
Prognostic Significance of Initial Absolute Lymphocyte Count in Adjuvant Radiotherapy for Pancreatic Adenocarcinoma


Abstract
:1. Introduction
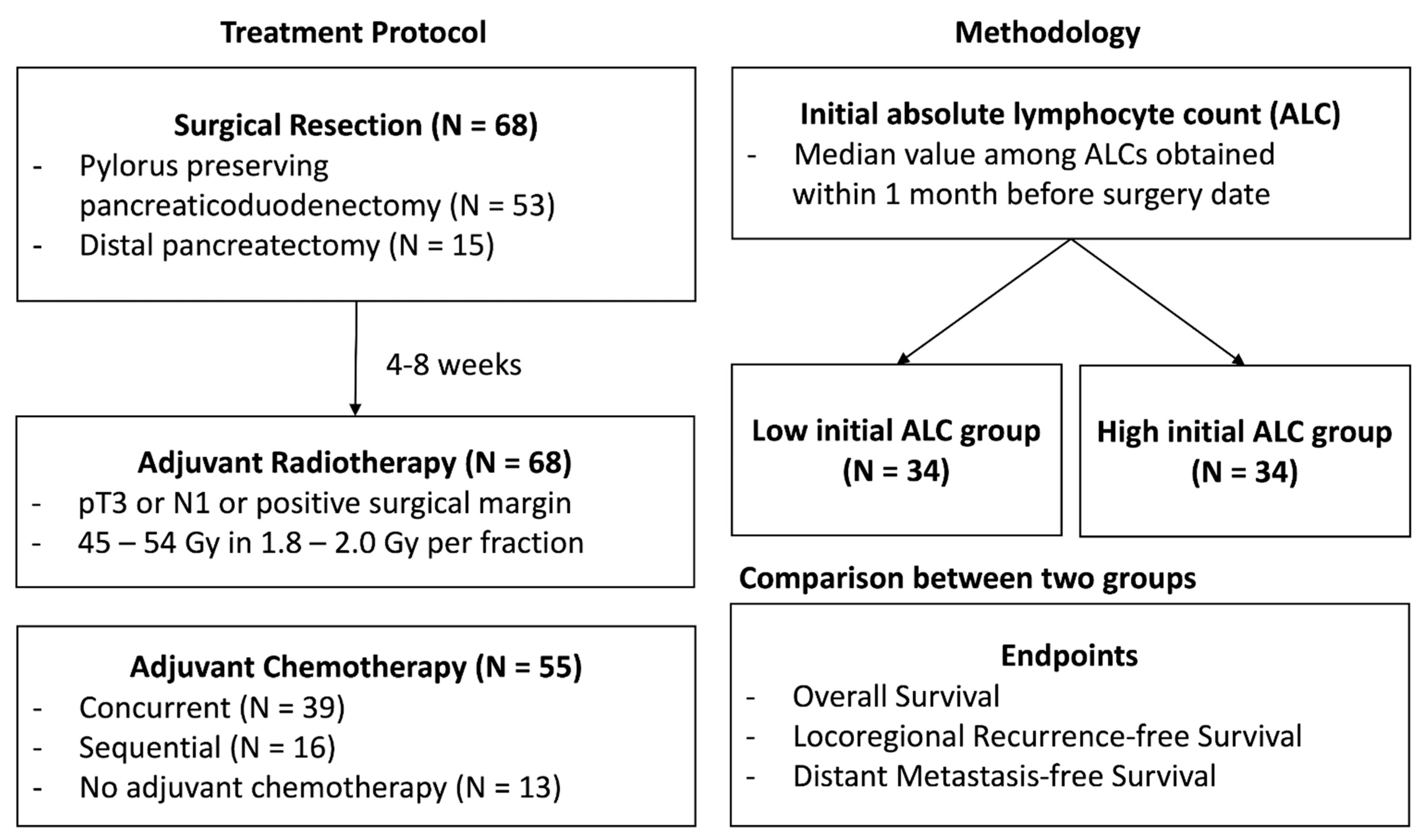
2. Materials and Methods
3. Results
3.1. Patient Characteristics between the High and Low Initial ALC Groups
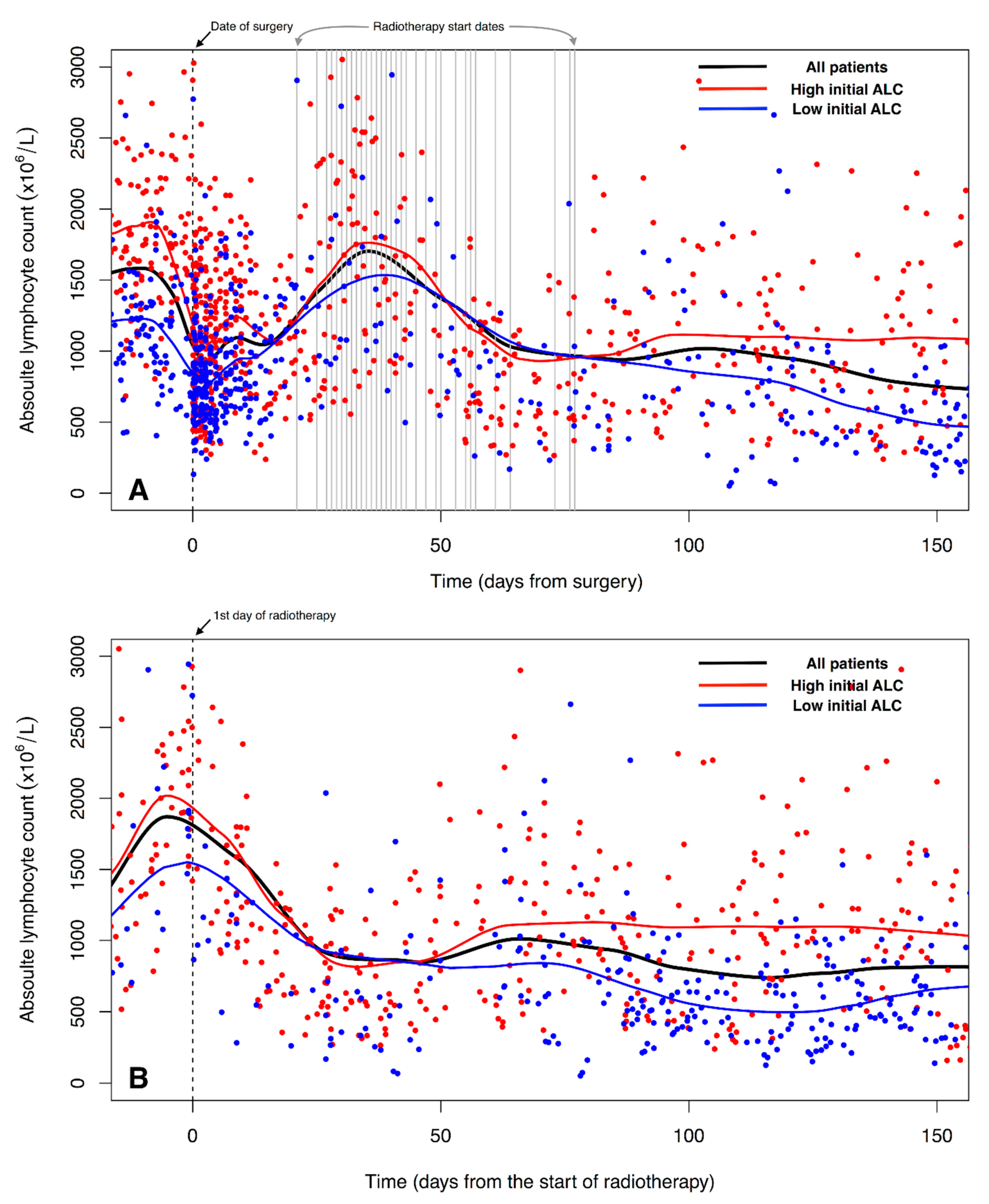
3.2. Changes of ALC over Time
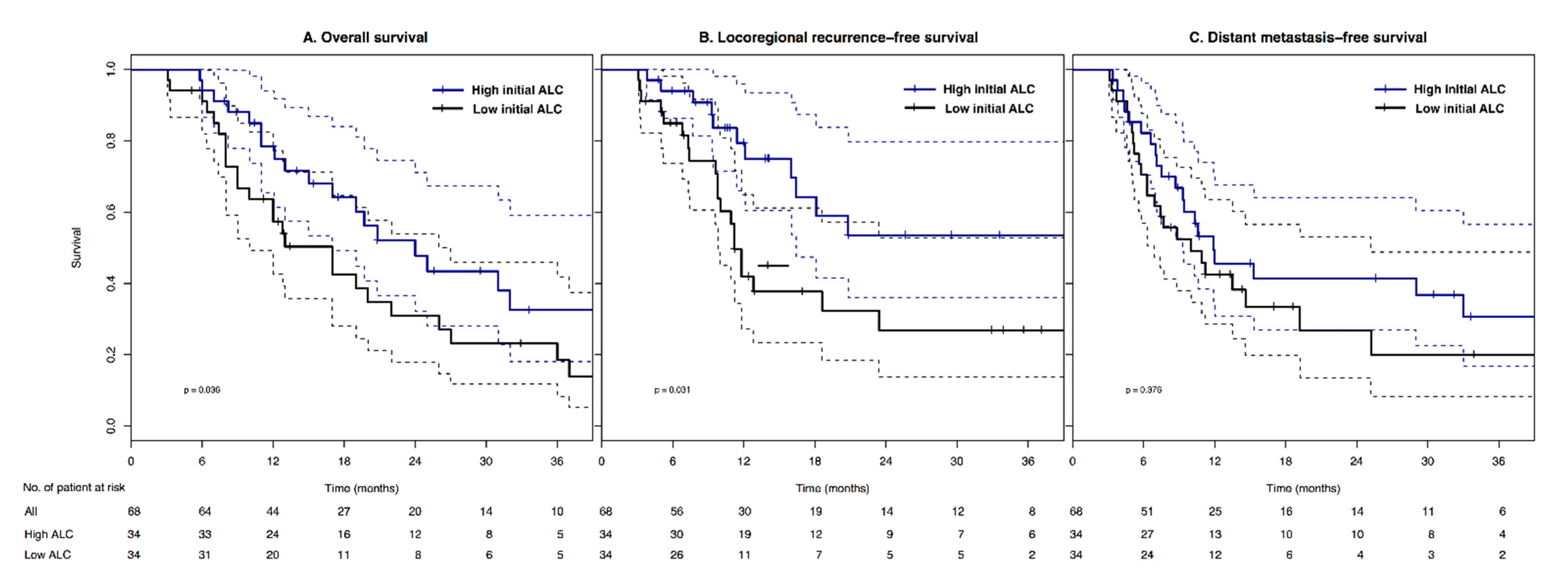
3.3. Comparison of Survivals between the High and Low Initial ALC Groups
3.4. Univariable and Multivariable Analyses Affecting Survivals
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ryan, D.P.; Hong, T.S.; Bardeesy, N. Pancreatic adenocarcinoma. N. Engl. J. Med. 2014, 371, 2140–2141. [Google Scholar] [CrossRef]
- Tempero, M.A.; Malafa, M.P.; Al-Hawary, M.; Behrman, S.W.; Benson, A.B.; Cardin, D.B.; Chiorean, E.G.; Chung, V.; Czito, B.; Del Chiaro, M.; et al. Pancreatic Adenocarcinoma, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 439–457. [Google Scholar] [CrossRef] [PubMed]
- Mizrahi, J.D.; Surana, R.; Valle, J.W.; Shroff, R.T. Pancreatic cancer. Lancet 2020, 395, 2008–2020. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Neoptolemos, J.P.; Palmer, D.H.; Ghaneh, P.; Psarelli, E.E.; Valle, J.W.; Halloran, C.M.; Faluyi, O.; O’Reilly, D.A.; Cunningham, D.; Wadsley, J.; et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): A multicentre, open-label, randomised, phase 3 trial. Lancet 2017, 389, 1011–1024. [Google Scholar] [CrossRef]
- Neoptolemos, J.P.; Dunn, J.A.; Stocken, D.D.; Almond, J.; Link, K.; Beger, H.; Bassi, C.; Falconi, M.; Pederzoli, P.; Dervenis, C.; et al. Adjuvant chemoradiotherapy and chemotherapy in resectable pancreatic cancer: A randomised controlled trial. Lancet 2001, 358, 1576–1585. [Google Scholar] [CrossRef]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.L.; Chone, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef] [PubMed]
