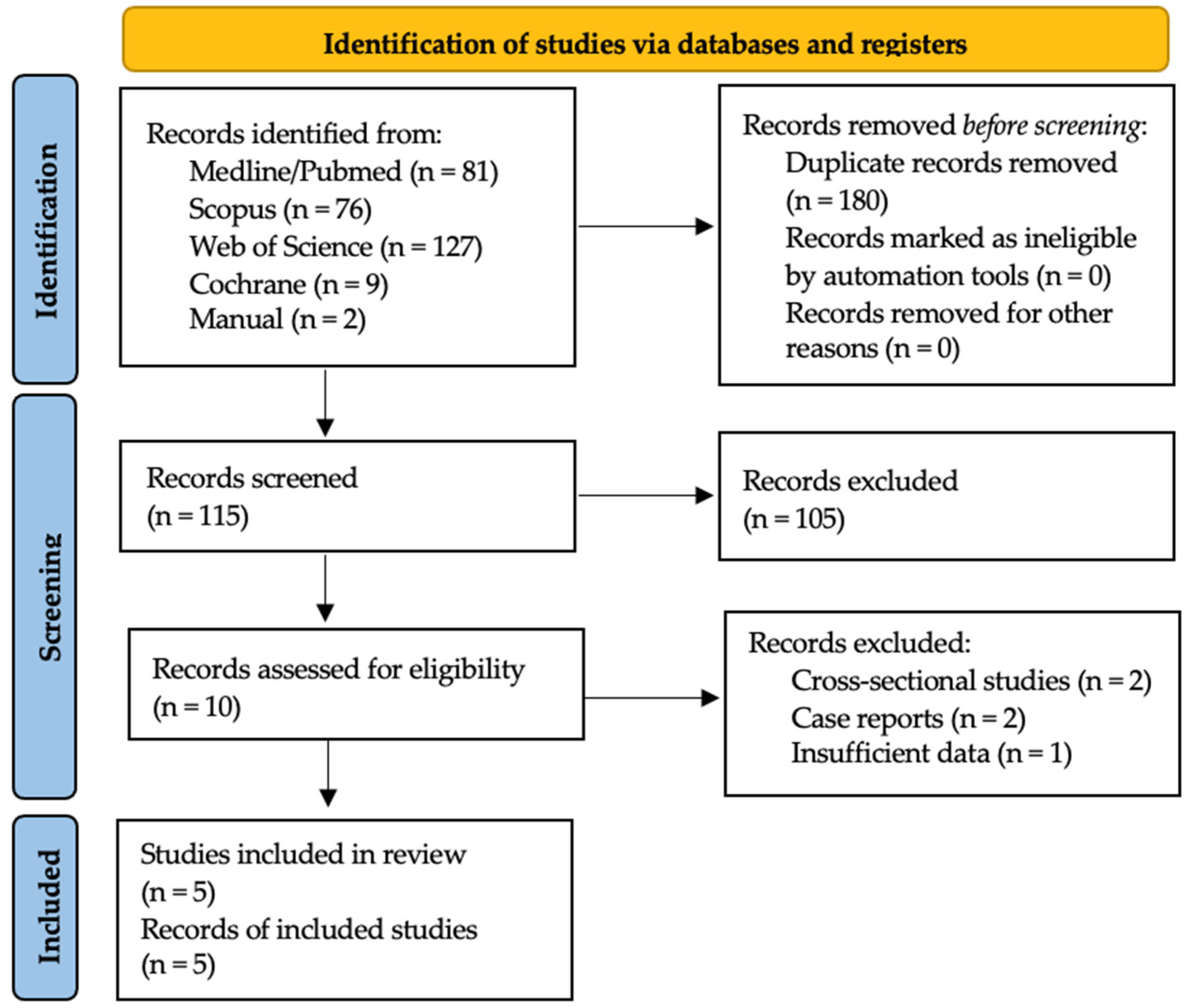
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment
3.4. Synthesis of Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. A retrospective study on clinical and radiological outcomes of oral implants in patients followed up for a minimum of 20 years. Clin. Implant Dent. Relat. Res. 2018, 20, 199–207. [Google Scholar] [CrossRef]
- Mangano, F.G.; Mastrangelo, P.; Luongo, F.; Blay, A.; Tunchel, S.; Mangano, C. Aesthetic outcome of immediately restored single implants placed in extraction sockets and healed sites of the anterior maxilla: A retrospective study on 103 patients with 3 years of follow-up. Clin. Oral Implants Res. 2017, 28, 272–282. [Google Scholar] [CrossRef]
- Bosshardt, D.D.; Chappuis, V.; Buser, D. Osseointegration of titanium, titanium alloy and zirconia dental implants: Current knowledge and open questions. Periodontol 2000 2017, 73, 22–40. [Google Scholar] [CrossRef]
- Mangano, C.; Iaculli, F.; Piattelli, A.; Mangano, F. Fixed restorations supported by Morse-taper connection implants: A retrospective clinical study with 10–20 years of follow-up. Clin. Oral Implants Res. 2015, 2, 1229–1236. [Google Scholar] [CrossRef] [PubMed]
- Brånemark, P.I.; Adell, R.; Breine, U.; Hansson, B.O.; Lindström, J.; Ohlsson, A. Intra-osseous anchorage of dental prostheses. I. Experimental studies. Scand. J. Plast. Reconstr. Surg. 1969, 3, 81–100. [Google Scholar] [CrossRef]
- Lee, J.W.Y.; Bance, M.L. Physiology of Osseointegration. Otolaryngol. Clin. N. Am. 2019, 52, 231–242. [Google Scholar] [CrossRef]
- Troiano, G.; Lo Russo, L.; Canullo, L.; Ciavarella, D.; Lo Muzio, L.; Laino, L. Early and late implant failure of submerged versus non-submerged implant healing: A systematic review, meta-analysis and trial sequential analysis. J. Clin. Periodontol. 2018, 45, 613–623. [Google Scholar] [CrossRef]
- Jawad, S.; Barclay, C.; Whittaker, W.; Tickle, M.; Walsh, T. A pilot randomised controlled trial evaluating mini and conventional implant retained dentures on the function and quality of life of patients with an edentulous mandible. BMC Oral Health. 2017, 17, 53. [Google Scholar] [CrossRef] [PubMed]
- Suarez, F.; Chan, H.L.; Monje, A.; Galindo-Moreno, P.; Wang, H.L. Effect of the timing of restoration on implant marginal bone loss: A systematic review. J. Periodontol. 2013, 84, 159–169. [Google Scholar] [CrossRef]
- Insua, A.; Monje, A.; Wang, H.L.; Miron, R.J. Basis of bone metabolism around dental implants during osseointegration and peri-implant bone loss. J. Biomed. Mater. Res. A 2017, 105, 2075–2089. [Google Scholar] [CrossRef]
