
Assisted Reproductive Technique and Abnormal Cord Insertion: A Systematic Review and Meta-Analysis

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Approach to the Systematic Literature Review
2.2. Eligibility Criteria, Information Sources, and Search Strategy
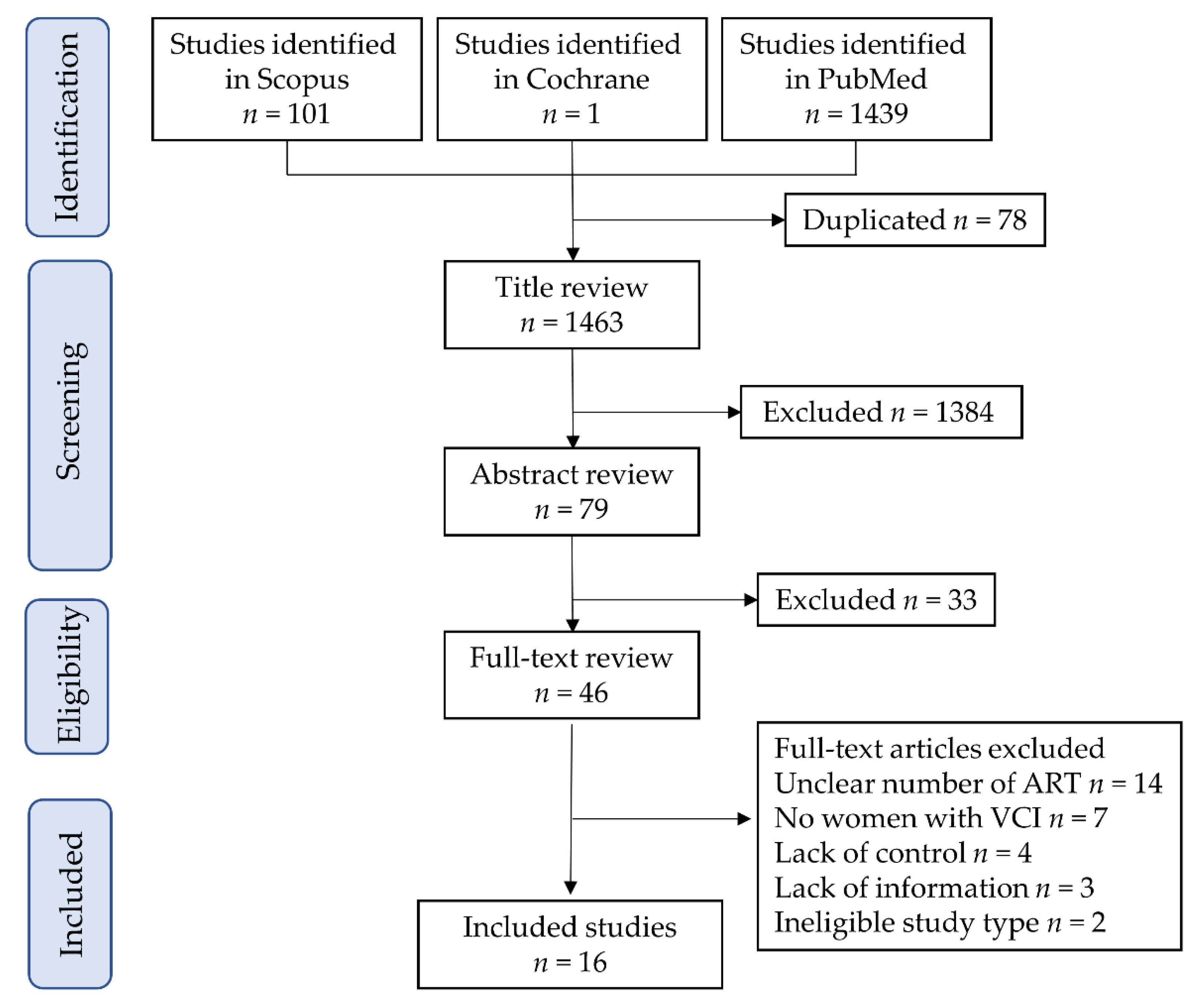
2.3. Study Selection
2.4. Data Extraction
2.5. Analysis of Outcome Measures and Assessment of Bias Risk
2.6. Meta-Analysis Plan
2.7. Statistical Analysis
3. Results
3.1. Study Selection
Risk of Bias of Eligible Studies
3.2. Study Characteristics
3.2.1. Number of Studies: Primary Outcome
3.2.2. Number of Studies: Secondary Outcomes
3.2.3. Number of Studies: A Sensitivity Analysis
3.3. Primary Outcome: Relationship between ART and ACI
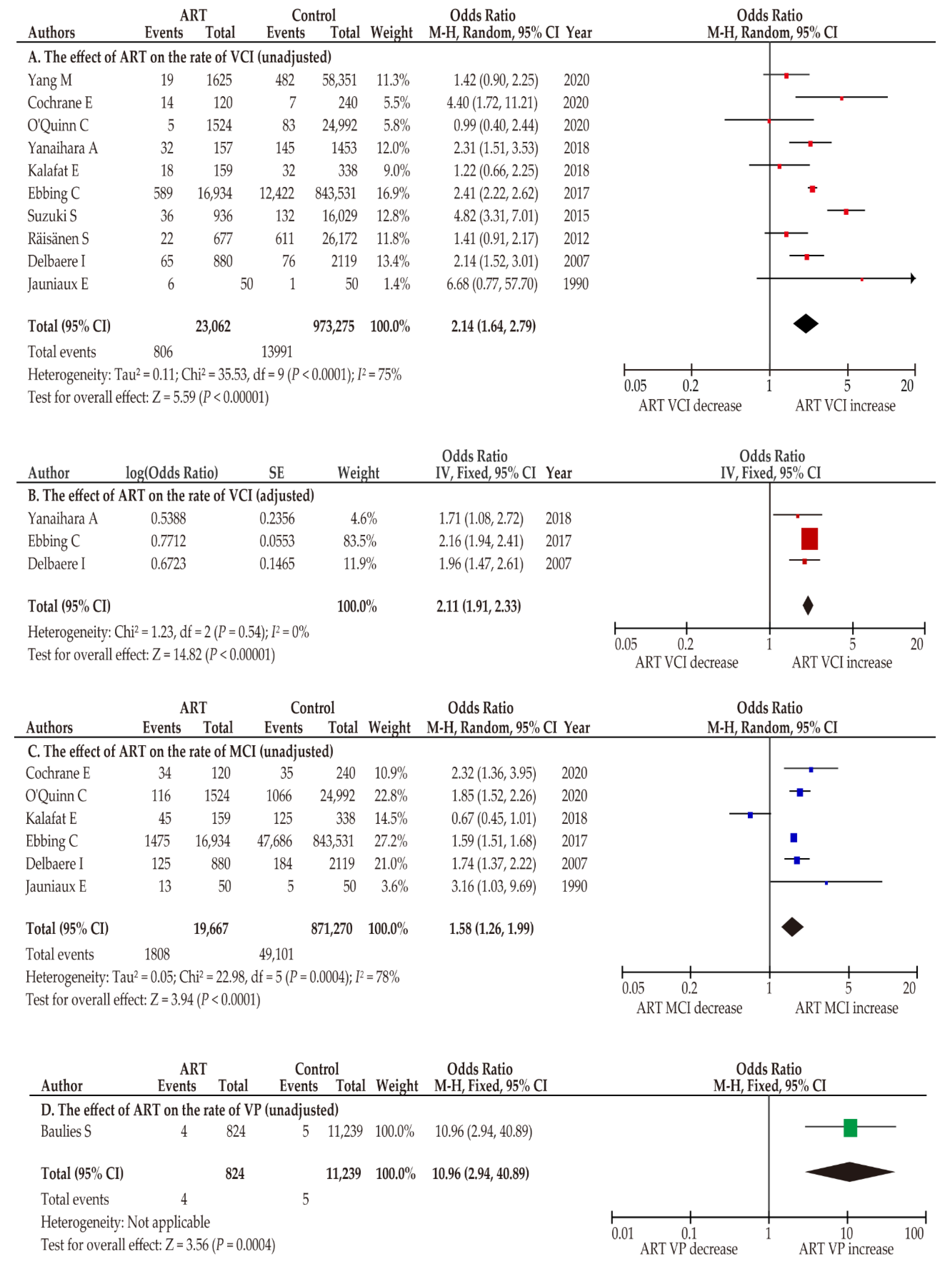
3.3.1. Effect of ART on VCI Incidence
3.3.2. Effect of ART on MCI Incidence
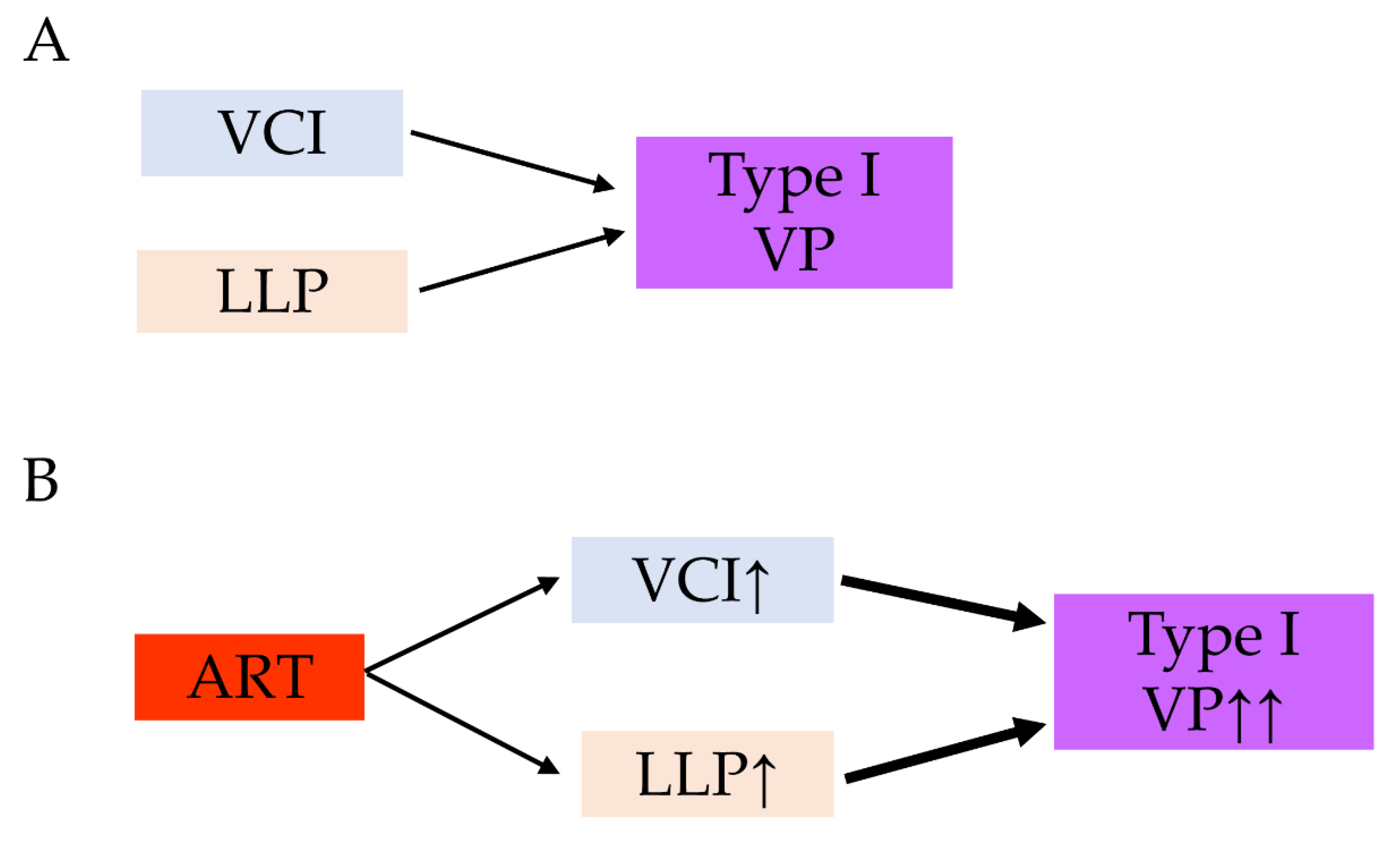
3.3.3. Influence of ART on the Incidence of Vasa Previa
3.4. Primary Outcome: Effect of Different Types of ART on the Rate of ACI
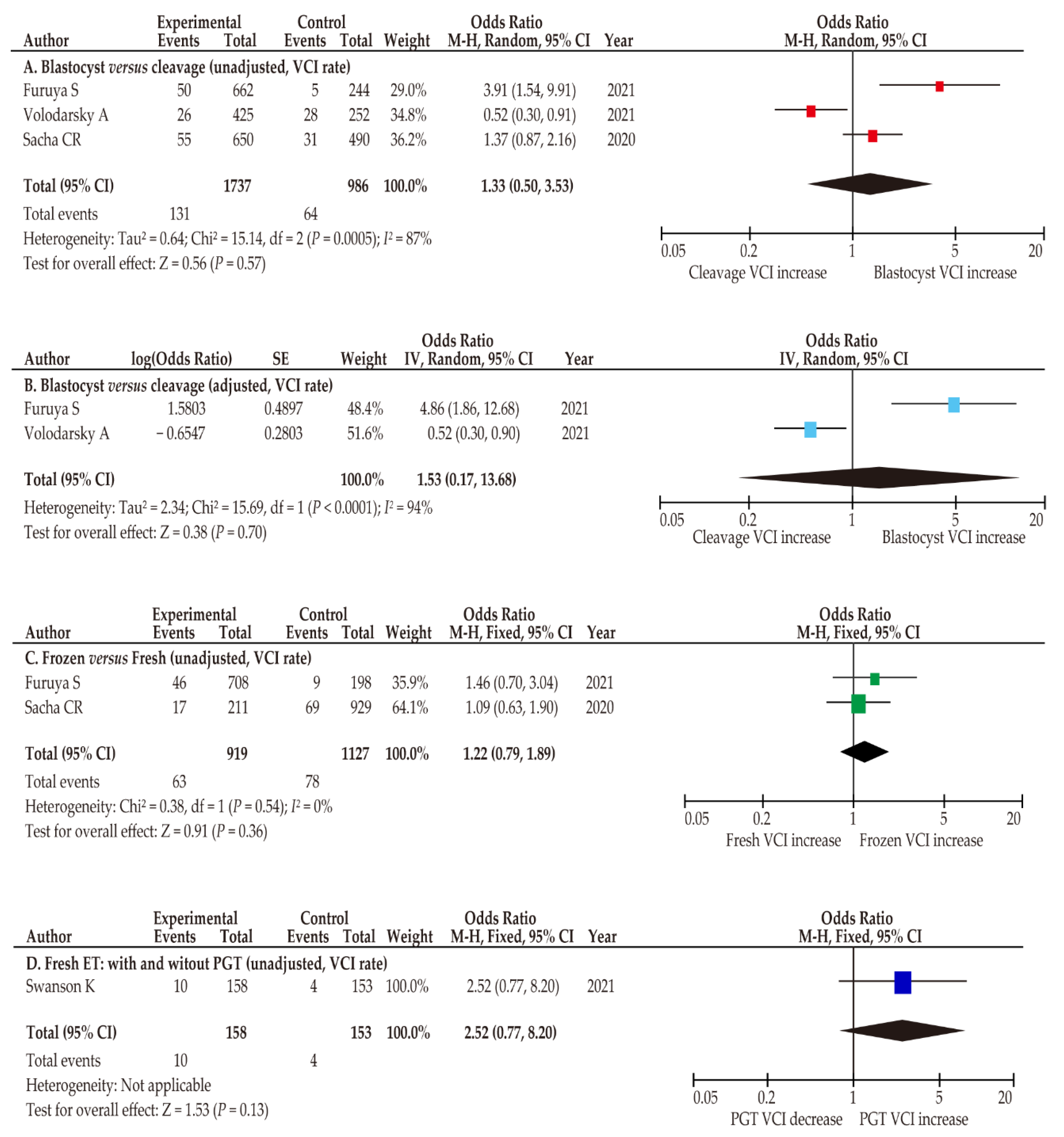
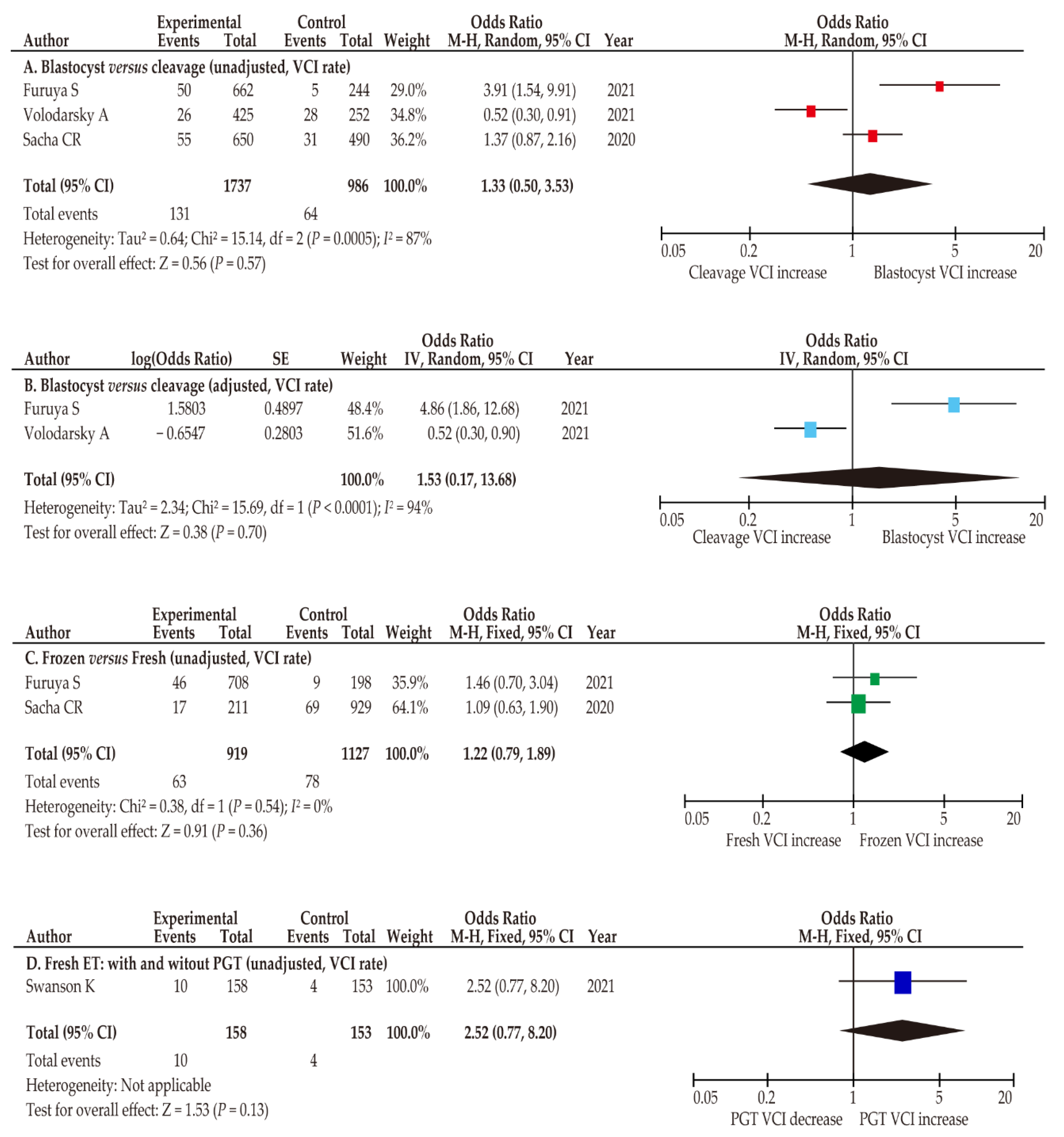
3.4.1. Blastocyst Transfer versus Cleavage-Stage Transfer
3.4.2. Frozen ET Versus Fresh ET
3.4.3. Effect of PGT on VCI
3.5. Secondary Outcomes: Delivery Outcomes of Women with ACI
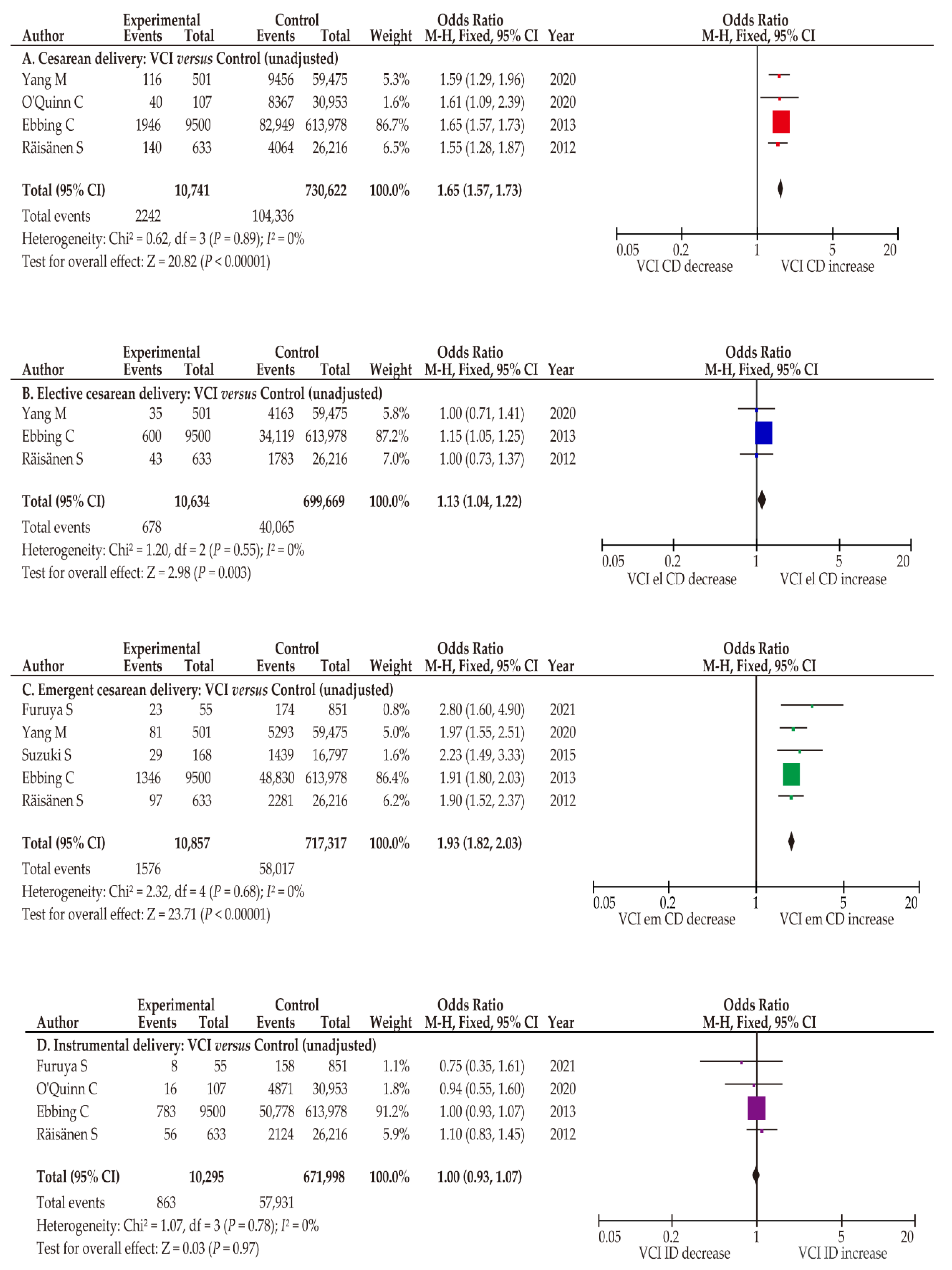
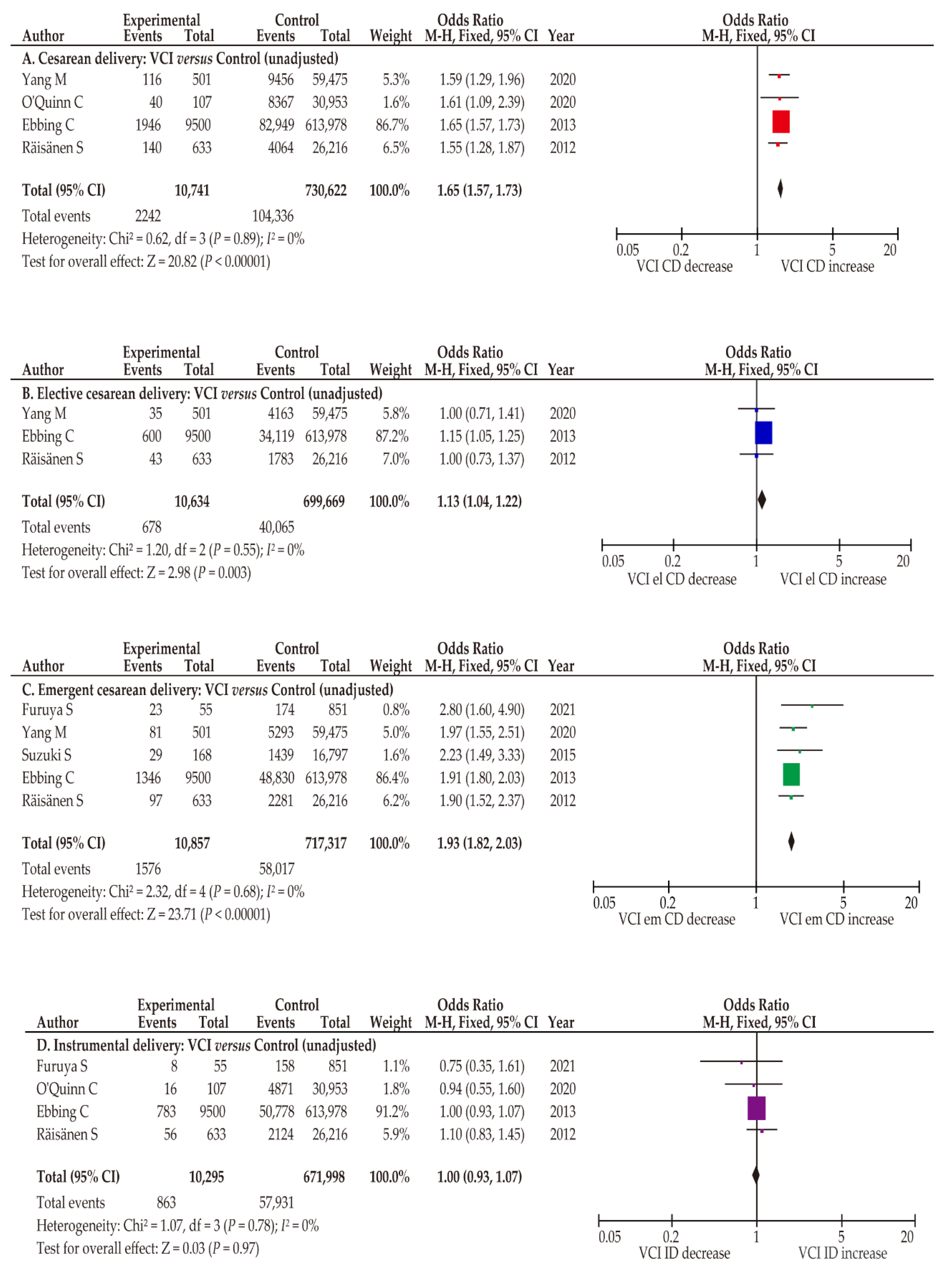
3.5.1. VCI Is Associated with an Increased Rate of Both Elective and Emergent CD
3.5.2. MCI Has a Potential to Be Associated with an Increased Rate of CD
3.5.3. Instrumental Delivery Was Not Increased in Women with ACI
3.6. Sensitivity Analysis: Patient Background and Obstetric Complications
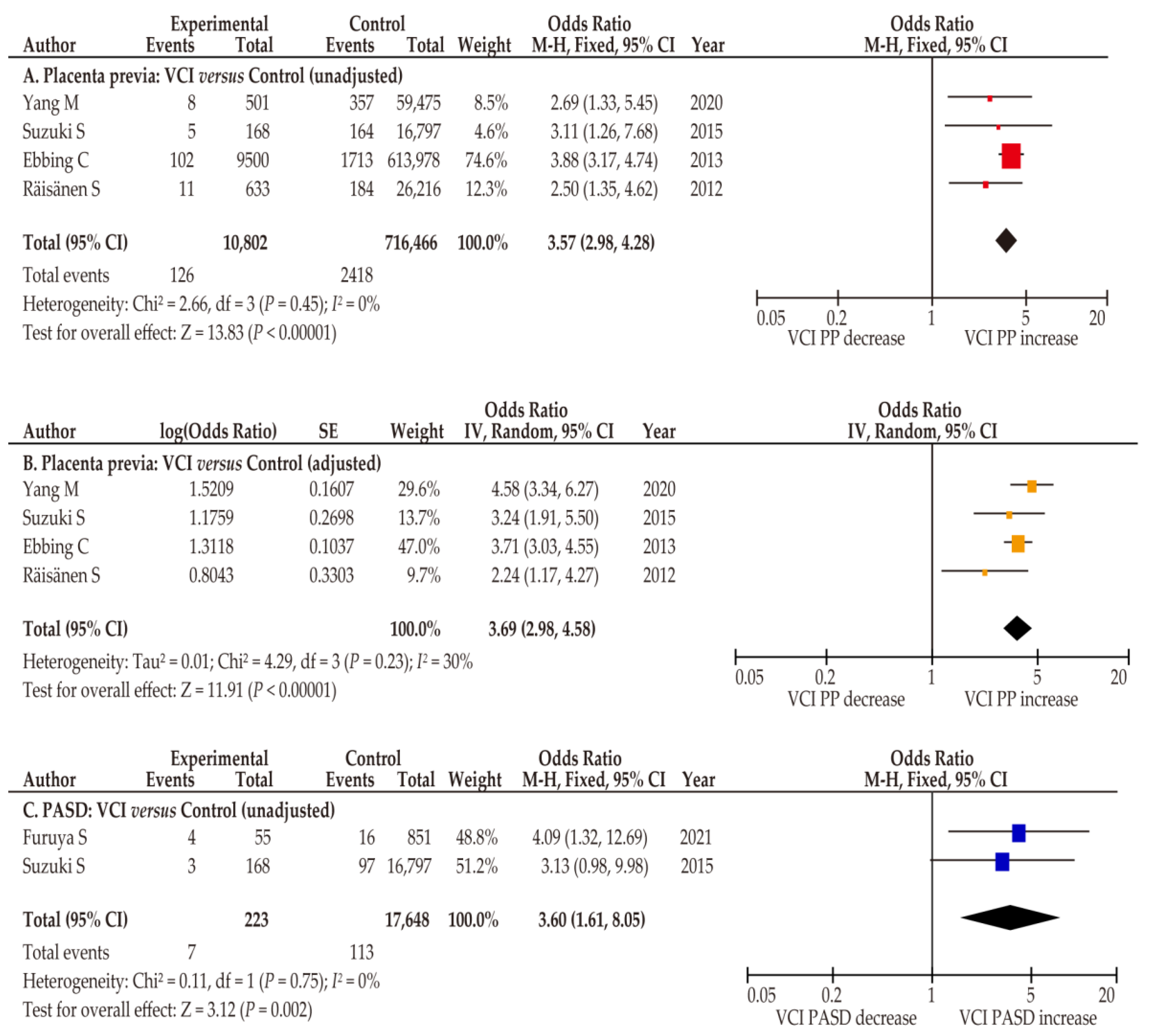
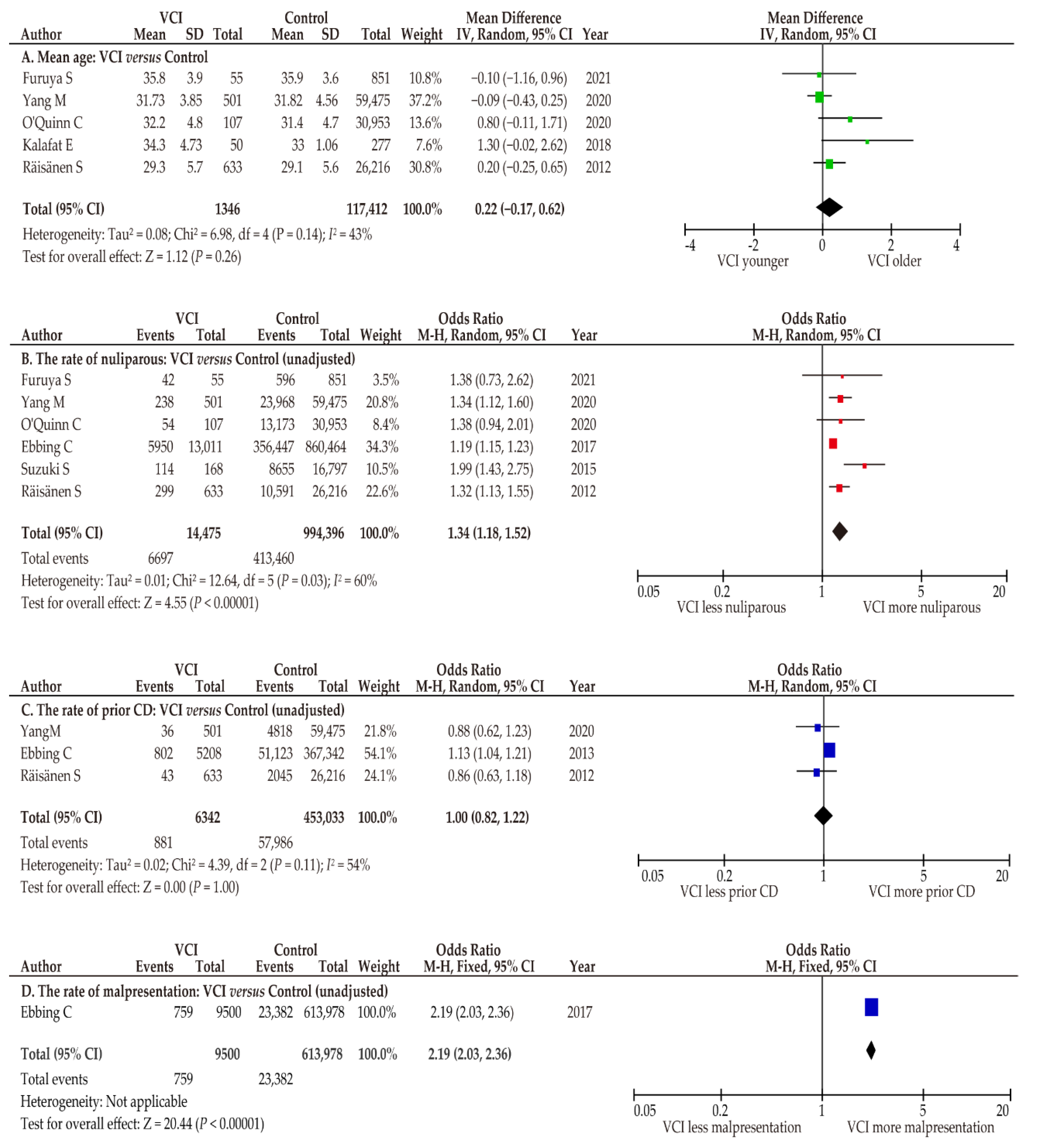
3.6.1. Abnormal Placentation
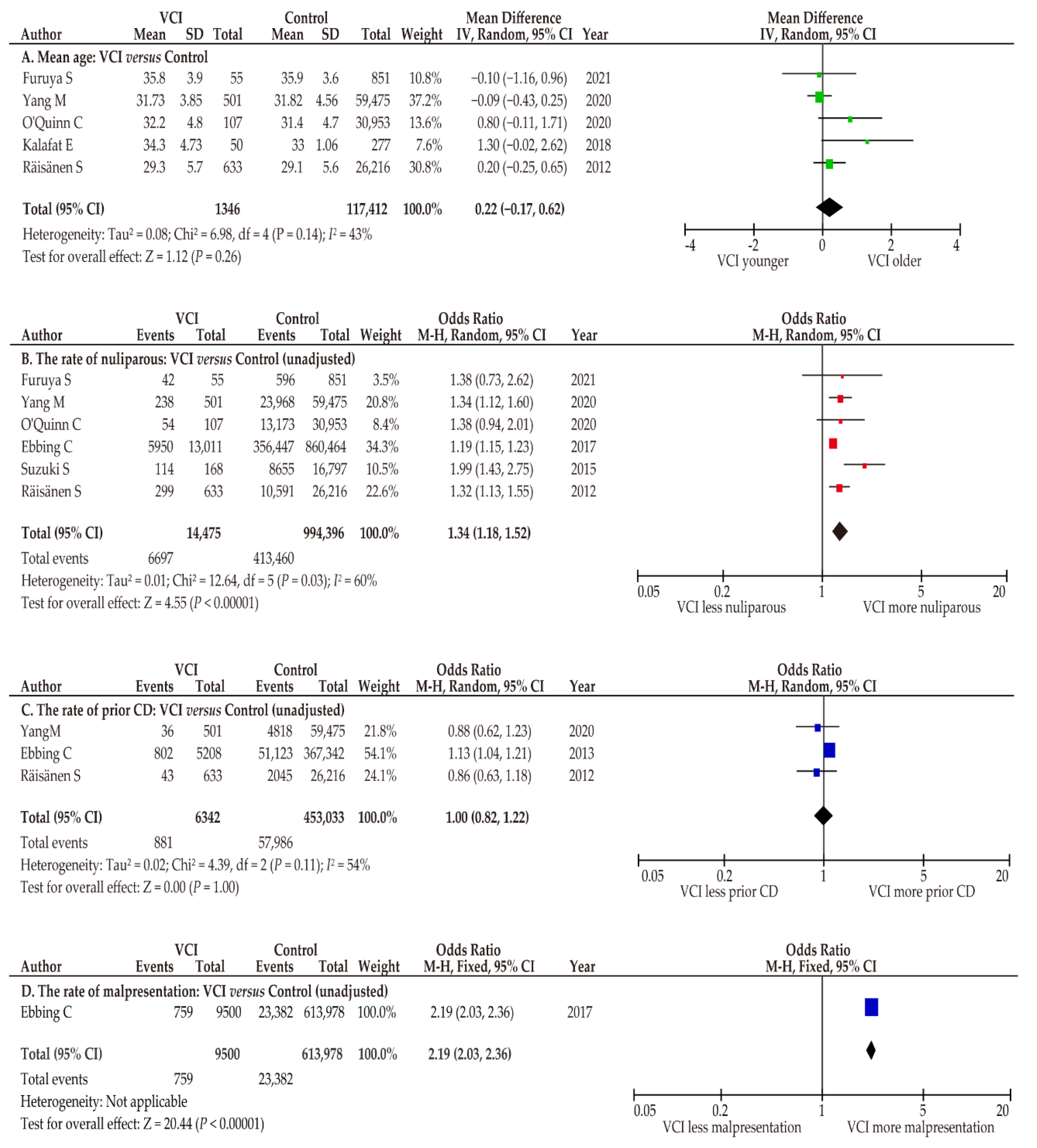
3.6.2. Patient Characteristics
3.6.3. Indications for Elective CD
3.6.4. Indications for Emergent CD
4. Discussion
4.1. Key Findings
4.2. Comparison with Existing Literature
4.2.1. Association between ART and ACI
4.2.2. Risk of ACI According to ART Type
4.2.3. Effect of ACI on the Rate of CD
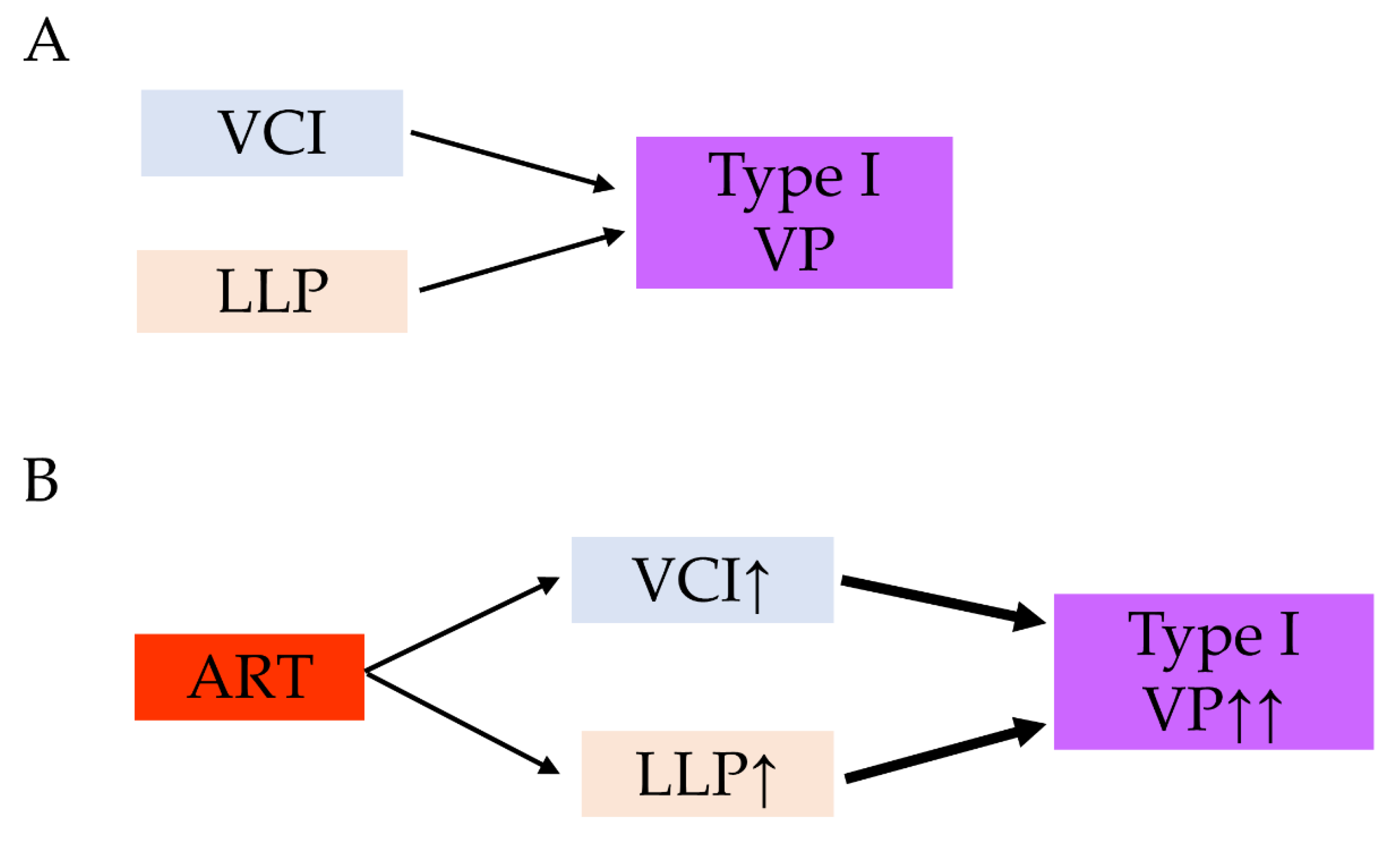
4.2.4. Relationship between VCI and Abnormal Placentation
4.3. Strengths and Limitations
5. Conclusions
5.1. Implications for Practice
5.2. Implications for Clinical Research
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Transparency
References
- Zahedi-Spung, L.D.; Stout, M.J.; Carter, E.B.; Dicke, J.M.; Tuuli, M.G.; Raghuraman, N. Obstetric outcomes in singleton pregnancies with abnormal placental cord insertions. Am. J. Perinatol. 2021; in press. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, D.; Eliner, Y. Performance of ultrasound for the visualization of the placental cord insertion. Curr. Opin. Obstet. Gynecol. 2019, 31, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, W.; Rojas, I.; Robert, J.A.; Schnapp, C.; Alcalde, J.L. Prenatal detection of velamentous insertion of the umbilical cord: A prospective color Doppler ultrasound study. Ultrasound. Obstet. Gynecol. 2003, 21, 564–569. [Google Scholar] [CrossRef] [PubMed]
