
Thromboembolism and Bleeding in COVID-19


Radboud University Medical Center, 6500 HB Nijmegen, The Netherlands
J 2021, 4(3), 476-485; https://doi.org/10.3390/j4030036
Submission received: 1 July 2021
/
Revised: 23 August 2021
/
Accepted: 25 August 2021
/
Published: 26 August 2021
(This article belongs to the Section Medicine & Pharmacology)
{kind=link}
Abstract
:Coronavirus disease 2019 (COVID-19) is characterized by a coagulation dysfunction which has different underlying mechanisms and factors. Patients with severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2) infection have an increased risk for thromboembolic and bleeding complications. Incidences are high, and mainly consist of venous thromboembolism (VTE), which significantly contributes to morbidity and mortality in affected patients. Thromboprophylaxis is recommended in all hospitalized COVID-19 patients. Therapeutic doses of antithrombotic agents are only beneficial in noncritically ill patients, and usual care thromboprophylaxis is sufficient in critically ill patients at the ICU. Regarding screening for VTE, high quality evidence is warranted to investigate the significance of asymptomatic DVT in the ICU setting and its influence on PE and mortality.
1. Introduction
In the early months of 2020, studies from Wuhan (China) analyzed the first hospitalized COVID-19 patients and discovered abnormally elevated coagulation parameters, especially d-dimer and fibrin degradation product (FDP) [1,2,3,4]. Cui et al. reported high frequencies of VTE with 25% in COVID-19 patients with severe pneumonia [5]. Even though bleeding is less common than thrombosis, it may occur, especially with the use of anticoagulation [6]. These early reports demonstrated that SARS-CoV-2 affects coagulation. Great caution in the management of patients is necessary, because COVID-19 related thromboembolism (TE) is associated with higher risk of death [7]. Guidelines already recommended the use of low molecular weight heparin (LMWH) for hospitalized COVID-19 patients in March 2020 [8]. This decision was based on a retrospective study by Tang et al., who reported that LMWH as thromboprophylaxis improves survival in patients with high d-dimer levels or sepsis-induced coagulopathy (SIC) scores [9]. Meanwhile, all worldwide guidelines recommend the use of anticoagulants in hospitalized patients, especially with LMWH [10]. However, randomized clinical trials on optimal antithrombotic regimens for out- and inpatients with COVID-19 are still in progress [11].
2. Prevalence
The prevalence of TE and bleeding varies depending on disease severity, intensive care unit (ICU) admission, and the use of extracorporeal life support (ECLS). ECLS is used as a rescue therapy in selected patients if conventional therapies such as mechanical ventilation (MV) are not successful [12]. However, ECLS increases the risk for both TE and bleeding due to contact activation of the coagulation cascade, thrombin generation, and fibrin deposition on artificial surfaces [13,14]. Therefore, we divided this paragraph into three subsections to describe COVID-19-related TE and bleeding of patients who are (1) hospitalized, (2) admitted to ICU, and (3) receiving ECLS. Numbers were provided from meta-analyses [15,16,17,18,19] and retrospective studies [12,20,21,22].
2.1. Hospitalized Patients
Regarding all hospitalized patients, the overall prevalence of venous thromboembolism (VTE) was 10–14.7% [15,18]. VTE included pulmonary embolism (PE) in 0–7.8%, and deep vein thrombosis (DVT) of the leg in 1–11.2% of the patients. Arterial thromboembolism (ATE) occurred less frequent than VTE and was found in 2–4% of the patients. ATE included myocardial infarction or acute coronary syndrome in 1.1%, and ischemic stroke in 1.4–1.6% of the patients [19]. Bleeding events occurred in 7.8% of the patients, from which 0.4–3.9% were classified as major bleeding [16,22,23].
2.2. Hospitalized Patients Admitted to the ICU
Complications were more frequent in patients who were admitted to the ICU. The prevalence of VTE was 23.2–28%, with PE in 3–13.5% and DVT in 15–21.1% of the patients [15]. The frequency of ATE was 3–12%, which included myocardial infarction or acute coronary syndrome in 8%, and ischemic stroke in 3% of the patients [17]. Bleeding events occurred in 4.4–11% of the patients [16,22].
2.3. Hospitalized Patients Receiving ECLS
In patients who receive ECLS, prevalence of TE varies between 11% and 41% [20,21]. PE occurred in 3–29%, ATE in 4–6%, ischemic stroke in 0.7%, and mechanical thrombotic events (in ECLS components) in 14% of the patients [12,20,21]. Prevalence of bleeding (including minor events) was 54–59%. Bleeding locations were in the upper respiratory tract in 47%, cannulation-related in 14–29%, pericardial tamponade in 12%, central nervous system in 6–10%, and gastrointestinal in 4–6% of the patients.
