
Endoscopic Sinus Surgery Significantly Reduces Eustachian Tube Dysfunction Symptoms in Patients with Chronic Rhinosinusitis: A Systematic Review and Meta-Analysis
 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Collection
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
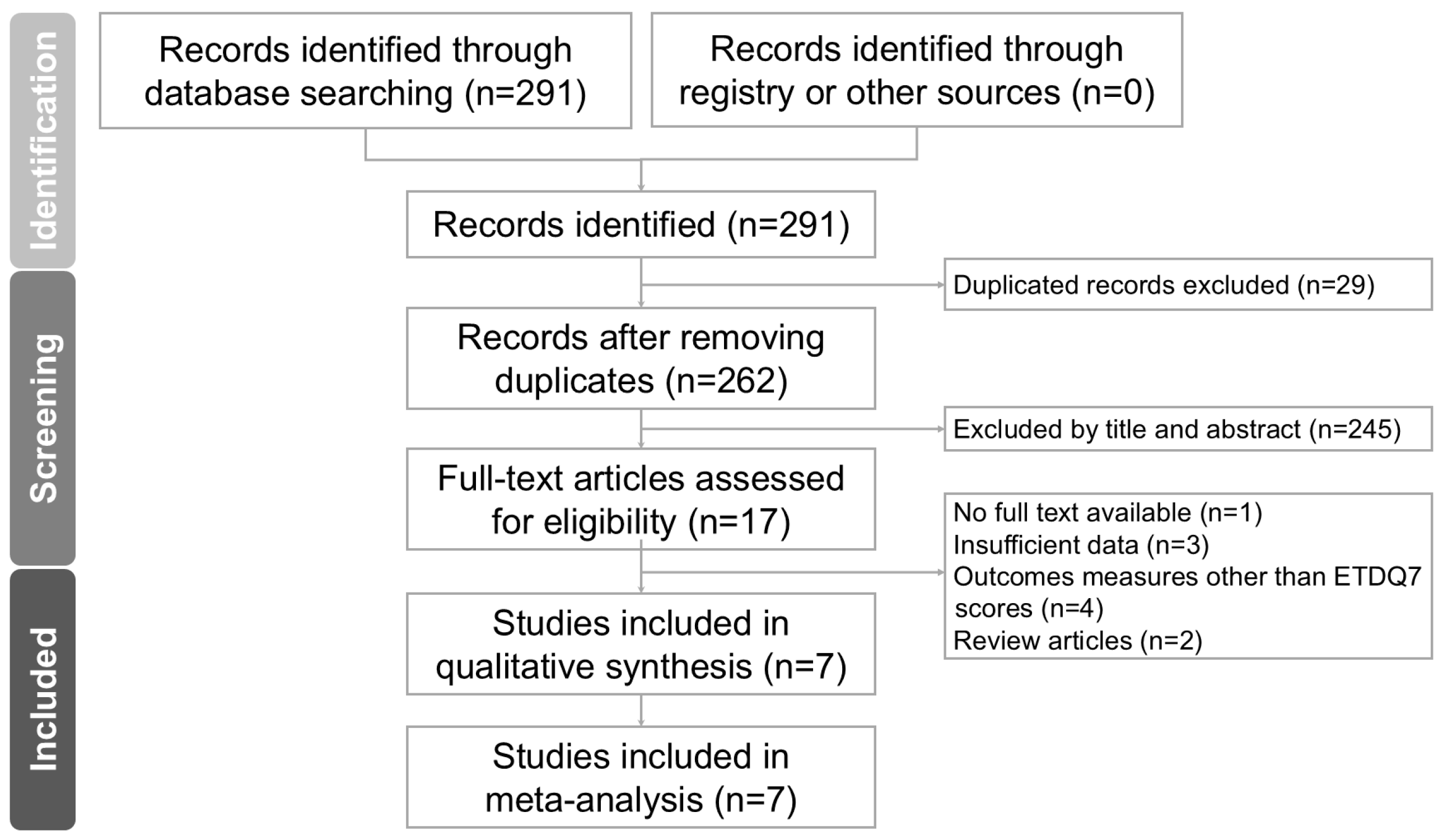
3.1. Study Selection
3.2. Baseline Characteristics
3.3. Methodological Quality Assessment of the Included Studies

{kind=link}
{kind=link}
| First Author and Year | Country | Study Period | Study Design | Inclusion Criteria | Exclusion Criteria | Total CRS Patients (n) | CRS + ETD (n) | Definition of ETD | Pre-op ETDQ-7 Score | Post-op ETDQ-7 Score |
|---|---|---|---|---|---|---|---|---|---|---|
| Bowles 2019 [17] | United Kingdom | August 2016– November 2017 | Prospective cohort study | Adult patients with refractory CRS despite a minimum of 6 months of medical therapy | Pre-existing otological disease, adequate response to medical therapy, patient preference for continuing medical therapy, contraindication to general anesthetic | 57 | 39 | ETDQ-7 ≥ 13.5 | 20.6 ± 10.34 | 11.4 ± 5.65 |
| Chang 2020 [18] | United States | December 2016–December 2018 | Retrospective cohort study | Adult patients diagnosed with CRS or RARS delineated by International Consensus Statement on Allergy and Rhinology | Known otologic comorbidities apart from ETD, prior otologic surgery, sinonasal diagnoses other than sinusitis | 302 | 180 | ETDQ-7 ≥ 14.5 | 25.5 ± 7.6 | 16.8 ± 8.5 |
| Higgins, 2020 [23] | United States | November 2016–December 2017 | Prospective case–control study | Adult CRS patients with persistent ETD without MEE despite a period of 6–8 weeks of maximum medical therapy | Ear surgery, adenoidectomy, Eustachian tube dilation, MEE, cholesteatoma, history of major ear surgery, severe atelectasis, congenital ear disorder, prior head and neck surgery | 60 | 60 | Mean ETDQ-7 ≥ 2.1 | 3.45 ± 1.061 | 2.164 ± 1.206 |
| Wu, 2020 [21] | United States | September 2018–March 2019 | Prospective cohort study | Adult patients with CRS after failed medical therapy according to International Consensus Statement on Allergy and Rhinology | Failure to complete preoperative ETDQ-7 and SNOT-22 questionnaires | 82 | 39 | ETDQ-7 ≥ 14.5 | 16.8 ± 8.2 | 12.7 ± 6.8 |