- de Los Reyes, S.; Henderson, J.; Eke, A.C. A systematic review and meta-analysis of velamentous cord insertion among singleton pregnancies and the risk of preterm delivery. Int. J. Gynaecol. Obstet. 2018, 142, 9–14. [Google Scholar] [CrossRef]
- Asoglu, M.R.; Crimmins, S.; Kopelman, J.N.; Turan, O.M.; Goetzinger, K.R. Marginal placental cord insertion: The need for follow up. J. Matern. Fetal Neonatal. Med. 2022, 35, 1629–1635. [Google Scholar] [CrossRef]
- Nkwabong, E.; Njikam, F.; Kalla, G. Outcome of pregnancies with marginal umbilical cord insertion. J. Matern. Fetal Neonatal. Med. 2021, 34, 1133–1137. [Google Scholar] [CrossRef]
- O’Quinn, C.; Cooper, S.; Tang, S.; Wood, S. Antenatal diagnosis of marginal and velamentous placental cord insertion and pregnancy outcomes. Obstet. Gynecol. 2020, 135, 953–959. [Google Scholar] [CrossRef]
- Debebe, S.K.; Cahill, L.S.; Kingdom, J.C.; Whitehead, C.L.; Chandran, A.R.; Parks, W.T.; Serghides, L.; Baschat, A.; Macgowan, C.K.; Sled, J.G. Wharton’s jelly area and its association with placental morphometry and pathology. Placenta 2020, 94, 34–38. [Google Scholar] [CrossRef]
- Pavalagantharajah, S.; Villani, L.A.; D’Souza, R. Vasa previa and associated risk factors: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2020, 2, 100117. [Google Scholar] [CrossRef]
- Buchanan-Hughes, A.; Bobrowska, A.; Visintin, C.; Attilakos, G.; Marshall, J. Velamentous cord insertion: Results from a rapid review of incidence, risk factors, adverse outcomes and screening. Syst. Rev. 2020, 9, 147. [Google Scholar] [CrossRef]
- Matsuzaki, S.; Ueda, Y.; Nagase, Y.; Matsuzaki, S.; Kakuda, M.; Kakuda, S.; Sakaguchi, H.; Hisa, T.; Kamiura, S. Placenta accreta spectrum disorder complicated with endometriosis: Systematic review and meta-analysis. Biomedicines 2022, 10, 390. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, S.; Nagase, Y.; Takiuchi, T.; Kakigano, A.; Mimura, K.; Lee, M.; Matsuzaki, S.; Ueda, Y.; Tomimatsu, T.; Endo, M.; et al. Antenatal diagnosis of placenta accreta spectrum after in vitro fertilization-embryo transfer: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 9205. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, S.; Endo, M.; Kimura, T. Vasa previa with an intact amniotic membrane. Am. J. Obstet. Gynecol. 2017, 216, 616. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, S.J.; Ngo, G.; Maurel, K.A.; Hasegawa, J.; Arakaki, T.; Melcer, Y.; Maymon, R.; Vendittelli, F.; Shamshirsaz, A.A.; Erfani, H.; et al. Timing of birth and adverse pregnancy outcomes in cases of prenatally diagnosed vasa previa: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2022; in press. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, S.; Kimura, T. Vasa Previa. N. Engl. J. Med. 2019, 380, 274. [Google Scholar] [CrossRef]
