

A Comprehensive Evaluation of Zirconia-Reinforced Glass Ionomer Cement’s Effectiveness in Dental Caries: A Systematic Review and Network Meta-Analysis




Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Exclusion Criteria
2.3. Search Methods and Data Collection
2.4. Quality Assessment and Risk of Bias
2.5. Quantitative Analysis and Synthesis of the Network Meta-Analysis (NMA)
3. Results
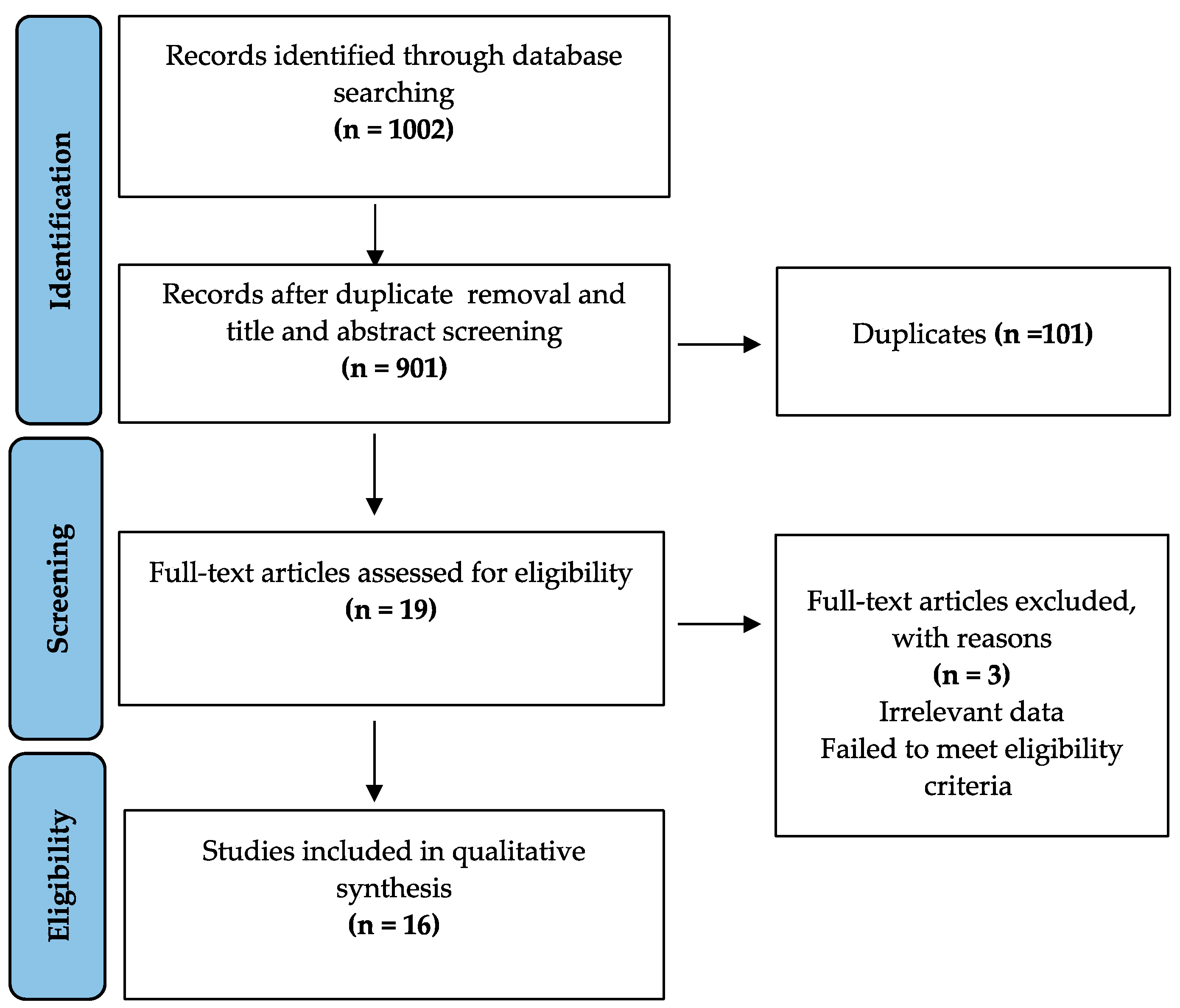
3.1. Search Results and Study Selection
3.2. Study Characteristics
3.2.1. Description of Compressive Strength Studies
3.2.2. Description of Microleakage Studies
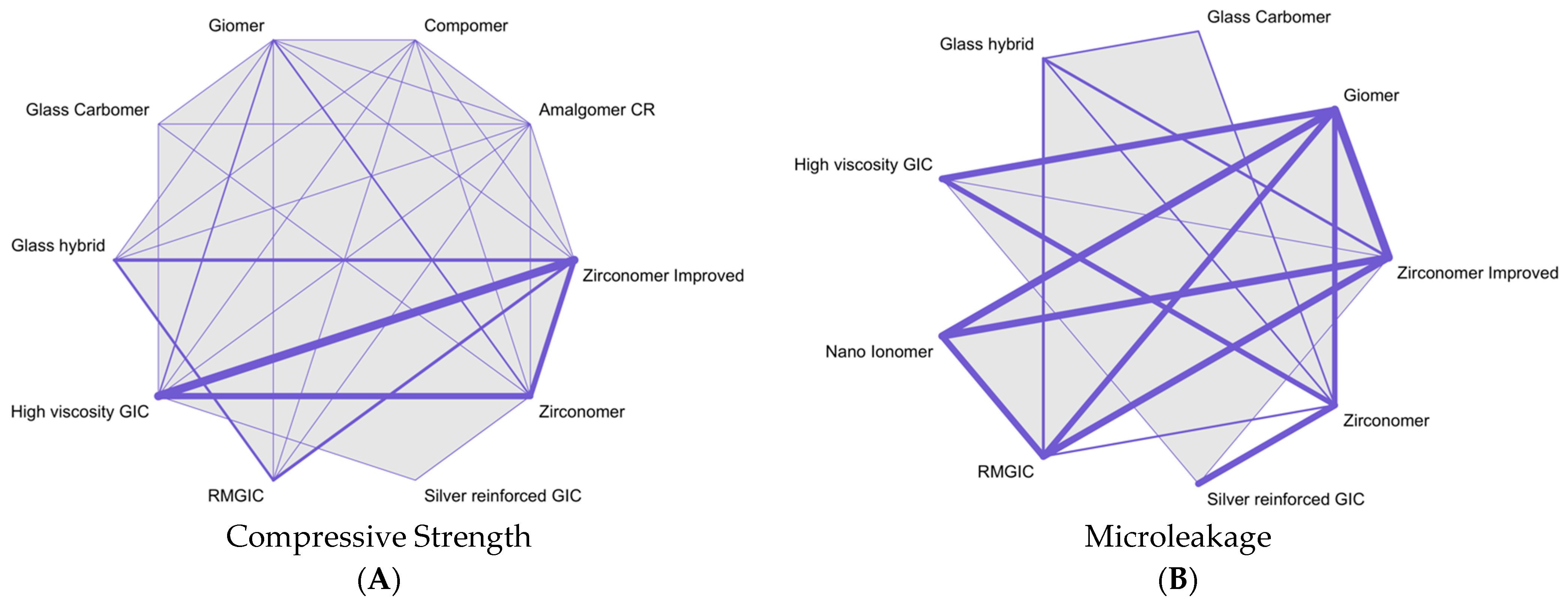
3.3. NMA Synthesis
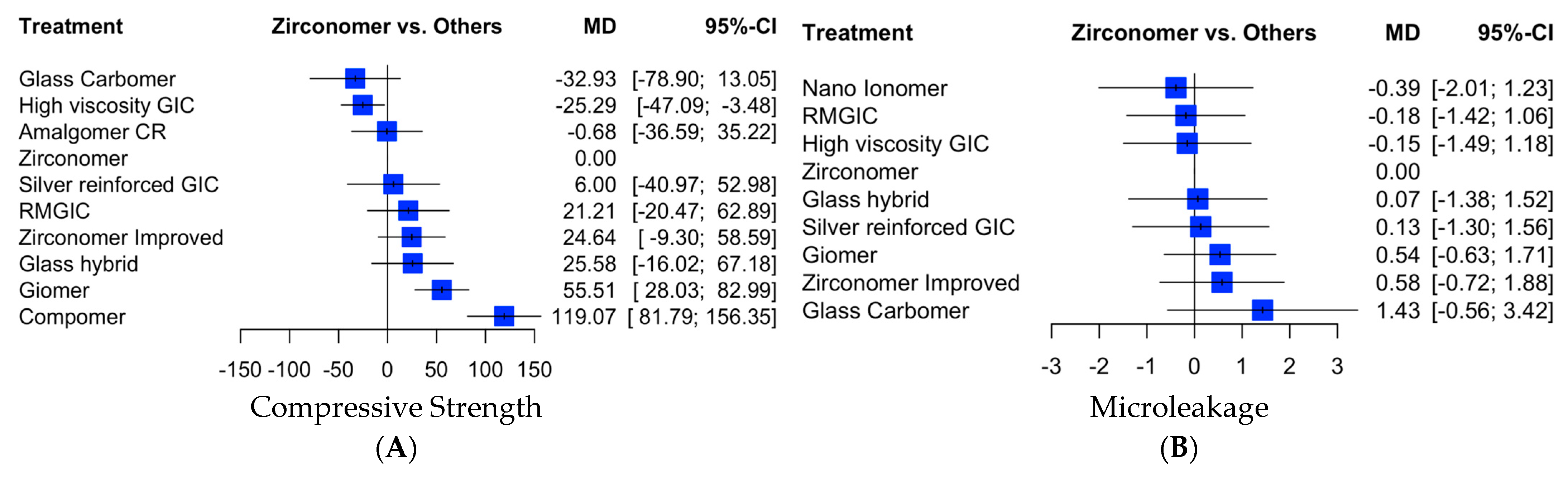
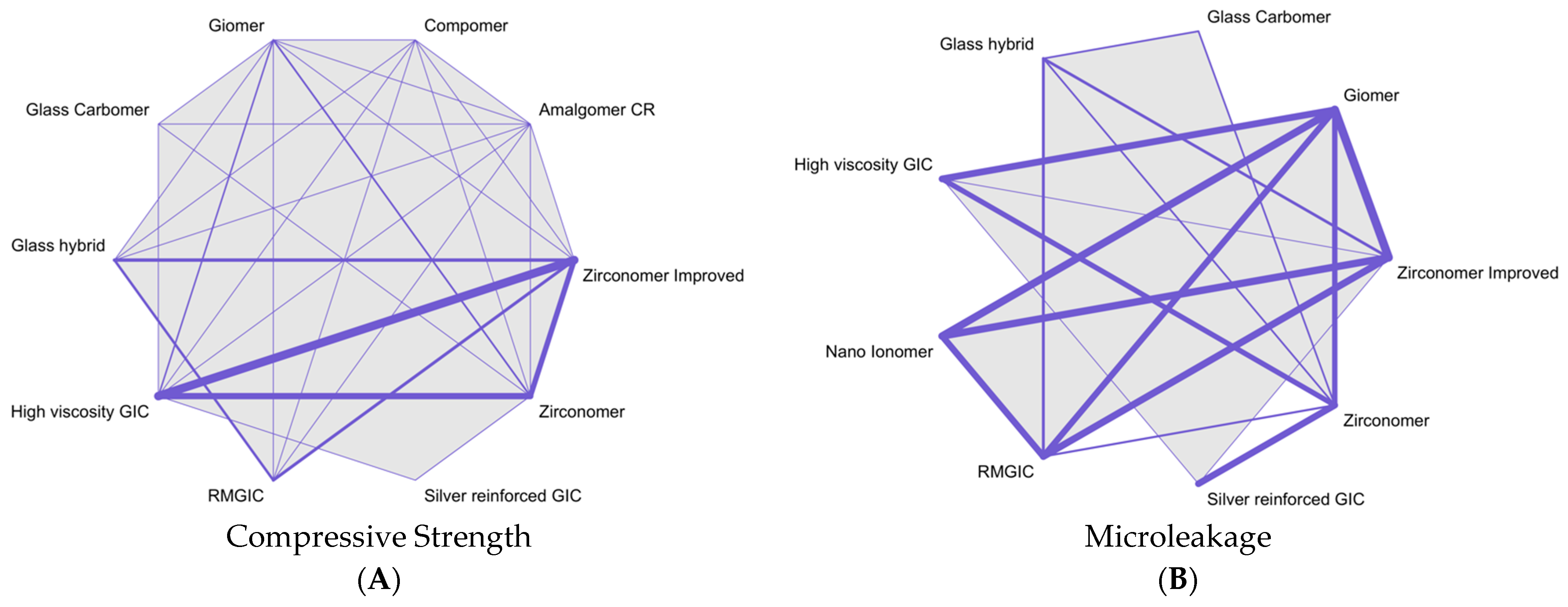
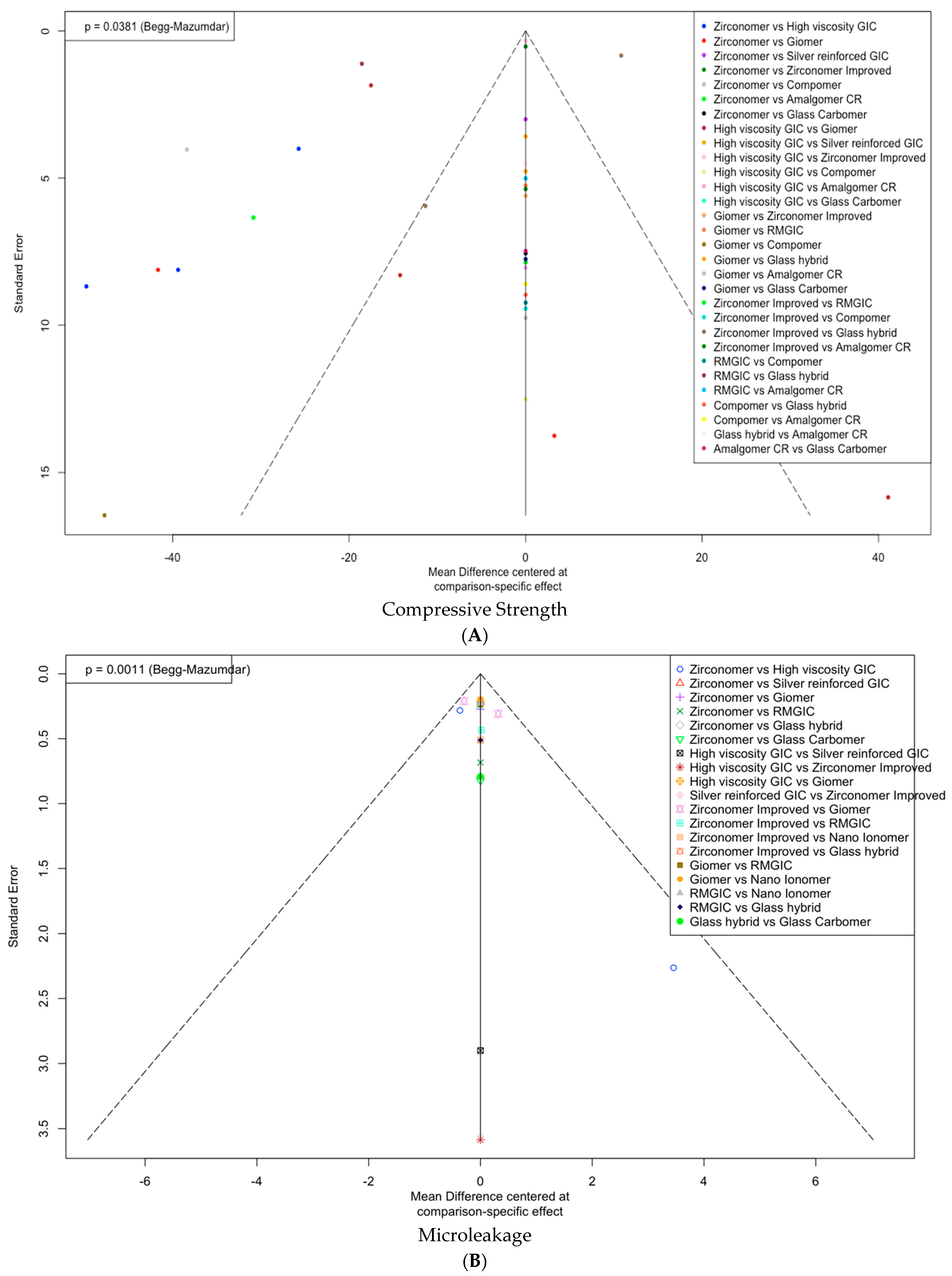
3.3.1. Compressive Strength
3.3.2. Microleakage
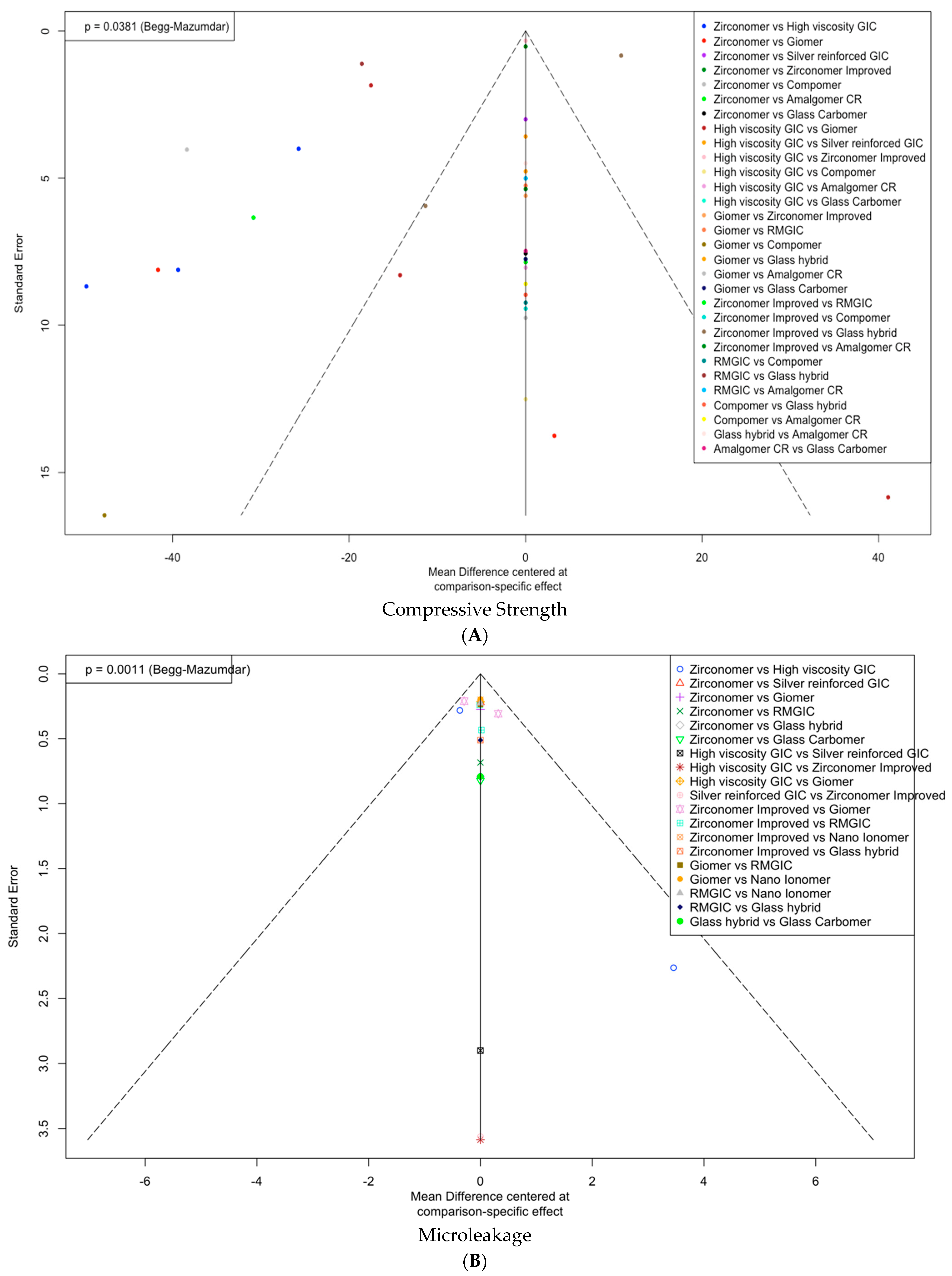
3.4. Assessment of Risk of Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Zhu, Y.; Wang, Y.; Zhang, S.; Li, J.; Li, X.; Ying, Y.; Yuan, J.; Chen, K.; Deng, S.; Wang, Q. Association of Polymicrobial Interactions with Dental Caries Development and Prevention. Front. Microbiol. 2023, 14, 1162380. [Google Scholar] [CrossRef] [PubMed]
- Fejerskov, O.; Bente, N.; Edwina, K. (Eds.) Dental Caries: The Disease and Its Clinical Management, 3rd ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2015; Volume 2, p. 235. [Google Scholar]
- Figundio, N.; Lopes, P.; Tedesco, T.K.; Fernandes, J.C.H.; Fernandes, G.V.O.; Mello-Moura, A.C.V. Deep Carious Lesions Management with Stepwise, Selective, or Non-Selective Removal in Permanent Dentition: A Systematic Review of Randomized Clinical Trials. Healthcare 2023, 11, 2338. [Google Scholar] [CrossRef]
- Pav, C.; Orlans, M.C.; O’toole, S.; Domejean, S.; Movahedi, S.; Banerjee, A. Restorative intervention thresholds and treatment decisions of general dental practitioners in London. Br. Dent. J. 2019, 227, 727–732. [Google Scholar] [CrossRef]
- Nicholson, J.W.; Sidhu, S.K.; Czarnecka, B. Fluoride exchange by glass-ionomer dental cements and its clinical effects: A review. Biomater Investig Dent. 2023, 10, 2244982. [Google Scholar] [CrossRef] [PubMed]
- Goenka, S.; Balu, R.; Kumar, T.S. Effects of nanocrystalline calcium deficient hydroxyapatite incorporation in glass ionomer cements. J. Mech. Behav. Biomed. Mater. 2012, 7, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D.; Kent, B.E. The glass-ionomer cement, a new translucent dental filling material. J. Chem. Technol. Biotechnol. 1971, 21, 313. [Google Scholar] [CrossRef]
- Nagaraja, U.P.; Kishore, G. Glass ionomer cement: The different generations. Trends Biomater. Artif. Organs 2005, 18, 158–165. [Google Scholar]
- Sidhu, S.K. Glass-ionomer cement restorative materials: A sticky subject? Aust. Dent. J. 2011, 56, 23–30. [Google Scholar] [CrossRef]
- Mount, G.J. Color Atlas of Glass Ionomer Cement, 2nd ed.; Martin Dunitz: London, UK, 2002. [Google Scholar]
- Food and Drug Administration. Dental Devices: Classification of Dental Amalgam, Reclassification of Dental Mercury, Designation of Special Controls for Dental Amalgam, Mercury, and Amalgam Alloy. Final Rule; Federal Register 74, No. 148; Food and Drug Administration, HHS: Silver Spring, MD, USA, 2009.
- Albeshti, R.; Shahid, S. Evaluation of Microleakage in Zirconomer®: A Zirconia Reinforced Glass Ionomer Cement. Acta. Stomatol. Croat. 2018, 52, 97–104. [Google Scholar] [CrossRef]
