
Temporal and Permanent Changes Induced by Maxillary Sinus Lifting with Bone Grafts and Maxillary Functional Endoscopic Sinus Surgery in the Voice Characteristics—Systematic Review




Abstract
1. Introduction
- Sinus lift + bone graft
- Sinus lift + bone graft + implant insertion
- Sinus lift + implant insertion without bone graft
- Sinus endoscopic surgery
2. Materials and Methods
2.1. Selection Criteria
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
2.1.3. Definition of Variables
Sinus Lifting with Bone Grafts
Functional Endoscopic Surgery (FESS) of the Maxillary Sinus
Voice Temporal Change
Voice Permanent Change
2.2. Evaluators’ Calibration
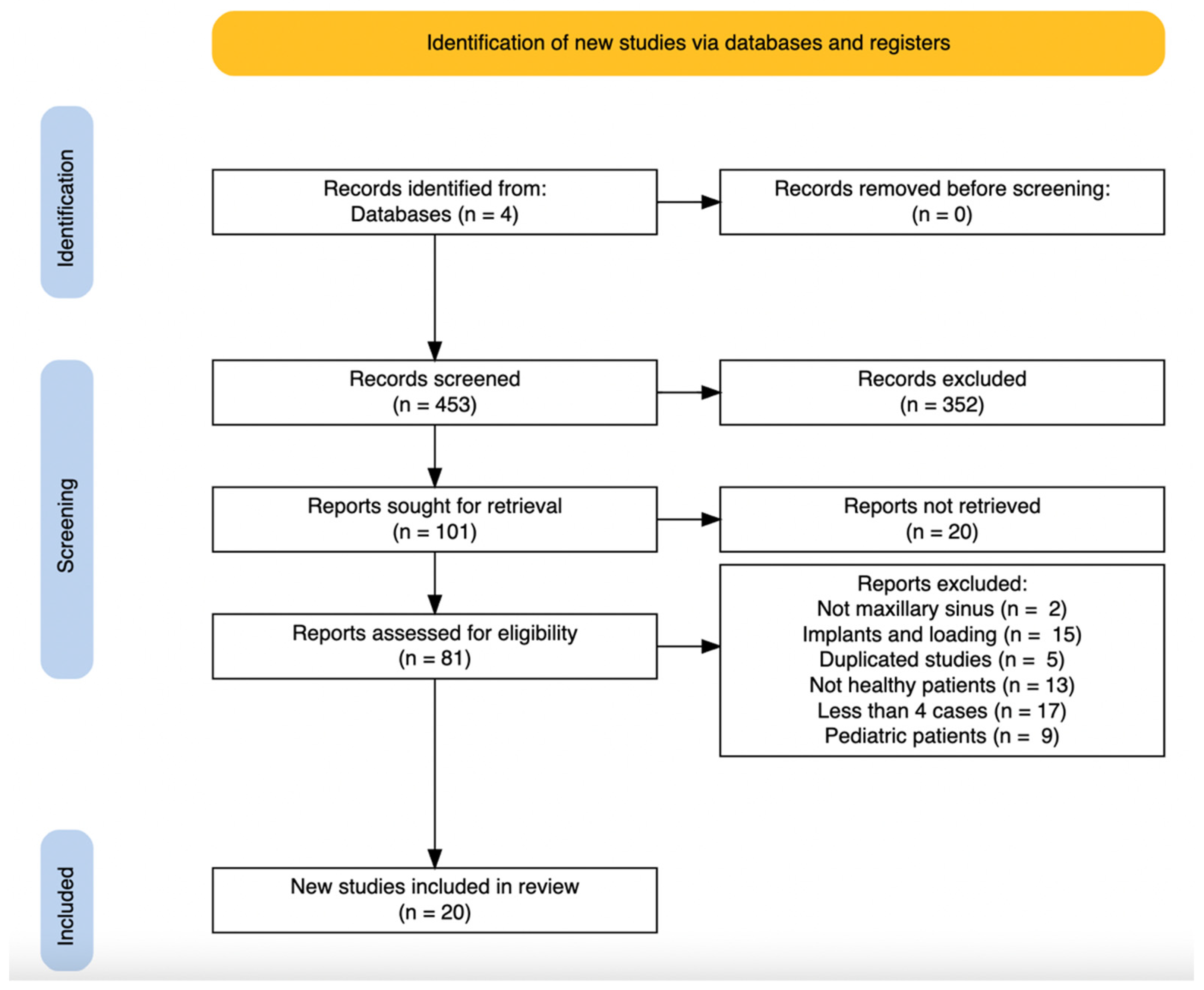
2.3. Article Selection
2.4. Data Collection
2.5. Risk of Bias
2.6. Data Analysis
3. Results
3.1. Sinus Elevation with Bone Graft
3.2. Functional Endoscopic Sinus Surgery
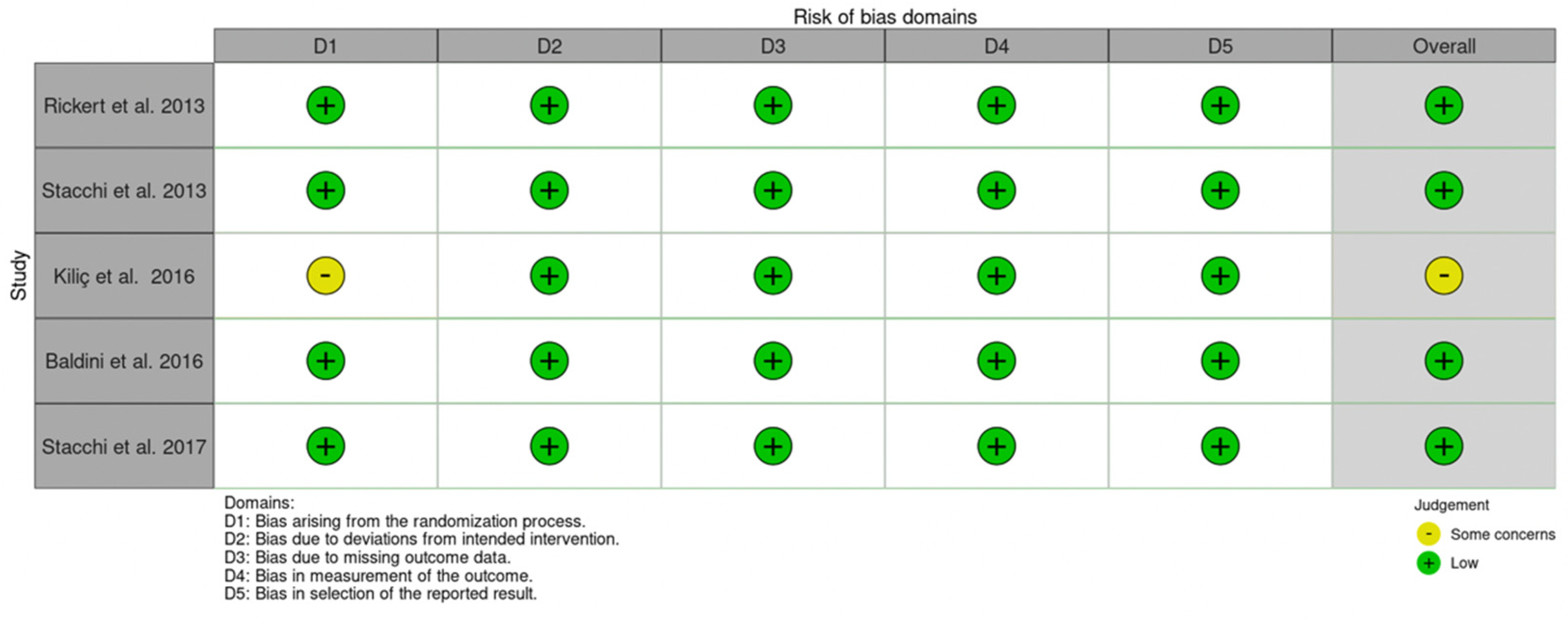
3.3. Risk of Bias Assessment for the Included Studies on Sinus Lifting with Bone Grafting
3.4. Risk of Bias Assessment for the Included Studies on FESS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sataloff, R.; Heman-Ackah, Y.; Hawkshaw, M. Clinical anatomy and physiology of the voice. Otolaryngol. Clin. N. Am. 2007, 40, 909–929. [Google Scholar] [CrossRef] [PubMed]
- Echternach, M.; Markl, M.; Richter, B. Dynamic real-time magnetic resonance imaging for the analysis of voice physiology. Curr. Opin. Otolaryngol. Head Neck Surg. 2012, 20, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Kummer, A. Disorders of Resonance and Airflow Secondary to Cleft Palate and/or Velopharyngeal Dysfunction. Semin. Speech Lang. 2011, 32, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Saggio, G.; Costantini, G. Worldwide Healthy Adult Voice Baseline Parameters: A Comprehensive Review. J. Voice, 2020; in press. [Google Scholar] [CrossRef]
- Pinyopodjanard, S.; Suppakitjanusant, P.; Lomprew, P.; Kasemkosin, N.; Chailurkit, L.; Ongphiphadhanakul, B. Instrumental Acoustic Voice Characteristics in Adults with Type 2 Diabetes. J. Voice 2021, 35, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Whalen, D.; Levitt, A. The universality of intrinsic F0 of vowels. J. Phon. 1995, 23, 349–366. [Google Scholar] [CrossRef]
- Reubold, U.; Harrington, J.; Kleber, F. Vocal aging effects on F0 and the first formant: A longitudinal analysis in adult speakers. Speech Commun. 2010, 52, 638–651. [Google Scholar] [CrossRef]
- Hassan, E.; Abdel Hady, A.; Shohdi, S.; Eldessouky, H.; Din, M. Assessment of dysphonia: Cepstral analysis versus conventional acoustic analysis. Logoped. Phoniatr. Vocology 2021, 46, 99–109. [Google Scholar] [CrossRef]
- Upadhya, S.; Cheeran, A.; Nirmal, J. Statistical comparison of Jitter and Shimmer voice features for healthy and Parkinson affected persons. In Proceedings of the 2017 Second International Conference on Electrical, Computer and Communication Technologies (ICECCT), Coimbatore, India, 22–24 February 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 1–6. [Google Scholar]
