
Subjective Experiences of Mental Health Crisis Care in Emergency Departments: A Narrative Review of the Qualitative Literature

 , ,
, ,
Abstract
1. Introduction
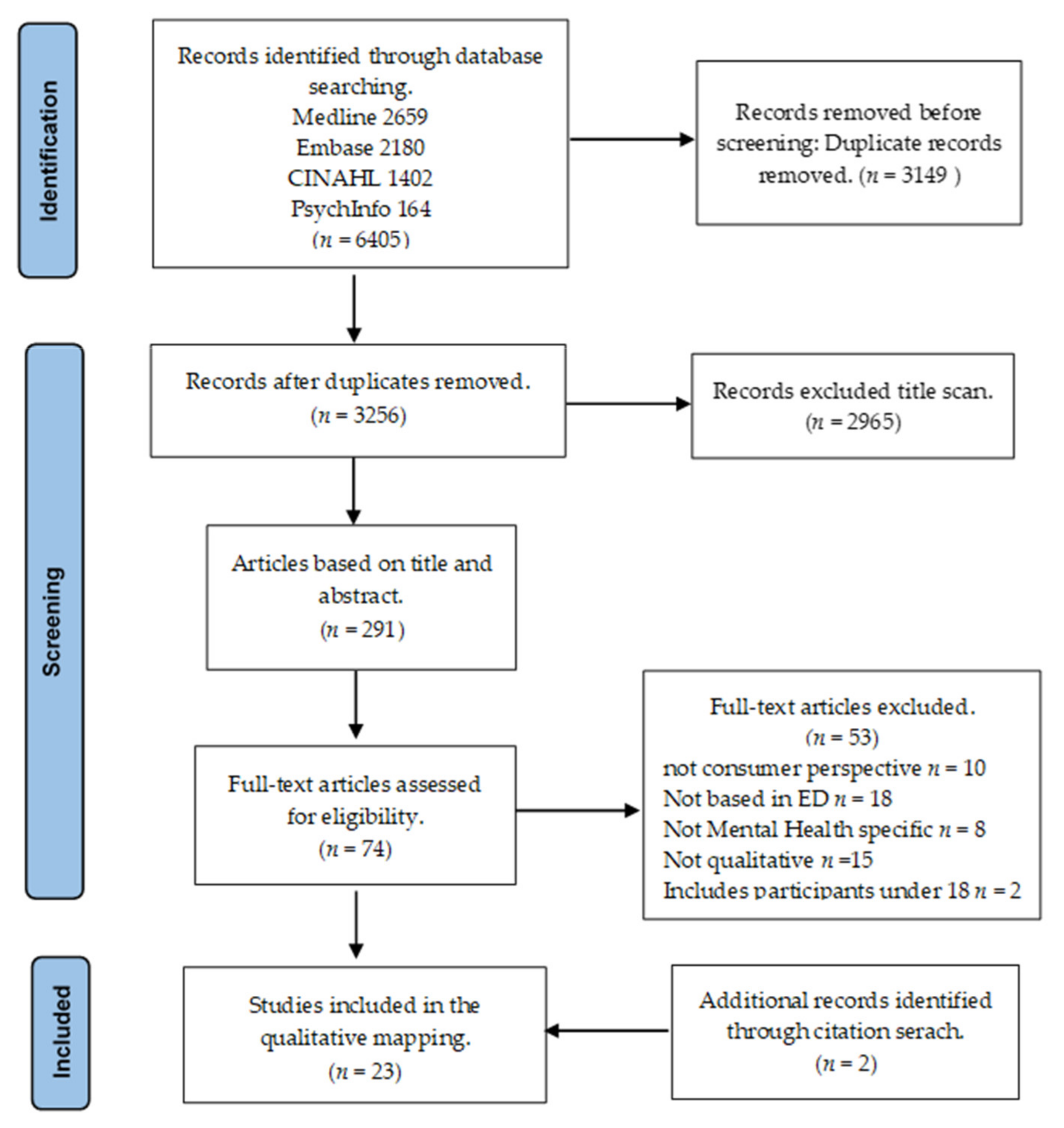
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.2.1. Study Design
2.2.2. Participants
2.2.3. Intervention
2.2.4. Comparison
2.2.5. Outcome
2.3. Study Selection and Data Extraction
3. Results
3.1. Characteristics of Studies
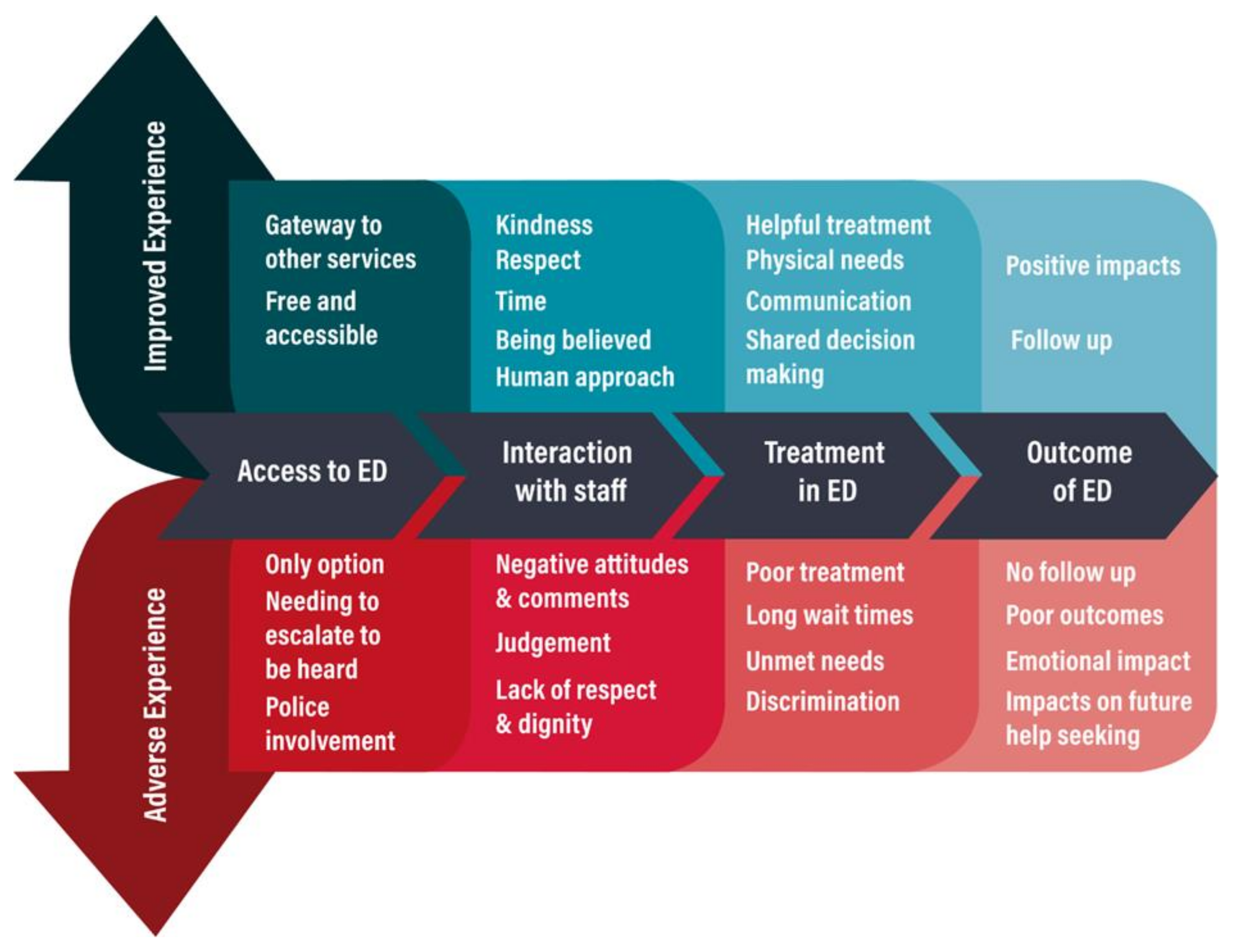
3.2. Narrative Analysis of the Subjective Experiences of People: The Journey Map of Experience in ED
3.2.1. Access to ED
ED Accessible and Appropriate
Only Option
3.2.2. Interactions with Staff
Positive Interactions with Staff
Knowledge and Expertise of Staff
Judgemental Attitudes
3.2.3. Experiences of Treatment
Positive Experiences of Treatment
Long Wait Times
Physical Space and Lack of Privacy
Unmet Needs
Poor Treatment
Discriminatory Treatment
Coercive and Restrictive Practices
3.2.4. Impact of ED
Follow up
Poor Outcomes
Negative Emotional Impact
Re-Traumatisation
Future Help-Seeking
4. Discussion
4.1. Strengths and Limitations of This Study
4.2. Implications and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Author | Year | Title | Journal | Study Design | Country | Participants | Data Collection | Data Analysis | Main Findings | Aim | Limitations/Strengths |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [67] | 2003 | What do consumers say they want and need during a psychiatric emergency? | Journal of Psychiatric Practice | Mixed methods | USA | n = 59 Participants with a diagnosis of mental illness and at least one emergency service experience involving medication, seclusion, or restraint | Survey and focus group Surveys were also conducted with mental health professionals | Thematic analysis | Mostly poor experiences with staff Variable experiences with treatment and addressing needs Adverse experiences with medication, seclusion and restraint and impact on future help-seeking | To better understand consumer experiences and preferences | More women than men Mostly Cauca-sian Length of time elapsed since ED on average eight years |
| [69] | 2002 | Patient feedback on liaison mental health care in A&E | Nursing Times | Mixed methods | UK | n = 17 Participants with experience of ED and hospital | Semi-structured interviewsUser satisfaction survey—including open-ended questions | Thematic analysis | Valued having staff with MH knowledge Variable experiences of treatment Long wait times | Explore experiences of consumers with MH liaison staff | Use of satisfac-tion survey with qualita-tive responses difficult to de-termine |
| [64] | 2005 | Service expectations and clinical characteristics of patients receiving psychiatric emergency services | Psychiatric Services | Mixed methods | USA | n = 82 Participants with previous admissions | Self-report survey | Content analysis | A mismatch between consumers expecta-tions and services available in ED | Explore the use of the psychiatric emergency department and expectations of services availa-ble in the emer-gency department | Unique survey form and grouping of content for analysis of open-ended questions |
| [52] | 2006 | Consumer and family experiences in the emergency department following a suicide attempt | Journal of psychiatric practice | Mixed methods | USA | n = 465 Participants who had visited the ED following a suicide attempt. Family members (n = 254) members | Surveys Separate anonymous surveys were created for two groups. Survey had mostly yes/no responses with one open-ended question | Thematic analysis of the open-ended question | Long wait times Mixed results re-garding interactions with staff Suicide attempts were not taken seriously Cultural needs not always addressed Did not feel listened to or provided with information | To understand the separate experiences of consumers and family members in the Emergency Department following a suicide attempt | Focus on sui-cide attempts Unable to compare sur-vey results between con-sumers and carers Majority female Majority Cau-casian |
| [68] | 2007 | Emergency department from the mental health client’s perspective | International Journal of Mental Health Nursing | Qualitative | Canada | n = 27 Participants (consumers) Family members (n = 7) and stakeholders (n = 5) | Focus groups (separate focus groups for consumers) | Thematic analysis | ED was the only option Long wait times Discriminatory treatment Lack of privacy Physical and basic needs not met Importance of the relationship with staff The criminalisation of mental health | To determine consumer and their family satisfaction with care received in ED | Participants self-selected Most had numerous experiences of ED Lack of diversity of culture and from regional areas Emphasis on the role of the PEN |