- Makanjuola, J.; Deb, S. Chemically activated glass-ionomer cements as bioactive materials in dentistry: A review. Prosthesis 2023, 5, 327–345. [Google Scholar] [CrossRef]
- Nicholson, J.W.; Sidhu, S.K.; Czarnecka, B. Enhancing the mechanical properties of glass-ionomer dental cements: A review. Materials 2020, 13, 2510. [Google Scholar] [CrossRef] [PubMed]
- Alvarenga, F.A.D.S.U.; Andrade, M.F.D.U.; Pinelli, C.; Rastelli, A.; Victorino, K.R.U.; Loffredo, L.D.C.U.M. Accuracy of digital images in the detection of marginal microleakage: An in vitro study. J. Adhes. Dent. 2012, 14, 335–338. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA Extension Statement for Reporting of Systematic Reviews Incorporating Network Meta-Analyses of Health Care Interventions: Checklist and Explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Stillwell, S.B.; Fineout-Overholt, E.; Melnyk, B.M.; Williamson, K.M. Evidence-Based Practice, Step by Step: Asking the Clinical Question: A Key Step in Evidence-Based Practice. AJN Am. J. Nurs. 2010, 110, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Joanna Briggs Institute. The Joanna Briggs Institute Critical Appraisal Tools for Use in JBI Systematic Reviews Checklist for Analytical Cross Sectional Studies; The Joanna Briggs Institute: North Adelaide, Australia, 2017. [Google Scholar]
- Krithikadatta, J.; Gopikrishna, V.; Datta, M. CRIS Guidelines (Checklist for Reporting In-Vitro Studies): A Concept Note on the Need for Standardized Guidelines for Improving Quality and Transparency in Reporting in-Vitro Studies in Experimental Dental Research. J. Conserv. Dent. 2014, 17, 301–304. [Google Scholar] [CrossRef]
- Walia, R.; Jasuja, P.; Verma, K.G.; Juneja, S.; Mathur, A.; Ahuja, L. A Comparative Evaluation of Microleakage and Compressive Strength of Ketac Molar, Giomer, Zirconomer, and Ceram-x: An in Vitro Study. J. Indian Soc. Pedod. Prev. Dent. 2016, 34, 280–284. [Google Scholar] [CrossRef]
- Bhatia, H.P.; Singh, S.; Sood, S.; Sharma, N. A comparative evaluation of sorption, solubility, and compressive strength of three different glass ionomer cements in artificial saliva: An in vitro study. Int. J. Clin. Pediatr. Dent. 2017, 10, 49–54. [Google Scholar] [CrossRef]
- Kumar, A.; Raj, A.; Singh, D.K.; Donthagani, S.; Kumar, M.; Ramesh, K. A New Zinc Reinforced Glass Ionomer Cement: A Boon in Dentistry. J. Pharm. Bioallied Sci. 2021, 13, S272–S275. [Google Scholar] [CrossRef]
- Shetty, C.; Sadananda, V.; Hegde, M.; Lagisetti, A.; Shetty, A.; Mathew, T.; Shetty, S. Comparative evaluation of compressive strength of Ketac Molar, Zirconomer, and Zirconomer Improved. Sch. J. Dent. Sci. 2017, 4, 259–261. [Google Scholar] [CrossRef]
- Patel, A.; Dalal, D.; Lakade, L.; Shah, P.; Caudhary, S.; Lodaya, R.; Vidyapeeth, B. Comparative evaluation of compressive strength and diametral tensile strength of zirconomer, ketac molar and Type IX GIC-An In-Vitro Study. J. Int. Soc. Prev. Community Dent. 2018, 10, 70091–70094. [Google Scholar] [CrossRef]
- Patil, K.M.; Hambire, U.V. Comparative Evaluation of Compressive, Flexural Strength and Micro Hardness of Different Dental Materials. Int. J. Sci. Res. Dev. 2016, 4, 444–448. [Google Scholar]
- Dhivya, S. In Vitro Comparative study of Sorption, Solubility and Compressive Strength of Three Modified Glass Ionomer Cements. Master’s Thesis, Vivekanandha Dental College for Women, Tiruchengode, India, 2020. [Google Scholar]