| Chen, 2021 [20] | China | December 2019–December 2020 | Prospective cohort study | Adult CRS patients with concurrent ETD and were refractory to conservative treatment for at least 12 weeks | Meniere’s disease, low-frequency sensorineural hearing loss, patulous Eustachian tube, chronic suppurative otitis media, acute upper respiratory infection and temporomandibular joint dysfunction | 70 | 70 | ETDQ-7 ≥ 14.5 + Tympanogram B/C ETDQ-7 ≥ 14.5 + ETS ≤ 5 | 20.13 ± 6.18 | 8.63 ± 3.62 |
| Chen, 2022 [19] | Taiwan | December 2016–December 2017 | Prospective cohort study | Adult CRS patients with unsatisfactory response to medical treatment for at least 2 months | History of radiotherapy of the head and neck region, ear surgery, pharyngeal surgery | 92 | 23 | ETDQ-7 ≥ 14.5 | 25.52 ± 7.7 | 10.6 ±8.31 |
| Hsieh, 2024 [22] | Taiwan | July 2018–June 2022 | Prospective cohort study 1 | Adult CRS patients with at least ethmoid and maxillary sinuses involved and diagnosis of ETD for at least 3 months | Elderly individuals, pregnant women, history of head and neck cancer, previous ear surgery, septoplasty, turbinate reduction procedures, TMJ disorder, aspirin-exacerbated respiratory disease | 25 | 25 | ETDQ-7 ≥ 14.5 + Inflation–deflation: (p) 2 Grade II-IV endoscopic inflammation score | 22.84 ± 7.39 | 16.24 ± 7.74 |
| Total (n) | - | - | - | - | - | 688 | 436 | - | - |
| First Author and Year | Total Number of CRS Patients | Nasal Polyposis | Allergic Rhinitis | Asthma | Revised ESS |
|---|---|---|---|---|---|
| Bowles 2019 [17] | 57 | 23 | - | 16 | - |
| Chang 2020 [18] | 302 | 60 | 63 | 114 | 136 |
| Higgins, 2020 [23] | 60 | 18 | - | - | 32 |
| Wu, 2020 [21] | 82 | - | - | - | - |
| Chen, 2021 [20] | 70 | 51 | 25 | 3 | 17 |
| Chen, 2022 [19] | 92 | 39 | 30 | 5 | 12 |
| Hsieh, 2024 [22] | 25 | 6 | 8 | 3 | - |
| Total, n (%) | 688 | 197 (32.5) | 126 (25.7) | 141 (25.8) | 197 (37.6) |
| A. First Author | Selection | Comparability | Outcomes | Total | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of Exposed Cohort | Selection of Nonexposed Cohort | Ascertainment of Exposure | Outcome not Present at the Start of the Study | Comparability Based on the Design or Analysis | Assessment of Outcomes | Length of Follow-Up | Adequacy of Follow-Up | ||
| Bowles 2019 [17] | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | 8 |
| Chang 2020 [18] | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | - | 7 |
| Wu 2020 [21] | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | 8 |
| Chen 2021 [20] | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | 8 |
| Chen 2022 [19] | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | 8 |