3. Mechanisms
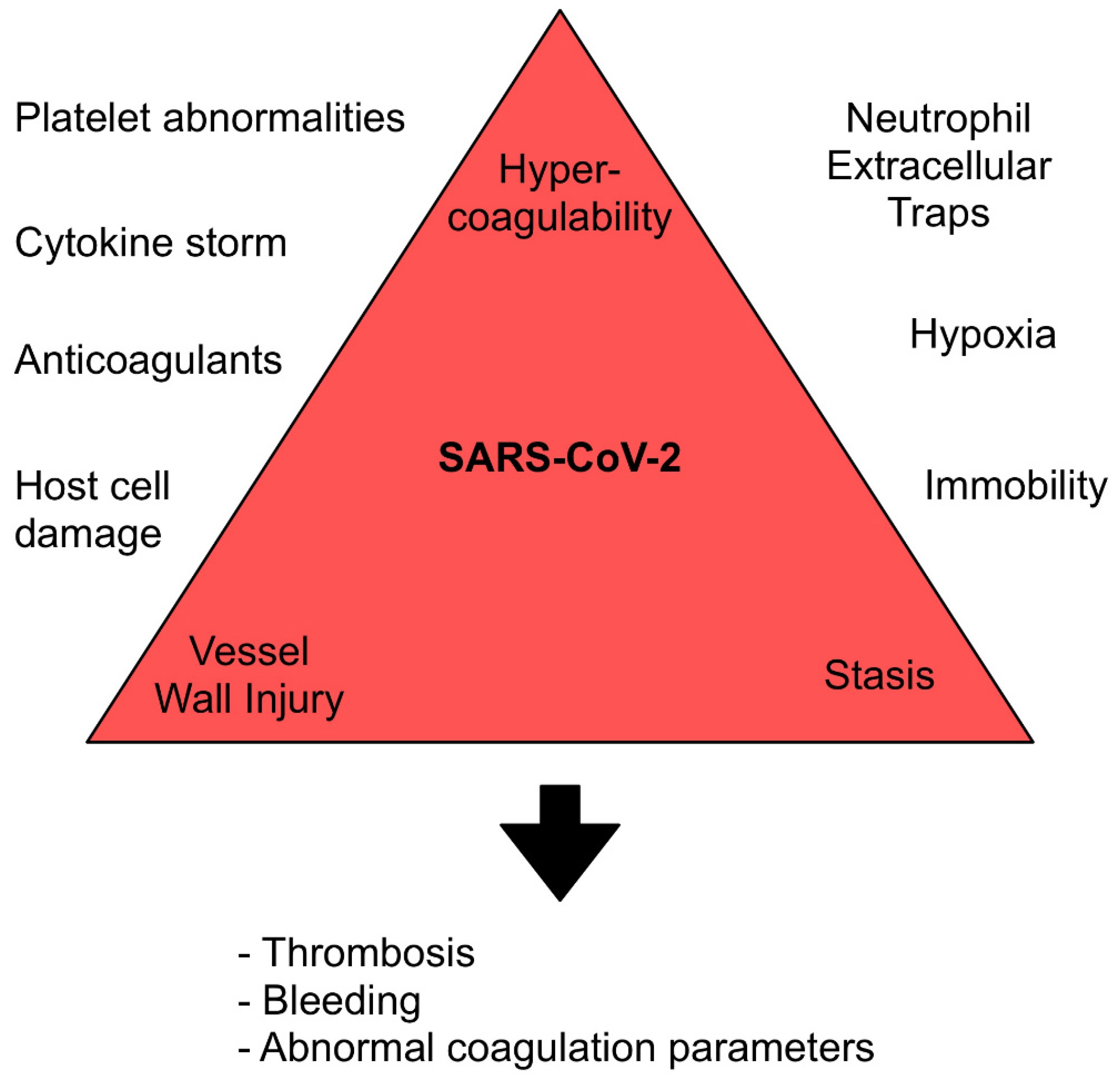
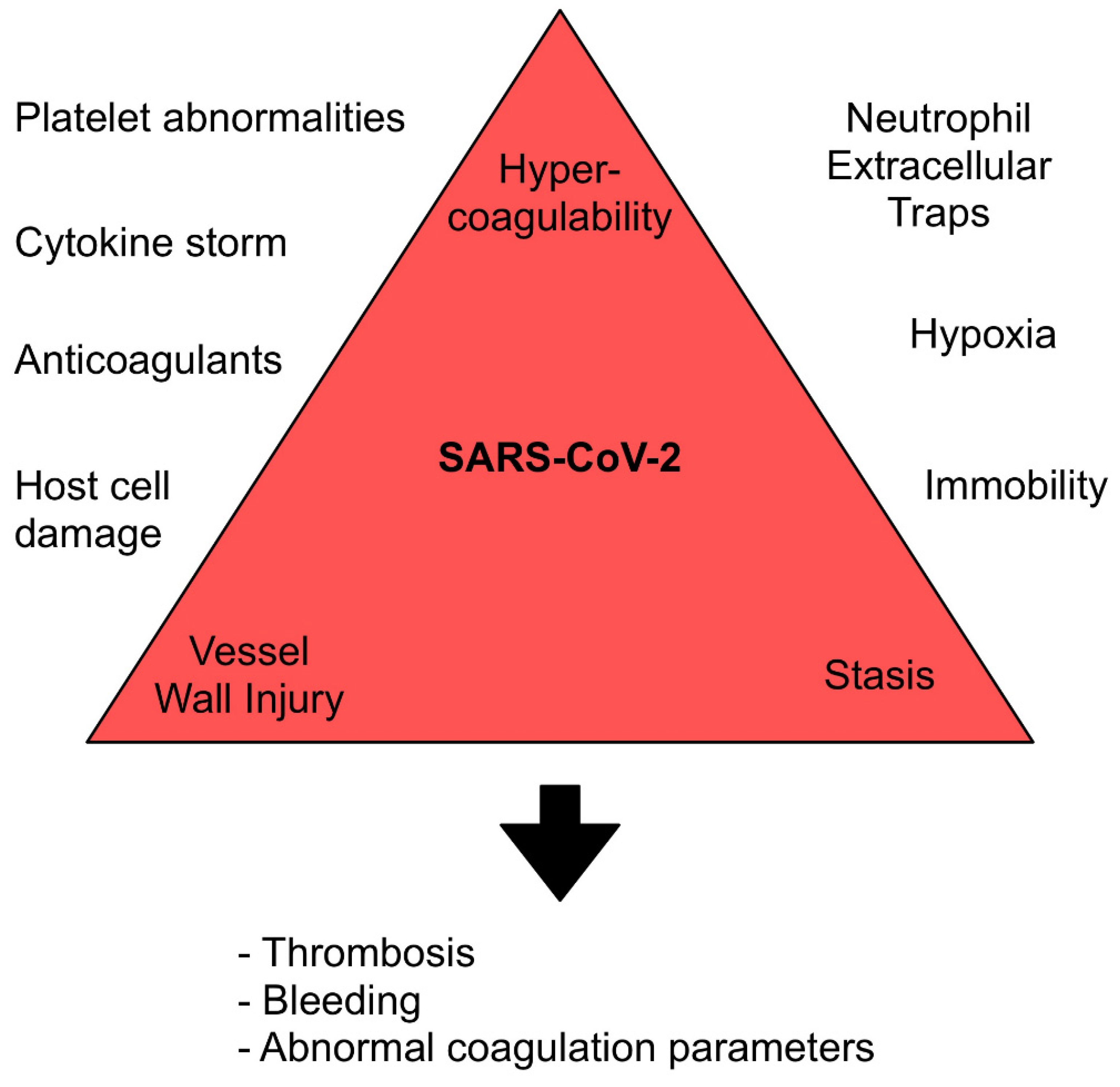
SARS-CoV-2 is a large, enveloped, positive-stranded RNA virus that contains spike-like projections of glycoproteins on the surface [24]. The latter surface proteins can attach to epithelial cells lining the lungs, arteries, heart, kidney, and intestines [25]. As of this moment, the interplay between overactive immune and coagulation systems starts, and together they promote thrombosis, bleeding, and abnormal coagulation parameters. Therefore, COVID-19 patients present abnormalities in all factors of the Virchow’s triad (Figure 1).