- Ferrand, C. Harmonics-to-noise ratio: An index of vocal aging. J. Voice 2002, 16, 480–487. [Google Scholar] [CrossRef]
- Sousa, R.; Ferreira, A.; Alku, P. The harmonic and noise information of the glottal pulses in speech. Biomed. Signal Process. Control 2014, 10, 137–143. [Google Scholar] [CrossRef][Green Version]
- Havel, M.; Hofmann, G.; Mürbe, D.; Sundberg, J. Contribution of paranasal sinuses to the acoustic properties of the nasal tract. Folia Phoniatr. Logop. 2014, 66, 109–114. [Google Scholar] [CrossRef]
- Bunton, K.; Story, B. The relation of nasality and nasalance to nasal port area based on a computational model. Cleft Palate-Craniofacial J. 2012, 49, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Park, H.; Kim, G.; Wang, S.; Roh, H.; Cho, K. Changes and recovery of voice quality after sinonasal surgery. Eur. Arch. Otorhinolaryngol. 2015, 272, 2853–2859. [Google Scholar] [CrossRef] [PubMed]
- Viswanath, N.; Rosenfield, D.; Baskin, D.; Wieber, S. Transient speech compromise following sublabial transsphenoidal surgery: A case report and findings of a small preliminary study. Ear Nose Throat J. 2000, 79, 286–289. [Google Scholar] [CrossRef]
- Kim, B.; Shin, J.; Kim, S.; Hong, Y.; Jeun, S.; Kim, S.; Hwang, J.; Yoo, S.; Lee, Y.; Shim, M.; et al. Hypernasality after using the endoscopic endonasal transsphenoidal approach for skull base tumors. Laryngoscope 2016, 126, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Kirk, E. Nasal’ speech–hyper or hypo. Eur. J. Hum. Genet. 2012, 20, 367. [Google Scholar] [CrossRef]
- Tepper, G.; Haas, R.; Schneider, B.; Watzak, G.; Mailath, G.; Jovanovic, S.A.; Busenlechner, D.; Zechner, W.; Watzek, G. Effects of sinus lifting on voice quality. A prospective study and risk assessment. Clin. Oral Implant. Res. 2003, 14, 767–774. [Google Scholar] [CrossRef]
- Ungor, C.; Saridoğan, C.; Yilmaz, M.; Tosun, E.; Senel, F.C.; Icten, O. An acoustical analysis of the effects of maxillary sinus augmentation on voice quality. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 175–184. [Google Scholar] [CrossRef]
- Stern, A.; Green, J. Sinus lift procedures: An overview of current techniques. Dent. Clin. N. Am. 2012, 56, 219–233. [Google Scholar] [CrossRef]
- Carrao, V.; DeMatteis, I. Maxillary sinus bone augmentation techniques. Oral Maxillofac. Surg. Clin. N. Am. 2015, 27, 245–253. [Google Scholar] [CrossRef]
- Danesh-Sani, S.A.; Loomer, P.M.; Wallace, S.S. A comprehensive clinical review of maxillary sinus floor elevation: Anatomy, techniques, biomaterials and complications. Br. J. Oral Maxillofac. Surg. 2016, 54, 724–730. [Google Scholar] [CrossRef]
- Gupta, K.K.; Jolly, K.; Bhamra, N.; Osborne, M.S.; Ahmed, S.K. The evolution of sinus surgery in England in the last decade—An observational study. World J. Otorhinolaryngol. Head Neck Surg. 2020, 7, 240–246. [Google Scholar] [CrossRef] [PubMed]