- Gagnon, R. No. 231-Guidelines for the management of vasa previa. J. Obstet. Gynaecol. Can. 2017, 39, e415–e421. [Google Scholar] [CrossRef]
- Schachter, M.; Tovbin, Y.; Arieli, S.; Friedler, S.; Ron-El, R.; Sherman, D. In vitro fertilization is a risk factor for vasa previa. Fertil. Steril. 2002, 78, 642–643. [Google Scholar] [CrossRef]
- Pirtea, L.C.; Grigoraş, D.; Sas, I.; Ilie, A.C.; Stana, L.G.; Motoc, A.G.; Jianu, A.M.; Mazilu, O. In vitro fertilization represents a risk factor for vasa praevia. Rom. J. Morphol. Embryol. 2016, 57, 627–632. [Google Scholar]
- Zhang, W.; Geris, S.; Al-Emara, N.; Ramadan, G.; Sotiriadis, A.; Akolekar, R. Perinatal outcome of pregnancies with prenatal diagnosis of vasa previa: Systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2021, 57, 710–719. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernan, M.A.; Reeves, B.C.; Savovic, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danna, S.M.; Graham, E.; Burns, R.J.; Deschenes, S.S.; Schmitz, N. Association between depressive symptoms and cognitive function in persons with diabetes mellitus: A systematic review. PLoS ONE 2016, 11, e0160809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ROBINS-I Detailed Guidance. 2016. Available online: https://www.riskofbias.info/welcome/home/current-version-of-robins-i/robins-i-detailed-guidance-2016 (accessed on 5 July 2022).
- Cochrane Handbook for Systematic Reviews of Interventions. Version 6.1. Chapter 10: Analysing Data and Undertaking Meta-Analyses. 2020. Available online: https://training.cochrane.org/handbook/current/chapter-10. (accessed on 5 July 2022).
- Furuya, S.; Kubonoya, K.; Yamaguchi, T. Incidence and risk factors for velamentous umbilical cord insertion in singleton pregnancies after assisted reproductive technology. J. Obstet. Gynaecol. Res. 2021, 47, 1772–1779. [Google Scholar] [CrossRef] [PubMed]
- Swanson, K.; Huang, D.; Kaing, A.; Blat, C.; Rosenstein, M.G.; Mok-Lin, E.; Gras, J.; Sperling, J.D. Is preimplantation genetic testing associated with increased risk of abnormal placentation after frozen embryo transfer. Am. J. Perinatol. 2021, 38, 105–110. [Google Scholar] [CrossRef]
- Volodarsky-Perel, A.; Ton Nu, T.N.; Buckett, W.; Machado-Gedeon, A.; Cui, Y.; Shaul, J.; Dahan, M.H. Effect of embryo stage at transfer on placental histopathology features in singleton live births resulting from fresh embryo transfers. Fertil. Steril. 2021, 115, 673–682. [Google Scholar] [CrossRef]
- Sacha, C.R.; Harris, A.L.; James, K.; Basnet, K.; Freret, T.S.; Yeh, J.; Kaimal, A.; Souter, I.; Roberts, D.J. Placental pathology in live births conceived with in vitro fertilization after fresh and frozen embryo transfer. Am. J. Obstet. Gynecol. 2020, 222, 360.e1–360.e16. [Google Scholar] [CrossRef]