| [53] | 2018 | Exploring the experiences of persons who frequently visit the emergency department for mental health-related reasons | Qualitative Health Research | Qualitative | Canada | n = 10 Participants who had 12+ ED visits within a 1-year time frame | Interviews | Thematic analysis using | ED was appropriate and unavoidable Participants felt dis-missed Prejudicial treatment Physical complaints legitimised the ED visit Lack of follow up Being known was both positive and negative Variable experience with staff Seeking connection | Explore the experiences of persons who frequently visit the emergency department (ED) for mental health-related reasons | Focus on fre-quent presenters Small sample size. Varying times since accessing ED Majority diagnosed with BPD; also co-occurring substance use disorder |
| [59] | 2006 | Service users and other stakeholders’ evaluation of a liaison mental health service in an accident and emergency department and a general hospital setting | Journal of Psychiatric and Mental Health Nursing | Qualitative | UK | n = 17 Participants (consumers) Professionals (n = 30). Professional stakeholders include A&E nurses, community M.H. professional and police | Interviews | Thematic content analysis | MH nurse improved ED experience Discomfort with phys-ical environment of ED | Explore what is important to service users and professional stakeholders in the provision of ED service | Random sam-pling, but small sample size Emphasis on the role of the MH liaison nurse Included first- time presenta-tions |
| [63] | 2019 | Satisfaction with emergency departments and other mental health services among patients with mental disorders | Healthcare Policy | Mixed Methods | Canada | n = 328 Participants who had presented to ED. | Surveys (standardised and qualitative items) and Interviews | Convergent mixed methods design integrating qualitative and quantitative data simultaneously | Variable experiences with staff and treatment Participants valued empathy and listening Lack of comfort and security in ED | Use and satisfaction with ED services | It included four models of ED Large sample size Integrative analysis Interview questions not provided |
| [51] | 2004 | Satisfaction with psychiatric services in the emergency department | Healthcare Policy | Mixed methods | Australia | n = 180 Participants who have presented to ED | Telephone interviews | Thematic analysis | High level of satisfac-tion with treatment in ED Long wait times Preference for staff with MH knowledge Inappropriate com-ments or treatment Chaotic environment in ED | Evaluation of people’s perceptions of and satisfaction with ED services | Large sample sizeSecondary analysis |
| [61] | 2016 | Patients’ experiences of psychiatric care in emergency departments: A secondary analysis | International Emergency Nursing | Qualitative Phenomenological method | USA | n = 9 Participants with a diagnosis of mental illness and previous experience accessing ED | Interviews and focus groups | Thematic analysis | Cold, clinical, and cha-otic physical environ-ment in ED Discriminatory treat-ment and feeling judged Loss of freedom Lack of privacy Long wait times Wanting staff with MH knowledge Mitigating effect of pos-itive interactions with staff | The primary aim is to describe the perceptions of ED visits by individuals experiencing a mental health crisis and identify themes to improve outcomes in ED settings | Secondary and comparative analysis of people who had also accessed an alternative to ED |
| [57] | 2015 | Patients with mental health issues in the emergency department: The relationship between coercion and perceptions of being helped, psychologically hurt and physically harmed | International Journal of Forensic Mental Health | Mixed methods | Canada | n = 49 Participants in an inpatient unit shortly after being triaged from the emergency department. Most involuntarily committed | Interviews Paper and pencil survey Likert and with open-ended questions | Thematic analysis of interview data | Mixed perceptions of treatment Lacking freedom Long wait times Importance of choice and shared decision making Treated differently Harmed by treatment | The aim was to understand how consumers perceived their experiences in the ED | Sampling bias, some people refused to participate because of the possible re-traumatisation Participants had all been transferred to the inpatient following ED presentation Most involun-tarily admis-sions |