- McCormick, J.P.; Hicks, M.D.; Grayson, J.W.; Woodworth, B.A.; Cho, D.Y. Endoscopic Management of Maxillary Sinus Diseases of Dentoalveolar Origin. Oral Maxillofac. Surg. Clin. N. Am. 2020, 32, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Aukštakalnis, R.; Simonavičiūtė, R.; Simuntis, R. Treatment options for odontogenic maxillary sinusitis: A review. Stomatologija 2018, 20, 22–26. [Google Scholar] [PubMed]
- Hara, Y.; Shiratsuchi, H.; Tamagawa, T.; Koshi, R.; Miya, C.; Nagasaki, M.; Ohyama, T.; Oka, S.; Sakashita, H.; Kaneko, T. A large-scale study of treatment methods for foreign bodies in the maxillary sinus. J. Oral Sci. 2018, 60, 321–328. [Google Scholar] [CrossRef]
- Akhlaghi, F.; Esmaeelinejad, M.; Safi, P. Etiologies and Treatments of Odontogenic Maxillary sinusisit. Iran. Red Crescent Med. J. 2015, 17, e25536. [Google Scholar] [CrossRef]
- Ashman, A.; Psaltis, A.J.; Wormald, P.J.; Tan, N.C.-W. Extended endoscopic approaches to the maxillary sinus. J. Laryngol. Otol. 2020, 134, 473–480. [Google Scholar] [CrossRef]
- Soardi, C.M.; Soardi, B.; Wang, H.L. Crestal Window Sinus Lift and Its Long-Term Clinical Outcomes. Int. J. Periodontics Restor. Dent. 2020, 40, 757–764. [Google Scholar] [CrossRef]
- Sbordone, C.; Toti, P.; Guidetti, F.; Califano, L.; Bufo, P.; Sbordone, L. Volume changes of autogenous bone after sinus lifting and grafting procedures: A 6-year computerized tomographic follow-up. J. Craniomaxillofac Surg. 2013, 41, 235–241. [Google Scholar] [CrossRef]
- Pesce, P.; Menini, M.; Canullo, L.; Khijmatgar, S.; Modenese, L.; Gallifante, G.; Del Fabbro, M. Radiographic and Histomorphometric Evaluation of Biomaterials Used for Lateral Sinus Augmentation: A Systematic Review on the Effect of Residual Bone Height and Vertical Graft Size on New Bone Formation and Graft Shrinkage. J. Clin. Med. 2021, 10, 4996. [Google Scholar] [CrossRef]
- Regev, E.; Smith, R.A.; Perrott, D.H.; Pogrel, M.A. Maxillary sinus complications related to endosseous implants. Int. J. Oral Maxillofac. Implant. 1995, 10, 451–461. [Google Scholar]
- Timmenga, N.M.; Raghoebar, G.M.; van Weissenbruch, R.; Vissink, A. Maxillary sinusitis after augmentation of the maxillary sinus floor: A report of 2 cases. J. Oral Maxillofac. Surg. 2001, 59, 2004. [Google Scholar] [CrossRef] [PubMed]
- Pignataro, L.; Mantovani, M.; Torretta, S.; Felisati, G.; Sambataro, G. ENT assessment in the integrated management of candidate for (maxillary) sinus lift. Acta Otorhinolaryngol. Ital. 2008, 28, 110–119. [Google Scholar] [PubMed]
- Kennedy, D.W.; Adappa, N.D. Endoscopic maxillary antrostomy: Not just a simple procedure. Laryngoscope 2011, 121, 2142–2145. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.L.; Wang, Y.Y.; Yang, Z.H.; Huang, D.; Weng, H.; Zeng, X.-T. Methodological quality (risk of bias) assessment tools for primary and secondary medical studies: What are they and which is better? Mil. Med. Res. 2020, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomized trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. CASP (for Cohort Studies) Checklist. 2019. Available online: https://casp-uk.net/casp-tools-checklists/cohort (accessed on 10 October 2021).