- Yang, M.; Zheng, Y.; Li, M.; Li, W.; Li, X.; Zhang, X.; Wang, R.; Zhang, J.; Zhou, F.; Yang, Q.; et al. Clinical features of velamentous umbilical cord insertion and vasa previa: A retrospective analysis based on 501 cases. Medicine 2020, 99, e23166. [Google Scholar] [CrossRef]
- Cochrane, E.; Pando, C.; Kirschen, G.W.; Soucier, D.; Fuchs, A.; Garry, D.J. Assisted reproductive technologies (ART) and placental abnormalities. J. Perinat. Med. 2020, 48, 825–828. [Google Scholar] [CrossRef]
- Yanaihara, A.; Hatakeyama, S.; Ohgi, S.; Motomura, K.; Taniguchi, R.; Hirano, A.; Takenaka, S.; Yanaihara, T. Difference in the size of the placenta and umbilical cord between women with natural pregnancy and those with IVF pregnancy. J. Assist. Reprod. Genet. 2018, 35, 431–434. [Google Scholar] [CrossRef] [Green Version]
- Kalafat, E.; Thilaganathan, B.; Papageorghiou, A.; Bhide, A.; Khalil, A. Significance of placental cord insertion site in twin pregnancy. Ultrasound Obstet. Gynecol. 2018, 52, 378–384. [Google Scholar] [CrossRef] [Green Version]
- Ebbing, C.; Johnsen, S.L.; Albrechtsen, S.; Sunde, I.D.; Vekseth, C.; Rasmussen, S. Velamentous or marginal cord insertion and the risk of spontaneous preterm birth, prelabor rupture of the membranes, and anomalous cord length, a population-based study. Acta Obstet. Gynecol. Scand. 2017, 96, 78–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, S.; Kato, M. Clinical significance of pregnancies complicated by velamentous umbilical cord insertion associated with other umbilical cord/placental abnormalities. J. Clin. Med. Res. 2015, 7, 853–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebbing, C.; Kiserud, T.; Johnsen, S.L.; Albrechtsen, S.; Rasmussen, S. Prevalence, risk factors and outcomes of velamentous and marginal cord insertions: A population-based study of 634,741 pregnancies. PLoS ONE 2013, 8, e70380. [Google Scholar] [CrossRef] [PubMed]
- Räisänen, S.; Georgiadis, L.; Harju, M.; Keski-Nisula, L.; Heinonen, S. Risk factors and adverse pregnancy outcomes among births affected by velamentous umbilical cord insertion: A retrospective population-based register study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 165, 231–234. [Google Scholar] [CrossRef]
- Delbaere, I.; Goetgeluk, S.; Derom, C.; De Bacquer, D.; De Sutter, P.; Temmerman, M. Umbilical cord anomalies are more frequent in twins after assisted reproduction. Hum. Reprod. 2007, 22, 2763–2767. [Google Scholar] [CrossRef] [Green Version]
- Baulies, S.; Maiz, N.; Muñoz, A.; Torrents, M.; Echevarría, M.; Serra, B. Prenatal ultrasound diagnosis of vasa praevia and analysis of risk factors. Prenat. Diagn. 2007, 27, 595–599. [Google Scholar] [CrossRef]