- Kalser, M.H.; Ellenberg, S.S. Pancreatic cancer. Adjuvant combined radiation and chemotherapy following curative resection. Arch. Surg. 1985, 120, 899–903. [Google Scholar] [CrossRef]
- Corsini, M.M.; Miller, R.C.; Haddock, M.G.; Donohue, J.H.; Farnell, M.B.; Nagorney, D.M.; Jatoi, A.; McWilliams, R.R.; Kim, G.P.; Bhatia, S.; et al. Adjuvant radiotherapy and chemotherapy for pancreatic carcinoma: The Mayo Clinic experience (1975–2005). J. Clin. Oncol. 2008, 26, 3511–3516. [Google Scholar] [CrossRef]
- Herman, J.M.; Swartz, M.J.; Hsu, C.C.; Winter, J.; Pawlik, T.M.; Sugar, E.; Robinson, R.; Laheru, D.A.; Jaffee, E.; Hruban, R.H.; et al. Analysis of fluorouracil-based adjuvant chemotherapy and radiation after pancreaticoduodenectomy for ductal adenocarcinoma of the pancreas: Results of a large, prospectively collected database at the Johns Hopkins Hospital. J. Clin. Oncol. 2008, 26, 3503–3510. [Google Scholar] [CrossRef]
- Smeenk, H.G.; van Eijck, C.H.; Hop, W.C.; Erdmann, J.; Tran, K.C.; Debois, M.; van Cutsem, E.; van Dekken, H.; Klinkenbijl, J.H.; Jeekel, J. Long-term survival and metastatic pattern of pancreatic and periampullary cancer after adjuvant chemoradiation or observation: Long-term results of EORTC trial 40891. Ann. Surg. 2007, 246, 734–740. [Google Scholar] [CrossRef] [PubMed]
- Neoptolemos, J.P.; Stocken, D.D.; Friess, H.; Bassi, C.; Dunn, J.A.; Hickey, H.; Beger, H.; Fernandez-Cruz, L.; Dervenis, C.; Lacaine, F.; et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N. Engl. J. Med. 2004, 350, 1200–1210. [Google Scholar] [CrossRef] [PubMed]
- Liao, W.C.; Chien, K.L.; Lin, Y.L.; Wu, M.S.; Lin, J.T.; Wang, H.P.; Tu, Y.K. Adjuvant treatments for resected pancreatic adenocarcinoma: A systematic review and network meta-analysis. Lancet Oncol. 2013, 14, 1095–1103. [Google Scholar] [CrossRef]