| Hsieh 2024 [22] | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | - | 7 |
| B. First Author | Selection | Comparability | Exposure | Total | |||||
| Representativeness of cases | Selection of controls | Definition of controls | Adequate cases definition | Comparability based on the design or analysis | Ascertainment of exposure | Same method of ascertainment | Non-response rate | ||
| Higgins 2020 [23] | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | ✵ | 8 |
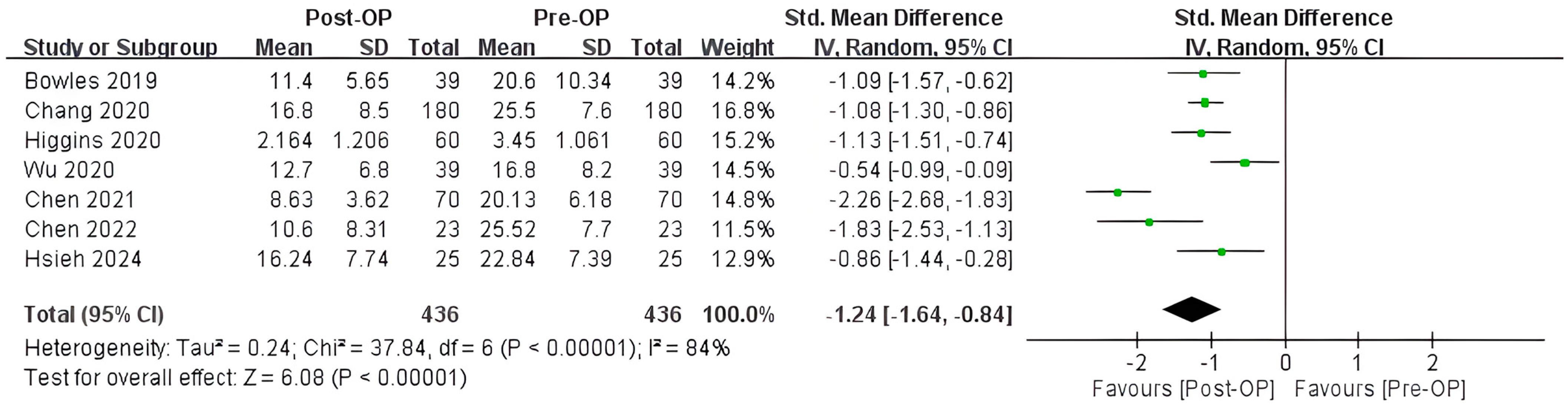
3.4. Primary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Schilder, A.G.M.; Bhutta, M.F.; Butler, C.C.; Holy, C.; Levine, L.H.; Kvaerner, K.J.; Norman, G.; Pennings, R.J.; Poe, D.; Silvola, J.T.; et al. Eustachian tube dysfunction: Consensus statement on definition, types, clinical presentation and diagnosis. Clin. Otolaryngol. 2015, 40, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Stoikes, N.F.; Dutton, J.M. The effect of endoscopic sinus surgery on symptoms of Eustachian tube dysfunction. Am. J. Rhinol. 2005, 19, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Marino, M.J.; Ling, L.C.; Yao, W.C.; Luong, A.; Citardi, M.J. Eustachian tube dysfunction symptoms in patients treated in a tertiary rhinology clinic. Int. Forum Allergy Rhinol. 2017, 7, 1135–1139. [Google Scholar] [CrossRef] [PubMed]
- Tangbumrungtham, N.; Patel, V.S.; Thamboo, A.; Patel, Z.M.; Nayak, J.V.; Ma, Y.; Choby, G.; Hwang, P.H. The prevalence of Eustachian tube dysfunction symptoms in patients with chronic rhinosinusitis. Int. Forum Allergy Rhinol. 2018, 8, 620–623. [Google Scholar] [CrossRef]
- Chen, T.; Shih, M.C.; Edwards, T.S.; Nguyen, S.A.; Meyer, T.A.; Soler, Z.M.; Schlosser, R.J. Eustachian tube dysfunction (ETD) in chronic rhinosinusitis with comparision to primary ETD: A systematic review and meta-analysis. Int. Forum Allergy Rhinol. 2022, 12, 942–951. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J. Executive summary of EPOS 2020 including integrated care pathways. Rhinology 2020, 58, 82–111. [Google Scholar] [CrossRef]
- Rotimi, O.; Mohamed, N.; Steele, K.B.P.; Bowles, P. Impact of endoscopic sinus surgery on Eustachian tube dysfunction in patients with chronic rhinosinusitis: Systematic review and meta-analysis. Rhinol. Online 2022, 5, 87–95. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- McCoul, E.D.; Anand, V.K.; Christos, P.J. Validating the clinical assessment of eustachian tube dysfunction: The Eustachian Tube Dysfunction Questionnaire (ETDQ-7). Laryngoscope 2012, 122, 1137–1141. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Higgins, J. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.; Higgins, J.P.T.; Altman, D.G. Chapter 10: Analysing Data and Undertaking Meta-Analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Version 6.4; Cochrane: London, UK, 2023. [Google Scholar]