3.1. Angiotensin-Converting Enzyme 2 Receptor Binding
The angiotensin-converting enzyme 2 (ACE-2) receptor is a transmembrane protein which lies on endothelial cells, macrophages and other cell types [26]. The glycosylated spike proteins of SARS-CoV-2 have a receptor binding domain (RBD) which binds to ACE-2 receptors and enables host cell entry. The affinity of RBDs in SARS-CoV-2 is 10–20-fold higher than in the previous SARS-CoV [6]. Type 2 pneumocytes are known as a major infection site; however, this entry mechanism has also been described in glomerular capillary loops, small intestine capillaries, and myocardiocytes [27]. The intracellular SARS-CoV-2 infection causes direct endothelial injury which has been reported in postmortem histological lung analyses [27,28]. Furthermore, there is infection of surrounding pericytes and perivascular cells in capillaries and venules throughout the body. They are directly connected to endothelial cells via gap junctions and regulate multiple physiological pathways [29]. One of these signal pathways is the upregulation of pro-coagulatory substances when inflammation occurs. Humans are characterized by an abundant expression of ACE-2 receptors and, therefore, have high vulnerability for viral entry and resultant vascular injury and local inflammation [6].
ACE-2 is classified as an aminopeptidase which plays an important role in the renin-angiotensin system (RAS) and converts angiotensin 2 into angiotensin (1–7). Angiotensin 2 can bind to the angiotensin type 1 receptor (AT1R) which triggers vasoconstriction, hypertrophy, fibrosis, proliferation, inflammation, and oxidative stress [30]. On the other hand, angiotensin-(1–7) binds to the MAS receptor and exerts actions, such as vasodilation, vascular protection, anti-fibrosis, anti-proliferation, and anti-inflammation. SARS-CoV-2 causes a downregulation of ACE-2 and thereby increases the damaging effects of angiotensin 2. Moreover, higher expression of ACE2 in patients with cardiovascular diseases has been associated with more respiratory symptoms in SARS-CoV-2 infections [31].
3.2. Regulated Cell Death
Death of host cells can be caused by several different mechanisms; however, it was observed that SARS-CoV induces apoptosis through modulating the “Akt” or “Protein kinase B” survival pathway [32]. This includes a highly inflammatory form of regulated cell death, known as pyroptosis, that occurs mostly on infection with intracellular pathogens. This process starts with the SARS-CoV E protein that induces calcium leakage to the cytosol from the Golgi storage, and with the open reading frame 3a that induces potassium efflux from the cytosol to extracellular spaces [33]. This imbalance of ionic concentrations and other direct stimulation pathways are activating the NLR family pyrin domain containing 3 inflammasome. Inflammasome activation causes the formation of gasdermin-D pores on cell membranes that enable interleukin secretion and the influx of water and, as a result, cell swelling and rupturing. Furthermore, open reading frame 3a of SARS-CoV-2 can induce direct apoptosis [33]. Regulated apoptosis, especially pyroptosis, can be found in any cell type and is the start of an intense inflammatory response that may become systemic because of releasing multiple proinflammatory cytokines, such as interleukin-1b and interleukin-18 [27]. Autopsy findings of COVID-19-infected lungs showed diffuse alveolar injury with the presence of intracellular virus and damaged cell membranes [28]. The histologic analysis revealed widespread thrombosis with microangiopathy. The authors reported that patients with COVID-19 had significantly more alveolar capillary microthrombi than patients with influenza. Furthermore, COVID-19 patients had significantly more pulmonary intussusceptive angiogenesis than patients with influenza.
3.3. Cytokine Storm
After entering (endothelial) cells and causing direct damage, SARS-CoV-2 shedding induces an inflammatory response. This includes the release of proinflammatory cytokines such as interleukin 1β (IL-1β), IL-2, IL-6, tumor necrosis factor (TNF), and granulocyte-macrophage colony-stimulating factor (GM-CSF) [34]. This process, also referred to as the cytokine storm, can become excessive and lead to upregulation of procoagulants such as tissue factor (TF), von Willebrand factor (vWF), P-selectin, factor VIII (FVIII), and fibrinogen. At the same time, it induces downregulation of anticoagulants such as endothelial protein C receptor (EPCR) and thrombomodulin (TM), modulation of fibrinolysis by increased expression of type 1 plasminogen activator inhibitor, and leukocyte recruitment.
In this way, the intense local inflammatory reaction develops into a systemic inflammatory response with dysregulation of coagulation [34]. Cytokine storm presents itself by common symptoms such as fever, fatigue, anorexia, headache, rash, diarrhea, myalgia, and neuropsychiatric findings [35]. However, it can induce complications such as disseminated intravascular coagulation (DIC), hypoxemia, hypotension, acute respiratory distress syndrome (ARDS), and death. Symptoms and complications can be due to direct tissue damage, physiological changes, or may result from immune-cell-mediated responses [35]. Studies reported that higher IL6 levels are strongly associated with COVID-19 severity and mortality [36,37]. Furthermore, COVID-19-associated cytokine storm influences coagulation parameters such as CRP and d-dimer, and the risk for thromboembolic complications [35].