- Balmanoukian, A.; Ye, X.; Herman, J.; Laheru, D.; Grossman, S.A. The association between treatment-related lymphopenia and survival in newly diagnosed patients with resected adenocarcinoma of the pancreas. Cancer Investig. 2012, 30, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Wild, A.T.; Ye, X.; Ellsworth, S.G.; Smith, J.A.; Narang, A.K.; Garg, T.; Campian, J.; Laheru, D.A.; Zheng, L.; Wolfgang, C.L.; et al. The Association Between Chemoradiation-related Lymphopenia and Clinical Outcomes in Patients With Locally Advanced Pancreatic Adenocarcinoma. Am. J. Clin. Oncol. 2015, 38, 259–265. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Clark, E.J.; Connor, S.; Taylor, M.A.; Madhavan, K.K.; Garden, O.J.; Parks, R.W. Preoperative lymphocyte count as a prognostic factor in resected pancreatic ductal adenocarcinoma. HPB 2007, 9, 456–460. [Google Scholar] [CrossRef]
- Carstens, J.L.; Correa de Sampaio, P.; Yang, D.; Barua, S.; Wang, H.; Rao, A.; Allison, J.P.; LeBleu, V.S.; Kalluri, R. Spatial computation of intratumoral T cells correlates with survival of patients with pancreatic cancer. Nat. Commun. 2017, 8, 15095. [Google Scholar] [CrossRef]
- Menetrier-Caux, C.; Ray-Coquard, I.; Blay, J.Y.; Caux, C. Lymphopenia in Cancer Patients and its Effects on Response to Immunotherapy: An opportunity for combination with Cytokines? J. Immunother. Cancer 2019, 7, 85. [Google Scholar] [CrossRef]
- Diehl, A.; Yarchoan, M.; Hopkins, A.; Jaffee, E.; Grossman, S.A. Relationships between lymphocyte counts and treatment-related toxicities and clinical responses in patients with solid tumors treated with PD-1 checkpoint inhibitors. Oncotarget 2017, 8, 114268–114280. [Google Scholar] [CrossRef]