- Lee, I.H.; Kim, D.H.; Kim, S.W.; Kim, S.W. Changes in symptoms of Eustachian tube dysfunction after nasal surgery. Eur. Arch. Otorhinolaryngol. 2022, 279, 5017–5023. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.Y.; Jang, S.; Seo, G.; Park, S.K. Effect of endoscopic sinus surgery on Eustachian tube function in adult sinusitis patients: A prospective case-control study. J. Clin. Med. 2021, 10, 4689. [Google Scholar] [CrossRef] [PubMed]
- Teo, N.W.; Mace, J.C.; Smith, T.L.; Hwang, P.H. Impact of endoscopic sinus surgery on otologic symptoms associated with chronic rhinosinusitis. World J. Otorhinolaryngol. Head Neck Surg. 2017, 3, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Maniakas, A.; Desrosiers, M.; Asmar, M.H.; Al Falasi, M.; Mfuna Endam, L.; Hopkins, C.; Philpott, C.; Erskine, S.; Smith, R.; Kilty, S. Eustachian tube symptoms are frequent in chronic rhinosinusitis and respond well to endoscopic sinus surgery. Rhinology 2018, 56, 118–121. [Google Scholar] [CrossRef]
- Bowles, P.F.; Agrawal, S.; Salam, M.A. Eustachian Tube dysfunction in chronic rhinosinusitis: Pre and post-operative results following endoscopic sinus surgery, a prospective study. Rhinology 2019, 57, 73–77. [Google Scholar] [CrossRef]
- Chang, M.T.; Hosseini, D.K.; Song, S.H.; Nayak, J.V.; Patel, Z.M.; Lee, J.Y.; Hwang, P.H. The Effect of Endoscopic Sinus Surgery on Eustachian Tube Dysfunction Symptoms. Otolaryngol. Head Neck Surg. 2020, 163, 603–610. [Google Scholar] [CrossRef]
- Chen, W.C.; Yang, K.L.; Lin, W.C.; Fang, K.C.; Wu, C.N.; Luo, S.D. Clinical outcomes of Eustachian tube dysfunction in chronic rhinosinusitis following endoscopic sinus surgery. J. Chin. Med. Assoc. 2022, 85, 782–787. [Google Scholar] [CrossRef]
- Chen, X.; Dang, H.; Chen, Q.; Chen, Z.; Ma, Y.; Liu, X.; Lin, P.; Zou, H.; Xiong, H. Endoscopic sinus surgery improves Eustachian tube function in patients with chronic rhinosinusitis: A multicenter prospective study. Rhinology 2021, 59, 560–566. [Google Scholar] [CrossRef]
- Wu, A.W.; Walgama, E.S.; Higgins, T.S.; Borrelli, M.; Vardanyan, N.; Hopp, S.; Shamsian, A.; Hopp, M.L. Eustachian Tube Quality of Life and Severity of Disease in Patients with Chronic Rhinosinusitis. Am. J. Rhinol. Allergy 2020, 34, 532–536. [Google Scholar] [CrossRef]