| [70] | 2019 | To receive the patient in crisis with psychiatric emergencies: study of subjective experience | Medico-psychological Annals, psychiatric journal | Qualitative | Belgium | n = 12 Participants in ED | Semi-structured interviews | Thematic analysis | Waiting room was not welcoming Valued human and relational qualities of ED staff | To understand the subjective experience of patients of the waiting room | 10 were first-time presentations |
| [66] | 2012 | Managing people with mental health presentations in emergency departments-a service exploration of the issues surrounding responsiveness from a mental health care consumer and carer perspective | Australasian Emergency Journal | mixed methods | Australia | n = 65 Survey n= 8 Focus group Participants who had utilised ED MH services in the previous six months and their families | Surveys and focus groups | Thematic analysis | ED necessary and ap-propriate Valued staff with MH knowledge Variable interactions with staff and treat-ment Unmet needs Long wait times Negative experiences in ED environment and wanting a separate MH space | Explore MH care in the ED specifically in relation to access and management | Small sample size in focus group Majority of participants female Limitations of satisfaction and dichotomous scaling Included consumers and carers Majority female |
| [71] | 2009 | Patient satisfaction with an emergency department psychiatric service | International Journal of Health Care Quality Assurance | Mixed methods | UK | n = 55 Participants who attended the ED | The Client Satisfaction Questionnaire Included two open-ended questions | Descriptive/thematic analysis | Variable experiences of staff and treatment Long wait times Lack of options Lack of information Communication | To measure the satisfaction of an emergency department psychiatric service | The response rate was low Only two open ended questions Positive bias in questions |
| [50] | 2002 | The quality of psychiatric services provided by an Australian tertiary hospital emergency department: a client perspective | Accident and Emergency Nursing | Mixed methods | Australia | n= 136 Participants who had to ED in the past six months | Telephone interviews | Thematic analysis | High level of satisfac-tion with service pro-vided by staff but some highly negative expe-riences Valued staff with MH knowledge | Evaluation of the inclusion of psychiatric nurse consultants | Focus on role of nurse consultants. Secondary analysis |
| [49] | 2003 | Patient satisfaction with psychiatric services | Journal of Psychiatric and Mental Health Nursing | Mixed methods | Australia | n= 136 Participants who had presented to the ED | Qualitative telephone interviews Structured questionnaire | Thematic/content coding of interview data | High level of satisfaction Valued staff with MH knowledge Long wait times Lack of privacy Inappropriate staff comments | Measure satisfaction with psychiatric services provided in a general ED | Results repre-sent same study by au-thors Secondary analysis |
| [62] | 2018 | Patient-centered values and experiences with emergency department and mental health crisis care | Administration and Policy in Mental Health | Qualitative | USA | n = 27 Participants who had received both psychiatric crisis care and community mental health services | Focus groups (n = 3) | Values-based coding | Not having basic needs met Negative experiences of involuntary treatment Valued communication and kindness Mitigating effect of positive staff interactions Valued shared decision making Wanted a quiet physical space | Explore consumers experiences and values about psychiatric care | A comparative study, some participants had received care in both ED and an alternative |
| [55] | 2019 | Why go to the emergency department? Perspectives from persons with borderline personality disorder | International Journal of Mental Health Nursing | Qualitative | Canada | n = 6 Participants diagnosed with borderline personality disorder with at least 12 ED visits with one year | Interviews | Thematic coding | ED was the only option Negative and discrim-inatory treatment Seeking connection Emotional impact of negative treatment | Understand the reasons why people with BPD go to the emergency and the perspective of persons with BPD | Focus on people with a diagnosis of BPD Small sample size Not generalisable Mostly women |