3.4. Neutrophil Extracellular Traps
Immune cells or leukocytes play an important role in cytokine production and other immune mechanisms. Patients with COVID-19 are characterized by high levels of circulating neutrophils, monocytes, and dendritic cells [38]. Neutrophils are of special interest; they are recruited early to infected cells and kill all kinds of pathogens by an oxidative burst and phagocytosis [39]. Together with various other pathways, neutrophils promote the formation of neutrophil extracellular traps (NET). NETs are small DNA structures that facilitate inflammation by enclosing pathogens. However, NETs can initiate platelet activation through toll-like receptors on various immune cells and thereby activate the receptor integrin αIIbβ3, which promotes platelet aggregation, granule release, phosphatidylserine exposure, coagulation factor activation, and thrombin generation. This results in excessive inflammatory reactions, damage to surrounding tissue, and thrombosis [40]. In an autopsy case series of COVID-19 patients, microvascular thrombi containing NETs were found in the lungs, kidneys, and heart tissues [41]. Nicolai et al. reported that excessive platelet and neutrophil activation of COVID-19 patients indicates severe illness and was higher in comparison to non-COVID-19 patients with pneumonia [41]. Regarding thrombosis, increased levels of neutrophil activation and NET formation in hospitalized COVID-19 patients are associated with higher risk of thrombotic complications [42].
3.5. Platelet Abnormalities
Platelets or thrombocytes can bind to different microbes, including viral pathogens. This interaction of pathogens and platelets triggers granule release, with further platelet activation, promotion of platelet–leukocyte interactions, and tissue infiltration, which is necessary for pathogen clearance [6]. In the majority of COVID-19 patients with mild or moderate symptoms, the platelet count is normal or slightly increased [43]. However, in COVID-19 patients who are critically ill, platelet count may be decreased and disseminated intravascular coagulation (DIC) can be found [1]. Thrombocytopenia can occur due to three different reasons. 1: The primary platelet production can be decreased because of cytokines that damage progenitor cells in the bone marrow or directly infected hematopoietic and bone marrow stromal cells. 2: Platelet destruction can be increased due to formation of autoantibodies and immune complexes which result in clearance of platelets by the immune system. 3: Finally, circulating platelets can decrease because of an enhanced platelet consumption. This consumption is caused by lung injury which increases platelet activation, aggregation, and wrapping into microthrombi.
3.6. Hypoxia and Immobility
Decreased oxygen pressure is present in patients with severe COVID-19 and can transform into severe hypoxic and/or hypercapnic respiratory failure. The ventilation to perfusion (V/Q) ratio is disturbed by capillary hyperperfusion and microvascular thrombosis, resulting in dead space in the lung with reduced pulmonary capillary flow [44]. Hypoxia can promote thrombosis by means of increasing blood viscosity and hypoxia-inducible factors (HIFs) which interact with multiple pro-thrombotic and inflammatory targets [45]. Immobilization plays an important role in hospitalized, especially ICU-admitted, COVID-19 patients as it is known to be an important risk factor for thrombosis, particularly VTE [46]. With regard to VTE, muscular and diaphragm dysfunction decreases venous blood flow in the legs and causes hypoxic activation of coagulation [47].
3.7. Anticoagulants
The increased bleeding risk of hospitalized COVID-19 patients is mostly associated with the use of anticoagulants. Unfractionated heparin (UFH) activates the enzyme inhibitor antithrombin III (AT) which then inactivates thrombin, factor Xa, and other proteases. LMWHs also bind to AT and accelerate the inhibition of factor Xa. However, unlike AT activated by heparin, AT activated by LMWH cannot inhibit thrombin (factor IIa), but can only inhibit clotting factor Xa. Eventually, both anticoagulants reduce the conversion of soluble fibrinogen into insoluble threads of fibrin and, therefore, decrease thrombosis formation.
4. Screening
Routine screening may help to detect DVT and prevent the occurrence of PE, however, it may increase incidental findings, exposure of healthcare professionals, and costs. Early studies reported that systematic screening for DVT was not associated with a higher diagnosis of VTE or a reduced diagnosis of PE [48]. Clinically guided screening remains the recommended approach, which is performed in suspected cases with clinical signs such as localized tenderness, pitting oedema, swelling in lower extremities, or central venous catheter dysfunction. Furthermore, guidelines suggest a low threshold for evaluation of thromboembolic disease in patients with rapid deterioration of pulmonary, cardiac, or neurological function, or of sudden, localized loss of peripheral perfusion [49]. Additionally, the presence of risk factors can be used for clinical decision-making. Li et al. reported that age, liver dysfunction, and atrial fibrillation were independent risk factors for systemic TE [50].
A main reason for the current guidelines is that observational studies or clinical trials with a direct comparison of patients with and without routine screening do not exist [49]. However, Boonyawat et al. reported significantly higher incidences of DVT in studies that performed compression ultrasound screening protocols than studies that did not perform routine screening, especially in patients residing in the ICU [18]. However, even though routine screening might increase the detection of DVT, the impact on development of PE or mortality is still unknown.
5. Laboratory Testing
The use of laboratory parameters for clinical decisions in COVID-19 patients remains challenging. Demelo-Rodriguez et al. reported that d-dimer levels above 1570 ng/mL were associated with asymptomatic DVT and higher cut-off levels for d-dimer might be necessary for the diagnosis of DVT in COVID-19 patients [51]. Zhan et al. investigated the diagnostic value of d-dimer in a meta-analysis with 2158 patients and found that d-dimer can diagnose COVID-19-related VTE with high sensitivity (90%), low specificity (60%), and acceptable accuracy (AUC 85%) [52]. Elevated d-dimer and fibrinogen levels are a common finding in all hospitalized COVID-19 patients [3] and, therefore, specificity of d-dimer testing for DVT or PE is low. Currently, guidelines recommend either for or against using coagulation parameters to guide management decisions [49].
6. Thromboprophylaxis
Prophylactic doses of anticoagulation for VTE have an important role in COVID-19 management as they are associated with lower mortality, however, indications for thromboprophylaxis depend on hospitalization and potential contraindications [53]. Furthermore, patients who are receiving anticoagulant or antiplatelet therapies for underlying conditions should continue these medications if they receive the diagnosis of COVID-19 [49].
6.1. Indication
Current guidelines recommend the use of thromboprophylaxis in hospitalized adults (<18 years) with COVID-19 if no contraindications (active bleeding or platelet count < 25 × 109/L) are present [49]. If pharmacological thromboprophylaxis is contraindicated, mechanical VTE prophylaxis such as intermittent pneumatic compression should be applied in immobilized patients [54].