- Bechara, S.; Kubilius, R.; Veronesi, G.; Pires, J.T.; Shibli, J.A.; Mangano, F.G. Short (6-mm) dental implants versus sinus floor elevation and placement of longer (≥10-mm) dental implants: A randomized controlled trial with a 3-year follow-up. Clin. Oral Implants Res. 2017, 28, 1097–1107. [Google Scholar] [CrossRef] [PubMed]
- Shibli, J.A.; Pires, J.T.; Piattelli, A.; Iezzi, G.; Mangano, C.; Mangano, F.; De Souza, S.L.; Gehrke, S.A.; Wang, H.-L.; Ehrenfest, D.M.D. Impact of Different Implant Surfaces Topographies on Peri-Implant Tissues: An Update of Current Available Data on Dental Implants Retrieved from Human Jaws. Curr. Pharm. Biotechnol. 2017, 18, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Lin, G.; Ye, S.; Liu, F.; He, F. A retrospective study of 30,959 implants: Risk factors associated with early and late implant loss. J. Clin. Periodontol. 2018, 45, 733–743. [Google Scholar] [CrossRef]
- Esposito, M.; Hirsch, J.M.; Lekholm, U.; Thomsen, P. Biological factors contributing to failures of osseointegrated oral implants. (I). Success criteria and epidemiology. Eur. J. Oral Sci. 1998, 106, 527–551. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Lips, P. Vitamin D physiology. Prog. Biophys. Mol. Biol. 2006, 92, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.T.; Antony, S.; Nandhu, M.S.; Sadanandan, J.; Naijil, G.; Paulose, C.S. Vitamin D3 restores altered cholinergic and insulin receptor expression in the cerebral cortex and muscarinic M3 receptor expression in pancreatic islets of streptozotocin induced diabetic rats. J. Nutr. Biochem. 2011, 22, 418–425. [Google Scholar] [CrossRef]
- Isaia, G.; Giorgino, R.; Rini, G.B.; Bevilacqua, M.; Maugeri, D.; Adami, S. Prevalence of hypovitaminosis D in elderly women in Italy: Clinical consequences and risk factors. Osteoporos. Int. 2003, 14, 577–582. [Google Scholar] [CrossRef]
- Javed, F.; Malmstrom, H.; Kellesarian, S.V.; Al-Kheraif, A.A.; Vohra, F.; Romanos, G.E. Efficacy of Vitamin D3 Supplementation on Osseointegration of Implants. Implant Dent. 2016, 25, 281–287. [Google Scholar] [CrossRef]
- Cho, Y.J.; Heo, S.J.; Koak, J.Y.; Kim, S.K.; Lee, S.J.; Lee, J.H. Promotion of osseointegration of anodized titanium implants with a 1 α,25-dihydroxy-vitamin D3 submicron particle coating. Int. J. Oral Maxillofac. Implants 2011, 26, 1225–1232. [Google Scholar]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane collaboration’s tool for assessing risk of bias in randomized trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 25 May 2022).