- Uğurlu, M. How Do the Surface Coating and One-Year Water Aging Affect the Properties of Fluoride-Releasing Restorative Materials? Niger. J. Clin. Pract. 2020, 23, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Asafarlal, S. Comparative Evaluation of Microleakage, Surface Roughness and Hardness of Three Glass Ionomer Cements–Zirconomer, Fujii IX Extra GC and Ketac Molar: An In Vitro Study. Dent. Health Curr. Res. 2017, 3, 59. [Google Scholar] [CrossRef]
- Ranadheer, E.; Shah, U.D.; Neelakantappa, K.K.; Fernandes, S. Comparative analysis of microleakage of zirconia-infused glass ionomer cement with miracle mix and amalgam: An In Vitro study. Cureus 2018, 10, e3672. [Google Scholar] [CrossRef]
- Salman, K.M.; Naik, S.B.; Kumar, N.K.; Merwade, S.; Brigit, B.; Jalan, R. Comparative evaluation of microleakage in class V cavities restored with giomer, resin-modified glass ionomer, zirconomer and nano-ionomer: An in vitro study. J. Int. Clin. Dent. Res. Organ. 2019, 11, 20. [Google Scholar] [CrossRef]
- Mahmoud, N.; Niazy, M.; Elyasaky, M. Evaluation of the Clinical Performance of Reinforced Glass Ionomer Restorations and Influence of Heat Application on Their Shear Bond Strength and Microleakage. Al-Azhar Dent. J. Girls 2020, 7, 521–529. [Google Scholar] [CrossRef]
- Sharafeddin, F.; Bakhtiarvand, N.A.; Jowkar, Z. Evaluation of the Effect of Home Bleaching Gel on Microleakage of Different Glass Ionomers Reinforced with Micro-Hydroxyapatite. J. Conserv. Dent. 2019, 22, 64–68. [Google Scholar] [CrossRef]
- Meral, E.; Baseren, N. Shear bond strength and microleakage of novel glass-ionomer cements: An in vitro study. Niger. J. Clin. Pr. 2019, 22, 566. [Google Scholar] [CrossRef]
- Ashok, L. A Comparative Evaluation of Microleakage Around Class V Cavities Restored with Five Different Tooth Coloured Restorative Materials: An In Vitro Study. Ph.D. Thesis, Sree Mookambika Institute of Denal Sciences, Kulasekharam, India, 2020. [Google Scholar]
- Kaladevi, M. Comparative Evaluation of Microleakage of Three Different Glass Ionomer Cements in Class V Cavity: An In Vitro Study. Ph.D. Thesis, Tamil Nadu Government Dental College and Hospital, Chennai, India, 2020. [Google Scholar]
- Anusavice, K.J.; Phillips, R.W.; Shen, C.; Rawls, H.R. Phillips’ Science of Dental Materials, 18th ed.; Elsevier/Saunders: St. Louis, MO, USA, 2013. [Google Scholar]
- Simmons, J.J. Silver–alloy powder and glass ionomer cement. J. Am. Dent. Assoc. 1990, 120, 49–52. [Google Scholar] [CrossRef]
- McLean, J.W.; Gasser, O. Glass-cermet cements. Quintessence Int. 1985, 16, 333–343. [Google Scholar] [PubMed]
- McCabe, J.F. Resin-modified glass-ionomers. Biomaterials 1998, 19, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.W.; Beata, C. The biocompatibility of resin-modified glass-ionomer cements for dentistry. Dent Mater. 2008, 4, 1702–1708. [Google Scholar] [CrossRef]
- Sidhu, S.K. Clinical evaluations of resin-modified glass-ionomer restorations. Dent. Mater. 2010, 26, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Amaral, R.; Özcan, M.; Valandro, L.F.; Balducci, I.; Bottino, M.A. Effect of Conditioning Methods on the Microtensile Bond Strength of Phosphate Monomer-Based Cement on Zirconia Ceramic in Dry and Aged Conditions. J. Biomed. Mater. Res. 2008, 85, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Croll, T.P.; Nicholson, J.W. Glass ionomer cements in pediatric dentistry: Review of the literature. Pediatr. Dent. 2002, 24, 423–429. [Google Scholar]