- Lee, B.M.; Byun, H.K.; Seong, J. Significance of lymphocyte recovery from treatment-related lymphopenia in locally advanced pancreatic cancer. Radiother. Oncol. 2020, 151, 82–87. [Google Scholar] [CrossRef]
- Yalamanchali, A.; Zhang, H.; Huang, K.C.; Mohan, R.; Lin, S.H.; Zhu, C.; Grossman, S.A.; Jin, J.Y.; Ellsworth, S.G. Patient-Specific Lymphocyte Loss Kinetics as Biomarker of Spleen Dose in Patients Undergoing Radiation Therapy for Upper Abdominal Malignancies. Adv. Radiat. Oncol. 2021, 6, 100545. [Google Scholar] [CrossRef] [PubMed]
- Ellsworth, S.G. Field size effects on the risk and severity of treatment-induced lymphopenia in patients undergoing radiation therapy for solid tumors. Adv. Radiat Oncol 2018, 3, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Wild, A.T.; Herman, J.M.; Dholakia, A.S.; Moningi, S.; Lu, Y.; Rosati, L.M.; Hacker-Prietz, A.; Assadi, R.K.; Saeed, A.M.; Pawlik, T.M.; et al. Lymphocyte-Sparing Effect of Stereotactic Body Radiation Therapy in Patients With Unresectable Pancreatic Cancer. Int. J. Radiat Oncol. Biol. Phys. 2016, 94, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Yovino, S.; Kleinberg, L.; Grossman, S.A.; Narayanan, M.; Ford, E. The etiology of treatment-related lymphopenia in patients with malignant gliomas: Modeling radiation dose to circulating lymphocytes explains clinical observations and suggests methods of modifying the impact of radiation on immune cells. Cancer Investig. 2013, 31, 140–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Low Initial ALC (N = 34) | High Initial ALC (N = 34) | p-Value | |
|---|---|---|---|
| Age (year) | 0.556 | ||
| Mean ± SD | 59.8 ± 9.9 | 58.4 ± 10.6 | |
| Gender | 0.615 | ||
| Male | 20 | 23 | |
| Female | 14 | 11 | |
| ECOG PS | 0.575 | ||
| 0–1 | 27 | 24 | |
| 2 | 7 | 10 | |