| [60] | 2006 | Consumer evaluation of a mental health liaison nurse service in the emergency department | Contemporary Nurse | Mixed-Method | Australia | n = 59 Participants who had accessed ED who had involvement with the M.H. liaison nurse while they were in the ED | phone survey/interviews | Coding | More positive experi-ence associated with having specialised MH staff MH nurses valued | Perceptions of treatment in ED | Focus on MHN One site. Limitations of satisfaction surveys. |
| [65] | 2020 | An inevitable response? A lived experience perspective on emergency responses to mental health crisis | Journal of Psychiatric Mental Health Nursing | A narrative account of personal experience | UK | n = 1 The individual experience of the author | Case study | Narrative analysis | Psychiatric pain is re-sponded to differently to physical pain Discriminatory treat-ment Criminalisation of MH | A narrative account of emergency pathways during psychiatric distress and potential impacts | Single individual Case study design |
| [54] | 2017 | “Hospital was the only option”: Experiences of frequent emergency department users in mental health | Administration and Policy in Mental Health | Mixed methods | USA | n = 20 Participants with diagnosis MI and addictions who frequently present to ED self-reported quantitative survey (n = 166) | In depth interviews survey | Thematic analysis | ED as appropriate/only option Mismatch of expecta-tions Discriminatory and unsatisfactory treat-ment Lack of follow up | To understand the experiences of service users who frequently present to ED | Frequent presentations to ED Includes an intervention group and treatment as usual |
| [58] | 2020 | Experiences of individuals who were physically restrained in the emergency department | JAMA Network Open | Qualitative | USA | n = 25 Participants who had been restrained in the ED | In-depth interviews | Thematic analysis | Harmful experiences of restraint Negative experiences with staff Lasting negative con-sequences of restraint | To characterise how individuals experience episodes of physical restraint during their ED visits | Majority male |
| [56] | 2017 | Don’t label me: A qualitative study of patients’ perceptions and experiences of sedation during behavioural emergencies in the emergency department. | Academic Emergency Medicine | Qualitative | Australia | n = 13 Participants who had received parenteral sedative medication | Face to face semi-structured interviews | Thematic analysis | Variable experiences of treatment Trust in staff Sedation seen as neces-sary Treated like a human being was important Long wait times led to distress Lack of debriefing and follow up Lack of information | Explore the perceptions and experiences of patients regarding the use of sedation during a mental health crisis | Small sample sizeConvenience sample Included par-ticipants who presented for the first time |
References
- Akther, S.F.; Molyneaux, E.; Stuart, R.; Johnson, S.; Simpson, A.; Oram, S. Patients’ experiences of assessment and detention under mental health legislation: Systematic review and qualitative meta-synthesis. BJPsych Open 2019, 5, e37. [Google Scholar] [CrossRef]
- Henderson, J. Neo-liberalism, community care and Australian mental health policy. Health Sociol. Rev. 2005, 14, 242–254. [Google Scholar] [CrossRef]
- Shen, G.C.; Eaton, J.; Snowden, L. Mainstreaming Mental Health Care in 42 Countries. Health Syst. Reform 2017, 3, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Marynowski-Traczyk, D.; Moxham, L.; Broadbent, M. A critical discussion of the concept of recovery for mental health consumers in the Emergency Department. Australas. Emerg. Nurs. J. 2013, 16, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Roggenkamp, R.; Andrew, E.; Nehme, Z.; Cox, S.; Smith, K. Descriptive Analysis of Mental Health-Related Presentations To Emergency Medical Services. Prehospital Emerg. Care 2018, 22, 399–405. [Google Scholar] [CrossRef]
- Larkin, G.L.; Beautrais, A.L.; Spirito, A.; Kirrane, B.M.; Lippmann, M.J.; Milzman, D. Mental Health and Emergency Medicine: A Research Agenda. Acad. Emerg. Med. 2009, 16, 1110–1119. [Google Scholar] [CrossRef] [PubMed]
- American College of Emergency Physicians. Mental Health Advocacy. Available online: https://www.acep.org/federal-advocacy/mental-health/ (accessed on 19 March 2020).