- Jauniaux, E.; Englert, Y.; Vanesse, M.; Hiden, M.; Wilkin, P. Pathologic features of placentas from singleton pregnancies obtained by in vitro fertilization and embryo transfer. Obstet. Gynecol. 1990, 76, 61–64. [Google Scholar]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Gavriil, P.; Jauniaux, E.; Leroy, F. Pathologic examination of placentas from singleton and twin pregnancies obtained after in vitro fertilization and embryo transfer. Pediatr. Pathol. 1993, 13, 453–462. [Google Scholar] [CrossRef]
- Hasegawa, J.; Iwasaki, S.; Matsuoka, R.; Ichizuka, K.; Sekizawa, A.; Okai, T. Velamentous cord insertion caused by oblique implantation after in vitro fertilization and embryo transfer. J. Obstet. Gynaecol. Res. 2011, 37, 1698–1701. [Google Scholar] [CrossRef]
- Ismail, K.I.; Hannigan, A.; O’Donoghue, K.; Cotter, A. Abnormal placental cord insertion and adverse pregnancy outcomes: A systematic review and meta-analysis. Syst. Rev. 2017, 6, 242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vahanian, S.A.; Lavery, J.A.; Ananth, C.V.; Vintzileos, A. Placental implantation abnormalities and risk of preterm delivery: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2015, 213, S78–S90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monie, I.W. Velamentous insertion of the cord in early pregnancy. Am. J. Obstet. Gynecol. 1965, 93, 276–281. [Google Scholar] [CrossRef]
- Hasegawa, J.; Farina, A.; Simonazzi, G.; Bisulli, M.; Puccetti, C.; Pilu, G.; Gabrielli, S.; Rizzo, N. Umbilical cord insertion into the lower segment of the uterus at 11 to 13 weeks’ gestation is associated with maternal serum PAPP-A. Prenat. Diagn. 2011, 31, 434–438. [Google Scholar] [CrossRef]
- Tsakiridis, I.; Dagklis, T.; Athanasiadis, A.; Dinas, K.; Sotiriadis, A. Impact of marginal and velamentous cord insertion on uterine artery doppler indices, fetal growth, and preeclampsia. J. Ultrasound Med. 2021; in press. [Google Scholar] [CrossRef]
- McLennan, J.E. Implications of the eccentricity of the human umbilical cord. Am. J. Obstet. Gynecol. 1968, 101, 1124–1130. [Google Scholar] [CrossRef]
- Hasegawa, J. Sonoembryological evaluations of the development of placenta previa and velamentous cord insertion. J. Obstet. Gynaecol. Res. 2015, 41, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Vuong, L.N.; Dang, V.Q.; Ho, T.M.; Huynh, B.G.; Ha, D.T.; Pham, T.D.; Nguyen, L.K.; Norman, R.J.; Mol, B.W. IVF Transfer of fresh or frozen embryos in women without polycystic ovaries. N. Engl. J. Med. 2018, 378, 137–147. [Google Scholar] [CrossRef]
- Malizia, B.A.; Hacker, M.R.; Penzias, A.S. Cumulative live-birth rates after in vitro fertilization. N. Engl. J. Med. 2009, 360, 236–243. [Google Scholar] [CrossRef] [Green Version]
- Diego, D.; Hipp, H.S. Reducing obstetric morbidity in in vitro fertilization pregnancies. JAMA Netw. Open 2021, 4, e2124170. [Google Scholar] [CrossRef]