| Preoperative CA 19-9 (U/mL) | 0.980 | ||
| Mean ± SD | 281.1 ± 583.9 | 277.5 ± 562.1 | |
| Initial ALC (×106/L) | |||
| Mean ± SD | 1217.8 ± 245.3 | 2049.3 ± 433.2 | <0.001 |
| Type of surgery | 0.079 | ||
| DP | 4 | 11 | |
| PPPD | 30 | 23 | |
| T stage | 0.261 | ||
| T1 | 0 | 1 | |
| T2 | 0 | 1 | |
| T3 | 32 | 32 | |
| T4 | 2 | 0 | |
| N stage | 1.000 | ||
| N0 | 11 | 12 | |
| N1 | 23 | 22 | |
| Resection margin | 1.000 | ||
| Positive | 9 | 9 | |
| Negative | 25 | 25 | |
| Chemotherapy | 0.026 | ||
| No chemotherapy | 9 | 4 | |
| Sequential | 11 | 5 | |
| Concurrent | 14 | 25 | |
| Radiotherapy dose (Gy) | 0.245 | ||
| Mean ± SD | 49.9 ± 2.8 | 50.8 ± 3.6 |
| Variable | 3 Year LRRFS (%) | p-Value (log-Rank) | 3 Year DMFS (%) | p-Value (log-Rank) | 3 Year OS (%) | p-Value (log-Rank) |
|---|---|---|---|---|---|---|
| Age (<61 vs. ≥61) | 41.2 vs. 37.9 | 0.932 | 32.0 vs. 21.0 | 0.378 | 33.3 vs. 15.2 | 0.138 |
| Gender (male vs. female) | 42.3 vs. 38.1 | 0.604 | 32.3 vs. 17.0 | 0.548 | 23.9 vs. 27.0 | 0.773 |
| ECOG PS (0–1 vs. 2) | 45.3 vs. 30.9 | 0.319 | 22.8 vs. 30.2 | 0.134 | 27.6 vs. 19.3 | 0.667 |
| Preoperative CA 19-9 (low vs. high) | 39.3 vs. 35.8 | 0.638 | 28.8 vs. 30.1 | 0.815 | 27.6 vs. 21.2 | 0.503 |
| Initial ALC (low vs. high) | 27.0 vs. 53.6 | 0.031 | 20.1 vs. 30.8 | 0.376 | 18.6 vs. 32.6 | 0.036 |
| Surgery (DP vs. PPPD) | 66.9 vs. 33.1 | 0.020 | 9.4 vs. 34.4 | 0.472 | 35.3 vs. 23.2 | 0.395 |
| N stage (N0 vs. N1) | 41.9 vs. 37.6 | 0.931 | 44.0 vs. 13.6 | 0.062 | 46.3 vs. 14.9 | 0.007 |
| Resection margin (− vs. +) | 48.3 vs. 12.9 | 0.090 | 28.3 vs. 27.2 | 0.352 | 32.3 vs. 0.0 | 0.076 |
| Chemotherapy (no vs. sequential vs. concurrent) | 34.4 vs. 33.7 vs. 46.0 | 0.733 | 20.5 vs. 35.2 vs. 25.5 | 0.752 | 17.6 vs. 23.0 vs. 30.4 | 0.860 |