- Australian Institute of Health and Welfare. Emergency Department Care 2016–2017: Australian Hospital Statistics; AIHW: Canberra, Australia, 2017. [Google Scholar]
- Capp, R.; Hardy, R.; Lindrooth, R.; Wiler, J. National Trends in Emergency Department Visits by Adults with Mental Health Disorders. J. Emerg. Med. 2016, 51, 131–135.e1. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Mental Health Services in Australia; Australian Institute of Health and Welfare: Canberra, Australia, 2021. [Google Scholar]
- Barratt, H.; García, A.R.; Clarke, K.; Moore, A.; Whittington, C.; Stockton, S.; Thomas, J.; Pilling, S.; Raine, R. Epidemiology of Mental Health Attendances at Emergency Departments: Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0154449. [Google Scholar] [CrossRef] [PubMed]
- Theriault, K.M.; Rosenheck, R.A.; Rhee, T.G. Increasing Emergency Department Visits for Mental Health Conditions in the United States. J. Clin. Psychiatry 2020, 81, 20m13241. [Google Scholar] [CrossRef] [PubMed]
- Care Quality Commission. Right Here, Right Now: People’s Experiences of Help, Care and Support. During a Mental Health Crisis; Care Quality Commission: London, UK, 2015. [Google Scholar]
- Ceniti, A.K.; Heinecke, N.; McInerney, S.J. Examining suicide-related presentations to the emergency department. Gen. Hosp. Psychiatry 2018, 63, 152–157. [Google Scholar] [CrossRef]
- Nordstrom, K.; Berlin, J.S.; Nash, S.S.; Shah, S.B.; Schmelzer, N.A.; Worley, L.L. Boarding of Mentally Ill Patients in Emergency Departments: American Psychiatric Association Resource Document. West. J. Emerg. Med. 2019, 20, 690–695. [Google Scholar] [CrossRef] [PubMed]
- Nicks, B.A.; Manthey, D.M. The Impact of Psychiatric Patient Boarding in Emergency Departments. Emerg. Med. Int. 2012, 2012, 360308. [Google Scholar] [CrossRef] [PubMed]
- Appelbaum, P.S. “Boarding” Psychiatric Patients in Emergency Rooms: One Court Says “No More”. Psychiatr. Serv. 2015, 66, 668–670. [Google Scholar] [CrossRef] [PubMed]
- Australasian College for Emergency Medicine. The Long Wait: An Analysis of Mental Health Presentations to Australian Emergency Departments. 2018. Available online: https://acem.org.au/getmedia/60763b10-1bf5-4fbc-a7e2-9fd58620d2cf/ACEM_report_41018 (accessed on 12 October 2020).
- Allison, S.; Bastiampillai, T.; O’Reilly, R.; Sharfstein, S.S.; Castle, D. Widespread emergency department access block: A human rights issue in Australia? Australas. Psychiatry 2019, 27, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Knott, J.; Gerdtz, M.; Dobson, S.; Daniel, C.; Graudins, A.; Mitra, B.; Bartley, B.; Chapman, P. Restrictive interventions in Victorian emergency departments: A study of current clinical practice. Emerg. Med. Australas. 2019, 32, 393–400. [Google Scholar] [CrossRef]
- McKenna, B.; Furness, T.; Maguire, T. A Literature Review and Policy Analysis on the Practice of Restrictive Interventions; State of Victoria Department of Health and Human Services: Melbourne, Australia, 2014. [Google Scholar]
- HMICFRS. Policing and Mental Health Picking Up the Pieces. 2018. Available online: https://www.justiceinspectorates.gov.uk/hmicfrs/wp-content/uploads/policing-and-mental-health-picking-up-the-pieces.pdf (accessed on 4 September 2020).
- Waldemar, A.K.; Arnfred, S.M.; Petersen, L.; Korsbek, L. Recovery-Oriented Practice in Mental Health Inpatient Settings: A Literature Review. Psychiatr. Serv. 2016, 67, 596–602. [Google Scholar] [CrossRef]
- Van Weeghel, J.; van Zelst, C.; Boertien, D.; Hasson-Ohayon, I. Conceptualizations, assessments, and implications of personal recovery in mental illness: A scoping review of systematic reviews and meta-analyses. Psychiatr. Rehabil. J. 2019, 42, 169. [Google Scholar] [CrossRef] [PubMed]
- Le Boutillier, C.; Leamy, M.; Bird, V.; Davidson, L.; Williams, J.; Slade, M. What Does Recovery Mean in Practice? A Qualitative Analysis of International Recovery-Oriented Practice Guidance. Psychiatr. Serv. 2011, 62, 1470–1476. [Google Scholar] [CrossRef] [PubMed]
- Oades, L.G.; Anderson, J. Recovery in Australia: Marshalling strengths and living values. Int. Rev. Psychiatry 2012, 24, 5–10. [Google Scholar] [CrossRef]
- Martinelli, A.; Ruggeri, M. An overview of mental health recovery-oriented practices: Potentiality, challenges, prejudices, and misunderstandings. J. Psychopathol. 2020, 26, 147–154. [Google Scholar]
- Deacon, B.J. The biomedical model of mental disorder: A critical analysis of its validity, utility, and effects on psychotherapy research. Clin. Psychol. Rev. 2013, 33, 846–861. [Google Scholar] [CrossRef]
- Davidson, L. A Key, not a Straitjacket: The Case for Interim Mental Health Legislation Pending Complete Prohibition of Psychiatric Coercion in Accordance with the Convention on the Rights of Persons with Disabilities. Health Hum. Rights 2020, 22, 163. [Google Scholar]
- Boscarato, K.; Lee, S.J.; Kroschel, J.; Hollander, Y.; Brennan, A.; Warren, N. Consumer experience of formal crisis-response services and preferred methods of crisis intervention. Int. J. Ment. Health Nurs. 2014, 23, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Carstensen, K.; Lou, S.; Jensen, L.G.; Nissen, N.K.; Ortenblad, L.; Pfau, M.; Ankersen, P.V. Psychiatric service users’ experiences of emergency departments: A CERQual review of qualitative studies. Nord. J. Psychiatry 2017, 71, 315–323. [Google Scholar] [CrossRef]