Thromboprophylaxis for quarantined patients with less severe COVID-19 but potential comorbidities, or for patients without COVID-19 who are less active because of quarantine, is not certain. The ongoing ETHIC trial and OVID study are investigating whether prophylactic-dose enoxaparin improves survival and reduces unplanned hospitalizations in ambulatory patients aged 50 or older [11]. As long as results of these RCTs are unknown, the current guidelines recommend that pharmacological prophylaxis should be reserved for those patients at highest risk, including those with limited mobility and history of prior VTE or active malignancy, and quarantined patients with mild symptoms should be advised to stay active at home.
Patients under ECMO therapy receive full-dose anticoagulation (mostly UFH) as a standard procedure and should not be administered with additional thromboprophylaxis. Guidelines of the Extracorporeal Life Support Organization (ELSO) suggest following the existing recommendations of non-COVID-19 patients, but target anticoagulation at the higher end of normal ECMO parameters [55].
6.2. Type and Dosing
LMWHs or UFH may be the preferred anticoagulants in hospitalized critically ill patients because of its shorter half-life, ability to be given intravenously or subcutaneously, and fewer known drug–drug interactions compared with other (oral) anticoagulants. However, in patients without risk for drug interactions, the use of direct oral anticoagulants (DOACs) can be considered [56].
The appropriate dosing of therapeutic anticoagulation with heparin was unclear during the first year of the pandemic. The recently published studies of the ATTACC multiplatform trial investigated whether therapeutic-dose anticoagulation improved outcomes for patients hospitalized with COVID-19 [57]. The intervention group of this randomized clinical trial was compared with a control group who received usual care thromboprophylaxis doses according to local practice. The results differ according to the severity of COVID-19 disease. In noncritically ill patients with COVID-19, therapeutic-dose anticoagulation with heparin showed increased survival to hospital discharge and reduced use of cardiovascular or respiratory organ support as compared with usual-care thromboprophylaxis [58]. However, in critically ill patients with COVID-19, therapeutic-dose anticoagulation with heparin did not improve survival or the need for organ support [59]. A separate randomized trial reported that intermediate-dose heparin also was not beneficial in critically ill COVID-19 patients [60]. A possible reason behind these findings could be that higher anticoagulation strategies cannot influence inflammation, thrombosis, and organ injury in patients who already suffer from advanced disease [61]. In summary, high-quality evidence showed that therapeutic doses of anticoagulation should be used in noncritically ill patients (admitted to the hospital but not requiring ICU-level care or organ support). If patients are critically ill at hospital admission, it is appropriate to administer usual care thromboprophylaxis according to local practices.
The therapeutic-dose anticoagulation (of the intervention group) included the LMWH enoxaparin (1.5 mg/kg subcutaneous once daily or 1 mg/kg subcutaneous twice daily), tinzaparin (175 anti-Xa IU/kg subcutaneous once daily), dalteparin (200 IU/kg subcutaneous once daily or 100 IU/kg subcutaneous twice a day), or intravenous infusion of UFH (according to total body weight and pragmatically adjusted according to local institutional policy to achieve an activated partial thromboplastin time (aPTT) of 1.5–2.5× the reference value). Additionally, the appropriate dosing of prophylaxis should be adjusted on the basis of comorbidities, bleeding complications, severe thrombocytopenia (platelet count <50 × 109/L or <25 × 109/L), or comorbidities (e.g., impaired renal function). Of note, thromboprophylaxis should be held only if the platelet count is <25 × 109/L or fibrinogen level is <0.5 g/L.
6.3. Extended Prophylaxis
Due to lack of high-quality evidence, extended VTE prophylaxis after hospital discharge is not recommended in the current guidelines [49]. However, the ongoing ACTIV-4c and MICHELLE trials are designed to compare the effectiveness and safety of antithrombotic therapy with no antithrombotic therapy after hospitalization in COVID-19 patients [11]. Antithrombotic agents for the two intervention groups of these trials include apixaban and rivaroxaban, respectively [11].
For certain high VTE risk patients without COVID-19, post-discharge prophylaxis has already been shown to be beneficial. The Food and Drug Administration approved the use of rivaroxaban 10 mg daily for 31 to 39 days in these patients [62]. High risk for VTE was identified with the Modified International Medical Prevention Registry on Venous Thromboembolism (IMPROVE) risk score ≥4, or the Modified IMPROVE VTE risk score ≥2 and D-dimer level >2 times the upper limit of normal [62]. Nevertheless, consideration of individual risk factors for VTE, including reduced mobility, bleeding risks, and feasibility, is necessary.
6.4. Pregnancy
VTE prophylaxis can reasonably be considered for pregnant women hospitalized with COVID-19, particularly for those who suffer from severe disease. If there are no contraindications to use, prophylactic heparin or low molecular weight heparin in critically ill or mechanically ventilated pregnant patients is recommended [49]. VTE prophylaxis after hospital discharge is not recommended for pregnant patients.