| Radiotherapy dose (<50.4 Gy vs. ≥50.4 Gy) | 34.4 vs. 44.9 | 0.414 | 26.0 vs. 27.3 | 0.379 | 15.9 vs. 33.8 | 0.243 |
| Variable | LRRFS | DMFS | OS | ||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age (<61 vs. ≥61) | 0.928 | 0.471–1.828 | 0.829 | ||||||
| ECOG PS (0–1 vs. 2) | 0.475 | 0.206–1.094 | 0.080 | ||||||
| Initial ALC (low vs. high) | 0.457 | 0.214–0.978 | 0.044 | 0.473 | 0.244–0.916 | 0.026 | |||
| Surgery (DP vs. PPPD) | 3.765 | 1.100–12.884 | 0.035 | ||||||
| N stage (N0 vs. N1) | 2.134 | 1.045–4.360 | 0.038 | 2.403 | 1.104–5.228 | 0.027 | |||
| Resection margin (− vs. +) | 2.682 | 1.110–6.483 | 0.028 | 1.909 | 0.898–4.058 | 0.093 | |||
| Chemotherapy (no vs. sequential) | 0.596 | 0.185–1.913 | 0.384 | 0.871 | 0.340–2.230 | 0.773 | 0.795 | 0.315–2.010 | 0.628 |
| Chemotherapy (no vs. concurrent) | 1.131 | 0.447–2.862 | 0.795 | 0.781 | 0.361–1.692 | 0.531 | 0.972 | 0.433–2.181 | 0.945 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heo, J.; Noh, O.K. Prognostic Significance of Initial Absolute Lymphocyte Count in Adjuvant Radiotherapy for Pancreatic Adenocarcinoma. Biomedicines 2022, 10, 2190. https://doi.org/10.3390/biomedicines10092190
Heo J, Noh OK. Prognostic Significance of Initial Absolute Lymphocyte Count in Adjuvant Radiotherapy for Pancreatic Adenocarcinoma. Biomedicines. 2022; 10(9):2190. https://doi.org/10.3390/biomedicines10092190
Chicago/Turabian StyleHeo, Jaesung, and O Kyu Noh. 2022. "Prognostic Significance of Initial Absolute Lymphocyte Count in Adjuvant Radiotherapy for Pancreatic Adenocarcinoma" Biomedicines 10, no. 9: 2190. https://doi.org/10.3390/biomedicines10092190
APA StyleHeo, J., & Noh, O. K. (2022). Prognostic Significance of Initial Absolute Lymphocyte Count in Adjuvant Radiotherapy for Pancreatic Adenocarcinoma. Biomedicines, 10(9), 2190. https://doi.org/10.3390/biomedicines10092190