- Bryce, G.; MacBeth, N. Vitamin D deficiency as a suspected causative factor in the failure of an immediately placed dental implant: A case report. J. R. Naval Med. Serv. 2014, 100, 328–332. [Google Scholar] [CrossRef]
- Fretwurst, T.; Grunert, S.; Woelber, J.P.; Nelson, K.; Semper-Hogg, W. Vitamin D deficiency in early implant failure: Two case reports. Int. J. Implant Dent. 2016, 2, 24. [Google Scholar] [CrossRef] [PubMed]
- Wagner, F.; Schuder, K.; Hof, M.; Heuberer, S.; Seemann, R.; Dvorak, G. Does osteoporosis influence the marginal peri-implant bone level in female patients? A cross-sectional study in a matched collective. Clin. Implant Dent. Relat. Res. 2017, 19, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Munhoz Pereira, T.; Alvim-Pereira, F.; Kaiser Alvim-Pereira, C.C.; Ignácio, S.A.; Machado de Souza, C.; Trevilatto, P.C. A complete physical mapping of the vitamin D receptor gene for dental implant loss: A pilot study. Clin. Oral Implants Res. 2019, 30, 1165–1178. [Google Scholar] [CrossRef]
- Thim, T.; Scholz, K.J.; Hiller, K.A.; Buchalla, W.; Kirschneck, C.; Fleiner, J.; Woelber, J.P.; Cieplik, F. Radiographic Bone Loss and Its Relation to Patient-Specific Risk Factors, LDL Cholesterol, and Vitamin D: A Cross-Sectional Study. Nutrients 2022, 14, 864. [Google Scholar] [CrossRef]
- Guido Mangano, F.; Ghertasi Oskouei, S.; Paz, A.; Mangano, N.; Mangano, C. Low serum vitamin D and early dental implant failure: Is there a connection? A retrospective clinical study on 1740 implants placed in 885 patients. J. Dent. Res. Dent. Clin. Dent. Prospects 2018, 12, 174–182. [Google Scholar] [CrossRef]
- Mangano, F.; Mortellaro, C.; Mangano, N.; Mangano, C. Is Low Serum Vitamin D Associated with Early Dental Implant Failure? A Retrospective Evaluation on 1625 Implants Placed in 822 Patients. Mediators Inflamm. 2016, 2016, 5319718. [Google Scholar] [CrossRef]
- Garg, P.; Ghalaut, P.; Dahiya, K.; Ravi, R.; Sharma, A.; Wakure, P. Comparative evaluation of crestal bone level in patients having low level of Vitamin D treated with dental implant with or without Vitamin D3 supplements. Natl. J. Maxillofac. Surg. 2020, 11, 199–206. [Google Scholar] [CrossRef]
- Kwiatek, J.; Jaroń, A.; Trybek, G. Impact of the 25-Hydroxycholecalciferol Concentration and Vitamin D Deficiency Treatment on Changes in the Bone Level at the Implant Site during the Process of Osseointegration: A Prospective, Randomized, Controlled Clinical Trial. J. Clin. Med. 2021, 10, 526. [Google Scholar] [CrossRef]
- Tabrizi, R.; Mohajerani, H.; Jafari, S.; Tümer, M.K. Does the serum level of vitamin D affect marginal bone loss around dental implants? Int. J. Oral. Maxillofac. Surg. 2021, 51, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Rapuri, P.B.; Gallagher, J.C.; Nawaz, Z. Caffeine decreases vitamin D receptor protein expression and 1,25(OH)2D3 stimulated alkaline phosphatase activity in human osteoblast cells. J. Steroid Biochem. Mol. Biol. 2007, 103, 368–371. [Google Scholar] [CrossRef] [PubMed]
- Greene-Finestone, L.S.; Berger, C.; de Groh, M.; Hanley, D.A.; Hidiroglou, N.; Sarafin, K.; Poliquin, S.; Krieger, J.; Richards, J.B.; Goltzman, D.; et al. 25-Hydroxyvitamin D in Canadian adults: Biological, environmental, and behavioral correlates. Osteoporos. Int. 2011, 22, 1389–1399. [Google Scholar] [CrossRef] [PubMed]