7. Conclusions
Thromboembolism and bleeding complications are common in COVID-19 patients and its frequency increases according to disease severity, ICU admission, and the use of invasive therapies. Different mechanisms involved in over-regulation of immune and coagulation system are identified. Complications are associated with increased mortality; therefore, evidential anticoagulation and screening protocols are warranted. Antithrombotic agents seem to be reasonable in all hospitalized patients without contraindication. Recent high-quality evidence showed that higher (therapeutic) doses of antithrombotic agents are only beneficial in noncritically ill patients who were primarily admitted to the general ward, and usual care thromboprophylaxis is sufficient in critically ill patients at the ICU and under ECMO therapy. Ongoing trials will determine the influence of antithrombotic agents on outcomes of non-hospitalized or discharged patients. Regarding screening for VTE, high quality evidence is warranted to investigate the significance of asymptomatic DVT in the ICU setting and its influence on PE and mortality.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
References
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Han, H.; Yang, L.; Liu, R.; Liu, F.; Wu, K.L.; Li, J.; Liu, X.H.; Zhu, C.L. Prominent changes in blood coagulation of patients with SARS-CoV-2 infection. Clin. Chem. Lab. Med. 2020, 58, 1116–1120. [Google Scholar] [CrossRef] [Green Version]
- Cui, S.; Chen, S.; Li, X.; Liu, S.; Wang, F. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J. Thromb. Haemost. JTH 2020, 18, 1421–1424. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Paz, L.; Capodanno, D.; Montalescot, G.; Angiolillo, D.J. Coronavirus Disease 2019–Associated Thrombosis and Coagulopathy: Review of the Pathophysiological Characteristics and Implications for Antithrombotic Management. J. Am. Heart Assoc. 2021, 10, e019650. [Google Scholar] [CrossRef] [PubMed]
- Malas, M.B.; Naazie, I.N.; Elsayed, N.; Mathlouthi, A.; Marmor, R.; Clary, B. Thromboembolism risk of COVID-19 is high and associated with a higher risk of mortality: A systematic review and meta-analysis. EClinicalMedicine 2020, 29, 100639. [Google Scholar] [CrossRef]
- Thachil, J.; Tang, N.; Gando, S.; Falanga, A.; Cattaneo, M.; Levi, M.; Clark, C.; Iba, T. ISTH interim guidance on recognition and management of coagulopathy in COVID-19. J. Thromb. Haemost. 2020, 18, 1023–1026. [Google Scholar] [CrossRef]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef]
- Ozsu, S.; Gunay, E.; Konstantinides, S.V. A review of venous thromboembolism in COVID-19: A clinical perspective. Clin. Respir. J. 2021, 15, 506–512. [Google Scholar] [CrossRef]
- Talasaz, A.H.; Sadeghipour, P.; Kakavand, H.; Aghakouchakzadeh, M.; Kordzadeh-Kermani, E.; Van Tassell, B.W.; Gheymati, A.; Ariannejad, H.; Hosseini, S.H.; Jamalkhani, S.; et al. Recent Randomized Trials of Antithrombotic Therapy for Patients with COVID-19: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 77, 1903–1921. [Google Scholar] [CrossRef]
- Barbaro, R.P.; MacLaren, G.; Boonstra, P.S.; Iwashyna, T.J.; Slutsky, A.S.; Fan, E.; Bartlett, R.H.; Tonna, J.E.; Hyslop, R.; Fanning, J.J.; et al. Extracorporeal membrane oxygenation support in COVID-19: An international cohort study of the Extracorporeal Life Support Organization registry. Lancet 2020, 396, 1071–1078. [Google Scholar] [CrossRef]
- Sklar, M.C.; Sy, E.; Lequier, L.; Fan, E.; Kanji, H.D. Anticoagulation Practices during Venovenous Extracorporeal Membrane Oxygenation for Respiratory Failure. A Systematic Review. Ann. Am. Thorac. Soc. 2016, 13, 2242–2250. [Google Scholar] [CrossRef] [PubMed]
- Granja, T.; Hohenstein, K.; Schüssel, P.; Fischer, C.; Prüfer, T.; Schibilsky, D.; Wendel, H.P.; Jaschonek, K.; Serna-Higuita, L.; Schlensak, C.; et al. Multi-Modal Characterization of the Coagulopathy Associated with Extracorporeal Membrane Oxygenation. Crit. Care Med. 2020, 48, e400–e408. [Google Scholar] [CrossRef]
- Tan, B.K.; Mainbourg, S.; Friggeri, A.; Bertoletti, L.; Douplat, M.; Dargaud, Y.; Grange, C.; Lobbes, H.; Provencher, S.; Lega, J.-C. Arterial and venous thromboembolism in COVID-19: A study-level meta-analysis. Thorax 2021. [Google Scholar] [CrossRef]
- Jiménez, D.; García-Sanchez, A.; Rali, P.; Muriel, A.; Bikdeli, B.; Ruiz-Artacho, P.; Le Mao, R.; Rodríguez, C.; Hunt, B.J.; Monreal, M. Incidence of VTE and Bleeding Among Hospitalized Patients with Coronavirus Disease 2019: A Systematic Review and Meta-analysis. Chest 2021, 159, 1182–1196. [Google Scholar] [CrossRef]
- Jenner, W.J.; Kanji, R.; Mirsadraee, S.; Gue, Y.X.; Price, S.; Prasad, S.; Gorog, D.A. Thrombotic complications in 2928 patients with COVID-19 treated in intensive care: A systematic review. J. Thromb. Thrombolysis 2021, 51, 595–607. [Google Scholar] [CrossRef] [PubMed]
- Boonyawat, K.; Chantrathammachart, P.; Numthavaj, P.; Nanthatanti, N.; Phusanti, S.; Phuphuakrat, A.; Niparuck, P.; Angchaisuksiri, P. Incidence of thromboembolism in patients with COVID-19: A systematic review and meta-analysis. Thromb. J. 2020, 18, 34. [Google Scholar] [CrossRef] [PubMed]
- Nannoni, S.; de Groot, R.; Bell, S.; Markus, H.S. Stroke in COVID-19: A systematic review and meta-analysis. Int. J. Stroke 2021, 16, 137–149. [Google Scholar] [CrossRef]
- Durak, K.; Kersten, A.; Grottke, O.; Zayat, R.; Dreher, M.; Autschbach, R.; Marx, G.; Marx, N.; Spillner, J.; Kalverkamp, S. Thromboembolic and Bleeding Events in COVID-19 Patients receiving Extracorporeal Membrane Oxygenation. Thorac. Cardiovasc. Surg. 2021. [Google Scholar] [CrossRef]
- Raasveld, S.J.; Delnoij, T.S.R.; Broman, L.M.; Lansink-Hartgring, A.O.; Hermans, G.; De Troy, E.; Taccone, F.S.; Quintana Diaz, M.; van der Velde, F.; Miranda, D.D.R.; et al. Extracorporeal Membrane Oxygenation in Patients With COVID-19: An International Multicenter Cohort Study. J. Intensive Care Med. 2021, 36, 8850666211007063. [Google Scholar] [CrossRef]