- Meyer, J.M.; Cattani-Lorente, M.A.; Dupuis, V. Compomers: Between glass-ionomer cements and composites. Biomaterials 1998, 19, 529–539. [Google Scholar] [CrossRef]
- Itota, T.; Carrick, T.E.; Yoshiyama, M.; McCabe, J.F. Fluoride Release and Recharge in Giomer, Compomer and Resin Composite. Dent. Mater. 2004, 20, 789–795. [Google Scholar] [CrossRef]
- Ulrike, M.; Ilie, N. Effect of gloss and heat on the mechanical behaviour of a glass carbomer cement. J. Dent. 2013, 41, 223–230. [Google Scholar] [CrossRef]
- Uday, K.; Salam, A. Fracture resistance of maxillary premolars with mod cavities restored with Zirconomer: An in vitro comparative study. Int. J. Appl. Dent. Sci. 2016, 2, 77–80. [Google Scholar]
- Nanavati, K.; Katge, F.; Chimata, V.K.; Pradhan, D.; Kamble, A.; Patil, D. Comparative Evaluation of Shear Bond Strength of Bioactive Restorative Material, Zirconia Reinforced Glass Ionomer Cement and Conventional Glass Ionomer Cement to the Dentinal Surface of Primary Molars: An in vitro Study. J. Dent. 2021, 4, 260. [Google Scholar] [CrossRef]
- Safy, R.K.; Elmohsen, H.A. Assessment of the Fracture Resistance of Novel Zirconia Reinforced Glass Ionomer in Comparison to Nano Hybrid Resin Composite Restorations. Egypt. Dent. J. 2019, 65, 3735–3744. [Google Scholar] [CrossRef]
- Khamverdi, Z.; Moshiri, Z. Zirconia: An up-to-date literature review. Avicenna J. Dent. Res. 2012, 4, 1–15. [Google Scholar]
- Saygili, G.; Mahmali, S.M. Comparative study of the physical properties of core materials. J. Periodontics Restor. Dent. 2002, 22, 355–363. [Google Scholar]
- Summitt, J.B.; Robbins, J.W.; Hilton, T.J.; Schwartz, R.S. Bonding to Enamel and Dentin. Fundamentals of Operative Dentistry, 3rd ed.; Quintessence Publishing Co., Inc.: Berlin, Germany, 2006; Volume 8, pp. 183–260. [Google Scholar]
- Van Noort, R.; Barbour, M.E. Introduction to Dental Materials; Elsevier Science Health Science div.: Amsterdam, The Netherlands, 2007; pp. 61–68. [Google Scholar]
- Sakaguchi, R.L.; Powers, J.M. Craig’s Restorative Dental Materials, 13th ed.; Elsevier Mosby: Amsterdam, The Netherlands, 2012; pp. 51–96. [Google Scholar]
- Cho, G.C.; Kaneko, L.M.; Donovan, T.E.; White, S.N. Diametral and Compressive Strength of Dental Core Materials. J. Prosthet. Dent. 1999, 82, 272–276. [Google Scholar] [CrossRef] [PubMed]
- Pereira, L.C.; Nunes, M.C.P.; Dibb, R.G.P.; Powers, J.M.; Roulet, J.-F.; Navarro, M.F. de L. Mechanical Properties and Bond Strength of Glass-Ionomer Cements. J. Adhes. Dent. 2002, 4, 73–80. [Google Scholar] [CrossRef]
- Nicholson, J.; Beata, C. Materials for the Direct Restoration of Teeth, 1st ed.; Woodhead Publishing: Sawston, UK, 2016; pp. 24–26. [Google Scholar]
- Prabhakar, A.R.; Thejokrishna, P.; Kurthukoti, A.J. A comparative evaluation of four restorative materials to support undermined occlusal enamel of permanent teeth. J. Indian Soc. Pedod. Prev. Dent. 2006, 24, 122–126. [Google Scholar] [CrossRef]
- Cattani-Lorente, M.A.; Godin, C.; Meyer, J.M. Early strength of glass ionomer cements. Dent. Mater. 1993, 9, 57–62. [Google Scholar] [CrossRef]
- Negm, M.M.; Beech, D.R.; Grant, A.A. An evaluation of mechanical and adhesive properties of polycarboxylate and glass ionomer cements. J. Oral Rehabil. 1982, 9, 161–167. [Google Scholar] [CrossRef]
- Anstice, H.M.; Nicholson, J.W.; McCabe, J.F. The effect of using layered specimens for determination of the compressive strength of glass-ionomer cements. J. Dent. Res. 1992, 71, 1871–1874. [Google Scholar] [CrossRef]