- Munn, Z.; Barker, T.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: An introduction to the JBI critical appraisal tool. JBI Evid. Synth. 2020, 18, 2127–2133. [Google Scholar] [CrossRef]
- Haddaway, N.R.; McGuinness, L.A.; Pritchard, C.C. PRISMA2020: R package and ShinyApp for producing PRISMA 2020 compliant flow diagrams. Zenodo 2021. [Google Scholar] [CrossRef]
- Shlomi, B.; Horowitz, I.; Kahn, A.; Dobriyan, A.; Chaushu, G. The effect of sinus membrane perforation and repair with Lambone on the outcome of maxillary sinus floor augmentation: A radiographic assessment. Int. J. Oral Maxillofac. Implant. 2004, 19, 559–562. [Google Scholar]
- Barone, A.; Crespi, R.; Aldini, N.N.; Fini, M.; Giardino, R.; Covani, U. Maxillary sinus augmentation: Histologic and histomorphometric analysis. Int. J. Oral Maxillofac. Implant. 2005, 20, 519–525. [Google Scholar]
- Barone, A.; Santini, S.; Marconcini, S.; Giacomelli, L.; Gherlone, E.; Covani, U. Osteotomy and membrane elevation during the maxillary sinus augmentation procedure. A comparative study: Piezoelectric device vs. conventional rotative instruments. Clin. Oral Implant. Res. 2008, 19, 511–515. [Google Scholar] [CrossRef] [PubMed]
- Ucer, C. Nasal suction technique for maxillary sinus floor elevation: A report of 24 consecutive patients. Int. J. Oral Maxillofac. Implant. 2009, 24, 1138–1143. [Google Scholar]
- Taschieri, S.; Corbella, S.; Del Fabbro, M. Use of plasma rich in growth factor for schneiderian membrane management during maxillary sinus augmentation procedure. J. Oral Implantol. 2012, 38, 621–627. [Google Scholar] [CrossRef] [PubMed]
- Rickert, D.; Vissink, A.; Huddleston Slater, J.; Meijer, H.; Raghoebar, G. Comparison between conventional and piezoelectric surgical tools for maxillary sinus floor elevation. A randomized controlled clinical trial. Clin. Implant Dent. Relat. Res. 2013, 15, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Stacchi, C.; Vercellotti, T.; Toschetti, A.; Speroni, S.; Salgarello, S.; Di Lenarda, R. Intraoperative complications during sinus floor elevation using two different ultrasonic approaches: A two-center, randomized, controlled clinical trial. Clin. Implant Dent. Relat. Res. 2015, 17 (Suppl. 1), e11725. [Google Scholar] [CrossRef] [PubMed]
- Lie, N.; Merten, H.A.; Meyns, J.; Lethaus, B.; Wiltfang, J.; Kessler, P. Elevation of the maxillary sinus membrane for de-novo bone formation: First results of a prospective study in humans. J. Craniomaxillofac Surg. 2015, 43, 1670–1677. [Google Scholar] [CrossRef]
- Schwarz, L.; Schiebel, V.; Hof, M.; Ulm, C.; Watzek, G.; Pommer, B. Risk Factors of Membrane Perforation and Postoperative Complications in Sinus Floor Elevation Surgery: Review of 407 Augmentation Procedures. J. Oral Maxillofac. Surg. 2015, 73, 1275–1282. [Google Scholar] [CrossRef]
- Kiliç, S.C.; Güngörmüş, M. Cone Beam Computed Tomography Assessment of Maxillary Sinus Floor Augmentation Using Beta-Tricalcium Phosphate Alone or in Combination with Platelet-Rich Plasma: A Randomized Clinical Trial. Int. J. Oral Maxillofac. Implant. 2016, 31, 1367–1375. [Google Scholar] [CrossRef]
- Baldini, N.; D’Elia, C.; Bianco, A.; Goracci, C.; de Sanctis, M.; Ferrari, M. Lateral approach for sinus floor elevation: Large versus small bone window—A split-mouth randomized clinical trial. Clin. Oral Implant. Res. 2017, 28, 974–981. [Google Scholar] [CrossRef]
- Alayan, J.; Ivanovski, S. A prospective controlled trial comparing xenograft/autogenous bone and collagen-stabilized xenograft for maxillary sinus augmentation— Complications, patient-reported outcomes and volumetric analysis. Clin. Oral Implant. Res. 2018, 29, 248–262. [Google Scholar] [CrossRef]
- Stacchi, C.; Lombardi, T.; Cusimano, P.; Berton, F.; Lauritano, F.; Cervino, G.; Di Lenarda, R.; Cicciù, M. Bone Scrapers Versus Piezoelectric Surgery in the Lateral Antrostomy for Sinus Floor Elevation. J. Craniofac. Surg. 2017, 28, 1191–1196. [Google Scholar] [CrossRef] [PubMed]
- López-Quiles, J.; Melero-Alarcón, C.; Cano-Duran, J.; Sánchez-Martínez- Sauceda, E.; Ortega, R. Maxillary sinus balloon lifting and deferred implantation of 50 osseointegrated implants: A prospective, observational, non-controlled study. Int. J. Oral Maxillofac. Surg. 2018, 47, 1343–1349. [Google Scholar] [CrossRef] [PubMed]
- Penttilä, M.A.; Rautiainen, M.E.; Pukander, J.S.; Karma, P.H. Endoscopic versus Caldwell-Luc approach in chronic maxillary sinusitis: Comparison of symptoms at one-year follow-up. Rhinology 1994, 32, 161–165. [Google Scholar] [PubMed]