- Dalager-Pedersen, M.; Lund, L.C.; Mariager, T.; Winther, R.; Hellfritzsch, M.; Larsen, T.B.; Thomsen, R.W.; Johansen, N.B.; Søgaard, O.S.; Nielsen, S.L.; et al. Venous thromboembolism and major bleeding in patients with COVID-19: A nationwide population-based cohort study. Clin. Infect. Dis. 2021, ciab003. [Google Scholar] [CrossRef]
- Kaatz, S.; Ahmad, D.; Spyropoulos, A.C.; Schulman, S. Definition of clinically relevant non-major bleeding in studies of anticoagulants in atrial fibrillation and venous thromboembolic disease in non-surgical patients: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2015, 13, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Shanmugam, C.; Mohammed, A.R.; Ravuri, S.; Luthra, V.; Rajagopal, N.; Karre, S. COVID-2019—A comprehensive pathology insight. Pathol. Res. Pract. 2020, 216, 153222. [Google Scholar] [CrossRef]
- Ghebrehiwet, B.; Peerschke, E.I. Complement and coagulation: Key triggers of COVID-19–induced multiorgan pathology. J. Clin. Investig. 2020, 130, 5674–5676. [Google Scholar] [CrossRef]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Avolio, E.; Madeddu, P. Discovering cardiac pericyte biology: From physiopathological mechanisms to potential therapeutic applications in ischemic heart disease. Vasc. Pharmacol. 2016, 86, 53–63. [Google Scholar] [CrossRef] [Green Version]
- Ni, W.; Yang, X.; Yang, D.; Bao, J.; Li, R.; Xiao, Y.; Hou, C.; Wang, H.; Liu, J.; Yang, D.; et al. Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19. Crit. Care 2020, 24, 422. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.-Y.; Ma, Y.-T.; Zhang, J.-Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, C.-M.; Ma, C.-W.; Chan, W.-Y.; Chan, H.Y.E. The SARS-Coronavirus Membrane protein induces apoptosis through modulating the Akt survival pathway. Arch. Biochem. Biophys. 2007, 459, 197–207. [Google Scholar] [CrossRef]
- Shi, C.-S.; Nabar, N.R.; Huang, N.-N.; Kehrl, J.H. SARS-Coronavirus Open Reading Frame-8b triggers intracellular stress pathways and activates NLRP3 inflammasomes. Cell Death Discov. 2019, 5, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, N.C.; Weitz, J.I. COVID-19 coagulopathy, thrombosis, and bleeding. Blood 2020, 136, 381–383. [Google Scholar] [CrossRef] [PubMed]
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef]
- Del Valle, D.M.; Kim-Schulze, S.; Huang, H.-H.; Beckmann, N.D.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T.H.; Madduri, D.; Stock, A.; et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat. Med. 2020, 26, 1636–1643. [Google Scholar] [CrossRef]
- Caricchio, R.; Gallucci, M.; Dass, C.; Zhang, X.; Gallucci, S.; Fleece, D.; Bromberg, M.; Criner, G.J. Preliminary predictive criteria for COVID-19 cytokine storm. Ann. Rheum. Dis. 2021, 80, 88–95. [Google Scholar] [CrossRef]
- Peruzzi, B.; Bencini, S.; Capone, M.; Mazzoni, A.; Maggi, L.; Salvati, L.; Vanni, A.; Orazzini, C.; Nozzoli, C.; Morettini, A.; et al. Quantitative and qualitative alterations of circulating myeloid cells and plasmacytoid DC in SARS-CoV-2 infection. Immunology 2020, 161, 345–353. [Google Scholar] [CrossRef]
- Barnes, B.J.; Adrover, J.M.; Baxter-Stoltzfus, A.; Borczuk, A.; Cools-Lartigue, J.; Crawford, J.M.; Daßler-Plenker, J.; Guerci, P.; Huynh, C.; Knight, J.S.; et al. Targeting potential drivers of COVID-19: Neutrophil extracellular trapsNeutrophil extracellular traps in COVID-19. J. Exp. Med. 2020, 217, e20200652. [Google Scholar] [CrossRef]
- Fuchs, T.A.; Brill, A.; Wagner, D.D. Neutrophil Extracellular Trap (NET) Impact on Deep Vein Thrombosis. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 1777–1783. [Google Scholar] [CrossRef] [Green Version]
- Nicolai, L.; Leunig, A.; Brambs, S.; Kaiser, R.; Weinberger, T.; Weigand, M.; Muenchhoff, M.; Hellmuth, J.C.; Ledderose, S.; Schulz, H.; et al. Immunothrombotic Dysregulation in COVID-19 Pneumonia Is Associated with Respiratory Failure and Coagulopathy. Circulation 2020, 142, 1176–1189. [Google Scholar] [CrossRef]
- Zuo, Y.; Zuo, M.; Yalavarthi, S.; Gockman, K.; Madison, J.A.; Shi, H.; Woodard, W.; Lezak, S.P.; Lugogo, N.L.; Knight, J.S.; et al. Neutrophil extracellular traps and thrombosis in COVID-19. J. Thromb. Thrombolysis 2020, 51, 446–453. [Google Scholar] [CrossRef]
- Panigada, M.; Bottino, N.; Tagliabue, P.; Grasselli, G.; Novembrino, C.; Chantarangkul, V.; Pesenti, A.; Peyvandi, F.; Tripodi, A. Hypercoagulability of COVID-19 patients in intensive care unit: A report of thromboelastography findings and other parameters of hemostasis. J. Thromb. Haemost. 2020, 18, 1738–1742. [Google Scholar] [CrossRef]
- Nitsure, M.; Sarangi, B.; Shankar, G.H.; Reddy, V.S.; Walimbe, A.; Sharma, V.; Prayag, S. Mechanisms of Hypoxia in COVID-19 Patients: A Pathophysiologic Reflection. Indian J. Crit. Care Med. 2020, 24, 967–970. [Google Scholar] [CrossRef]
- Gupta, N.; Zhao, Y.-Y.; Evans, C.E. The stimulation of thrombosis by hypoxia. Thromb. Res. 2019, 181, 77–83. [Google Scholar] [CrossRef]
- Gatt, M.E.; Paltiel, O.; Bursztyn, M. Is prolonged immobilization a risk factor for symptomatic venous thromboembolism in elderly bedridden patients? Results of a historical-cohort study. Thromb. Haemost. 2004, 91, 538–543. [Google Scholar] [CrossRef]
- Pottier, P.; Hardouin, J.B.; Lejeune, S.; Jolliet, P.; Gillet, B.; Planchon, B. Immobilization and the risk of venous thromboembolism. A Meta-Anal. Epidemiol. Stud. Thromb. Res. 2009, 124, 468–476. [Google Scholar] [CrossRef]
- Lapébie, F.-X.; Minville, V.; Ribes, A.; Combis, B.; Thery, A.; Geeraerts, T.; Silva, S.; Bura-Rivière, A.; Vardon-Bounes, F. Systematic Screening for Deep Vein Thrombosis in Critically Ill Inpatients With COVID-19: Impact on the Incidence of Venous Thromboembolism. Front. Med. 2021, 7, 624808. [Google Scholar] [CrossRef]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 10 June 2021).