- Chalissery, V.P.; Nikhil, M.; Mohammed, A.; Abdulaziz, M.A.; Elna, P.C.; Shilpa, H.B.; Sukumaran, A. Study of the mechanical properties of the novel zirconia-reinforced glass ionomer cement. J. Contemp Dent. Pract. 2016, 17, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Dheeraj, M.; Johar, S.; Jandial, T.; Sahi, H.; Verma, S. Comparative Evaluation of Compressive Strength and Diametral Tensile Strength of Zirconomer with GIC and Amalgam. J. Med. Dent. Sci. 2019, 7, 52–56. [Google Scholar] [CrossRef]
- Mohanty, S.; Ramesh, S. Fracture resistance of three posterior restorative materials: A preliminary in vitro study. J. Adv. Pharm. Educ. Res. 2017, 7, 291–294. [Google Scholar]
- Ruengrungsom, C. Evaluation of Physical/Mechanical Properties, Ion Release, and Rechargeable Efficacy of Contemporary Ion-leaching Restorative Materials. Ph.D. Thesis, University of Melbourne, Melbourne, Australia, 2021. [Google Scholar]
- Xu, X.; John, O.B. Compressive strength, fluoride release and recharge of fluoride-releasing materials. Biomaterials 2003, 24, 2451–2461. [Google Scholar] [CrossRef]
- Tiwari, S.; Mallikarjuna, K.; Deepak, B.; Shilpi, G.; Sudhanshu, S.; Saurabh, S.; Aishwarya, S.; Manoj, G. Antibacterial activity and fluoride release of glass-ionomer cement, compomer and zirconia reinforced glass-ionomer cement. J. Clin. Diagn. Res. 2016, 10, ZC90–ZC93. [Google Scholar] [CrossRef]
- Castro, A.; Robert, E.F. Microleakage of a new improved glass ionomer restorative material in primary and permanent teeth. Pediatr. Dent 2002, 24, 23–28. [Google Scholar]
- Lutz, F.; Krejci, I.; Barbakow, F. Quality and durability of marginal adaptation in bonded composite restorations. Dent. Mater. 1991, 7, 107–113. [Google Scholar] [CrossRef]
- Kidd, E.A.M. Microleakage: A review. J. Dent. 1976, 4, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Brännström, M.; Vojinović, O. Response of the dental pulp to invasion of bacteria around three filling materials. ASDC J. Dent. Child. 1976, 43, 83–89. [Google Scholar]
- Oskoee, S.S.; Oskoee, P.A.; Navimipour, E.J.; Ajami, A.A.; Azar, F.P.; Rikhtegaran, S.; Amini, M. Comparison of the Effect of Nd: YAG and Diode Lasers and Photodynamic Therapy on Microleakage of Class V Composite Resin Restorations. J. Dent. Res. Dent. Clin. Dent. Prospect. 2013, 7, 74–80. [Google Scholar] [CrossRef]
- Vanishree, H.S.; Shanthala, B.M.; Bobby, W. The comparative evaluation of fracture resistance and microleakage in bonded amalgam, amalgam, and composite resins in primary molars. Indian J. Dent. Res. 2015, 26, 446–450. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.K.; Gupta, J.; Saraswathi, V.; Ballal, V.; Acharya, S.R. Comparative evaluation of microleakage in Class V cavities using various glass ionomer cements: An in vitro study. J. Interdiscip. Dent. 2012, 2, 164. [Google Scholar] [CrossRef]
- Fatima, N.; Mohiuddin, S.; Iqbal, W. Effect on Micro-Leakage of Composite Resoration with Two Different Adhesives after Bleaching. Smile Dent. J. 2015, 10, 28–32. [Google Scholar] [CrossRef]
- Karagenç, B.; Gençoǧlu, N.; Ersoy, M.; Cansever, G.; Külekçi, G. A comparison of four different microleakage tests for assessment of leakage of root canal fillings. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Alani, A.H.; Toh, C.G. Detection of microleakage around dental restorations: A review. Oper. Dent. 1997, 22, 173–185. [Google Scholar]
- Jacobsen, P.H.; Fraunhofer, J.A.V. Assessment of microleakage using a conductimetric technique. J. Dent. Res. 1975, 54, 41–48. [Google Scholar] [CrossRef]