- Chiapasco, M.; Felisati, G.; Maccari, A.; Borloni, R.; Gatti, F.; Di Leo, F. The management of complications following displacement of oral implants in the paranasal sinuses: A multicenter clinical report and proposed treatment protocols. Int. J. Oral Maxillofac. Surg. 2009, 38, 1273–1278. [Google Scholar] [CrossRef]
- Hernández-García, E.; Moro-Velázquez, L.; González-Herranz, R.; Godino-Llorente, J.I.; Plaza, G. Effect of Functional Endoscopic Sinus Surgery on Voice and Speech Recognition. J. Voice 2020, 34, 650.e1–650.e6. [Google Scholar] [CrossRef]
- Yadav, S.P.S.; Singh, K.; Gulia, J.S.; Hooda, A. Swing door technique for uncinectomy versus standard technique: A comparative study. Singap. Med. J. 2021, 62, 92–95. [Google Scholar] [CrossRef]
- Yang, K.L.; Luo, S.D.; Tsai, M.H.; Chang, Y.; Kuo, H.Y.; Chen, W.C. Nasality outcome in unilateral chronic rhinosinusitis following functional endoscopic sinus surgery. J. Formos. Med. Assoc. 2021; in press. [Google Scholar] [CrossRef]
- Stacchi, C.; Andolsek, F.; Berton, F.; Perinetti, G.; Navarra, C.O.; Di Lenarda, R. Intraoperative Complications During Sinus Floor Elevation with Lateral Approach: A Systematic Review. Int. J. Oral Maxillofac. Implant. 2017, 32, e107–e118. [Google Scholar] [CrossRef]
- Ghasemi, S.; Fotouhi, A.; Moslemi, N.; Chinipardaz, Z.; Kolahi, J.; Paknejad, M. Intra- and Postoperative Complications of Lateral Maxillary Sinus Augmentation in Smokers vs Nonsmokers: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2017, 32, 759–767. [Google Scholar] [CrossRef]
- Schlund, M.; Meeus, J.; Politis, C.; Ferri, J. Management of sinus graft infection-a systematic review. Int. J. Oral Maxillofac. Surg. 2021; in press. [Google Scholar] [CrossRef]
- Bitner, B.F.; Prasad, K.R.; Goshtasbi, K.; Dunn, B.S.; Kuan, E.C. Outcomes of Concurrent Functional Endoscopic Sinus Surgery and Rhinoplasty: A Meta-analysis. Am. J. Rhinol. Allergy 2021, 35, 587–595. [Google Scholar] [CrossRef]
- Kim, E.; Duncavage, J. Prevention and management of complications in maxillary sinus surgery. Otolaryngol. Clin. N. Am. 2010, 43, 865–873. [Google Scholar] [CrossRef]
- Kim, S.; Ward, L.A.; Butaric, L.N.; Maddux, S.D. Ancestry-based variation in maxillary sinus anatomy: Implications for health disparities in sinonasal disease. Anat. Rec. 2022, 305, 18–36. [Google Scholar] [CrossRef] [PubMed]
- Chirilă, L.; Rotaru, C.; Filipov, I.; Săndulescu, M. Management of acute maxillary sinusitis after sinus bone grafting procedures with simultaneous dental implants placement–A retrospective study. BMC Infect Dis. 2016, 16, 94. [Google Scholar] [CrossRef] [PubMed]
- Kumar, H.; Jain, R. Review: The role of computational simulation in understanding the postoperative sinonasal environment. Clin. Biomech. 2019, 68, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Leite, S.H.P.; Jain, R.; Douglas, R.G. The clinical implications of computerized fluid dynamic modelling in rhinology. Rhinology 2019, 57, 2–9. [Google Scholar] [PubMed]
- Krennmair, S.; Weinländer, M.; Forstner, T.; Malek, M.; Krennmair, G.; Postl, L. The influence of different forms of sinus membrane perforation on the prevalence of postoperative complications in lateral window sinus floor elevation: A retrospective study. Clin. Implant Dent. Relat. Res. 2022, 24, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Ye, M.; Liu, W.; Cheng, S.; Yan, L. Outcomes of implants placed after osteotome sinus floor elevation without bone grafts: A systematic review and meta-analysis of single-arm studies. Int. J. Implant Dent. 2021, 7, 72. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Authors/Year/ Type of Study | Intervention | Number of Patients/SINUSES | Follow-Up | Complications | Voice Evaluation | Parameters | Type of Voice Change | Duration | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Membrane Perforation | Sinusitis | Membrane Thickening | Infection | Inflammation | Pain | Hematoma/Bleeding | Wound Dehiscence | ||||||||
| Tepper et al. [18] 2003 Cases study | Bilateral sinus lifting with lateral window. Iliac crest grafts + anorganic bovine bone + platelet rich plasma (PRP) | 4/8 | NA | - | - | - | - | - | - | - | - | Yes | Singing and speaking voice profile, periodicity, and spectral analysis | No | NA |