- Hsieh, C.Y.; Lin, W.C.; Lin, C.C.; Chou, Y.F. Combined balloon Eustachian tuboplasty endoscopic sinus surgery for patients with chronic rhinosinusitis and Eustachian tube dysfunction. Int. Forum Allergy Rhinol. 2024, 14, 1327–1336. [Google Scholar] [CrossRef] [PubMed]
- Higgins, T.S.; Cappello, Z.J.; Wu, A.W.; Ting, J.Y.; Sindwani, R. Predictors of eustachian tube dysfunction improvement and normalization after endoscopic sinus surgery. Laryngoscope 2020, 130, E721–E726. [Google Scholar] [CrossRef] [PubMed]
- Wuraola, O.A.; Afolabi, A.O.; Ologe, F.E. Tympanometry and endoscopic diagnosis of eustachian tube dysfunction in patients with chronic rhinosinusitis. Niger. Postgrad. Med. J. 2023, 30, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Finkelstein, Y.; Talmi, Y.P.; Rubel, Y.; Bar-Ziv, J.; Zohar, Y. Otitis media with effusion as a presenting symptom of chronic sinusitis. J. Laryngol. Otol. 1989, 103, 827–832. [Google Scholar] [CrossRef]
- O’Connor, R.D.; Ort, H.; Leong, A.B.; Cook, D.A.; Street, D.; Hamburger, R.N. Tympanometric changes following nasal antigen challenge in children with allergic rhinitis. Ann. Allergy 1984, 53, 468–471. [Google Scholar]
- Adams, S.M.; Derbarsegian, A.; Sedaghat, A.R.; Phillips, K.M. Impact of medical treatment for chronic rhinosinusitis on eustachian tube dysfunction. Int. Forum Allergy Rhinol. 2023, 14, 850–852. [Google Scholar] [CrossRef]
- OuYang, Z.; Lou, Z.; Lou, Z.; Jin, K.; Sun, J.; Chen, Z. The effect of concurrent nasal surgery on the eustachian tube function and myringoplasty outcomes. Am. J. Otolaryngol. 2021, 42, 102926. [Google Scholar] [CrossRef]
- Ryu, G.; Kim, H.Y.; Jung, Y.G.; Hong, S.D. Endotypes of Asian chronic rhinosinusitis with nasal polyps: A narrative review. Precis. Future Med. 2022, 6, 170–176. [Google Scholar] [CrossRef]
- Juszczak, H.M.; Loftus, P.A. Role of Allergy in Eustachian Tube Dysfunction. Curr. Allergy Asthma Rep. 2020, 20, 54. [Google Scholar] [CrossRef]
- Bernkopf, E.; Cristalli, G.; de Vincentiis, G.C.; Bernkopf, G.; Capriotti, V. Temporomandibular Joint and Otitis Media: A Narrative Review of Implications in Etiopathogenesis and Treatment. Medicina 2022, 58, 1806. [Google Scholar] [CrossRef]