- Going, R.E.; Howard, M.M.; Stanley, G.P. Quantitative method for studying microleakage in vivo and in vitro. J. Dent. Res. 1968, 47, 1128–1132. [Google Scholar] [CrossRef]
- Gogna, R.; Jagadis, S.; Shashikal, K. A comparative in vitro study of microleakage by a radioactive isotope and compressive strength of three nanofilled composite resin restorations. J. Conserv. Dent. 2011, 14, 128–131. [Google Scholar] [CrossRef]
- Hilton, T.J. Can modern restorative procedures and materials reliably seal cavities? In vitro investigations. Part 2. Am. J. Dent. 2002, 15, 279–289. [Google Scholar]
- Taylor, M.; Lynch, E. Microleakage. J. Dent. 1992, 20, 3–10. [Google Scholar] [CrossRef]
- Baghdadi, Z.D. Microleakage of a single-bottle adhesive system with 3 restorative materials: In vitro study and clinical considerations. Compend. Contin. Educ. Dent. 2003, 24, 755–758. [Google Scholar] [PubMed]
- Baig, M.S.; Garry, J.P.F. Conventional glass-ionomer materials: A review of the developments in glass powder, polyacid liquid and the strategies of reinforcement. J. Dent. 2015, 43, 897–912. [Google Scholar] [CrossRef] [PubMed]
- Barbhai, S.; Shetty, R.; Joshi, P.; Mehta, V.; Mathur, A.; Sharma, T.; Chakraborty, D.; Porwal, P.; Meto, A.; Wahjuningrum, D.A.; et al. Evaluation of Root Anatomy and Canal Configuration of Human Permanent Maxillary First Molar Using Cone-Beam Computed Tomography: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 10160. [Google Scholar] [CrossRef] [PubMed]
- Souza, P.P.; Aranha, A.M.; Hebling, J.; Giro, E.M.; de Souza Costa, C.A. In vitro cytotoxicity and in vivo biocompatibility of contemporary resin-modified glass-ionomer cements. Dent. Mater. 2006, 22, 838–844. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year | Study Design | Property Tested | Population | Intervention | Comparative | Sample Size | Dimensions of Specimen |
|---|---|---|---|---|---|---|---|
| Walia R/2016 [21] | Comparative cross-sectional study | Compressive strength | Cylindrical cement specimens | Zirconomer | High-viscosity GIC | 15 | 5 mm × 6 mm |
| Giomer | 5 mm × 6 mm | ||||||
| Bhatia H/2017 [22] | Comparative cross-sectional study | Compressive strength | Cylindrical cement specimens | Zirconomer | High-viscosity GIC | 15 | 4 mm × 6 mm |
| Silver-reinforced GIC | 4 mm × 6 mm | ||||||
| Canturk K/2020 [23] | Comparative cross-sectional study | Compressive strength | Cylindrical cement specimens | Zirconomer-improved | RMGIC | 10 | 4 mm × 6 mm |
| Compomer | 4 mm × 6 mm | ||||||
| Glass hybrid | 4 mm × 6 mm | ||||||
| Giomer | 4 mm × 6 mm | ||||||
| Amalgomer CR | 4 mm × 6 mm | ||||||
| Shetty C/2017 [24] | Comparative cross-sectional study | Compressive strength | Cylindrical cement specimens | Zirconomer | High-viscosity GIC | 10 | 3 mm × 6 mm |
| Zirconomer-improved | 3 mm × 6 mm | ||||||
| Patel A/2018 [25] | Comparative cross-sectional study | Compressive strength | Cylindrical cement specimens | Zirconomer | High-viscosity GIC | 10 | 6 mm × 12 mm |
| Patil K/2016 [26] | Comparative cross-sectional study | Compressive strength | Cylindrical cement specimens | Zirconomer | Giomer | 5 | 5 mm × 5 mm |
| High-viscosity GIC | 5 mm × 5 mm | ||||||
| Compomer | 5 mm × 5 mm | ||||||
| S Dhivya/2017-2020 [27] | Comparative cross-sectional study | Compressive strength | Cylindrical cement specimens | Zirconomer-improved | Glass Hybrid | 15 | 4 mm × 6 mm |