| Shlomi et al. [42] 2004 Comparative cases study | Unilateral and bilateral lateral window + demineralized freeze-dried human lamellar bone sheet + 50/50 mix of autogenous + anorganic bovine bone | 36/73 | 4 to 6 months | 20 | - | - | - | - | - | - | - | No | NA | NA | NA |
| Barone et al. [43] 2005 Comparative cases study | Bilateral sinus lifting with lateral window. 100% autogenous bone OR Mix of 50% autogenous + 50% porcine | 18/36 | 5 months | 3 | - | - | - | - | - | - | - | No | NA | NA | NA |
| Barone et al. [44] 2008 Comparative cases study | Bilateral sinus lifting the windows were completed either with with rotative instruments (control) piezosurgery (test) + corticocancellous porcine bone | 13/26 | 5 to 6 months | 4 (test group) 3 (control group) | - | - | - | - | - | - | - | No | NA | NA | NA |
| Ucer C. [45] 2009 Cases study | Lateral window + ipsilateral nasal suction + internal collagen membrane + anorganic bovine bone | 24/31 | NA | - | - | - | - | - | - | - | - | No | NA | NA | NA |
| Taschieri et al. [46] 2012 Cases study | Lateral window + PRFG clot + deproteinized bovine bone combined with the liquid fraction of PRFG | 8/8 | NA | 2 | 1 | - | - | - | 1 | 3 hematomas | - | No | NA | NA | NA |
| Rickert et al. [47] 2013 Randomized controlled clinical trial | Bilateral sinus lifting with rotative instruments (control) and piezosurgery (test) + Lateral window + autogenous grafts particles and blocks | 36/72 | 1,2,3 and 12 weeks | 4 (test group) 4 (control group) | - | - | - | - | - | - | - | No | NA | NA | NA |
| Stacchi et al. [48] 2013 Randomized controlled clinical trial | Unilateral sinus lifting with lateral window or lateral erosion + bone grafts (xenograft OR allograft) | 72/72 | Day 0 | 4 (lateral window) | - | - | - | - | - | - | - | No | NA | NA | NA |
| Lie et al. [49] 2015 Prospective study | Bilateral sinus lifting With lateral window + Mix of autogenous bone and xenograft OR resorbable membrane made of poly (D,L)- lactide (PDLLA) | 5/10 | Up to 6 months | - | - | - | - | - | - | - | - | No | NA | NA | NA |
| Schwarz et al. [50] 2015 Retrospective study | Sinus lifting with lateral window + mix of autologous bone and deproteinized bovine bone | 300/407 | NA | 34 | 11 | - | - | - | - | - | 5 | No | NA | NA | NA |
| Kiliç et al. [51] 2016 Randomized clinical trial | Sinus lifting with lateral window + beta-tricalcium phosphate OR beta-tricalcium phosphate + platelet rich plasma | 18/18 | 10 days to 6 months | 3 | - | - | - | - | - | - | - | No | NA | NA | NA |
| Baldini et al. [52] 2016 Randomized clinical trial | Bilateral sinus lifting with large (control) OR small (test) window + deproteinized bovine bone | 16/32 | 7, 14, 30, and 180 days | 4 (control group) 3 (test group) | - | - | - | - | - | 3 | - | No | NA | NA | NA |
| Alayan et al. [53] 2017 Prospective controlled | Unilateral or bilateral sinus lift with lateral window + mix of autogenous bone with anorganic bovine bone (control) OR anorganic bovine bone with collagen (test) | 60/60 | 1 week 2 weeks and 5 months | 8 (test group) | 1 (control) | - | - | 3 (control) 1 (test) | 4 hematoma (control) 1 hematoma (test) | 3 (control) 1 (test) | No | NA | NA | NA | |
| Stacchi et al. [54] 2017 Randomized controlled | Bilateral sinus lifting with lateral window prepared with piezosurgery (control) OR bone scrapers (test) + Hydroxyapatite particles | 25/50 | Day 0 | 3 (control group) 4 (test group) | - | - | - | - | - | 1minor hemorrhage (test) | - | No | Na | NA | NA |
| Lopez-Quiles et al. [55] 2018 Prospective non-controlled | Transcrestal + Osteotome + balloon lifting + anorganic bovine bone | 27/27 | 5–24 to months | 1 | - | - | - | - | - | - | - | No | NA | NA | NA |
| Authors/Year/Type of Study | Intervention | Number of Patients/Sinuses | Follow-Up | Complications | Voice Evaluation | Parameters | Type of Voice Change | Duration |
|---|---|---|---|---|---|---|---|---|
| Penttila et al. [56] 1995 Comparative cases study | Functional endoscopy (FESS) Versus Caldwell-Luc (CL) for treating chronic maxillary sinusitis | 143 patients in total 71 patients Caldwell-Luc unilateral 72 patients Functional endoscopy unilateral | Up to 1 year | Score of 35 in CL Score of 2 in FESS Cheek pain tenderness 54 in CL and 3 in FESS Epiphora 2 in CL and 2 in FESS Other post-nasal drip, eye symptoms, cosmetic dryness 10 in CL and 11 in FESS | No | NA | NA | NA |