- Ghidini, A.; Gandhi, M.; McCoy, J.; Kuller, J.A. Society for maternal-fetal medicine consult series #60: Management of pregnancies resulting from in vitro fertilization. Am. J. Obstet. Gynecol. 2022, 226, B2–B12. [Google Scholar] [PubMed]
- Gross, A.; Markota Ajd, B.; Specht, C.; Scheier, M. Systematic screening for vasa previa at the 20-week anomaly scan. Acta Obstet. Gynecol. Scand. 2021, 100, 1694–1699. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Tanaka, K.; Osato, K.; Kusaka, H.; Maegawa, Y.; Taniguchi, H.; Ikeda, T. Evaluation of maternal and neonatal outcomes of assisted reproduction technology: A retrospective cohort study. Medicina 2020, 56, 32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caughey, A.B.; Cahill, A.G.; Guise, J.M.; Rouse, D.J. Safe prevention of the primary cesarean delivery. Am. J. Obstet. Gynecol. 2014, 210, 179–193. [Google Scholar] [CrossRef]
- Matthews, K.C.; Quinn, A.S.; Chasen, S.T. Potentially preventable primary cesarean sections in future placenta accreta spectrum. Am. J. Perinatol. 2022, 39, 120–124. [Google Scholar] [CrossRef]
- Hasegawa, J.; Matsuoka, R.; Ichizuka, K.; Sekizawa, A.; Okai, T. Velamentous cord insertion: Significance of prenatal detection to predict perinatal complications. Taiwan J. Obstet. Gynecol. 2006, 45, 21–25. [Google Scholar] [CrossRef] [Green Version]
- Hasegawa, J.; Matsuoka, R.; Ichizuka, K.; Sekizawa, A.; Farina, A.; Okai, T. Velamentous cord insertion and atypical variable decelerations with no accelerations. Int. J. Gynaecol. Obstet. 2005, 90, 26–30. [Google Scholar] [CrossRef]
- Hasegawa, J.; Matsuoka, R.; Ichizuka, K.; Sekizawa, A.; Farina, A.; Okai, T. Velamentous cord insertion into the lower third of the uterus is associated with intrapartum fetal heart rate abnormalities. Ultrasound Obstet. Gynecol. 2006, 27, 425–429. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | ART No. | ART ACI | Cont No. | Cont ACI | Crude OR (95%CI) | Adjusted OR (95%CI) |
|---|---|---|---|---|---|---|---|
| VCI | |||||||
| Yang M [29] | 2020 | 1625 | 19 | 58,351 | 482 | 1.41 (0.89–2.23) | -- |
| Cochrane E [30] | 2020 | 120 | 14 | 240 | 7 | 4.40 (1.72–11.21) | -- |
| O’Quinn C [7] | 2020 | 1524 | 5 | 24,992 | 83 | 0.99 (0.40–2.44) | -- |
| Yanaihara A # [31] | 2018 | 157 | 32 | 1453 | 145 | 2.31 (1.51–3.53) | 1.72 (1.08–2.72) |
| Kalafat E * [32] | 2018 | 159 | 18 | 338 | 32 | 1.22 (0.66–2.25) | -- |
| Ebbing C [33] | 2017 | 16,934 | 589 | 843,531 | 12,422 | 2.41 (2.22–2.62) | 2.16 (1.94–2.41) |
| Suzuki S [34] | 2015 | 936 | 36 | 16,029 | 132 | 4.82 (3.31–7.01) | -- |
| Räisänen S [36] | 2012 | 677 | 22 | 26,172 | 611 | 1.41 (0.91–2.17) | -- |
| Delbaere I * [37] | 2007 | 880 | 65 | 2119 | 76 | 2.14 (1.52–3.01) | 1.96 (1.47–2.61) |
| Jauniaux E [39] | 1990 | 50 | 6 | 50 | 1 | 6.68 (0.77–57.70) | -- |
| MCI | |||||||
| Cochrane E [30] | 2020 | 120 | 34 | 240 | 35 | 2.32 (1.36–3.95) | -- |