- Chang, M.T.; Roozdar, P.; Lin, Y.T.; Lee, J.Y.; Nayak, J.V.; Patel, Z.M.; Hwang, P.H. Effect of dupilumab on Eustachian tube dysfunction in patients with chronic rhinosinusitis with nasal polyposis. Int. Forum Allergy Rhinol. 2023, 13, 1561–1563. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, D.; Nakayama, T.; Minagawa, S.; Adachi, T.; Mitsuyama, C.; Shida, Y.; Nakajima, T.; Haruna, S.I.; Matsuwaki, Y. Dupilumab improves eosinophilic otitis media associated with eosinophilic chronic rhinosinusitis. Allergol. Int. 2023, 72, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, H.; Matsubara, A.; Nakagawa, T.; Ohta, N.; Izuhara, K.; Shirasaki, T.; Abe, T.; Takeda, I.; Shinkawa, H. The role of periostin in eosinophilic otitis media. Acta Otolaryngol. 2012, 132, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Ishida, A.; Ohta, N.; Suzuki, Y.; Kakehata, S.; Okubo, K.; Ikeda, H.; Shiraishi, H.; Izuhara, K. Expression of pendrin and periostin in allergic rhinitis and chronic rhinosinusitis. Allergol. Int. 2012, 61, 589–595. [Google Scholar] [CrossRef]
- El-Anwar, M.W.; Elnabtity, N.M.; Nada, E.; Abdelmonem, S. Relationship between nasal polyposis and Eustachian tube function. Egypt. J. Otolaryngol. 2022, 38, 45. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, K.-S.; Chen, W.-C.; Wu, C.-N.; Wee, Y.-S.; Wang, C.-S.; Wu, C.-C.; Luo, S.-D. Endoscopic Sinus Surgery Significantly Reduces Eustachian Tube Dysfunction Symptoms in Patients with Chronic Rhinosinusitis: A Systematic Review and Meta-Analysis. Biomedicines 2024, 12, 2484. https://doi.org/10.3390/biomedicines12112484
Yang K-S, Chen W-C, Wu C-N, Wee Y-S, Wang C-S, Wu C-C, Luo S-D. Endoscopic Sinus Surgery Significantly Reduces Eustachian Tube Dysfunction Symptoms in Patients with Chronic Rhinosinusitis: A Systematic Review and Meta-Analysis. Biomedicines. 2024; 12(11):2484. https://doi.org/10.3390/biomedicines12112484
Chicago/Turabian StyleYang, Kai-Shan, Wei-Chih Chen, Ching-Nung Wu, Yin-Shen Wee, Ching-Shuen Wang, Cheng-Chih Wu, and Sheng-Dean Luo. 2024. "Endoscopic Sinus Surgery Significantly Reduces Eustachian Tube Dysfunction Symptoms in Patients with Chronic Rhinosinusitis: A Systematic Review and Meta-Analysis" Biomedicines 12, no. 11: 2484. https://doi.org/10.3390/biomedicines12112484
APA StyleYang, K.-S., Chen, W.-C., Wu, C.-N., Wee, Y.-S., Wang, C.-S., Wu, C.-C., & Luo, S.-D. (2024). Endoscopic Sinus Surgery Significantly Reduces Eustachian Tube Dysfunction Symptoms in Patients with Chronic Rhinosinusitis: A Systematic Review and Meta-Analysis. Biomedicines, 12(11), 2484. https://doi.org/10.3390/biomedicines12112484