| RMGIC | 4 mm × 6 mm | ||||||
| Uğurlu M/2020 [28] | Comparative cross-sectional study | Compressive strength | Cylindrical cement specimens | Zirconomer | Glass Carbomer | 10 | 4 mm × 6 mm |
| Amalgomer CR | 4 mm × 6 mm | ||||||
| High-viscosity GIC | 4 mm × 6 mm | ||||||
| Giomer | 4 mm × 6 mm |
| Author/Year | Study Design | Property Tested | Population | Intervention | Comparative | Sample Size | Test Type Used | Dye Used | Microscopy |
|---|---|---|---|---|---|---|---|---|---|
| Asafarlal S/2017 [29] | In vitro study | Microleakage | Premolar teeth | Zirconomer | High viscosity GIC | 15 | Dye absorbance | Methylene blue | Spectrophotometry |
| Ranadheer E/2018 [30] | In vitro study | Microleakage | Premolar teeth | Zirconomer | Silver reinforced GIC | 10 | Dye penetration | Methylene blue | Stereomicroscopy |
| Mohammed Salman K/2019 [31] | In vitro study | Microleakage | Premolar teeth | Zirconomer-improved | Giomer | 15 | Dye penetration | Methylene blue | Stereomicroscopy |
| RMGIC | |||||||||
| Nano ionomer | |||||||||
| Mahmoud N/2020 [32] | In vitro study | Microleakage | Molar teeth | Zirconomer-improved | Glass hybrid | 10 | Dye penetration | Methylene blue | Stereomicroscopy |
| RMGIC | |||||||||
| Sharafeddin F/2019 [33] | In vitro study | Microleakage | Molar teeth | Zirconomer | RMGIC | 5 | Dye penetration | Basic fuchsine | Stereomicroscopy |
| Meral E/2019 [34] | In vitro study | Microleakage | Molar teeth | Zirconomer | Glass hybrid | 8 | Dye penetration | Basic fuchsine | Stereomicroscopy |
| Glass Carbomer | |||||||||
| Ashok L/2017–2020 [35] | In vitro study | Microleakage | Premolar teeth | Zirconomer-improved | Giomer | 8 | Dye penetration | Silver nitrate | Stereomicroscopy |
| Kaladevi M/2017–2020 [36] | In vitro study | Microleakage | Premolar teeth | Zirconomer-improved | High viscosity GIC | 10 | Dye Penetration | Silver paint | SEM |
| Silver reinforced GIC | |||||||||
| Walia R/2016 [21] | Comparative cross-sectional study | Microleakage | Premolar teeth | Zirconomer | High viscosity GIC | 15 | Dye penetration | Methylene blue | Stereomicroscopy |
| Comparison Compound | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Amalgomer CR | −64.73 (−119.78; −9.68) | −65.85 (−103.93; −27.78) | 10.76 (−43.66; 65.18) | −6.59 (−59.73; 46.55) | −12.87 (−67.60; 41.86) | −21.63 (−74.95; 31.69) | 1.03 (−53.59; 55.65) | −3.44 (−56.90; 50.02) | ||
| −119.76 (−161.84; −77.68) | Compomer * | 75.58 (34.52; 116.64) | 58.14 (2.86; 113.42) | 161.90 (104.04; 219.76) | 43.10 (−12.35; 98.55) | 186.20 (130.41; 241.99) | 61.29 (5.71; 116.87) | |||
| −56.20 (−91.20; −21.19) | 63.56 (26.58; 100.55) | Giomer * | 117.54 (62.97; 172.11) | 20.88 (−32.36; 74.12) | 79.69 ( 47.48; 111.89) | 5.84 (−47.57; 59.25) | 66.16 (34.28; 98.03) | 24.03 (−29.52; 77.58) | ||
| 32.24 (−17.09; 81.58) | 152.00 (97.52; 206.48) | 88.44 (41.84; 135.04) | Glass Carbomer | −23.63 (−78.20; 30.94) | . | −9.73 (−64.19; 44.73) | ||||
| Intervention compound | −26.26 (−68.86; 16.34) | 93.49 (49.38; 137.61) | 29.93 (−10.19; 70.05) | −58.51 (−115.14; −1.87) | Glass hybrid | 4.31 (−33.17; 41.78) | −8.20 (−45.71; 29.31) | |||
| 24.60 (−11.41; 60.62) | 144.36 (106.83; 181.89) | 80.80 (53.13; 108.47) | −7.64 (−53.68; 38.40) | 50.87 (9.15; 92.58) | High viscosity GIC | −46.90 (−99.78; 5.98) | −25.48 (−47.29; −3.67) | −40.70 (−93.11; 11.71) | ||
| −21.89 (−64.58; 20.79) | 97.86 (53.67; 142.06) | 34.30 (−5.91; 74.51) | −54.14 (−110.83; 2.55) | 4.37 (−33.10; 41.84) | −46.50 (−88.29; −4.71) | RMGIC | −12.65 (−50.23; 24.92) | |||