- Kunutsor, S.K.; Apekey, T.A.; Steur, M. Vitamin D and risk of future hypertension: Meta-analysis of 283,537 participants. Eur. J. Epidemiol. 2013, 28, 205–221. [Google Scholar] [CrossRef]
- Cashman, K.D.; Dowling, K.G.; Škrabáková, Z.; Gonzalez-Gross, M.; Valtuena, J.; De Henauw, S.; Michaelsen, K.F. Vitamin D deficiency in Europe: Pandemic? Am. J. Clin. Nutr. 2016, 103, 1033–1044. [Google Scholar] [CrossRef] [PubMed]
- Pludowski, P.; Holick, M.F.; Grant, W.B.; Konstantynowicz, J.; Mascarenhas, M.R.; Haq, A.; Povoroznyuk, V.; Balatska, N.; Barbosa, A.P.; Karonova, T.; et al. Vitamin D supplementation guidelines. J. Steroid Biochem. Mol. Biol. 2018, 175, 125–135. [Google Scholar] [CrossRef]
- Rusińska, A.; Płudowski, P.; Walczak, M.; Borszewska-Kornacka, M.K.; Bossowski, A.; Chlebna-Sokół, D.; Czech-Kowalska, J.; Dobrzańska, A.; Franek, E.; Helwich, E.; et al. Vitamin D Supplementation Guidelines for General Population and Groups at Risk of Vitamin D Deficiency in Poland-Recommendations of the Polish Society of Pediatric Endocrinology and Diabetes and the Expert Panel with Participation of National Specialist Consultants and Representatives of Scientific Societies-2018 Update. Front. Endocrinol. 2018, 9, 246. [Google Scholar] [CrossRef]
- Dvorak, G.; Fügl, A.; Watzek, G.; Tangl, S.; Pokorny, P.; Gruber, R. Impact of dietary vitamin D on osseointegration in the ovariectomized rat. Clin. Oral Implants Res. 2012, 23, 1308–1313. [Google Scholar] [CrossRef]
- Liu, W.; Zhang, S.; Zhao, D.; Zou, H.; Sun, N.; Liang, X.; Dard, M.; Lanske, B.; Yuan, Q. Vitamin D supplementation enhances the fixation of titanium implants in chronic kidney disease mice. PLoS ONE 2014, 9, e95689. [Google Scholar] [CrossRef]
- Charoenngam, N.; Shirvani, A.; Holick, M.F. The ongoing D-lemma of vitamin D supplementation for nonskeletal health and bone health. Curr. Opin. Endocrinol. Diabetes Obes. 2019, 26, 301–305. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D status: Measurement, interpretation, and clinical application. Ann. Epidemiol. 2009, 19, 73–78. [Google Scholar] [CrossRef]
- Monje, A.; Suarez, F.; Galindo-Moreno, P.; García-Nogales, A.; Fu, J.H.; Wang, H.L. A systematic review on marginal bone loss around short dental implants (<10 mm) for implant-supported fixed prostheses. Clin. Oral Implants Res. 2014, 25, 1119–1124. [Google Scholar] [CrossRef] [PubMed]
- Howe, M.S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Abdelhay, N.; Prasad, S.; Gibson, M.P. Failure rates associated with guided versus non-guided dental implant placement: A systematic review and meta-analysis. BDJ Open 2021, 7, 31. [Google Scholar] [CrossRef]

{kind=link}
| Study | Reason for Exclusion |
|---|---|
| Wagner et al., 2017, Thim et al., 2022 [25,27] | Cross-sectional studies |
| Bryce et al., 2014, Fretwurst et al., 2016 [23,24] | Case report |
| Munhoz et al., 2019 [26] | Insuficient data |
| Author and Year | Study | Patients (Number) | Gender (Male/Female) | Mean Age (Years) | Vitamin D Serum Level (Patients) | Timing of Vitamin D Sampling | Implants (Number) | Implants Location | Implants Survival (%) | Marginal Bone Loss (mm)/DM | Bone Remodeling during Osseointegration (mm)/DM | Mean Follow-Up (Months) | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mangano et al., 2018 [28] | Retrospective study. Three cohorts | 885 | 455 | 430 | 57.3 ± 14.4 | G1: <10 ng/mL: 27 G2: 10–30 ng/mL: 448 G3: >30 ng/mL: 410 | Two weeks prior to surgery | 1740 | - | G1: 88.9 G2: 95.6 G3: 97.1 | - | - | 168 |