- Hobbs, M. Crisis intervention in theory and practice: A selective review. Br. J. Med. Psychol. 1984, 57, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Ball, J.S.; Links, P.S.; Strike, C.; Boydell, K. “It’s overwhelming. Everything seems to be too much”: A theory of crisis for individuals with severe persistent mental illness. Psychiatr. Rehabil. J. 2005, 29, 10–17. [Google Scholar] [CrossRef]
- Borschmann, R.; Henderson, C.; Hogg, J.; Phillips, R.; Moran, P. Crisis interventions for people with borderline personality disorder. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Colquhoun, H. Current Best Practices for the Conduct of Scoping Reviews. 2016. Available online: https://www.equator-network.org/wp-content/uploads/2016/06/Gerstein-Library-scoping-reviews_May-12.pdf (accessed on 20 May 2020).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Mays, N.; Pope, C.; Popay, J. Systematically reviewing qualitative and quantitative evidence to inform management and policy-making in the health field. J. Health Serv. Res. Policy 2005, 10, 6–20. [Google Scholar] [CrossRef] [PubMed]
- Zomerdijk, L.G.; Voss, C. Service Design for Experience-Centric Services. J. Serv. Res. 2009, 13, 67–82. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Perreault, M.; Pawliuk, N.; Veilleux, R.; Rousseau, M. Qualitative Assessment of Mental Health Service Satisfaction: Strengths and Limitations of a Self-Administered Procedure. Community Ment. Health J. 2006, 42, 233–242. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Coyle, J.; Healy, D. The meaning of patient satisfaction: An explanation of high reported levels. Soc. Sci. Med. 1998, 47, 1351–1359. [Google Scholar] [CrossRef]
- Thomas, D. A General Inductive Approach for Analyzing Qualitative Evaluation Data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Glaser, B.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine: Chicago, IL, USA, 1967; pp. 2–6. [Google Scholar]
- DeSantis, L.; Ugarriza, D.N. The concept of theme as used in qualitative nursing research. West. J. Nurs. Res. 2000, 22, 351–372. [Google Scholar] [CrossRef] [PubMed]
- Ryan, G.W.; Bernard, H.R. Techniques to Identify Themes. Field Methods 2003, 15, 85–109. [Google Scholar] [CrossRef]
- Samson, S.; Granath, K.; Alger, A. Journey Mapping the User Experience. Coll. Res. Libr. 2017, 78, 459. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Summers, M.; Happell, B. Patient satisfaction with psychiatric services provided by a Melbourne tertiary hospital emergency department. J. Psychiatr. Ment. Health Nurs. 2003, 10, 351–357. [Google Scholar] [CrossRef]
- Summers, M.; Happell, B. The quality of psychiatric services provided by an Australian tertiary hospital emergency department: A client perspective. Accid. Emerg. Nurs. 2002, 10, 205–213. [Google Scholar] [CrossRef]
- Happell, B.; Summers, M. Satisfaction with psychiatric services in the emergency department. Int. Psychiatry 2004, 1, 3–4. [Google Scholar] [CrossRef][Green Version]
- Cerel, J.; Currier, G.W.; Conwell, Y. Consumer and Family Experiences in the Emergency Department Following a Suicide Attempt. J. Psychiatr. Pr. 2006, 12, 341–347. [Google Scholar] [CrossRef] [PubMed]
- VanDyk, A.D.; Young, L.; Macphee, C.; Gillis, K. Exploring the Experiences of Persons Who Frequently Visit the Emergency Department for Mental Health-Related Reasons. Qual. Health Res. 2017, 28, 587–599. [Google Scholar] [CrossRef]
- Wise-Harris, D.; Pauly, D.; Kahan, D.; De Bibiana, J.T.; Hwang, S.W.; Stergiopoulos, V. “Hospital was the Only Option”: Experiences of Frequent Emergency Department Users in Mental Health. Adm. Policy Ment. Health Ment. Health Serv. Res. 2016, 44, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Vandyk, A.; Bentz, A.; Bissonette, S.; Cater, C. Why go to the emergency department? Perspectives from persons with borderline personality disorder. Int. J. Ment. Health Nurs. 2019, 28, 757–765. [Google Scholar] [CrossRef]
- Yap, C.Y.L.; Knott, J.C.; Kong, D.C.M.; Gerdtz, M.; Stewart, K.; Taylor, D.M. Don’t Label Me: A Qualitative Study of Patients’ Perceptions and Experiences of Sedation During Behavioral Emergencies in the Emergency Department. Acad. Emerg. Med. 2017, 24, 957–967. [Google Scholar] [CrossRef] [PubMed]
- Harrison, N.; Mordell, S.; Roesch, R.; Watt, K. Patients with Mental Health Issues in the Emergency Department: The Relationship Between Coercion and Perceptions of Being Helped, Psychologically Hurt, and Physically Harmed. Int. J. Forensic Ment. Health 2015, 14, 161–171. [Google Scholar] [CrossRef]
- Wong, A.H.; Ray, J.M.; Rosenberg, A.; Crispino, L.; Parker, J.; McVaney, C.; Iennaco, J.D.; Bernstein, S.L.; Pavlo, A.J. Experiences of Individuals Who Were Physically Restrained in the Emergency Department. JAMA Netw. Open 2020, 3, e1919381. [Google Scholar] [CrossRef]
- Eales, S.; Callaghan, P.; Johnson, B. Service users and other stakeholders’ evaluation of a liaison mental health service in an accident and emergency department and a general hospital setting. J. Psychiatr. Ment. Health Nurs. 2006, 13, 70–77. [Google Scholar] [CrossRef]