| −6.69 (−63.81; 50.43) | 113.07 (55.03; 171.11) | 49.51 (−2.74; 101.76) | −38.93 (−102.86; 24.99) | 19.57 (−41.29; 80.44) | −31.29 (−78.29; 15.71) | 15.21 (−45.72; 76.13) | Silver reinforced GIC | −9.44 (−62.18; 43.30) | . | |
| −0.68 (−36.59; 35.22) | 119.07 (81.79; 156.35) | 55.51 (28.03; 82.99) | −32.93 (−78.90; 13.05) | 25.58 (−16.02; 67.18) | −25.29 (−47.09; −3.48) | 21.21 (−20.47; 62.89) | 6.00 ( −40.97; 52.98) | Zirconomer | 19.69 (−32.73; 72.11) | |
| −25.33 (−63.87; 13.21) | 94.43 (54.31; 134.55) | 30.87 (−3.72; 65.45) | −57.57 (−109.84; −5.31) | 0.93 (−34.92; 36.79) | −49.93 (−83.98; −15.89) | −3.43 (−39.36; 32.49) | −18.64 (−74.55; 37.26) | −24.64 (−58.59; 9.30) | Zirconomer-improved | |
| Comparison Compound | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Giomer | 0.82 (−0.66; 2.30) | 1.04 (−0.43; 2.50) | 0.77 (−0.72; 2.25) | 0.53 (−0.98; 2.04) | −0.06 (−1.12; 1.01) | ||||
| −0.89 (−3.06; 1.27) | Glass Carbomer | 1.37 (−0.73; 3.47) | 1.42 (−0.73; 3.57) | ||||||
| 0.47 (−1.02; 1.96) | 1.36 (−0.61; 3.33) | Glass hybrid | 0.16 (−1.57; 1.90) | 0.05 (−2.05; 2.15) | −0.40 (−2.13; 1.33) | ||||
| 0.69 (−0.67; 2.05) | 1.58 (−0.75; 3.92) | 0.22 (−1.59; 2.03) | High viscosity GIC | 10.22 (4.36; 16.07) | −0.66 ( −2.10; 0.79) | 0.89 (−6.28; 8.06) | |||
| Intervention compound | 0.93 (−0.41; 2.26) | 1.82 (−0.58; 4.22) | 0.46 (−1.31; 2.23) | 0.24 (−1.59; 2.06) | Nano ionomer | −0.27 (−1.75; 1.21) | −0.80 (−2.27; 0.67) | ||
| 0.72 (−0.38; 1.81) | 1.61 (−0.54; 3.76) | 0.25 (−1.14; 1.63) | 0.03 (−1.55; 1.61) | −0.21 (−1.57; 1.15) | RMGIC | −0.65 (−2.60; 1.30) | −0.54 (−1.65; 0.56) | ||
| 0.40 (−1.41; 2.22) | 1.30 (−1.15; 3.74) | −0.06 (−2.08; 1.96) | −0.28 (−2.19; 1.62) | −0.52 (−2.65; 1.61) | −0.31 (−2.18; 1.55) | Silver reinforced GIC | 0.90 (−0.58; 2.38) | −9.32 (−16.45; −2.20) | |
| 0.54 (−0.63; 1.71) | 1.43 (−0.56; 3.42) | 0.07 (−1.38; 1.52) | −0.15 (−1.49; 1.18) | −0.39 (−2.01; 1.23) | −0.18 (−1.42; 1.06) | 0.13 (−1.30; 1.56) | Zirconomer | ||
| −0.04 (−1.01; 0.93) | 0.85 (−1.32; 3.02) | −0.51 (−1.91; 0.90) | −0.73 (−2.29; 0.83) | −0.97 (−2.29; 0.35) | −0.76 (−1.78; 0.26) | −0.45 (−2.34; 1.45) | −0.58 (−1.88; 0.72) | Zirconomer-improved | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manisha, S.; Shetty, S.S.; Mehta, V.; SA, R.; Meto, A. A Comprehensive Evaluation of Zirconia-Reinforced Glass Ionomer Cement’s Effectiveness in Dental Caries: A Systematic Review and Network Meta-Analysis. Dent. J. 2023, 11, 211. https://doi.org/10.3390/dj11090211
Manisha S, Shetty SS, Mehta V, SA R, Meto A. A Comprehensive Evaluation of Zirconia-Reinforced Glass Ionomer Cement’s Effectiveness in Dental Caries: A Systematic Review and Network Meta-Analysis. Dentistry Journal. 2023; 11(9):211. https://doi.org/10.3390/dj11090211
Chicago/Turabian StyleManisha, Srikurmam, Soumya S Shetty, Vini Mehta, Rizwan SA, and Aida Meto. 2023. "A Comprehensive Evaluation of Zirconia-Reinforced Glass Ionomer Cement’s Effectiveness in Dental Caries: A Systematic Review and Network Meta-Analysis" Dentistry Journal 11, no. 9: 211. https://doi.org/10.3390/dj11090211
APA StyleManisha, S., Shetty, S. S., Mehta, V., SA, R., & Meto, A. (2023). A Comprehensive Evaluation of Zirconia-Reinforced Glass Ionomer Cement’s Effectiveness in Dental Caries: A Systematic Review and Network Meta-Analysis. Dentistry Journal, 11(9), 211. https://doi.org/10.3390/dj11090211