| Garg et al., 2020 [30] | RCT | 32 | - | - | 20–40 (range) | G1: <30 ng/mL (supplement): 16 G2: <30 ng/mL: 16 | At the time of diagnosis. The subsequent blood samples were taken at 3-month and 6-month follow-up period from G1 patients | 32 | Mandibular posterior teeth | 100 | - | G1: M: 0.832 D: 1.085 G2: M: 0.229 D: 0.285 RVG | 6 |
| Kwiatek et al., 2021 [31] | RCT | 122 | 57 | 65 | 43.8 ± 12.15 | G1: <30 ng/mL (supplement): 48 G2: <30 ng/mL: 43 G3: >30 ng/mL: 31 | On the day of surgery, after six weeks, and after twelve weeks. | 122 | Premolar and molar mandible | 100 | - | G1: 0.08 ± 0.93 G2: 0.53 ± 0.77 G3: 0.48 ± 0.74 RVG | 3 |
| Tabrizi et al., 2021 [32] | Prospective study. Three cohorts | 90 | 56 | 34 | G1: 41.50 ± 10.13 G2: 45.03 ± 11.16 G3: 40.73 ± 9.95 | G1: <10 ng/mL: 30 G2: 10–30 ng/mL: 30 G3: >30 ng/mL: 30 | At the time of loading and 12 months later | 90 | Molar mandible | 100 | G1: 1.38 ± 0.33 G2: 0.89 ± 0.16 G3: 0.78 ± 0.12/RVG | - | 12 |
| Selection | Comparability | Outcome | Number of Stars (Out of 9) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Study | S1 | S2 | S3 | S4 | C1 | C2 | E1 | E2 | E3 | |
| Mangano et al., 2018 [28] | ★ | ★ | ★ | 0 | ★ | ★ | 0 | ★ | ★ | 7 |
| Tabrizi et al., 2021 [32] | ★ | ★ | ★ | 0 | ★ | ★ | 0 | 0 | ★ | 6 |
| Study | Random Sequence Generation | Allocation Concealment | Blinding of Participants and Personnel | Blinding of Outcome Assessment | Incomplete Outcome Data | Selective Reporting | Other Bias |
|---|---|---|---|---|---|---|---|
| Garg et al., 2020 [30] |  |  |  |  |  |  |  |
| Kwiatek et al., 2021 [31] |  |  |  |  |  |  |  |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bazal-Bonelli, S.; Sánchez-Labrador, L.; Cortés-Bretón Brinkmann, J.; Cobo-Vázquez, C.; Martínez-Rodríguez, N.; Beca-Campoy, T.; Santos-Marino, J.; Rodríguez-Fernández, E.; Alvarado-Lorenzo, M. Influence of Serum Vitamin D Levels on Survival Rate and Marginal Bone Loss in Dental Implants: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 10120. https://doi.org/10.3390/ijerph191610120
Bazal-Bonelli S, Sánchez-Labrador L, Cortés-Bretón Brinkmann J, Cobo-Vázquez C, Martínez-Rodríguez N, Beca-Campoy T, Santos-Marino J, Rodríguez-Fernández E, Alvarado-Lorenzo M. Influence of Serum Vitamin D Levels on Survival Rate and Marginal Bone Loss in Dental Implants: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(16):10120. https://doi.org/10.3390/ijerph191610120
Chicago/Turabian StyleBazal-Bonelli, Santiago, Luis Sánchez-Labrador, Jorge Cortés-Bretón Brinkmann, Carlos Cobo-Vázquez, Natalia Martínez-Rodríguez, Tomás Beca-Campoy, Juan Santos-Marino, Emilio Rodríguez-Fernández, and Mario Alvarado-Lorenzo. 2022. "Influence of Serum Vitamin D Levels on Survival Rate and Marginal Bone Loss in Dental Implants: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 16: 10120. https://doi.org/10.3390/ijerph191610120
APA StyleBazal-Bonelli, S., Sánchez-Labrador, L., Cortés-Bretón Brinkmann, J., Cobo-Vázquez, C., Martínez-Rodríguez, N., Beca-Campoy, T., Santos-Marino, J., Rodríguez-Fernández, E., & Alvarado-Lorenzo, M. (2022). Influence of Serum Vitamin D Levels on Survival Rate and Marginal Bone Loss in Dental Implants: A Systematic Review. International Journal of Environmental Research and Public Health, 19(16), 10120. https://doi.org/10.3390/ijerph191610120