| Chiapasco et al. [57] 2009 Retrospective study | Functional endoscopy sinus surgery for removal of displaced implants into the maxillary sinus (without oro-antral communication) OR Anterior-lateral window for the removal of displaced implants into the maxillary sinus (in case of oro-antral communication OR Functional endoscopy + lateral window in case or obstruction of the maxillary ostium and oro-antral communication | 6 patients/6 sinus 17 patients/17 sinus unilateral 4 patients/4 sinus unilateral | 1, 6 and 12 months | 1 nasal hemorrhage in a FESS case 1 case of relapse and infection | No | NA | NA | NA |
| Hernández-García et al. [58] 2020 Prospective study | Functional endoscopy sinus surgery ant their effects on voice and speech recognition In healthy patients, with nasal polyps and undergoing sinus surgery | 53 patients 26 FESS 27 healthy | Baseline 2 weeks and 3 months | No postsurgical complications were described | Yes | Grade, Roughness, Breathiness, Asthenia, and Strain (GRBAS assessment) | FESS produces decrease of F0 (fundamental frequency) Change in the vocal tract that increased the error of recognition in FESS patients | 3 months |
| Yadav S et al. [59] 2021 Prospective controlled study | Functional endoscopy sinus surgery patients with chronic maxillary sinusitis Comparing the standard technique uncinectomy + middle meatus antrostomy (MMA) Versus swing door technique | 60 patients 30 with the standard technique 30 with the swing door technique | 2 and 6 weeks | At 2 weeks, 8 complications were observed in patients treated with the standard technique as follows: 2 Remnants of uncinate process 3 Blocked MMA 3 Adhesions At 6 weeks only 1 minor complication was found in a patient treated with the standard technique In addition, the following symptoms were observed at 6 weeks (more symptoms in the standard method than the swing door technique: Nasal obstruction Postnasal drip Nasal discharge | No | No | No | NA |
| Yang et al. [60] 2021 Comparative cases study | Unilateral functional endoscopy sinus surgery in patients with chronic rhinosinusitis. | 42 patients 21 with limited surgery (1 sinus) 21 with wide opening surgery (more than 1 sinus ipsilateral) | Before surgery 6 months after surgery 12 months after surgery | Not reported | Yes | Objective nasality outcomes measured with a nasometer AND Subjectively nasality assessed by a Visual Analogue Scale (VAS) by the patients, and by questionnaires by their partners | Increased nasalance and nasality | Objective nasalance score increased 1 year after FESS Subjective self-reported nasality assessment improved significantly postoperatively. |
| CASE SERIES | 1. Clear Inclusion Criteria | 2. Condition Measured in a Standard, Way | 3. Valid Methods for Identification of the Condition | 4. Consecutive Inclusion of Participants? | 5. Complete Inclusion of Participants? | 6. Clear Report of Demographics | 7. Clear Report of Clinical Information | 8. Outcomes or Follow-Up Clearly Reported? | 9. Clear Reporting of Sites’/Clinics’ Demographic Information? | 10. Appropriate Statistics | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tepper et al. 2003 | Unclear | Yes | No | No | Yes | Yes | No | No | Yes | No | ||||||||||||||||||||
| Shlomi et al. 2004 | No | Yes | Yes | Unclear | Unclear | Yes | No | No | No | No | ||||||||||||||||||||
| Barone et al. 2005 | Yes | Yes | Yes | No | Yes | Yes | Yes | No | No | Yes | ||||||||||||||||||||
| Barone et al. 2008 | Yes | Yes | Yes | No | Unclear | No | Yes | No | No | No | ||||||||||||||||||||
| Ucer 2009 | No | No | Yes | Yes | No | No | No | No | Yes | No | ||||||||||||||||||||
| Taschieri et al. 2012 | Yes | Yes | Yes | No | Unclear | Yes | No | Yes | Yes | No | ||||||||||||||||||||
| RESULTS PERCENTAGES | Y | N | U | Y | N | U | Y | N | U | Y | N | U | Y | N | U | Y | N | U | Y | N | U | Y | N | U | Y | N | U | Y | N | U |
| 50 | 33.3 | 16.6 | 83.3 | 16.6 | - | 83.3 | 16.6 | - | 66.6 | 16.6 | 16.6 | 16.6 | 33.3 | 50 | 66.6 | 33.3 | - | 66.6 | 33.3 | - | 16.6 | 83.3 | - | 50 | 50 | - | 16.6 | 83.3 | - | |