| O’Quinn C [7] | 2020 | 1524 | 116 | 24,992 | 1066 | 1.85 (1.52–2.26) | -- |
| Kalafat E * [32] | 2018 | 159 | 45 | 338 | 125 | 0.67 (0.45–1.01) | -- |
| Ebbing C [33] | 2017 | 16,934 | 1475 | 843,531 | 47,686 | 1.59 (1.51–1.68) | 1.43 (1.34–1.53) |
| Delbaere I * [37] | 2007 | 880 | 125 | 2119 | 184 | 1.74 (1.37–2.22) | 1.29 (1.05–1.59) |
| Jauniaux E [39] | 1990 | 50 | 13 | 50 | 5 | 3.16 (1.03–9.69) | -- |
| VP | |||||||
| Baulies S [38] | 2007 | 824 | 4 | 11,239 | 5 | 10.96 (2.94–40.89) | -- |
| Author | Year | Exp No. | Exp Events | Cont No. | Cont Events | Crude OR (95%CI) | Adjusted OR (95%CI) |
|---|---|---|---|---|---|---|---|
| Blastocyst versus Cleavage | |||||||
| Furuya S [25] | 2021 | 662 | 50 | 244 | 5 | 3.91 (1.54–9.91) | 4.86 (1.86–12.68) |
| Volodarsky A [27] | 2021 | 425 | 26 | 252 | 28 | 0.52 (0.30–0.91) | 0.5 (0.3–0.9) |
| Sacha CR [28] | 2020 | 650 | 55 | 490 | 31 | 1.37 (0.87–2.16) | -- |
| Frozen ET versus Fresh ET | |||||||
| Furuya S [25] | 2021 | 708 | 46 | 198 | 9 | 1.46 (0.70–3.04) | 1.58 (0.79–3.55) |
| Sacha CR [28] | 2020 | 211 | 17 | 929 | 69 | 1.09 (0.63–1.90) | -- |
| Frozen ET with versus without PGT | |||||||
| Swanson K [26] | 2021 | 158 | 10 | 153 | 4 | 2.52 (0.77–8.20) | -- |
| Author | Year | Control No. | Control Events | VCI No. | VCI Events | Crude OR (95%CI) | Adjusted OR (95%CI) |
|---|---|---|---|---|---|---|---|
| CD (all) | |||||||
| Yang M [29] | 2020 | 59,475 | 9456 | 501 | 116 | 1.59 (1.29–1.96) | -- |
| O’Quinn C [7] | 2020 | 30,953 | 8367 | 107 | 40 | 1.61 (1.09–2.39) | -- |
| Ebbing C [35] | 2013 | 613,978 | 82,949 | 9500 | 1946 | 1.65 (1.57–1.73) | 1.54 (1.47–1.62) |
| Räisänen S [36] | 2012 | 26,216 | 4064 | 633 | 140 | 1.55 (1.28–1.87) | -- |
| Elective CD | |||||||
| Yang M [29] | 2020 | 59,475 | 4163 | 501 | 35 | 1.00 (0.71–1.41) | -- |
| Ebbing C [35] | 2013 | 613,978 | 34,119 | 9500 | 600 | 1.15 (1.05–1.25) | 1.11 (1.02–1.22) |
| Räisänen S [36] | 2012 | 26,216 | 1783 | 633 | 43 | 1.00 (0.73–1.37) | -- |
| Emergent CD | |||||||
| Furuya S [25] | 2021 | 851 | 174 | 55 | 23 | 2.80 (1.60–4.90) | -- |
| Yang M [29] | 2020 | 59,475 | 5293 | 501 | 81 | 1.97 (1.55–2.51) | -- |
| Suzuki S [34] | 2015 | 16,797 | 1439 | 168 | 29 | 2.23 (1.49–3.33) | -- |
| Ebbing C [35] | 2013 | 613,978 | 48,830 | 9500 | 1346 | 1.91 (1.80–2.03) | 1.80 (1.69–1.91) |
| Räisänen S [36] | 2012 | 26,216 | 2281 | 633 | 97 | 1.90 (1.52–2.37) | -- |
| Instrumental delivery | |||||||
| Furuya S [25] | 2021 | 851 | 158 | 55 | 8 | 0.75 (0.35–1.61) | -- |
| O’Quinn C [7] | 2020 | 30,953 | 4871 | 107 | 16 | 0.94 (0.55–1.60) | -- |
| Ebbing C [35] | 2013 | 613,978 | 50,778 | 9500 | 783 | 1.00 (0.93–1.07) | 0.90 (0.83–0.97) |
| Räisänen S [36] | 2012 | 26,216 | 2124 | 633 | 56 | 1.10 (0.83–1.45) | -- |
| Author | Year | Cont No. | Cont Events | VCI No. | VCI Events | Crude OR (95% CI) | Adjusted OR (95% CI) |
|---|---|---|---|---|---|---|---|