- Wand, T.; Schaecken, P. Consumer evaluation of a mental health liaison nurse service in the Emergency Department. Contemp. Nurse 2006, 21, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Harris, B.; Beurmann, R.; Fagien, S.; Shattell, M. Patients’ experiences of psychiatric care in emergency departments: A secondary analysis. Int. Emerg. Nurs. 2015, 26, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.C.; Owino, H.; Ansari, S.; Adams, L.; Cyr, J.M.; Gaynes, B.N.; Glickman, S.W. Patient-Centered Values and Experiences with Emergency Department and Mental Health Crisis Care. Adm. Policy Ment. Health Ment. Health Serv. Res. 2018, 45, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Fleury, M.-J.; Grenier, G.; Farand, G.G.A.L. Satisfaction with Emergency Departments and Other Mental Health Services among Patients with Mental Disorders. Health Policy 2019, 14, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, L.L.; Schecter, J.M.; Underwood, J.A.; Tyrka, A.R.; Price, L.H. Service Expectations and Clinical Characteristics of Patients Receiving Psychiatric Emergency Services. Psychiatr. Serv. 2005, 56, 743–745. [Google Scholar] [CrossRef]
- White, C.J. An inevitable response? A lived experienced perspective on emergency responses to mental health crises. J. Psychiatr. Ment. Health Nurs. 2020, 28, 90–93. [Google Scholar] [CrossRef]
- Morphet, J.; Innes, K.; Munro, I.; O’Brien, A.; Gaskin, C.J.; Reed, F.; Kudinoff, T. Managing people with mental health presentations in emergency departments—A service exploration of the issues surrounding responsiveness from a mental health care consumer and carer perspective. Australas. Emerg. Nurs. J. 2012, 15, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.H.; Carpenter, D.; Sheets, J.L.; Miccio, S.; Ross, R. What do consumers say they want and need during a psychiatric emergency? J. Psychiatr. Pract. 2003, 9, 39–58. [Google Scholar] [CrossRef] [PubMed]
- Clarke, D.E.; Dusome, D.; Hughes, L. Emergency department from the mental health client’s perspective. Int. J. Ment. Health Nurs. 2007, 16, 126–131. [Google Scholar] [CrossRef]
- Callaghan, P.; Eales, S.; Coats, T.; Bowers, L.; Bunker, J. Patient feedback on liaison mental health care in A&E. Nurs. Times 2002, 98, 34–36. [Google Scholar]
- Meriaux, M.; Denis, J.; Michel, V.; Hendrick, S. To receive the patient in crisis in psychiatric emergencies: Subjective experience study. Ann. Med.-Psychol. 2019, 177, 526–533. [Google Scholar]
- O’Regan, C.; Ryan, M. Patient satisfaction with an emergency department psychiatric service. Int. J. Health Care Qual. Assur. 2009, 22, 525–534. [Google Scholar] [CrossRef]
- Duggan, M.; Harris, B.; Chislett, W.-K.; Calder, R. Nowhere Else to Go: Why Australia’s Health System Results in People with Mental Illness Getting ‘Stuck’ in Emergency Departments. 2020. Available online: https://www.vu.edu.au/sites/default/files/nowhere-else-to-go-people-mental-illness-stuck-emergency-departments-report-mitchell-institute.pdf. (accessed on 2 June 2020).
- Unwin, M.; Crisp, E.; Stankovich, J.; McCann, D.; Kinsman, L. Socioeconomic disadvantage as a driver of non-urgent emergency department presentations: A retrospective data analysis. PLoS ONE 2020, 15, e0231429. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, N.; Savic, M.; McCann, T.V.; Emond, K.; Sandral, E.; Smith, K.; Roberts, L.; Bosley, E.; Lubman, D.I. “I was worried if I don’t have a broken leg, they might not take it seriously”: Experiences of men accessing ambulance services for mental health and/or alcohol and other drug problems. Health Expect. 2019, 22, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Repper, J. The deserving and the undeserving: Selectivity and progress in a community care service. J. Ment. Health 1995, 4, 483–498. [Google Scholar] [CrossRef]
- Olthuis, G.; Prins, C.; Smits, M.-J.; van de Pas, H.; Bierens, J.; Baart, A. Matters of Concern: A Qualitative Study of Emergency Care from the Perspective of Patients. Ann. Emerg. Med. 2014, 63, 311–319.e2. [Google Scholar] [CrossRef]
- Innes, K.; Morphet, J.; O’Brien, A.P.; Munro, I. Caring for the mental illness patient in emergency departments–an exploration of the issues from a healthcare provider perspective. J. Clin. Nurs. 2014, 23, 2003–2011. [Google Scholar] [CrossRef]
- Broadbent, M.; Moxham, L.; Dwyer, T. Implications of the emergency department triage environment on triage practice for clients with a mental illness at triage in an Australian context. Australas. Emerg. Nurs. J. 2014, 17, 23–29. [Google Scholar] [CrossRef]
- Gulrajani, R. Physical environmental factors affecting factors affecting patients’ stress in the accident and emergency department. Accid. Emerg. Nurs. 1995, 3, 22–27. [Google Scholar] [CrossRef]
- Greenfield, T.K.; Stoneking, B.C.; Humphreys, K.; Sundby, E.; Bond, J. A Randomized Trial of a Mental Health Consumer-Managed Alternative to Civil Commitment for Acute Psychiatric Crisis. Am. J. Community Psychol. 2008, 42, 135–144. [Google Scholar] [CrossRef]
- Kerrison, S.A.; Chapman, R. What general emergency nurses want to know about mental health patients presenting to their emergency department. Accid. Emerg. Nurs. 2007, 15, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Ray, J.D.; Overman, A.S. Hard facts about soft skills. AJN Am. J. Nurs. 2014, 114, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Kumble, S.; McSherry, B. Seclusion and restraint: Rethinking regulation from a human rights perspective. Psychiatry Psychol. Law 2010, 17, 551–561. [Google Scholar] [CrossRef]