- Li, W.; Xu, Z.; Xiang, H.; Zhang, C.; Guo, Y.; Xiong, J. Risk factors for systemic and venous thromboembolism, mortality and bleeding risks in 1125 patients with COVID-19: Relationship with anticoagulation status. Aging 2021, 13, 9225–9242. [Google Scholar] [CrossRef]
- Demelo-Rodríguez, P.; Cervilla-Muñoz, E.; Ordieres-Ortega, L.; Parra-Virto, A.; Toledano-Macías, M.; Toledo-Samaniego, N.; García-García, A.; García-Fernández-Bravo, I.; Ji, Z.; de-Miguel-Diez, J.; et al. Incidence of asymptomatic deep vein thrombosis in patients with COVID-19 pneumonia and elevated D-dimer levels. Thromb. Res. 2020, 192, 23–26. [Google Scholar] [CrossRef]
- Zhan, H.; Chen, H.; Liu, C.; Cheng, L.; Yan, S.; Li, H.; Li, Y. Diagnostic Value of D-Dimer in COVID-19: A Meta-Analysis and Meta-Regression. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211010976. [Google Scholar] [CrossRef]
- Moonla, C.; Sosothikul, D.; Chiasakul, T.; Rojnuckarin, P.; Uaprasert, N. Anticoagulation and In-Hospital Mortality from Coronavirus Disease 2019: A Systematic Review and Meta-Analysis. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211008999. [Google Scholar] [CrossRef]
- Ho, K.M.; Tan, J.A. Stratified meta-analysis of intermittent pneumatic compression of the lower limbs to prevent venous thromboembolism in hospitalized patients. Circulation 2013, 128, 1003–1020. [Google Scholar] [CrossRef] [Green Version]
- Extracorporeal Life Support Organization (ELSO). Guidelines for Adult Respiratory Failure. Version 1.4. 2017. Available online: https://www.elso.org/Portals/0/ELSO%20Guidelines%20For%20Adult%20Respiratory%20Failure%201_4.pdf (accessed on 28 May 2021).
- Bikdeli, B.; Madhavan, M.V.; Gupta, A.; Jimenez, D.; Burton, J.R.; Der Nigoghossian, C.; Chuich, T.; Nouri, S.N.; Dreyfus, I.; Driggin, E.; et al. Pharmacological Agents Targeting Thromboinflammation in COVID-19: Review and Implications for Future Research. Thromb. Haemost. 2020, 120, 1004–1024. [Google Scholar] [CrossRef]
- Houston, B.L.; Lawler, P.R.; Goligher, E.C.; Farkouh, M.E.; Bradbury, C.; Carrier, M.; Dzavik, V.; Fergusson, D.A.; Fowler, R.A.; Galanaud, J.P.; et al. Anti-Thrombotic Therapy to Ameliorate Complications of COVID-19 (ATTACC): Study design and methodology for an international, adaptive Bayesian randomized controlled trial. Clin. Trials 2020, 17, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Therapeutic Anticoagulation with Heparin in Noncritically Ill Patients with Covid-19. N. Engl. J. Med. 2021. [CrossRef]
- Therapeutic Anticoagulation with Heparin in Critically Ill Patients with Covid-19. N. Engl. J. Med. 2021. [CrossRef]
- Investigators, I. Effect of Intermediate-Dose vs Standard-Dose Prophylactic Anticoagulation on Thrombotic Events, Extracorporeal Membrane Oxygenation Treatment, or Mortality Among Patients With COVID-19 Admitted to the Intensive Care Unit: The INSPIRATION Randomized Clinical Trial. JAMA 2021, 325, 1620–1630. [Google Scholar] [CrossRef]
- Xue, M.; Zeng, Y.; Qu, H.-Q.; Zhang, T.; Li, N.; Huang, H.; Zheng, P.; Hu, H.; Zhou, L.; Duan, Z.; et al. Heparin-binding protein levels correlate with aggravation and multiorgan damage in severe COVID-19. ERJ Open Res. 2021, 7, 00741–02020. [Google Scholar] [CrossRef]
- Spyropoulos, A.C.; Lipardi, C.; Xu, J.; Peluso, C.; Spiro, T.E.; De Sanctis, Y.; Barnathan, E.S.; Raskob, G.E. Modified IMPROVE VTE Risk Score and Elevated D-Dimer Identify a High Venous Thromboembolism Risk in Acutely Ill Medical Population for Extended Thromboprophylaxis. TH Open 2020, 4, e59–e65. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
Mechanisms of coagulation abnormalities in COVID-19 patients.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Durak, K. Thromboembolism and Bleeding in COVID-19. J 2021, 4, 476-485. https://doi.org/10.3390/j4030036
AMA Style
Durak K. Thromboembolism and Bleeding in COVID-19. J. 2021; 4(3):476-485. https://doi.org/10.3390/j4030036
Chicago/Turabian StyleDurak, Koray. 2021. "Thromboembolism and Bleeding in COVID-19" J 4, no. 3: 476-485. https://doi.org/10.3390/j4030036
APA StyleDurak, K. (2021). Thromboembolism and Bleeding in COVID-19. J, 4(3), 476-485. https://doi.org/10.3390/j4030036