| Cohort Studies | Section A: Are the Results of the Study Valid? | Section B: What Are the Results? | Section C: Will The Results Help Locally? | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. The Study Addresses a Clearly Focused Issue? | 2. Was the Cohort Recruited in an Acceptable Way? | 3. Was the Exposure Accurately Measured to Minimize Bias? | 4. Was the Outcome Accurately Measured to Minimize Bias? | 5a. Have the Authors Identified All Important Confounding Factors? | 5b. Confounding Factors in the Design and/or Analysis Were Taken into Consideration | 6a. Was the Follow-Up of the Subjects Complete Enough? | 6b. Was the Follow-Up of Subjects Long Enough? | 7. What Are the Results of the Study | 8. How Precise Are the Results? | 9. Do You Believe the Results? | 10. Can the Results Be Applied to the Local Population? | 11. Do the Results of the Study Fit with Other Available Evidence? | 12. What Are the Implications of the Study for Practice? | |
| Lie et al. 2015 Prospective study | Y | N | Y | Y | N | N | Y | CT | CT | N | CT | N | Y | CT |
| Schwarz et al. 2015 Retrospective study | Y | Y | Y | Y | CT | Y | Y | Y | Y | Y | Y | CT | Y | Y |
| Alayan et al. 2017 Prospective controlled | Y | Y | Y | Y | CT | N | Y | Y | Y | Y | Y | Y | Y | Y |
| Lopez-Quiles et al. 2018 Prospective no controlled | Y | Y | Y | Y | N | N | Y | Y | Y | Y | Y | CT | Y | Y |
| CASE SERIES | 1. Clear Inclusion Criteria | 2. Condition Measured in a Standard, Way | 3. Valid Methods for Identification of the Condition | 4. Consecutive Inclusion of Participants? | 5. Complete Inclusion of Participants? | 6. Clear Report of Demographics | 7. Clear Report of Clinical Information | 8. Outcomes or Follow-Up Clearly Reported? | 9. Clear Reporting of Sites’/Clinics’ Demographic Information? | 10. Appropriate Statistics | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Penttila et al. 1995 | No | Yes | No | No | Yes | Yes | No | Yes | Yes | Yes | ||||||||||||||||||||
| Yang et al. 2021 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | ||||||||||||||||||||
| RESULTS PERCENTAGES | Y | N | U | Y | N | U | Y | N | U | Y | N | U | Y | N | U | Y | N | U | Y | N | U | Y | N | U | Y | N | U | Y | N | U |
| 50 | 50 | - | 100 | - | - | 50 | 50 | - | 50 | 50 | - | 100 | - | - | 100 | - | - | 50 | 50 | - | 100 | - | - | 100 | - | - | 100 | - | - | |
| Cohort Studies | Section A: Are the Results of the Study Valid? | Section B: What Are the Results? | Section C: Will the Results Help Locally? | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. The Study Addresses a Clearly Focused Issue? | 2. Was the Cohort Recruited in an Acceptable way? | 3. Was the Exposure Accurately Measured to Minimize Bias? | 4. Was the Outcome Accurately Measured to Minimize Bias? | 5a. Have the Authors Identified All Important Confounding Factors? | 5b. Confounding Factors in the Design and/or Analysis Were Taken into Consideration | 6a. Was the Follow-Up of the Subjects Complete Enough? | 6b. Was the Follow-Up of Subjects Long Enough? | 7. What Are the Results of the Study | 8. How Precise Are the Results? | 9. Do You Believe the Results? | 10. Can the Results Be Applied to the Local Population? | 11. Do the Results of the Study Fit with Other Available Evidence? | 12. What Are the Implications of the Study for Practice? | |
| Chiapasco et al. 2009 | Y | CT | Y | Y | N | N | Y | Y | Y | Y | Y | Y | Y | Y |
| Hernández-García et al. 2020 | Y | Y | Y | Y | N | N | Y | CT | Y | Y | Y | Y | Y | Y |
| Yang et al. 2021 | Y | CT | Y | Y | Y | N | Y | CT | Y | Y | Y | Y | Y | Y |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delgado-Ruiz, R.; Botticelli, D.; Romanos, G. Temporal and Permanent Changes Induced by Maxillary Sinus Lifting with Bone Grafts and Maxillary Functional Endoscopic Sinus Surgery in the Voice Characteristics—Systematic Review. Dent. J. 2022, 10, 47. https://doi.org/10.3390/dj10030047
Delgado-Ruiz R, Botticelli D, Romanos G. Temporal and Permanent Changes Induced by Maxillary Sinus Lifting with Bone Grafts and Maxillary Functional Endoscopic Sinus Surgery in the Voice Characteristics—Systematic Review. Dentistry Journal. 2022; 10(3):47. https://doi.org/10.3390/dj10030047
Chicago/Turabian StyleDelgado-Ruiz, Rafael, Daniele Botticelli, and Georgios Romanos. 2022. "Temporal and Permanent Changes Induced by Maxillary Sinus Lifting with Bone Grafts and Maxillary Functional Endoscopic Sinus Surgery in the Voice Characteristics—Systematic Review" Dentistry Journal 10, no. 3: 47. https://doi.org/10.3390/dj10030047
APA StyleDelgado-Ruiz, R., Botticelli, D., & Romanos, G. (2022). Temporal and Permanent Changes Induced by Maxillary Sinus Lifting with Bone Grafts and Maxillary Functional Endoscopic Sinus Surgery in the Voice Characteristics—Systematic Review. Dentistry Journal, 10(3), 47. https://doi.org/10.3390/dj10030047