- WHO. Guidance on Community Mental Health Services: Promoting Person-Centred and Rights-Based Approaches; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Al-Maraira, O.A.; Hayajneh, F.A. Use of Restraint and Seclusion in Psychiatric Settings: A Literature Review. J. Psychosoc. Nurs. Ment. Health Serv. 2019, 57, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Brophy, L.M.; Roper, C.E.; Hamilton, B.E.; Tellez, J.J.; McSherry, B.M. Consumers and their supporters’ perspectives on poor practice and the use of seclusion and restraint in mental health settings: Results from Australian focus groups. Int. J. Ment. Health Syst. 2016, 10, 6. [Google Scholar] [CrossRef]
- Bombard, Y.; Baker, G.R.; Orlando, E.; Fancott, C.; Bhatia, P.; Casalino, S.; Onate, K.; Denis, J.-L.; Pomey, M.-P. Engaging patients to improve quality of care: A systematic review. Implement. Sci. 2018, 13, 98. [Google Scholar] [CrossRef]
- Australian Government Department of Health and Ageing. National Mental Health Report 2013: Tracking Progress of Mental Health Reform in Australia 1993–2011; Australian Government Department of Health and Ageing: Canberra, Australia, 2013. [Google Scholar]
- Hall, A.E.; Bryant, J.; Sanson-Fisher, R.; Fradgley, E.A.; Proietto, A.M.; Roos, I. Consumer input into health care: Time for a new active and comprehensive model of consumer involvement. Health Expect. 2018, 21, 707–713. [Google Scholar] [CrossRef]
- National Mental Health Commission. Monitoring Mental Health and Suicide Prevention Reform: National Report 2019; National Mental Health Commission: Sydney, Australia, 2019. [Google Scholar]
- NHS. NHS Mental Health Implementation Plan. 2019/20-2023/24; NHS: London, UK, 2019. [Google Scholar]


| Person/Population AND | Subjective Experience AND | Characteristic AND | Environment |
|---|---|---|---|
| Consumer * or “service user *” or patient * or client * | experience * or subjective or perception * or perspective * or qualitative or preference * or satisfaction | psychiatric * or “mental health” or “mental Illness” or “mental health crisis” or psychological* or “mental disorder” or “emotional trauma” or “psychological trauma” or “emotional distress” or “psychological distress” or “mental distress” or suicidal or “suicide attempt” or “self-harm” or “substance use” or “substance abuse | “emergency department *” or “emergency service *” or “accident and emergency” or ambulance or police |
| Theme | N Studies | Studies |
|---|---|---|
| Access to ED | ||
| Accessible and appropriate | 10 | [50,53,54,55,61,63,65,66,67,68] |
| Only option | 13 | [53,54,55,57,58,61,63,65,66,67,68,70,71] |
| Interactions with staff | ||
| Positive interactions with staff | 14 | [49,50,51,53,59,60,62,63,66,67,68,69,70,71] |
| Knowledge and expertise | 9 | [50,51,59,60,63,66,68,69,71] |
| Judgemental attitudes | 14 | [50,52,53,54,55,60,61,63,64,65,67,68,70,71] |
| The mitigating effect of staff | 9 | [49,50,52,56,57,59,62,63,67,70] |
| Experience of treatment | ||
| Wait times | 18 | [50,51,52,54,55,56,57,58,59,61,63,65,66,67,68,69,70,71] |
| Poor and inadequate treatment | 16 | [51,52,53,54,55,56,58,59,61,62,63,64,65,67,68,70] |
| Positive experiences of treatment | 6 | [50,51,57,63,64,66] |
| Discriminatory treatment | 15 | [50,52,53,55,56,58,59,60,61,62,65,67,68,70,71] |
| Unmet needs | 11 | [50,51,55,59,63,65,66,67,68,70,71] |
| Restrictive practices | 8 | [52,53,56,58,61,62,65,67] |
| Privacy | 14 | [49,50,51,53,59,61,62,63,66,67,68,69,70,71] |
| Physical environment | 10 | [50,57,59,61,62,65,67,68,70,71] |
| Outcome of ED | ||
| Poor outcomes | 7 | [53,58,59,65,68,70,71] |
| Negative emotional impact | 8 | [50,52,54,56,57,59,66,68] |
| Impact on future help-seeking | 3 | [61,62,67] |
| Positive outcomes | 3 | [50,51,57] |
| Follow Up | 15 | [50,51,52,55,58,59,61,62,63,65,66,68,69,70,71] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roennfeldt, H.; Wyder, M.; Byrne, L.; Hill, N.; Randall, R.; Hamilton, B. Subjective Experiences of Mental Health Crisis Care in Emergency Departments: A Narrative Review of the Qualitative Literature. Int. J. Environ. Res. Public Health 2021, 18, 9650. https://doi.org/10.3390/ijerph18189650
Roennfeldt H, Wyder M, Byrne L, Hill N, Randall R, Hamilton B. Subjective Experiences of Mental Health Crisis Care in Emergency Departments: A Narrative Review of the Qualitative Literature. International Journal of Environmental Research and Public Health. 2021; 18(18):9650. https://doi.org/10.3390/ijerph18189650
Chicago/Turabian StyleRoennfeldt, Helena, Marianne Wyder, Louise Byrne, Nicole Hill, Rory Randall, and Bridget Hamilton. 2021. "Subjective Experiences of Mental Health Crisis Care in Emergency Departments: A Narrative Review of the Qualitative Literature" International Journal of Environmental Research and Public Health 18, no. 18: 9650. https://doi.org/10.3390/ijerph18189650
APA StyleRoennfeldt, H., Wyder, M., Byrne, L., Hill, N., Randall, R., & Hamilton, B. (2021). Subjective Experiences of Mental Health Crisis Care in Emergency Departments: A Narrative Review of the Qualitative Literature. International Journal of Environmental Research and Public Health, 18(18), 9650. https://doi.org/10.3390/ijerph18189650