| Previa | |||||||
| Yang M [29] | 2020 | 59,475 | 357 | 501 | 8 | 2.69 (1.33–5.45) | 4.58 (3.34–6.27) |
| Suzuki S [34] | 2015 | 16,797 | 164 | 168 | 5 | 3.11 (1.26–7.68) | 3.24 (0.91–5.5) |
| Ebbing C [35] | 2013 | 613,978 | 1713 | 9500 | 102 | 3.88 (3.17–4.74) | 3.71 (3.03–4.55) |
| Räisänen S [36] | 2012 | 26,216 | 184 | 633 | 11 | 2.50 (1.35–4.62) | 2.24 (1.17–4.27) |
| PASD | |||||||
| Furuya S [25] | 2021 | 851 | 16 | 55 | 4 | 4.09 (1.32–12.69) | -- |
| Suzuki S [34] | 2015 | 16,797 | 97 | 168 | 3 | 3.13 (0.98–9.98) | -- |
| Author | Year | Cont No. | VCI No. | Cont Age | VCI Age | Cont Nuli | VCI Nuli | Control mal | Vci mal | Control Prior CD | VCI Prior CD |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Furuya S [25] | 2021 | 851 | 55 | 35.9 ± 3.6 | 35.8 ± 3.9 | 596 | 42 | -- | -- | -- | -- |
| Yang M [29] | 2020 | 59,475 | 501 | 31.82 ± 4.56 | 31.73 ± 3.85 | 23,968 | 238 | -- | -- | 4818 | 36 |
| O’Quinn C [7] | 2020 | 30,953 | 107 | 31.4 ± 4.7 | 32.2 ± 4.8 | 13,173 | 54 | -- | -- | -- | -- |
| Kalafat E * [32] | 2018 | 277 | 50 | 33 ± 1.06 C | 34.3 ± 4.73 C | -- | -- | -- | -- | -- | -- |
| Ebbing C † [33] | 2017 | 860,464 | 13,011 | -- | -- | 356,447 | 5950 | -- | -- | -- | -- |
| Suzuki S [34] | 2015 | 16,797 | 168 | -- | -- | 8655 | 114 | -- | -- | -- | -- |
| Ebbing C † [35] | 2013 | 613,978 | 9500 | -- | -- | 256,136 | 4292 | 23,382 | 759 | A | B |
| Räisänen S [36] | 2012 | 26,216 | 633 | 29.1 ± 5.6 | 29.3 ± 5.7 | 10,591 | 299 | -- | -- | 43 | 2045 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsuzaki, S.; Ueda, Y.; Matsuzaki, S.; Nagase, Y.; Kakuda, M.; Lee, M.; Maeda, M.; Kurahashi, H.; Hayashida, H.; Hisa, T.; et al. Assisted Reproductive Technique and Abnormal Cord Insertion: A Systematic Review and Meta-Analysis. Biomedicines 2022, 10, 1722. https://doi.org/10.3390/biomedicines10071722
Matsuzaki S, Ueda Y, Matsuzaki S, Nagase Y, Kakuda M, Lee M, Maeda M, Kurahashi H, Hayashida H, Hisa T, et al. Assisted Reproductive Technique and Abnormal Cord Insertion: A Systematic Review and Meta-Analysis. Biomedicines. 2022; 10(7):1722. https://doi.org/10.3390/biomedicines10071722
Chicago/Turabian StyleMatsuzaki, Shinya, Yutaka Ueda, Satoko Matsuzaki, Yoshikazu Nagase, Mamoru Kakuda, Misooja Lee, Michihide Maeda, Hiroki Kurahashi, Harue Hayashida, Tsuyoshi Hisa, and et al. 2022. "Assisted Reproductive Technique and Abnormal Cord Insertion: A Systematic Review and Meta-Analysis" Biomedicines 10, no. 7: 1722. https://doi.org/10.3390/biomedicines10071722
APA StyleMatsuzaki, S., Ueda, Y., Matsuzaki, S., Nagase, Y., Kakuda, M., Lee, M., Maeda, M., Kurahashi, H., Hayashida, H., Hisa, T., Mabuchi, S., & Kamiura, S. (2022). Assisted Reproductive Technique and Abnormal Cord Insertion: A Systematic Review and Meta-Analysis. Biomedicines, 10(7), 1722. https://doi.org/10.3390/biomedicines10071722